![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
66 Cards in this Set
- Front
- Back
|
the immittance battery of tests |
1. is sensitive in detecting middle ear disorder 2. can be helpful as a cross-check to pure-tone audiometry 3. can be useful in differentiating cochlear from retrocochlear disorder |
|
|
impedance vs. admittance vs. immittance |
immittance is the accepted clinical term that encompases both |
|
|
immittance |
total opposition to the flow of energy through a vibrating system and total energy flow through a vibrating system |
|
|
immittance test battery |
1. tympanometry 2. static immittance 3. acoustic thresholds |
|
|
3 parts of probe tip |
1. air pump (changes pressure in space between probe tip and ear drum) 2. speaker (transmits sound into ear canal space) 3. microphone (picks up sound generated) |
|
|
when probe tip pump is set at atmospheric pressure |
eardrum behaves normally, most flexible, most sound absorbed |
|
|
when probe tip set at high pressure |
forces ear drum inwards, increases rigidity, more sound reflected back to probe tip |
|
|
when probe tip set at low pressure |
forces ear drum outwards, increases rigidity, more sound reflected back to probe tip |
|
|
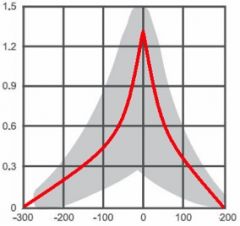
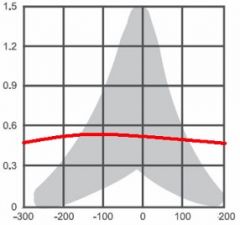
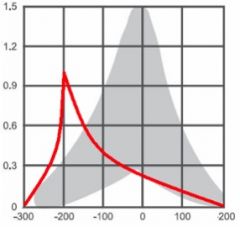
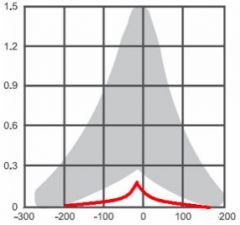
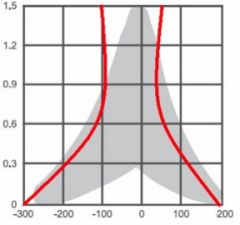
tympanogram horizontal axis |
pressure changes- from -300 through 0 (atmospheric) to +200, in decaPascals (daPa) |
|
|
tympanogram vertical avis |
amount of sound absorbed (admitted) by the eardrum; mhos |
|
|
mho |
opposite of ohm, quantified admittance to the flow of energy |
|
|
Type A- normal ear, no air-bone gap expected |
|
|
Type B- eardrum inflexible, fluid in middle ear; generally otitis media with effusion |
|
|
Type C- negative pressure point, consistant with eustachian tube malfunction; may signal oncoming or healing ear infection |
|
|
Type AS- normal middle ear pressure but inflexible; otosclerosis or cholesteatoma |
|
|
Type AD- no pressure point, signals ossicular disarticulation |
|
|
acoustic reflex |
when a sound is of sufficient intensity, it will elicit a reflex of the middle-ear musculature; primarily of the stapedius muscle -activated in both ears even if only stimulated in one -tests CONDUCTIVE component, will be normal if only sensorineural damage |
|
|
normal range of acoustic reflex |
70dB-100dB |
|
|
functions of acoustic reflex |
may be inner ear protection- we don't really know |
|
|
acoustic reflex arc |
stimulus noise->cochlea->8th nerve->brain stem->7th nerve->back to BOTH ears and stapedius muscles |
|
|
nomenclature for acoustic reflexes |
right/left ipsilateral (uncrossed) right/left contralateral (crossed) |
|
|
the acoustic reflex is defined by |
the stimulated ear |
|
|
acoustic reflex if sensorineural hearing loss |
will still be normal |
|
|
fluid in ear- effect on acoustic reflex |
obscures |
|
|
acoustic reflex if conductive component in one ear (ex. right ear) |
-right ear ipsilateral and right and left ear contralateral acoustic reflex will be absent -left ear ipsilateral acoustic reflex will be normal |
|
|
acoustic component if conductive problems in both ears |
absent |
|
|
if normal tympanogram but absent acoustic reflex |
check which pathways are involved- may be facial nerve weakness on one side |
|
|
if normal tympanogram but absent contralateral acoustic reflexes |
consistent with brainstem lesion |
|
|
acoustic reflex decay |
normal for reflex to maintain strength for 10 seconds; if decays before, may be 8th nerve lesions |
|
|
optimal listening intensity |
1000 and 2000 Hz (?) |
|
|
four major applications of auditory evoked potential measurement |
1. infant hearing screening (most important) 2. prediction of hearing sensitivity 3. diagnostic assessment of central auditory nervous system function 4. monitoring auditory nervous system function during surgery |
|
|
equiptment for auditory evoked potentials |
1. differential amplifier 2. bandpass filter 3. signal averaging (summing) computer |
|
|
auditory evoked potential |
small electrical voltage potentials evoked by sound |
|
|
differential amplifier |
rejects electrical activity recorded at two different electrodes when the electrical impulses are identical (leaving the AEP)- called common mode rejection |
|
|
bandpass filter |
auditory evoked potential frequencies are restricted to a vary narrow band; bandpass filtering cuts out extreme high and low frequencies not ordinarily expected to fall in the range of the AEP |
|
|
signal averaging (summing) computer |
extracts the time-locked auditory evoked potential from the random EEG noise; several thousand stimuli (clicks) presented, electrical activity summed towards zero so eventually AEP is left |
|
|
auditory brainstem response (ABR) |
most commonly used evoked potential, occurs within the first 10 msec following signal onset ("time-locked") |
|
|
electrocochleography |
putting probe (surgically) near cochlea, monitor 8th nerve during surgery, records 3 electrical potentials |
|
|
3 electrical potentials recorded by electrocochleography |
1. summating potential (builds and sparks AP) 2. cochlear microphonic 3. action potential (wave I of ABR) |
|
|
source of cochlear microphonic believed to be |
hair cells |
|
|
source of ABR waves |
uncertain but come from brainstem |
|
|
why ABR is useful |
-can be recorded from surface electrodes -waves robust -patient can be asleep etc. -repeatable |
|
|
ABR- wave latencies vs. wave amplitudes |
wave latencies (delays between waves) stable across patients, amplitudes far less stable |
|
|
wave V of ABR |
most robust wave in ABR; latency increases as auditory stimulus decreases; amplitude decreases as stimulus intensity decreases -used to estimate hearing threshold for difficult-to-test adult -may be low for infants (only test high/low), become robust for everyone ~18 months |
|
|
why ABR is tested binaurally |
faster, speeds up infant screening |
|
|
cortical radiations and auditory cortex radiations |
less clinical utility due to variability of AEPs across subjects, more for research than clinical |
|
|
presumed anatomical source of AEPs |
late latency response- auditory cortex middle latency response- medial geniculate body (?) auditory brainstem response (ABR)- brainstem |
|
|
late latency responses are |
less reliable; ABR more reliable |
|
|
auditory steady-state response (ASSR) |
the auditory evoked potential, elicited with modulated tones that can be used to predict hearing sensitivity in patients of all ages -elicited by a tone; ASSR follows modulation rate of the stimulus |
|
|
otoacoustic emissions |
-backwards emitted wave -cochlear echoes -related to tinnitus -outer hair cells presumed source- noise changes shape, shape changing causes vibrations on basilar membrane, vibrations emanate backwards through system- so need healthy ear to get them |
|
|
2 classes of OAEs |
-spontaneous OAEs- when not stimulated, in 50% of people with hearing WNL, absent when not normal; not linked to tinnitus -evoked OAEs- need stimulus- Transient Evoked OAEs and Distortion Product OAEs |
|
|
Transient Evoked OAEs |
click-evoked |
|
|
Distortion Product OAEs |
two-tone stimulus, cochlea generates another tone "of its own", called distortion product |
|
|
clinical applications for OAEs |
1. infant screening 2. pediatric assessment 3. cochlear function monitoring 4. certain diagnostic cases -doesn't measure degree of hearing loss accurately, but whether there is loss or not; helps determine diagnosis |
|
|
electronystagmography (ENG) |
vestibular assessment -nystagmus (eye movements), etc. |
|
|
using audiologic knowledge- what to ask/tell patient |
don't tell them how they hear, ask how it affects them (communication etc.) |
|
|
elements of a report |
-case history -otoscopic inspection -immittance -the audiogram: type of hearing loss, degree of hearing loss, configuration of hearing loss, symmetry of hearing loss -speech audiometry -recommendations (follow-up etc.) |
|
|
identify need for intervention |
-degree/type of hearing loss, audiogram morphology, degree of handicap, patient motivation |
|
|
process of getting hearing aid |
-assessment (audiological and medical) -earmold impressions -hearing aid assessment -follow-ups |
|
|
questions to be anwered by the audiological assessment for a hearing aid |
-auditory needs- hearing loss -treatment needs- why seeking hearing aid, motivation, patient's physical and psychological status, etc. |
|
|
determining treatment needs |
-self-assessment scales -loudness discomfort data |
|
|
factors affecting negative prognosis |
-patient doesn't perceive a problem -not enough or too much hearing loss -"difficult" hearing loss -very poor speech recognition -disease in middle ear |
|
|
amplification strategies/options |
-type of amplification system (hearing aid, implant, etc.) -which ear (monaural vs. binaural, better or worse) -device style |
|
|
binaural advantage of hearing aids |
-loudness enhancement -improved spatial hearing (localization) -balanced hearing |
|
|
hearing aid fitting approaches |
-estimating amplification targets (soft, moderate, and loud sounds) -ensure that soft sounds audible, loudness discomfort level not exceeded -get patient input |
|
|
when hearing aid arrives |
check to make sure it's working |