![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
69 Cards in this Set
- Front
- Back

Pt presents with creamy, white, curd-like patches over erythematous mucosa. The rub off the mucosa easily. What is your Dx and how do you Tx? |
Dx: Oral Candidiasis aka Thrush Tx: Antifungals (azoles), improve hygiene, rinse with chlorhexidine or 50/50 H2O2 + H2O |
|

Why might a Pt have this Dz? |
|
|

What is this and what is it called? |
Variation of Candidiasis - Erythematous Form (angular chelitis of the mouth) |
|

What is this a Sx of? |
Erythematous Form of Candidiasis |
|

What Dx tests will you run on this Pt? |
|
|

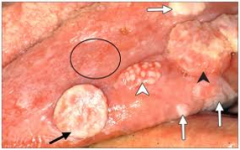
What is this and what is it called? |
Leukoplakia: premalignant, hyperkeratotic, white patch/plaque (doesn't rub off) |
|

What is this and what is it called? |
Erythroplakia: premalignant, hyperkeratotic, erythematous patch/plaque (doesn't rub off) |
|

Pt presents with these lesions in mouth that have been there for 3 weeks. Pt is a pack a day smoker. What is your next step and what is at the top of your Diff Dx? |
Leukoplakia that may lead to Oral SCC Refer to Dentist, Oral Surgeon, ENT for biopsy |
|
What is this and what is it called? |
Squamous Cell Carcinoma of the mouth: malignant neoplasm of the stratified squamous epithelium that is capable of local, invasive destruction and distant metastasis. |
|
|
What statistics surround Oral SCC? |
|
|

Who is at risk for this? |
People who smoke tobacco (nicotine is carcinogenic) and people who drink alcohol. |
|

What is the Px and Tx for this Pt? |
SCC lesions <4 mm have a low metastasis rate SCC lesions <2 cm can be resected surgically |
|
|
What is a good oral exam necessary? |
To catch lesions before they become malignant |
|

What is this and what is it called? |
Aphthous Ulcer or Ulcerative Stomatits |
|
|
What are the 3 different types of Stomatitis and how are they differentiated? |
|
|

Pt comes in with a yellow/grey, painful ulcer with a white fibrinoid center with a red halo around it. What is it called? |
Aphthous Stomatitis |
|

What is this Pt's Px? |
Minor Stomatitis - heal in 10-14 days without a scar |
|

What is this Pt's Px? |
Major Stomatitis - heal in 14+ days and will leave a scar |
|
|
Pt presents with oral ulcers, Hx of fever, burning sensation in mouth, and vesicles that have ruptured and scabbed over. What is the Dx and why? |
Herpetic Stomatitis: Vesicles, scabbed ulcers, Hx of fever & burning sensation are all Dx criteria for HSV infxn. |
|

How would you Tx this Pt? |
Antiviral meds and education about infxn and what triggers outbreaks (stress, other infxn or reduced immune response) |
|

What causes this? |
HSV 1 infxn |
|

How is this Pt different than someone with oral vesicular ulcers? |
Pt still has an HSV 1 infxn but it has manifested on the vermillion border of the lip - called Herpes Labialis |
|

Pt presents with sore, inflamed, scratchy throat. What is the likely Dx? |
Pharyngitis |
|

What can cause this? |
|
|
|
Pt presents with: Fever > 38 C Tender anterior cervical adenopathy Pharyngotonsillar exudate NO Cough Dx and why? |
Group A Beta-hemolytic Strep The 4 Sxs are the Centor Criteria |
|
|
Pt presents with red, sandpaper like rash over entire body and has Hx of GABHS in the past week. What is the Dx and what is the complication? |
Scarlatina Rash Rheumatic Heart Dz |
|

What is the most likely Dx for this Pt? |
GABHS |
|
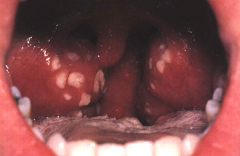
Pt presents with Fever, halitosis, Cervical LAD, Odynophagia and pharyngeal exam reveals this. What is the most likely Dx? |
Tonisillitis |
|

Pt presents with tonisilitis. What do you need to do and why? |
Perform a throat culture to r/in or r/o GABHS or Mononucleosis. |
|
|
Labs come back and confirm a Dx of GABHS what is the Tx? |
Abx: Penicillin, Erythomycin, or Macrolides |
|
|
How does the Centor Criteria work? |
Rating scale on four criteria: fever > 38 C, anterior cervical adenopathy, no cough, tonsillar exudate. If Pt has 1 Sx - no lab & no tx. If Pt has 2-3 Sxs run a lab and tx. If Pt has 4 Sxs no need to run a lab - just tx. |
|

Pt presents with Hx of exhaustion, marked cervical LAD, tonsils w/exudate that is hairy appearing. What is at the top of your Diff Dx list and what is your next step? |
Mononucleosis caused by Eppstein Barr virus. Run a monospot EBV titer. Although may only give positive result after 2-6 wks of infxn |
|
|
What Abx is contraindicated in Mono infxn and why? |
Penicillin - it causes a rash |
|

What is this and what is it called? |
Peritonsillar Abscess "Quinsy": Infection that invades tonsillar capsule and surrounding tissue, usually preceded by cellulitis |
|
|
Pt presents w/severe sore throat, odynophagia, trismus, medial deviation of soft palate and uvula, "hot potato" voice. What is the most likely Dx and what is the best Tx/management? |
Dx: Peritonsillar abscess/quinsy Tx: Abx (parenteral if can't swallow oral), I&D (oral surgeon), Tonsillectomy, analgesics for pain, NSAIDs, salt water gargles |
|

What is this Pt at risk for? |
Airway obstruction & aspiration pneumonia |
|
|
Pt presents complaining of local swelling of the face, pain, tenderness, erythema on buccal mucosa. What is the most likely Dx and how do you Tx? |
Sialadenitis
|
|

What may have caused this? |
Sialadenitis
|
|
|
How is hoarseness different from stridor? |
Hoarseness: abnormal vibration of the vocal cords that results in a breathy/raspy voice Stridor: high pitched whistle on inspiration due to turburlent airflow through narrow/obstructed airway |
|
|
What causes laryngitis? |
|
|
|
What is the most common cause of hoarseness? |
Laryngitis
|
|
|
When should you refer a Pt with stridor? |
ALWAYS and when there is a rapid onset it should be an EMERGENT referral |
|
|
Stridor is inspiratory when? |
the narrowing is above the vocal cords |
|
|
Stridor is expiratory when? |
the narrowing is below the vocal cords |
|
|
What are the Tx possibilities for a Pt with Laryngitis? |
|
|
|
Pt is a 26 yo female and presents with a SHx that indicates she is a professional singer. She has had hoarseness for 3 weeks. What is the most likely Dx & Tx? |

Dx: Vocal Cord Nodules Tx: refer to specialist for voice modification/speech therapy & surgical removal |
|
|
Complications of Vocal Cord trauma include: |
|
|
|
Pt presents w/ dysphonia, hoarseness, odynophagia, otalgia. SHx reveals Pt does not smoke but PMHx indicates HSV 16 infxn. What is the most likely Dx and how would you confirm? |
Early stage Laryngeal Cancer - SCC Refer to Otolaryngology for biopsy, CT/MRI, and labs |
|
|
Pt presents w/hoarsness for 3 wks, no PMHx of URI, SHx reveals Pt is a smoker. What is at the top of your Diff Dx list and why? |
Laryngeal SCC Smokers are at the greatest risk |
|

Pt presents w/dysphonia, weight loss, otalgia, LAD, stridor. Laryngoscopy reveals this. Dx & Tx? |
Dx: Later stage Laryngeal SCC Tx: refer to Oncology/Otolaryngology who will attempt to cure, preserve swallowing fxn, preserve useful voice, avoid permanent tracheostomy |
|
|
A Pt comes in for a routine HEENT exam. When you examine the mouth you should also examine what? How? |
Teeth Shape, alignment, defects, mobility, color, plaque, sensitivity to percussion |
|
|
Pt presents with obvious evidence of dental caries. How will you educate them? |
Educate Pt on prevention of oral Dz by:
|
|

During your oral exam, you discover pale, yellow, sticky deposits on the teeth. What do you tell your Pt and how do you educate them? |
Pt has dental plaque Education:
|
|
|
Bacteria metabolize sugar into acidic products that breakdown tooth enamel resulting in |

Dental Caries |
|
|
Saliva and Fluoride do what for teeth? |
Saliva has antimicrobial properties Fluoride helps remineralize teeth |
|
|
How do Dental Caries progress? |
Initial - involves enamel only and asymptomatic Moderate - dentin invaded and Sxs include hot/cold/sweet sensitivity & pain with chewing/percussion Severe - pulp involved and pain is severe and persisitent |
|

Pt's oral exam reveals this. Pt complains that gums bleed during flossing and that they are tender. Dx? |
Gingivitis (reversible with improved oral hygiene) |
|
|
Plaque buildup, infxn, hormonal changes, oral FB may all be causes of |

Gingivitis |
|

This Pt has poor oral hygiene and that has caused the periodontal dz. Correct or Incorrect & why? |
Incorrect - Pt has Necrotizing Gingivitis which is a local infxn and not related to oral hygiene |
|

This Pt has a fever, LAD, halitosis, and oral exam reveals this. What is the Dx and what is the Tx? |
Dx: Necrotizing Gingivitis Tx: Oral Penicillin TID 10d + warm half-strength peroxide rinse |
|
|
A group of microorganism-induced inflammatory dzs that lead to the destruction of the supporting stxs of the teeth: alveolar bone, periodontal ligament, adjacent soft tissues |
Periodontal Dz |
|
|
Periodontal dz starts with Gingivitis and then progresses to |
Periodontitis |
|
|
Gingival, Periodontal, Periapical are the 3 types of |
Dental Abscess |
|

What is this and what is it called? |
Gingival Abscess: Injury/Infxn of surface of the gum |
|

What is this and what is it called? |
Periodontal Abscess: Infxn deeper in the gum |
|

What is this and what is it called? |
Periapical Abscess: Infxn of the pulp |
|
|
Gingival & Periodontal Abscess will present with |
|
|
|
Periapical Abscess will present with |
|
|
|
You suspect a dental abscess in your Pt. What do you do next? |
Refer to a dentist for:
|