![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
97 Cards in this Set
- Front
- Back
|
what is the most common cause of cervical myelopathy? |
the most common causes degenerative cervical spondylosis |
|
|
patient presents to the office complaining of clumsiness in the hands and gait imbalance what is the diagnosis What is the next most appropriate step in management. |
cervical myelopathy MRI or CT myelogram for patient with a pacemaker to R/O Most common associated lumbar spinal stenosis |
|
|
based on gait and ambulatory function if one is having difficulty with gait but is fully employed what grade myelopathy does the patient have? |
grade 2 |
|
|
if one is unable to walk without assistance what grade myelopathy does does the patient have? |
grade 4 |
|
if the patient holds fingers extended and adducted the small finger spontaneously abducts what is the diagnosis |
finger escape sign =cervical myelopathy |
|
|
lateral x-ray of the cervical spine pavlo ratio less than ____is suggestive congenital narrow cervical spine? |
0.8. predisposing to stenosis and spinal cord compression |
|
|
patient's with improved with nonoperative outcomes associated with larger transverse area of the spinal cord_____? |
greater than 70 mm |
|
|
what is the treatment in a patient with kyphosis greater than 10° that involves 1 or 2 levels of compression? |
ACDF anterior corpectomy hybrid |
|
|
what is the treatmen 4 patient with kyphosis less than 10° that involves 1 or 2 levels of compression? |
ACDF anterior corpectomy hybrid |
|
|
what is the treatment for patient with kyphosis greater than 10° and involves 3 or more levels of compression? |
anterior corpectomy to correct the kyphosis and posterior decompression |
|
|
what is the treatment for patient with less than 10° rigid kyphosis that involves 3 or more levels of compression |
posterior alone laminoplasty versus laminectomy plus fusion |
|
|
the patient with cervical kyphosis Which variables has the strongest association with poor clinical outcomes in patients who undergo expansive laminoplasty for cervical spondylotic myelopathy? |
Local kyphosis angle >13° is contraindicated |
|
|
what is the most common complication with an anterior approach to the cervical spine? |
RIGHT recurrent laryngeal nerve injury if not improved at 6 weeks consult ENT |
|

A 47-year old female with Type-2 diabetes and a pacemaker presents with bilateral buttock and leg pain that is worse with prolonged walking and improves with sitting. Her lower extremity symptoms are severe enough that she reports she feels "unstable" on her feet. Physical exam shows 5/5 strength in all muscles groups in the lower extremity. clonus is present with forced ankle dorsiflexion on physical exam. A lumbar myelogram is performed . What is the most appropriate next step in treatment. 1. Lumbar decompression 2. Lumbar decompression with arthrodesis 3. A trial of physical therapy and NSAIDS 4. Lumbar epidural steroid injections 5. CT myelogram of cervical spine |
The clinical presentation and imaging studies are consistent with concurrent symptoms of myelopathy and neurogenic claudication in a patient with lumbar degenerative spondylolisthesis. An CT myelogram of the cervical spine would be the most appropriate next step in management as the patient is unable to obtain an MRI due to the pacemaker.ans5 |
|

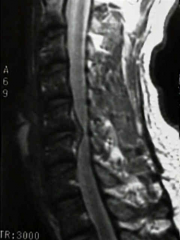
A 68-year-old female presents with progressive loss of ability to ambulate and dexterity problems with her hands. Six months ago she was able to walk with a cane, but now has difficulty with ambulating with a walker. She also reports difficulty with her hands and needs assistance with eating. Physical exam shows limited neck extension. Radiographs, tomography, and magnetic-resonance-imaging are shown in Figure A, B, and C respectively. What is the most appropriate treatment? 1. NSAIDS, physical therapy, and clinical observation 2. C3 to C6 cervical laminectomy 3. C3 to C6 laminoplasty using an open-door technique 4. C3 to C6 decompressive laminectomy with instrumented fusion 5. Multilevel anterior cervical decompression with strut grafting and anterior plate fixation, followed by posterior decompression and fusion |

The patients symptoms are consistent with progressive cervical myelopathy. Her symptoms are progressive and severe, and therefore surgical decompression is indicated. She has cervical kyphosis as demonstrated on physical exam and imaging, with compression at three levels (C3/4, C4/5, C5/6). An anterior procedure is mandatory to correct her kyphosis and remove the anterior compressive lesions. Of the options listed, only answer 5 involves an anterior procedure, and therefore, it is the most appropriate treatment.ans5 |
|
|
Which of the following variables has the strongest association with poor clinical outcomes in patients who undergo expansive laminoplasty for cervical spondylotic myelopathy? 1. Multi-level stenosis 2. Duration of symptoms 3. Local kyphosis angle > 13 degrees 4. Osteoporosis 5. MRI finding of CSF effacement
|
Fixed cervical kyphosis is associated with poor functional outcomes when performing an expansive laminoplasty for cervical spondylotic myelopathy. |
|
|
All of the following clinical signs are characteristic of an upper motor neuron disorder EXCEPT 1. Fasciculations 2. Spasticity 3. Muscle weakness 4. Exaggerated deep tendon reflexes 5. Sustained clonus
|
Fasciculations are a clinical sign of a lower motor neuron disorders. The lower motor neuron is defined as the nerve fibers traveling from the anterior horn of the spinal cord to the peripheral muscle. Lesions to the lower motor neuron are characterized by fasciculations and flaccid paralysis. The upper motor neuron is defined as the nerve fibers traveling from the motor cortex of the brain to the anterior horn of the spinal cord. Upper motor neuron disorders are characterized by spastic paralysis, exaggerated deep tendon reflexes, sustained clonus, and an up-going Babinski sign. Muscle weakness is a clinical sign of both upper and lower motor neuron disorders. ans1 |
|
|
what is the most common neurologic complication after a laminoplasty and a myelopathic patient with cervical stenosis? clinical presentation? |
C5 palsy weakness deltoid and biceps |
|
|
Following a C3-C7 laminoplasty in a myelopathic patient with cervical stenosis, the most common neurologic complication would manifest with which of the following new postoperative exam findings 1. Change in voice and difficulty swallowing 2. Triceps weakness 3. Deviation of the tongue 4. Ptosis, miosis, anhydrosis 5. Biceps weakness
|
C5 palsy (deltoid and biceps weakness) is the most likely neurologic complication following cervical laminoplasty, with an incidence of ~5%. Its pathogenesis and the options for prevention and treatment remain unidentified and many controversies exist. Two theories to account for the pathogenesis of C5 palsy exist: 1) nerve root injury 2) segmental spinal cord disorder. Neither of these hypotheses has been consistently supported and evidence to refute each hypothesis can be found in the literature. Although patients with C5 palsy generally have a good prognosis for neurologic and functional recovery, those with severe paralysis require significantly longer recovery times when compared to more mild cases.ans5 |
|
|
Which classification system for cervical myelopathy focuses exclusively on lower extremity function? 1. Nurick 2. Japanese Orthopaedic Association 3. Modified Japanese Orthopaedic Association 4. Ranawat 5. Oswestry |
The Nurick Classification system is a classification system for cervical myelopathy that focuses on the ambulatory status of the patient. Incorrect Answers: |
|
A 45-year-old man presents with increasing difficulty ambulating normally and clumsiness when he is either combing his hair or buttoning his shirt. A sagittal cut of his MRI is shown in Figure A. What is the next most appropriate step in management? 1. Observation 2. Epidural injection 3. Physical therapy and anti-inflammatory medication 4. Anterior cervical diskectomy and fusion 5. Posterior cervical laminectomy and fusion |
The MRI scans demonstrate a midline soft cervical disc herniation. Controversy had existed as to whether this entity is best managed by an anterior approach or a posterior cervical laminotomy-foraminotomy. The Herkowitz Spine article from 1990 prospectively compared 28 patients treated with anterior discectomy and fusion to 16 treated with posterior laminotomy-foraminotomy. 26 of 28 patients in the anterior group had excellent or good results and 12 of 16 in the posterior group had excellent or good results, measured by relief of pain and weakness at mean 4.2 year follow-up. This study agreed with other previous ones that demonstrated the anterior approach for cervical central soft disc herniations is superior to the posterior approach.ans4 |
|
|
what is the most important prognostic variable relating to neurologic recovery and incomplete spinal cord injury |
severity of neurologic deficitits completeness |
|
|
was most common incomplete spinal cord injury? clinical presentation & what is hyperpathia? |
central cord syndrome Weakness and hand dexterity upper extremity is affected worse than the lower extremities hyperpathia burning in the distal upper extremity |
|
|
physical exam findings of upper motor neuron involvement? name 8 physical exam findings and test to diagnose upper motor neuron involvement
|
upper motor neuron equals spasticity think of cervical myelopathy the finger with upper motor neuron
|
|
|
physical exam finding of lower motor neuron signs |
flaccid paralysis fibrillations fasciculations hypotonia areflexia weakness and strength everything goes down with lower motor neuron deficits
|
|
|
which incomplete spinal cord injury has a worse prognosis for recovery? clinical presentation? |
anterior cord syndrome lower extremity is affected more than upper extremities loss of motor and loss of pain and temperature |
|
|
which incomplete spinal cord injury has the excellent prognosis for recovery? |
Brown Sequard syndrome |
|
|
described the clinical presentation of a Brown Sequard syndrome? |
step on the LEFT loss of motor function on the LEFT ipsilateral and contralateral loss pain and temperature classically 2 levels below |
|
|
A 79-year old man falls sustaining a hyperextension injury to his neck. A lateral radiograph, CT scan and MRI are seen in Figures A through C. On motor examination, he has 3/5 strength in his deltoids, elbow and wrist flexors and extensors. He has 4/5 strength in his hip flexors, knee flexors, extensors, ankle dorsiflexors and plantarflexors. Sensation is preserved in both his upper and lower extremities as well as his sacral segments. Injury to which of the following tracts contributes greatest to his motor function deficits? 1. Fasciculus gracilis 2. Fasciculus cuneatus 3. Anterior corticospinal 4. Lateral corticospinal 5. Lateral spinothalamic
|
The clinical scenario describes a patient with central cord syndrome, resulting in an injury to his lateral corticospinal tract. Figures A through C show a spondylotic spine with central narrowing and CSF effacement that is worse at the C4-5 level. The lateral corticospinal tract is the main descending motor tract (Illustration A). Its anatomic position places the upper extermity motor tracts at greater risk than the lower extremity tracts. As such, injury to the lateral corticospinal tract is characterized by upper greater than lower extremity involvement and motor deficits being more pronounced than sensory deficits. |
|
|
A 73-year-old man falls forward from standing height and sustaining a hyperextension injury to his neck. Physical exam of his lower extremities shows he has 4+ of 5 strength to hip flexion, knee extension, and ankle plantar flexion. Physical exam of his upper extremities shows 4 of 5 deltoid and triceps strength, with 3 of 5 wrist flexion and finger flexion strength. A CT scan and MRI are shown in Figures A and B. Which of the following neurologic pathways was most likely affected? 1. Posterior funiculi 2. Lateral corticospinal tract 3. Central Gray matter 4. Lateral spinothalamic tract 5. Ventral spinothalamic tract
|
The clinical presentation is most consistent with a central cord syndrome, which is believe to be caused by involvement of the lateral corticospinal tract. |
|
|
Which of the following clinical scenarios would be an indication for surgical intervention of the spine? 1. 18-year-old male with T12 burst fracture, stable alignment, and no neuro deficit. 2. 25-year-old male with trans-colonic gun shot wound and cord hemi-transection without retained bullet fragment. 3. 80-year-old female with global upper extremity weakness but preserved lower extremity function after fall. 4. 37-year-old male with type III odontoid fracture. 5. 18-year-old male with incomplete sensory and motor deficits after gun shot wound with retained bullet fragment in the lumbar spinal canal. |
Removal of retained bullet fragments within the spinal canal in a patient with incomplete sensory/motor deficits may improve patient function and therefore is recommended. ans5 |
|
|
what are the 6th indication for an anterior approach to the cervical spine? |
|
|
|
what is the name of the anterior tubercle of the transverse process of C6? |
carotid tubercle |
|
|
|
|
|

|
|
|
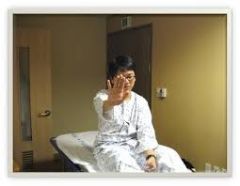
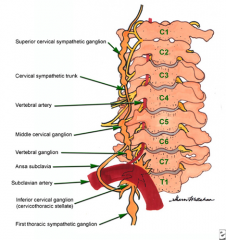
A myelopathic patient undergoes anterior cervical diskectomy and fusion through a left sided approach. Facial asymmetry is noticed postoperatively in the recovery room. A clinical photo is shown in Figure A. What additional finding would likely be found on physical exam? 1. Pupillary dilation and hyperhidrosis on the patient's right side 2. Pupillary dilation and hyperhidrosis on the patient's left side 3. Pupillary constriction and hyperhidrosis on the patient's right side 4. Pupillary constriction and anhidrosis on the patient's left side 5. Pupillary constriction and anhidrosis on the patient's right side |
Horner's syndrome is a rare but known complication of anterior approaches to the cervical spine. Horner’s Syndrome classically presents with 1. ipsilateral ptosis (drooping eyelid caused by injury to nerve to Muller’s muscle) 2. ipsilateral miosis (pupillary constriction caused by injury to long ciliary nerve to pupil dilator) and 3. usually (but not always) ipsilateral anhidrosis. Horner's Syndrome is caused by an injury to the cervical sympathetic ganglia/trunk, which are located anterolaterally to the longus colli and longus capitis muscles. These muscles lie anterolaterally to the cervical vertebral bodies.ans4 |
|
|
what is the joint reaction force of the ankle joint |
5 times body weight with walking on level surfaces |
|
|
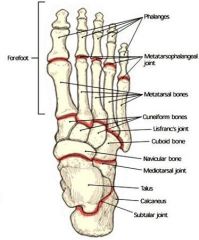
defined articulations of the subtalar jointN what motion takes place at the subtalar joint? |

this joint = talus plus calcaneous, the motion is only inversion/eversion there is no plantar flexion or dorsiflexion |
|
|
defined the articulations of the transverse tarsal joint AKA underlying underlying? |
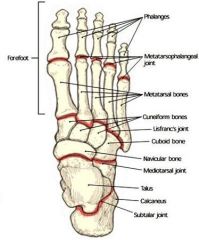
transverse tarsal joint = talonavicular ( medially)+calcaneal cuboid (laterally ) |
|
|
what adjustment to the joints in the foot make in order to have stable hindfoot and midfoot for toe off? |
there is inversion of the subtalar of the subtalar joints which locks the transverse tarsal joints AKA talonavicular and calcaneal cuboid |
|
|
what anatomic structure is the primary structure in the foot for load forced transfer between the hindfoot in the forefoot during stance? |
the plantar aponeuroses |
|
|
what is a MNeumonic for stance phase as it relates to gait cycle? |
I Like My Tea Pre-Sweetened, I Like My Teapot I – initial contact heel strike Like – Loading response My – M mid stance Tea – T terminal stance Pre- Previous swing Sweeten- Swing phase swing phase(In My Teapot ) I – initial swing or toe off M – mid swing T – terminal swing |
|
|
where is the bodies Center gravity? allergies a Center gravity affected during an adult male step? |
|
|
|
Which of the following best describes the relationship of the subtalar and transverse tarsal joints during the phases of gait? 1. Eversion of the subtalar joint locks the transverse tarsal joint 2. Transverse tarsal (Chopart) joint axes are parallel during heel strike 3. The calcaneus is in inversion throughout stance phase 4. Tibialis anterior concentrically contracts during stance phase 5. During push-off the foot becomes flexible due to eversion of the calcaneus |
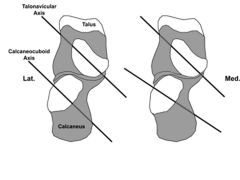
The transverse tarsal (Chopart) joints consist of the talonavicular and calcaneocuboid joints. The transverse tarsal axes are parallel during most of the heel strike phase when the subtalar joint is everted.Incorrect Answers: |
|
|
Which phase of gait is affected most in a patient with quadriceps atrophy? 1. Terminal swing 2. Preswing 3. Initial swing 4. Midstance 5. Midswing
|

Quadriceps weakness is most likely to affect the stance phase of the gait cycle, making midstance the correct answer. During the normal stance phase of gait, the quadriceps contracts to prevent buckling of the knee. In a patient with quadriceps atrophy, the patient leans forward at the hip causing the center of gravity to fall anterior to the knee. This causes the knee to go into hyperextension. In contrast, weakness of the hamstrings or the hip flexors are most likely to affect the swing phase of gait by limiting limb advancement.ans4 |
|
|
Which of the following descriptions of muscle activity during normal gait is correct? 1. Gastrocnemius-soleus contracts eccentrically during heel strike 2. Gastrocnemius-soleus contracts concentrically during heel strike 3. Gastrocnemius-soleus contracts concentrically during swing phase 4. Tibialis anterior contracts concentrically during toe-off 5. Tibialis anterior contracts eccentrically after heel strike |
One stride (heel strike to heel strike of one leg) of normal gait has been divided into the stance (62%) and swing (38%) phases. The stance phase is further divided into heel strike, foot flat, and toe off. Proper gait requires coordinated contraction of the leg muscles. The tibialis anterior (TA) muscle fires eccentrically at heel strike to lower the foot to the ground, while the gasto-soleus (GS) complex is dormant. The TA then relaxes, while the GS eccentrically contracts as the body’s weight is transferred forward over the foot during foot-flat. As the foot propels the body forward during toe-off, the GS contracts concentrically, while the TA remains dormant. As swing commences, the TA then fires concentrically producing dorsiflexion to clear the foot over the ground while the GS relaxes. Certain conditions like cerebral palsy result in improper firing of the muscles during the gait cycle, resulting in altered gait mechanics.ans5 |
|
|
|
|
|
The primary antagonist of the anterior tibial tendon is innervated by which of the following nerves? nerve roots 1. Superficial peroneal nerve 2. Deep peroneal nerve 3. Tibial nerve 4. Posterior tibial nerve 5. Sural nerve |
primary antagonist of the anterior tibial tendon is the peroneus longus, which is innervated by the -superficial peroneal nerve L5-S1. ans1 |
|
|
The primary antagonist of the posterior tibialis (PT) is innervated by which of the following nerves? nerve roots |
The peroneus brevis (PB) -superficial peroneal nerve L5-S1and posterior tibialis (PT) are antagonists to each other. |
|
|
The primary antagonist of the peroneus longus (PL) is innervated by which of the following nerves? nerve roots |
peroneus longus (PL) and tibialis anterior (TA)--deep peroneal nerve L4/L5 are antagonists to each other as the PL plantarflexes and everts, while the TA dorsiflexes and inverts the foot. |
|
|
The primary antagonist of the peroneus brevis (PB) is innervated by which of the following nerves? nerve roots |
The peroneus brevis (PB) and posterior tibialis (PT) tibial nerve L4/L5 are antagonists to each other. |
|
|
what type of collagen is found in the annulus fibrosis and the nucleus pulposus?characterize in terms of collagen amount glycan amount and physiologic function |
the annulus– type I collagen as obliquely oriented, high collagen low proteoglycan ratio high tensile strength to prevent intravertebral distraction the nucleus has type II collagenlow collagen high protein glycan ratio high compressibility "step 1 tense step 2 bounce" |
|
|
describe the blood supply that the intravertebral disc receive |
The disc is avascular nutrition reaches the nucleus pulposus. Diffusion from the endplates. |
|
|
at the intervertebral disc AGES is what happens pathologically
|
decreased (water & proteoglycan & pH) increase KaratIn suLfATE to CHONDROITIN sulfate ratio, lactate increase conversion to fibrocartilage, increase and degraded enzyme activity no change in the quantity of collagen |
|

A 37-year-old male feels a "pop" in his low back while lifting a heavy object. Four weeks later he continues to have significant low back pain, with no complaints of symptoms in his leg. A T2-weighted MRI is shown in Figure A with a red arrow identifying an abnormal finding in an anatomic structure. What type of collagen is primarily responsible for the biological properties of this anatomic structure? 1. Type I 2. Type II 3. Type V 4. Type IX 5. Type XI |
The clinical presentation is consistent with an annular tear. The annulus fibrosis is composed of primarily type I collagen. |
|
|
Recent studies have shown that cells of the intervertebral discs are biologically responsive and increase their production of matrix metalloproteinases, nitric oxide, interleukin-6, and prostaglandin E2 when stimulated by what molecule 1. osteoprotegerin (OPG) 2. interleukin-1 beta 3. transforming growth factor-beta 4. receptor activator of nuclear factor-kB ligand (RANKL) 5. parathyroid hormone (PTH) |
"cells of the intervertebral discs are biologically responsive and increase their production of matrix metalloproteinases, nitric oxide, interleukin-6, and prostaglandin E2 when stimulated by interleukin-1 beta. The effect is more dramatic in normal, nondegenerated discs where spontaneous synthesis of these mediators is low. Nevertheless, cells of the herniated degenerated discs where spontaneous production was high were still capable of further increasing their synthesis of several of these biochemical agents in response to interleukin-1 beta.Ans2 |
|
|
intervertebral discs are biologically responsive and increase their production of matrix metalloproteinases, nitric oxide, interleukin-6, and prostaglandin E2 when stimulated by what molecule? |
interleukin-1 beta |
|
|
Which of the following are progressive changes seen with aging of the intervertebral disc? 1. Increase in water content 2. Increase in large aggregated proteoglycans 3. An increased keratin sulfate to chondroitin sulfate ratio 4. A decrease in degradative enzyme activity 5. An increase in nutritional transport |
As aging occurs, increased degradative enzyme activity is seen in the intervertebral disk. |
|
|
with internal impingement what causes the BENNETT lesion
|
|
|
|
was the physical exam finding and the pitcher wrist pain and posterior shoulder is worse with throwing especially during the late cocking and early acceleration phase
|
decrease in internal rotation loss greater than 20°
|
|
|
The term internal impingement is used in throwers to describe a condition where the posterior-superior glenoid labrum impinges on which structure? 1. The anterior rotator cuff 2. The posterior rotator cuff 3. The anterior glenohumeral ligaments 4. The posterior glenohumeral ligaments 5. The biceps tendon |
Internal impingement is seen in throwers with the arm in a cocked position of abduction and external rotation. Often due to posterior soft tissue tightness, the posterior cuff impinges on the posterior superior labrum and is felt to contribute to SLAP tears and articular sided cuff tears. ans2 |
|
|
Internal impingement commonly occurs in overhead athletes and is very common amongst elite baseball pitchers. In which phase of throwing does this pathologic process occur? 1. Wind-up 2. Early cocking 3. Late cocking 4. Deceleration 5. Follow-through
|
Internal impingement refers to the impingement within the glenohumeral joint which occurs as the posterosuperior glenoid labrum makes contact with the greater tuberosity, causing impingement on the posterior rotator cuff. This occurs commonly among baseball pitchers during late cocking and early acceleration as the shoulder joint reaches it's maximum external rotation. |
|
|
the wound incapability of a bullet directly relates to what?_____ |
the amount Kinetic energy processes |
|
|
patient is a Vietnam veteran with a purple heart metal presents with anemia neurotoxicity emesis and abdominal colic what is the diagnosis? |
plumbism – lead intoxication |
|
|
what bullet velocity is considered low velocity causing Gustillo and ANDERSON type 1-2 wounds |
velocity < 2000 ft./s |
|
|
what bullet velocity is considered high velocity causing GUstillo and ANDERSON type III wounds most commonly associated injury with this kind bullet wound |
velocity > 2000 ft./s high risk for infection an compartment syndrome Because the high zone of injury and devitalized tissue |
|
|
what is the treatment for a low energy gunshot wound? |
low energy gunshot wound treatment – local wound care – tetanus – short course of antibiotics primary closure of the wound is contraindicated |
|
|
what his treatment for high energy gunshot wound? |
high-energy – ORIF versus ex-fix tetanus and short course of antibiotics |
|
|
what is the treatment of a gunshot wound that is intra-articular? |
arthrotomy with removal of the missile because it can lead to plumbism arthritis and local inflammation |
|
|
what is the treatment of a gunshot wound to the femur low energy? |
low energy femur and gunshot wound – IM nailing |
|
|
what is the treatment gunshot wound to the femur high-energy? |
high-energy femur gunshot wound – ex-fixator |
|
|
with the treatment gunshot wound to the spine with associated perforated viscus? |
bullets the spine and viscus – do not remove the bullet broad-spectrum IV antibiotics for 7-14 days |
|
|
gunshot wound to the spine with an incomplete motor deficit that is a brown Séquardsyndrome what is the treatment |
bullet causing Brown-Séquard syndrome treatment is surgical decompression and bullet fragment removal if the bullet fragments are Near the neurologic level that is being affected |
|
|
A 21-year-old male presents to the emergency department after sustaining a gun shot wound to his abdomen. Subsequent radiographs reveal a bullet in the L2 vertebral body. Physical exam shows no neurologic deficits. He undergoes emergent laparotomy and is found to have a small bowel laceration. What would be the preferred treatment following his exploratory laparotomy and small bowel repair? 1. Intravenous antibiotic coverage for Gram negative bacteria for 7 days 2. Surgical decompression and bullet fragment removal 3. Observation 4. Broad-spectrum oral antibiotic coverage for 7 days 5. Broad-spectrum intravenous antibiotic coverage for 7 days
|
The clinical presentation is consistent with a GSW with bowel perforation and a retained bullet in the vertebral body. Because the patient is neurologically intact broad-spectrum intravenous antibiotic coverage for 7 days is the most appropriate treatment. ans5 |
|
|
A 24-year-old man who sustained a gunshot wound to the abdomen ten hours earlier was brought to the emergency department. On physical examination he was found to have 4 of 5 weakness in his bilateral lower extremities. Radiographs are shown in Figure A. Computed tomography of the lumbar spine showed retained missile in the vertebral body and paraspinal soft tissues, but not within the spinal canal. His FAST was positive and he underwent an emergent exploratory laparotomy where an injury to the cecum was identified and treated. Management should now include which of the following? 1. Bullet fragment removal from a transabdominal approach 2. Bullet fragment removal from a retroperitoneal approach 3. Broad-spectrum oral antibiotics for 3-5 days 4. Broad-spectrum intravenous antibiotics for 7-14 days 5. IV methylprednisolone at 5.4mg/kg/h for 48 hours
|
The patient in the scenario has a GSW to the lumbar spine with neurologic deficits but without a retained missile in the spinal canal. In patients with visceral injury, the treatment is broad-spectrum antibiotic coverage for 7 days. |
|
|
what type of immunologic response is type I anaphylactic reaction |
type I his IgE mediated by mask cells and basal cells associated with an allergy |
|
|
what type of immunologic response is a type II anybody dependent hypersensitivity reaction mediated by? |
type 2 antibody dependent hypersensitivity mediated by IgG and IgM antibodies |
|
|
what type of immunologic responses type III immune complex deposition hypersensitivity reaction |
mediated by IgG and IgM antibodies |
|
|
what type of immunologic response is metallic orthopedic implants and mediated by what types of cells? |
type 4 delayed type hypersensitivity reaction similar to tuberculosis skin test |
|
|
which antibody is the most comment immunoglobulin in the body |
most common IgG |
|
|
which immunoglobulin is the 1st type of antibiotic to appearafter exposure to an antigen |
IgM |
|
|
which class of any body is found and external secretions |
IgA IgA IgA |
|
|
which class of antibody confers protection against parasites and allergic reactions |
IgE |
|
|
What is the first class of antibody to appear in serum after exposure to a foreign antigen? 1. IgA 2. IgD 3. IgE 4. IgG 5. IgM
|
IgM is the first class of antibody to appear in our serum after exposure to an antigen. IgG is the most abundant immunoglobulin in our body. IgA is the major class of antibody in external secretions such as intestinal mucus, bronchial mucus, saliva, and tears. IgE is important in conferring protection against parasites and is also increased in allergic reactions.ans5 |
|
|
The acquired immune response mediated by the interaction between the T cell receptor and major histocompatibility complex requires which of the following first steps? 1. Antigen phagocytosis by T cells 2. Antigen processing and presentation to T cells 3. Antigen recognition by natural killer T cells 4. Antigen proliferation by polymerase chain reaction 5. T cell disulfide bond cleavage and enzymatic processing
|
The process of antigen processing and presentation is the first step of the acquired immune response. This is performed by the so called antigen presentation cells (APC) of which B cells and dentritic cells are two examples. The APC breaks down the protein antigen in a multitude of enzymatic reactions and presents key peptide sequences via the major histocompatibility complex (MHC) receptors. Once presented on the surface of the APC, the T-cell receptor recognizes the MHC/antigen complex leading to T-cell activation. At no point in this process are antigens phagocytosed by T cells.ans2 |
|
|
A type IV (delayed-type hypersensitivity reaction) can be seen in which of the following scenarios? 1. Packed red blood cell transfusion 2. Platelet transfusion 3. Immune inert scaffold placement 4. Metal plate and screw placement for fracture 5. Red man syndrome from vancomycin administration |
A type IV, or delayed-type hypersensitivity reaction, can be seen with placement of orthopedic hardware. Type IV hypersensitivity is often called delayed type hypersensitivity as the reaction takes two to three days to develop. Unlike the other types, it is not antibody mediated but rather is a type of cell-mediated response.ans4 |
|
|
pediatric patient less than 3 presents with intoeing what to other 2 conditions must be ruled out |
DDH and metatarsus adductus |
|
|
what 3 physical exam test can be used to assess tibial torsion as a child, what is considered normal |
|
|
|
A 2-year-old boy is brought to your clinic by his mother for being "pigeon-toed". Each of the following measurements found on physical examination are a routine part of defining the child's lower extremity rotational profile EXCEPT. 1. thigh-foot axis 2. transmalleolar axis 3. measurement of the Q angle 4. heel-bisector angle 5. foot progression angle |
"active treatment of childhood rotational disorders is unnecessary in most cases. Prudent care consists of reassurance and education about the natural history of the condition". The correct answer is Figure C which demonstrates the measurement of the Q angle. The Q angle can be affected by femoral anteversion and tibial torsion, but typically is not a part of the rotational profile. The 5 components of Staheli's rotational profile include internal and external hip rotation (shown in Illustration A), thigh-foot axis (Figure A), transmalleolar axis (Figure B), heel-bisector angle (Figure D), and foot progression angle (Figure E). Normal values for clinical measurements are: foot progression angle -5 to 20 degrees, IR and ER up to 70 degrees, thigh-foot axis between -10 to 20 degrees, transmalleolar axis -4 at birth to 23 degrees at maturity, and the heel-bisector line normally passes through the second web space.ans3 |
|

|
MRSA MUPIROCIN |
|

what the diagnosis with the treatment |
|
|

what the diagnosis was a treatment |
fungal infection tinia pedis topical antifungals topical antifungals |
|

what the diagnosis with the treatment |
acne mechanic, AKA folliculitis, name athlete to wear protective padding observe for keratolytics
|
|

what is the diagnosis what is the treatment what is the cause |
impetigo, topical BACTROBAN or ERYTHROMYCIN patient sports most common organism include Streptococcus pyogenes staph aureus |
|
|
patient has splenomegaly malaise nausea headache pharyngitis What is the diagnosis what is the cause what is the treatment wwith the most common complication |
the diagnosis is mononucleosis it causes Epstein-Barr virus the treatment is no contact sports for 3-5 weeks until splenomegaly completely resolves Splenic rupture within the 1st 3 weeks.equal DEATH |
|
|
A 75-year-old man is brought to the ER after a fall. He complains of right leg pain, and a radiograph is shown in Figure A. Prior to operative fixation of the fracture, biopsy and staging procedures reveal that this is a metastatic lesion. Which of the following primary cancer diagnoses is associated with the shortest life expectancy following pathologic fracture? 1. Lung 2. Thyroid 3. Prostate 4. Breast 5. Renal
|
This patient is presenting with a pathologic fracture of the proximal tibia. Prior to definitive fixation, the nature of the tumor needs to be determined through biopsy and staging to assist with operative planning. In terms of life expectency, lung cancer and melanoma have the worst median survival (<6 months) and 5 year survival (<5%) when bone metastases are present. ans1 |
|
|
An elderly female has just been diagnosed with lung cancer. If her cancer metastasizes to bone, what is the most common site of subsequent pathologic fracture? 1. Proximal femur 2. Distal femur 3. Proximal humerus 4. Humeral shaft 5. Thoracic spine
|
While the spine is the most common site for all boney metastasis, the proximal femur is the most common site for pathologic fracture secondary to metastasis to bone. ans1 |