Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
168 Cards in this Set
- Front
- Back
|
Provide the normal gas values (including pH).
|
pH: 7.35-7.45
Drop the 7 pCO2: 35-45 Multiply 45 x 2 pO2>90 Divide 45 by 2 HCO3 = 22 (up to 28) |
|
|
What is the Henderson-Hasselbalch equation?
|
pH=HCO3/pCO2
|
|
|
Acid-Base Disorder:
pH 7.40 HCO3 23 pCO2 40 |
pH nl
HCO3 nl pCO2 nl Normal ABG |
|
|
Acid-Base Disorder:
pH 7.50 HCO3 35 pCO2 42 |
pH Basic (Alkalosis)
HCO3 Elevated (Must be metabolic) pCO2 Normal (No compensation) Thus, it's a metabolic alkalosis without compensation. |
|
|
Acid-Base Disorder:
pH 7.33 HCO3 13 pCO2 28 |
pH: Acidic
HCO3: Low pCO2: Low--must be compensatory mechanism because don't have an alkalosis Metabolic acidosis with respiratory compensation. |
|
|
Acid-Base Disorder:
pH 7.42 HCO3 32 pCO2 64 |
pH Normal
HCO3 High--metabolic alkalosis pCO2 High--respiratory acidosis Mixed disorder; combined metabolic alkalosis and respiratory acidosis |
|
|
Acid-Base Disorder:
pH 7.20 HCO3 18 pCO2 40 |
pH Low--Acidosis
HCO3 Low pCO2 Low Metabolic acidosis without compensation. (normal pCO2 is 35-45) |
|
|
Acid-Base Disorder:
pH 7.20 HCO3 24 pCO2 54 |
pH: Acidosis
HCO3: Normal pCO2: Elevated Respiratory acidosis without compensation. |
|
|
Acid-Base Disorder:
pH 7.52 HCO3 22 pCO2 22 |
pH: Alkalosis
HCO3: Normal pCO2: Low Respiratory alkalosis without compensation. |
|
|
Acid-Base Disorder:
pH 7.66 HCO3 36 pCO2 30 |
pH: Alkalosis
HCO3: Elevated pCO2: Normal/Low Combined metabolic and respiratory alkalosis. |
|
|
Acid-Base Disorder:
pH 7.47 HCO3 14 pCO2 22 |
pH Alkalosis
HCO3 Low pCO2 Low Respiratory alkalosis with compensation. |
|
|
Acid-Base Disorder:
pH 7.46 HCO3 35 pCO2 53 |
pH Alkalosis
HCO3 Elevated pCO2 Elevated Metabolic alkalosis with compensation |
|
|
Acid-Base Disorder:
pH 7.39 HCO3 12 pCO2 22 |
pH Normal
HCO3 Low--Met acidosis pCO2 Low--Resp alkalosis Mixed: Metabolic acidosis and respiratory alkalosis |
|
|
Acid-Base Disorder:
pH 7.34 HCO3 31 pCO2 62 |
pH Acidosis
HCO3 Elevated pCO2 Elevated--acidosis Respiratory acidosis with compensation |
|
|
Acid-Base Disorder:
pH 7.10 HCO3 15 pCO2 50 |
pH Acidosis
HCO3 Low--acidosis pCO2 High--acidosis Combined metabolic and respiratory acidosis. |
|
|
Respiratory acidosis vs alkalosis:
Causes |
Resp acidosis:
Hypoventilation: -Airway obstruction -Lung dz -Opioids, narcotics, sedatives -Weakening of respiratory mm Resp alkalosis: -Hyperventilation (early high altitude exposure) -ASA ingestion (early) |
|
|
Metabolic acidosis vs alkalosis:
Causes |
Met acidosis:
CHECK ANION GAP (Na+ - (Cl + HCO3); nl range is 8-12 If normal gap****: Diarrhea Glue sniffing Renal tubular acidosis Hyperchloremia If anion gap: MUDPILES***** Methanol Uremia DKA Paraldehyde/Phenformin Iron tablets or INH Lactic acidosis Ethylene glycol Salicylates Met alkalosis: Diuretic use Vomiting Antacid use Hyperaldosteronism |
|
|
Rental tubular acidosis:
Type I vs Type II vs Type IV |
Type I (distal)-Defect in CD's ability to excrete H+. Assocd w/hypokalemia and risk for Ca2+ kidney stones
Type II: Proximal; defect in proximal tubule HCO3- reabsorption. Assocd w/hypokalemia and hypophophatemic rickets. Type IV: Hyperkalemia; hypoaldosteronism or lack of CD response to aldosterone; assocd w/hyperkalemia, inhibition of ammonium excretion in proximal tubule. Leads to acidic urine due to dec'd buffering capacity. |
|
|
How does acidosis/alkalosis affect extracellular K concentrations?
|
Because of H+/K+ pump:
Acidosis: increases extracell K+ Alkalosis: decreases extracell K+ |
|
|
A patient with recent kidney transplant on cyclosporin for immunosuppression requires an antifungal agent for candidiasis
What drug would result in cyclosporin toxicity? |
Ketoconazole (interferes with cyp450)
|
|
|
A patient presents with renal insufficiency
What alterations need to be made in his doses of digoxin and digitoxin respectively? |
Digoxin is renally excreted, so decrease dose.
Digitoxin not renally excreted, so don't have to change dose. |
|
|
What effect will a renal stone that obstructs the ureter have on GFR and FF?
|
Dec GFR
Dec FF |
|
|
What is the maximal serum glucose concentration at which glucose can be absorbed in the tubules?
|
Will start to spill glucose around 200 mg/dL, but will saturate at 350 mg/dL
|
|
|
What change in a basic metabolic panel might you expect in a young pt being treated for status asthmaticus?
|
beta-agonists will shift K+ into cells-->hypokalemia
|
|
|
MUD PILES
|
Methanol
Uremia DKA Paraldehyde or phenformin Iron tablets or INH Lactic acidosis Ethylene glycol Salicylates |
|
|
A patient taking lisinopril complains of new onset, constant coughing
What medication class should this patient be switched to? |
Angiotensin receptor blocker (sartan)
|
|
|
A patient with heart failure exacerbation needs medical diuresis but has a sulfa allergy
What diuretic can be used? |
Loop & thiazide are both sulfa drugs, so use Ethacrynic acid
|
|
|
A patient presents with hypertension, hypokalemia, metabolic alkalosis, and low plasma renin.
What is the diagnosis, and how do you treat it? |
Primary hyperaldosteronism
Treat w/spironolactone |
|
|
Type of diuretic:
Triamterene |
K+ sparing
|
|
|
Type of diuretic:
Acetazolamide |
Carbonic anyhydrase inhibitor
|
|
|
Type of diuretic:
Hydrochlorothiazide |
Thiazide
|
|
|
Type of diuretic:
Bumetanide |
Loop
|
|
|
Type of diuretic:
Spironolactone |
K+ Sparine--aldost antag
|
|
|
Type of diuretic:
Chlorothiazide |
Thiazide
|
|
|
Type of diuretic:
Ethacrynic acid |
Loop, not a sulfa drug
|
|
|
Type of diuretic:
Mannitol |
Osmotic
|
|
|
Type of diuretic:
Metolazone |
Thiazide
|
|
|
Type of diuretic:
Chlorthalidone |
Thiazide
|
|
|
Type of diuretic:
Furosemide |
Loop
|
|
|
Type of diuretic:
Amiloride |
K+ sparing
|
|
|
Type of diuretic:
Torsemide |
Loop
|
|
|
Appropriate diuretic:
Acute pulmonary edema |
Heart failure-->LMNOP
Loop |
|
|
Appropriate diuretic:
Idiopathic hypercalciuria |
Thiazide to retain Ca2+
|
|
|
Appropriate diuretic:
Glaucoma |
Acetazolamide, Mannitol
|
|
|
Appropriate diuretic:
Mild to moderate CHF with expanded ECV |
Mild: Thiazide
Classically for HF: Loop |
|
|
Appropriate diuretic:
In conjunction with loop or thiazide diuretics to retain K+ |
Any K+ sparing diuretic
|
|
|
Appropriate diuretic:
Edema a/w nephrotic syndrome |
Loop
|
|
|
Appropriate diuretic:
Increased intracranial pressure |
Mannitol
|
|
|
Appropriate diuretic:
Mild to moderate hypertension |
Thiazide--HCTZ
|
|
|
Appropriate diuretic:
Hypercalcemia |
Loop to lose Ca2+
|
|
|
Appropriate diuretic:
Altitude sickness |
Acetazolamide
|
|
|
Appropriate diuretic:
Hyperaldosteronism |
Spironolactone or eplerenone
|
|
|
What is the equation for the renal clearance of any substance?
|
Renal clearance = UxV/Px
|
|
|
A 40 year-old pt of yours weighs 100 kg.
What is her estimated plasma volume? |
20% x 100 kg x 1/4 L/kg = 5L
|
|
|
What factors/substances cause hyperkalemia?
What factors/substances cause hypokalemia? |
Hyperkalemia:
K+ sparing diuretics ACE inhibitors Acidosis Insulin-deficiency Beta-agonists Hyperosmolarity Digitalis Cellular lysis Hypokalemia: Loop diuretics Thiazides Insulin Beta-agonists Alkalosis Hyposmolarity DKA Heart/Renal failure |
|
|
What are the actions of angiotensin II?
|
Direct vasoconstricting effect
Raises aldosterone levels-->Inc Na and H2O reabsorption in proximal tubule Dec'd renal blood flow, but inc'd GFR and FF |
|
|
What is the site of action of mannitol?
What is the site of action of the thiazides? |
Mannitol: Woks at proximal convoluted tubule
Thiazides: Early distal tubule |
|
|
What substances can be used to estimate GFR?
What substances can be used to estimate renal plasma flow? |
GFR: Cr, Inulin
RPF: PAH |
|
|
What do the presence of casts indicate?
|
Hematuria/pyuria is of renal origin
|
|
|
Proliferative vs Membranous Glomerular Disorders
|
Proliferative: hypercercellular glomeruli
Membranous: thickening of glomerular BM |
|
|
Nephritic Syndrome:
Pathophys Presentation |
NephrItic = Inflammatory process. When involves glomeruli-->hematuria and RBC casts in urine
a/w azotemia--elevated BUN/Cr, oliguria, HTN, proteinuria (<3.5 g/day) |
|
|
Azotemia vs Uremia
|
Azotemia: elevated BUN/Cr
Uremia: azotemia + systemic effect (pleuritis, pericarditis, EKG changes, etc.) |
|
|
Acute Poststreptococcal Glomerulonephritis:
Pathophys LM/EM presentation |
Glomeruli enlarged, hypercellular, nphils, lumpy-bumpy appearance
Subepithelial immune complex humps Frequently seen in children. Resolves spontaneously |
|
|
Rapidly progressive glomerulonephritis:
Pathophys LM/EM presentation IF presentation |
LM--crescent-moon shape; crescents consist of fibrin and plasma proteins (e.g., C3b) w/glomerular fn parietal cells, monocytes, macs
Severe causes: -Goodpasture Syndrome (type II hypersens); Abs to GBM and alveolar BM-->linear immunofluorescence -Wegener's granulomatosis (c-ANCA) -Microscopic polyangitis (p-ANCA) |
|
|
Diffuse proliferative glomerulonephritis:
LM/EM presentation Pathophys |
Most common cause of death in SLE, Membranoproliferative GN
EM: subendothelial DNA-anti-DNA IC's |
|
|
Berger's Disease:
Pathophys |
Inc'd synthesis of IgA with IC's deposit in mesangium
Often presents/flares with URI or acute gastroenteritis |
|
|
Alport's syndrome;
Pathophys Presentation |
Mutation in type IV collagen-->split BM
Can't see, can't pee, ca'n't hear (Nerve disorders, ocular disorders, deafness) |
|
|
What is nephrotic syndrome?
|
NephrOtic syndrome presents with massive prOteinuria (>3.5g/day, frothy urine), edema, hyperlipidemia, fatty casts
|
|
|
Membranous glomerulonephritis:
Pathophys LM/EM presentation |
Diffuse capillary and GBM thickening
Spike and dome appearance with subepithelial deposits (nephrotic syndrome) Caused by drugs, infections, SLE; most common adult cause of nephrotic syndrome |
|
|
Minimal change disease:
Pathophys LM/EM presentation |
LM--normal glomeruli
EM--foot process effacement May be triggered by recent infection or immune stimulus. Most common in children. Responds to steroids. |
|
|
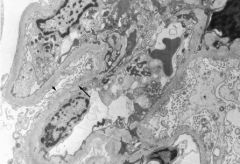
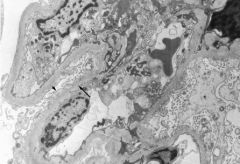
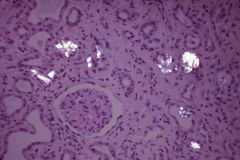
Minimal change dz; normal glomeruli on LM but effacement of foot processes on EM (arrowhead). The full arrow points to a normal foot process.
Treatment consists of steroids. |
|
|
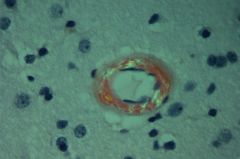
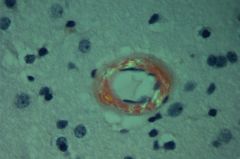
Amyloidosis--congo red stain demonstrates amyloid deposits in artery wall that show apple-green birefringence under polarized light.
|
|
|
Amyloidosis is associated with _______.
|
Multiple myeloma, TB, RA
|
|
|
Diabetic glomerulonephropaty:
Pathophys |
Nonenzymatic glycosylation of GBM-->inc'd permeability, thickening
Nonenzymatic glycosylation of efferent arterioles-->inc'd GFR-->mesangial expansion |
|
|
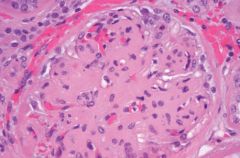
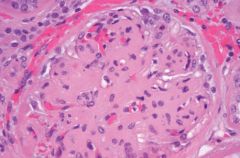
Diabetic glomerulosclerosis--nodular diabetic glomerulosclerosis (also known as Kimmelstiel-Wilson syndrome); characterized by acellular ovoid nodules in periphery of glomerulus.
|
|
|
Membranoproliferative GN:
Type I vs Type II-- EM appearance Causes |
Type I: tram-track appearance due to GBM splitting caused by mesangial ingrowth
Most common cause; HBV, HCV, SLE (more association than cause) Type II: Dense dposits Associated with C3 nephritic factor |
|
|
What renal conditions are associated with hypocomplementemia?
|
Post-strep GN
Membranoproliferative GN (Type II) Lupus nephritis |
|
|
Which glomerular disease:
Most common nephrotic syndrome in children · |
Minimal Change Dz
|
|
|
Which glomerular disease:
IF: granular pattern of immune complex deposition; LM: diffuse capillary thickening |
Membranous GN
|
|
|
Which glomerular disease:
IF: granular pattern of immune complex deposition; LM: hypercellular glomeruli |
Acute post-strep GN
|
|
|
Which glomerular disease:
IF: linear pattern of immune complex deposition |
Anti-GBM Abs with Goodpasture's
|
|
|
Which glomerular disease:
IF: deposition of lgG, lgM, lgA, and C3 in the mesangium |
IgA nephropathy
|
|
|
Which glomerular disease: Kimmelstiei-Wilson lesions (nodular glomerulosclerosis)
|
Diabetic glomerulonephropathy
|
|
|
Which glomerular disease:
Most common nephrotic syndrome in adults |
Membranous GN
|
|
|
Which glomerular disease:
EM: loss of epithelial foot processes |
Minimal Change Dz
|
|
|
Which glomerular disease:
Nephrotic syndrome associated with hepatitis B |
Membranoproliferative GN
|
|
|
Which glomerular disease:
Nephrotic syndrome associated with HIV |
Focal segmental glomerulosclerosis
|
|
|
Which glomerular disease:
Anti-GBM antibodies, hematuria, hemoptysis |
Goopasture's
|
|
|
Which glomerular disease:
EM: subendothelial humps and tram-tack appearance |
Membranoproliferative GN
|
|
|
Which glomerular disease:
Nephritis, deafness, cataracts |
Alport Syndrome
|
|
|
Which glomerular disease:
LM: crescent formation in the glomeruli |
Crescentic GN (aka Rapidly progressive GN)
|
|
|
Which glomerular disease:
LM: segmental sclerosis and hyalinosis |
Focal segmental GN
|
|
|
Which glomerular disease:
Purpura on back of arms and legs, abdominal pain, lgA nephropathy |
Henoch-Schloei Purpura
|
|
|
Which glomerular disease:
LM: wire-loop appearance |
SLE
|
|
|
Which glomerular disease:
Apple-green birefringence with Congo-red stain under polarized light |
Renal amyloidosis
|
|
|
Which glomerular disease:
EM: spiking of the GBM due to electron dense subepithelial deposits |
Membranous GN
|
|
|
Under what circumstances would you see:
RBC Cast |
Acute GN
|
|
|
Under what circumstances would you see:
WBC Cast |
Pyelonephritis, acute interstitial nephritis
|
|
|
Under what circumstances would you see:
Bacterial cast |
Acute pyelonephritis
|
|
|
Under what circumstances would you see:
Epithelial cell cast |
Renal tubular damage
|
|
|
Under what circumstances would you see:
Waxy cast |
Waxy = stasis of urine flow, so much be chronic renal failure
|
|
|
Under what circumstances would you see:
Fatty cast |
Nephrotic syndrome
|
|
|
Under what circumstances would you see:
Granular cast |
Non-specific, can be seen with acute tubular necrosis
|
|
|
Glomerular histology reveals multiple mesangial nodules.
This lesion is indicative of what disease? |
Diabetic glomerulonephropathy
|
|
|
A teenager presents with nephrotic syndrome and hearing loss.
What is the disease? |
Alport's Syndrome
|
|
|
A 4 year-old boy presents with facial edema and proteinuria.
What is the appropriate treatment? |
Steroids (this is Min Change Dz)
|
|
|
What is the only radiolucent kidney stone?
|
uric acid stones
|
|
|
Calcium kidney stones:
Frequency Causes |
75-85% of all kidney stones
Consists of calcium oxalate, calcium phosphate, or both. Caused by conditions that cause hyperCa2+ (cancer, hyperPTH) Oxalate crystals can result from ethylene glycol (antifreeze) or Vitamin C abuse |
|
|
Ammonium magnesium phosphate kidney stones:
Frequency Causes |
15% of kidney stones
Caused by infection with urease-positive bugs (Proteus, Staph, Klebsiella) can form staghorn calculi that can be nidus for UTIs |
|
|
Uric acid kidney stones:
Frequency Causes |
RADIOLUCENT
5% of stones Strong assocn w/gout; often seen in dz w/inc'd cell turnover such as leukemia |
|
|
Which kidney stones can be treated by alkalinization of urine?
Which stone would be worsesned by alkaluria? |
Use alkaluria to tx Cystine stones (only 1% of renal stones)
DO NOT use alkaluria to tx ammonium magnesium phosphate stones |
|
|
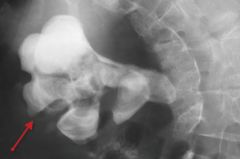
Calcium oxalate outlining a large right renal collecting duct system creating a "staghorn" calculus--can be calcium stone OR ammonoium magnesium phosphate (which present as STAGHORN)
|
|
|
Calcium oxalate crystals in kidney, viewed with polarizers. Tubular failure in oxalate nephropathy can result from vitamin C or antifreeze abuse.
|
|
|
Renal cell carcinoma:
Histologic features Risk factors Presentation Site of Mets Associated disorders |
Polygonal clear cells in renal tubular cells
Inc'd incidence w/smoking and obesity Manifests with hematuria, palpable mass, secondary polycythemia, flank pain, fever, weight loss Paraneoplastic syndromes (ectopic EPO, ACTH, PTHrP, prolactin) INvades IVC and spreads hematogenously; mets to lung and bone Assocd w/von Hippel-Lindau syndrome and gene deletion in chromosome 3 |
|
|
Wilms' Tumor:
AKA Presentation Cause |
AKA nephroblastoma
(Most common renal malignancy of early childhood) Contains embryonic glomerular structures Presents with huge, palpable flank mass, andn/or hematuria Deletion of tumor suppressor gene WT1; may be part of WAGR complex (Wilms tumor, Aniridia, GU malformn, MR) |
|
|
Renal cell carcinoma. Histology shows polygonal cells with small nuclei and abundant clear cytoplasm with a rich, delicate branching vasculature.
|
|
|
Transitional cell carcioma:
Presentation Risk Factors |
Most common tumor of urinary tract system, can occur in renal calyces, renal pelvis, ureters, bladder
Painless hematuria suggests bladder cancer Risk factors in your Pee SAC: Phenacetin Smoking Aniline Dyes Cyclophosphamide |
|
|
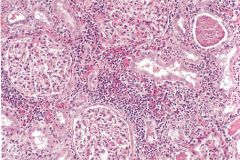
Pyelonephritis:
Acute vs Chronic-- Histologic features Presentation |
Acute pyelonephritis:
-Affects cortex w/sparing of glomeruli/vessels Presents w/fever, CVA tenderness, nausea, vomiting WHITE CELL CASTS CLASSIC for this Chronic: Coarse, asymmetric corticomedullary scarring, blunted calyx Tubules can contain eosinophilic casts (thyroidization of kidney) |
|
|
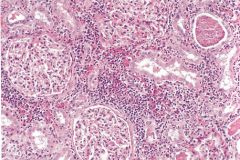
Acute pyelonephritis characterized by nphilic infiltration and abscess formation within renal interstitium. Abscesses may rupture, introducing collections of white cells to tubular lumen.
|
|
|
Chronic pyelonephritis with lymphocytic invasion and fibrosis.
|
|
|
Acute Interstitial Nephritis:
Cause Presentation Treatment Urinalysis finding |
Most common cause of acute renal failure; mostly drug-induced
Cause: Drugs--NSAIDS, PCN/cephalosporins (methicillin), sulfonamides (TMP-SMX, foresmide), cipro, cimetidine, allopurinol Tx w/2 weeks steroids Presentation: fever, rash, ephilia, azotemia Muddy brown (granular) casts = key finding |
|
|
Acute Tubular Necrosis:
Cause Presentation |
Cause:
aminoglycosides, cephalosporins, polymixins Contrast dye Rhabdomyolysis/myoglobinuria from seizures, cocaine, crush injuries FIndings: 4+ blood in urine, no RBC on urine cell count (because it's myoglobin in urine), renal failure |
|
|
Renal Papillary Necrosis:
Causes Pathophys |
Sloughing of papillae-->gross hematria, proteinuria
May be triggered by recent infection or immune stimulus A/W: DM Acute pyelonephritis Chronic acetaminophen use Sickle cell anemia |
|
|
Acute renal failure:
Definition Prerenal vs Intrinsic vs Postrenal-- Pathophys and Examples |
Acute renal failure--abrupt decline in renal fn w/inc'd Cr and BUN over several days
1) Prerenal azoetmia--due to dec'd RBF (HYPOTENSION, dehydration, hypovolemia, shock, renal vasoconstricion as with NSAIDs)-->dec'd GFR, Na/H2O and Urea retained by kidney to reserve volume so, BUN/Cr ratio increases Intrinsic renal: Acute tubular necrosis or ischemia/toxins; necrosis leads to debris obstructing tubule and fluid backflow across necrotic tubule; results in dec'd GFR. Urine has epithelial/granular casts. BUN reabsorption impaired-->dec'd BUN/Cr ratio Postrenal--outflow obstruction (stones, BPH, neoplasia, congenital anomalies); develops ONLY with BILATERAL obstruction |
|
|
Acute vs Chronic Renal Failure:
Most common causes |
Acute: Acute tubular necrosis
Chronic: HTN, DM |
|
|
What is uremia?
|
Clinical syndrome marked by inc'd BUN and inc'd Cr
Presents with nausea, anorexia Pericarditis Asterixis (hand-flapping tremor) Encephalopathy PLT dysfn |
|
|
UTI caused by Proteus vulgaris.
Associated renal stone? |
Ammonium Magnesium Phosphtate Stone-->Staghorn calculi
|
|
|
A patient reports a long-term history of acetaminophen use.
What is she at increased risk of? |
Renal papillary necrosis--but NSAIDs can do this too!
|
|
|
What artery prevents a horseshoe kidney from ascending in the abdomen?
|
IMA
|
|
|
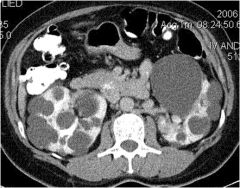
CT Scan of ADPKD
|
|
|
ADPKD:
Pathophys Presentation At risk of? |
AD mutation in APKD1/2-->multiple, large, b/l cysts that ultimately destroy kidney parenchyma
Presents w/flank pain, hematuria, HTN (inc'd renin production), urinary infection, progressive renal failure Risk of polycystic liver dz, berry aneurysms, mitral valve prolapse |
|
|
ARPKD:
Presentation |
Infantile presentation of ADPKD in parenchyma.
ASsocd w/hepatic fibrosis. Can lead ot Potter's if develop renal failure in utero. |
|
|
Central pontine myelinosis:
Cause |
Rapid correction of hyponatremia
|
|
|
How does EKG reflex K+ levels?
|
Low K+ - Flat T waves
High K+ - Peak T waves |
|
|
What is the WAGR complex?
|
Wilms' Tumor
Aniridia GU malformn Retardation (mental) |
|
|
Which glomerular disease:
IF: granular pattern of immune complex deposition; LM: diffuse capillary thickening |
Membranous GN
|
|
|
Which glomerular disease:
IF: granular pattern of immune complex deposition; LM: hypercellular glomeruli |
Acute poststrep GN
|
|
|
Which glomerular disease:
IF: linear pattern of immune complex deposition |
Goodpasture's
|
|
|
Which glomerular disease:
IF: deposition of lgG, lgM, lgA, and C3 in the mesangium |
IgA neprhopathy
|
|
|
Which glomerular disease:
EM: subendothelial humps and tram-tack appearance |
Membranoproliferative GN
|
|
|
Which glomerular disease:
Nephritis, deafness, cataracts |
Alport Syndrome
|
|
|
Which glomerular disease:
LM: crescent formation in the glomeruli |
Crescentic/Rapidly Progressive GN
|
|
|
Which glomerular disease:
LM: segmental sclerosis and hyalinosis |
Focal segmental glomerulosclerosis
|
|
|
Which glomerular disease:
Purpura on back of arms and legs, abdominal pain, lgA nephropathy |
Henock Schonlein Purpura
|
|
|
Which glomerular disease:
EM: spiking of the GBM due to electron dense subepithelial deposits |
Memranous GN
|
|
|
Diagnose:
pH 7.50 HCO3 35 pCO2 42 |
Metabolic alkalosis w/o compensation
|
|
|
Diagnose:
pH 7.33 HCO3 13 pCO2 28 |
Metabolic acidosis w/compensation
|
|
|
Diagnose:
pH 7.20 HCO3 18 pCO2 40 |
Metabolic acidosis w/o compensation
|
|
|
Diagnose:
pH 7.66 HCO3 36 pCO2 30 |
Metabolic and respiratory alkalosis
|
|
|
Diagnose:
pH 7.47 HCO3 14 pCO2 22 |
Resp alkalosis w/compensation
|
|
|
Diagnose:
pH 7.10 HCO3 15 pCO2 50 |
Combined metabolic and respiratory acidosis
|
|
|
Risk factors for transitional cell carcinoma?
|
PSAC
Smoking--- Phenacetin (acetaminophen) Smoking Aniline dyes Cyclophosphamide |
|
|
What are the causes of acidosis with an elevated anion gap?
|
MUDPILES
Methanol Uremia DKA Paraldehyde/phenformin Fe tables or INH Lactic acidosis EtOH or ethylene glycol Salicylates |
|
|
What changes will be seen in a basic metabolic panel in a patient with renal failure?
|
High K+
High PO4 Low Ca2+ High BUN/Cr |
|
|
CT scan reveals massively enlarged kidney bilaterally.
Diagnosis? |
ADPKD
|
|
|
Which electrolyte disturbance:
Correcting too rapidly may result in central pontine myelinosis |
Hyponatremia
|
|
|
Which electrolyte disturbance:
Peaked T waves |
Hyperkalemia
|
|
|
Which electrolyte disturbance:
Tetany |
Hypocalcemia
|
|
|
Which electrolyte disturbance:
Arrhythmias |
High/low K+
Low Mg2+ |
|
|
Which electrolyte disturbance:
Decreased deep tendon reflexes |
Hypermg2+
|
|
|
Which electrolyte disturbance:
Flattened T waves, U waves on EKG |
Low K+
|
|
|
Which renal pathology:
Most common tumor of the urinary tract system |
Transitional cell ca
|
|
|
Which renal pathology:
Most common renal malignancy of early childhood (ages 2-4) |
Wilms' Tumor
|
|
|
Which renal pathology:
Histologic appearance of renal cell carcinoma |
Clear cell carcinoma
|
|
|
Which renal pathology:
Histological appearance of chronic pyelonephritis |
Thyroidization of kidney
|
|
|
Which renal pathology:
Fever + rash + hematuria + eosinophilia |
AIN
|
|
|
Which renal pathology:
Cancer associated with Schistosoma haematobium |
Squamous cell carcinoma of bladder
|
|
|
Which renal pathology:
Treatment for cystine kidney stones |
Alkalinization of urine
|