![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
patients are able to perform activities of daily living if elbow range of motion of___degrees to ___ degrees flexion/ extension is achieved |
30 -130 |
|
|
|
most activities require a ___degree arc of motion at the elbow to be functional |
100 |
|
|
|
a___ degree loss of extension is well tolerated by most patients |
30 |
|
|
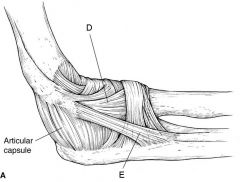
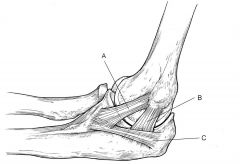
Figures A (this digram) and B (see hint) are diagrams depicting the ligamentous attachments about the elbow. To restore elbow flexion, in addition to releasing the articular capsule, which ligament should be released? |

|
|
|
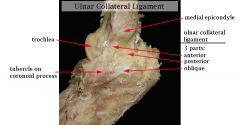
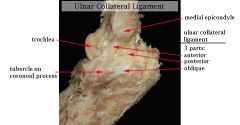
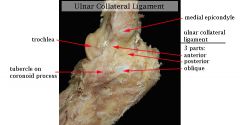
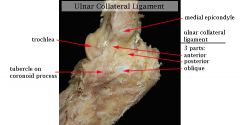
WHICH LIGMENT in elbow is attached dorsal to the axis of rotation and has greater variation in length? |
posterior band of the MCL |
|
|
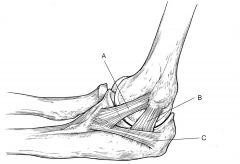
-which band of the MCL (AMCL) maintains a constant length (isometric) throughout the entire arc of movement? -which letter? |
anterior A=anterior |
|
|
anterior capsule stabilizes the elbow to ___stress in extension, |
varus-valgus |
|
|
anterior band of the MCL is a primary stabilizer, especially in ___ |
flexion. |
|
|
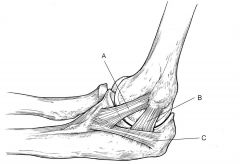
Release of theanterior band of the medial collateral ligament leads to ___ instability. letter? |
valgus a=anterior |
|
|
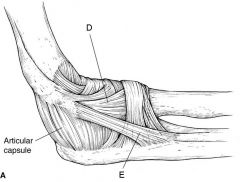
Release of the lateral ulnar collateral ligament (LUCL) leads to ___. letter? |
posterolateral rotatory instability (PLRI). E=LUCL |
|
|
|
clinical presentation is consistent with post-traumatic elbow stiffness following an elbow fracture-dislocation. What initial treatment option will likely provide the greatest improvement in this patients functional range of motion? |

Supervised exercise therapy with static progressive elbow splinting |
|
|

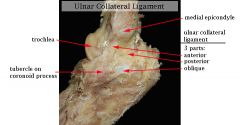
What is the effect of released the the posterior oblique portion of the medial collateral ligament of the elbow? |
-gain flexion in patients with post-traumatic contracture |
|
|
The ____ ligament is one of the primary static stabilizers of the elbow |
medial ulnar collateral |
|
|
MCL provides resistance to ___ &___stresses. |
valgus and distractive |
|
|
____ are the most important against valgus stresses in elbow? |
anterior oblique fibers (of the anterior bundle) |
|
|
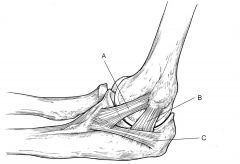
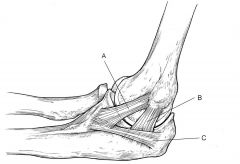
___ is involved elbow contractures and releasing it can yield significant flexion gains? letter? |

posterior bundle -B |
|
|
|
Has the highest tensile strength of any elbow ligament |
anterior oblique bundle of the medial ulnar collateral ligament. |
|
|
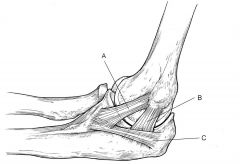
Is reconstructed in the Tommy John procedure/ -letter? |

anterior oblique bundle of the medial ulnar collateral ligament. -A |
|
|
|
Is the primary ligamentous restraint to valgus force during throwing |

anterior oblique bundle of the medial ulnar collateral ligament. |
|
|
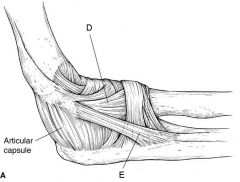
Is responsible for the pivot shift of the elbow? -ID letters D & E? |
-Lateral ulnar collateral (LUCL) insufficiency is responsible for posterolateral rotatory instability and a positive pivot shift of the elbow. -E-LCL D-radial collateral band |
|
|
|
if total elbow arthroplasty what is the MC restriction? |
permanent 5-lb lifting restriction |
|
|
|
Elbow Stiffness and Contractures MC complication? -MC tx? |

MCC-Post-operative heterotopic ossification tx-low-dose radiation therapy or indomethacin |
|
|
Dx? MoI? MC cause? -Stx? |
-Lateral Epicondylitis (Tennis Elbow) - repetitive pronation and supination with elbow in extension -eccentric overload of ECRB Stx=Release and debridement of ECRB origin |
|
|
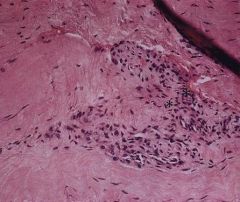
pain that is reproduced with gripping, resisted long finger extension, resisted wrist extension while the elbow is fully extended, and maximum passive wrist flexion. -dx? -microscopic evaluation of the tissue reveals?MC associated condition? |
|
|
|
|
pain with resisted supination with the arm and wrist in extension characteristically seen with ___ |
radial tunnel syndrome. |
|
|
- common extensor wad, that also includes 6 muscles? -Overuse injury involving eccentric overload of which muscle? innervation of MC muscle involved? |
|
|
|

A 12-year-old baseball pitcher describes progressive worsening of medial elbow pain on his throwing side What is the most likely cause of his symptoms? Moi? -MC complication? |
- Little League Elbow= Medial epicondyleapophysitis - repetitive contraction of the flexor-pronator mass stresses the chondro-osseous originvalgus loading -Ulnar nerve neuropathy |
|
|

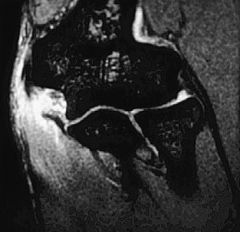
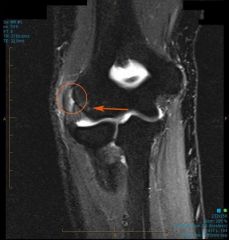
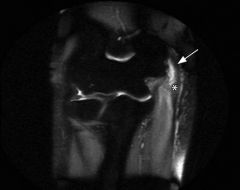
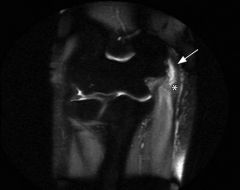
A 10-year-old little league pitcher has the triad of medial elbow pain in his throwing arm, decreased throwing effectiveness, and decreased throwing distance DX? Stx? best test to Confirm StX finding? |

-Little Leaguer's elbow. medial apophysitis. -Pediatric UCL reconstruction using palmaris longus autograft MRI- UCL insufficiency |
|
|

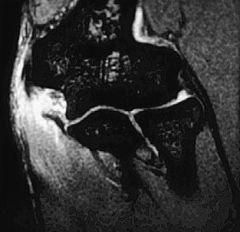
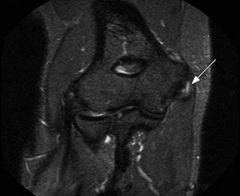
A 13-year-old pitcher develops pain over the lateral aspect of his throwing elbow. He has an effusion and a painful click on passive elbow rotation. What is the most likely diagnosis? classification/describe? Stx? |
- Osteochondritis dissecans -Type II Cartilage fracture with bony collapse or displacement -diagnostic arthroscopy and drilling of capitellum |
|
|
almost always occurs in the dominant elbow in boys between 5 and 12 years of age; -dx/define? - |
Panner disease exhibits an irregular epiphysis,=pathologic process is believed to be caused by an interferrence in blood supply to growing epiphysis, which results in resorption & eventual repair and replacement of the ossification center; |
|
|

Loose bodies present in elbow joint with OCD is classified as? mech sx? -best test to confirm? why? |
Type III -PE=catching, locking grinding motion restriction -MRI to assess size extent of edema, cartilage status |
|
|
Dx? Moi? Stx? MC complication with Stx? |
-Medial Epicondylitis (Golfer's Elbow) -repetitive wrist flexion/forearm pronation -Open debridement and reattachment of flexor-pronator mass -Medial antebrachial cutaneous nerve neuropathy |
|
|
-name 5 the muscles affected/innervation? -only muscle innervated by ulnar ner? -MC tendons implicated in this dx?? |
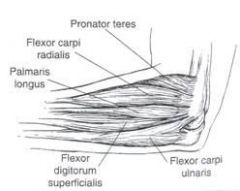
- Flexor-pronator mass includes
|
|
|
MRI with this & provocative tests pain with resisted forearm pronation and wrist flexion dx? -with this Dx MC tx of MC complication? -arises from the __of the brachial plexus. |
- Medial Epicondylitis (Golfer's Elbow) - transpose Medial antebrachial cutaneous nerve neuropathy into brachialis muscle -medial cord |
|
|

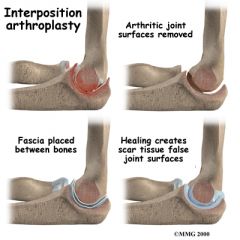
A 66 year old woman has chronic elbow pain and loss of function. She has severe morning stiffness and takes several medications for this. -DX? -What is the most appropriate definitive treatment? -stx dependent on what PE findings? |

severe rheumatoid arthritis.-->Elbow Arthritis -total elbow arthroplasty -competent elbow ligaments and adequate bone stock->unconstrained TEA |
|
|

younger patients with decreased ROM & this xray. Stx? - if there is an extension contracture preoperatively tx? |

- olecranon fossa debridement (Outerbridge-Kashiwagi procedure) -decompress the ulnar nerve - |
|
|

MC location to find osteophytes? |
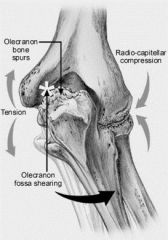
-olecranon tip and posteromedial olecranon fossa |
|
|
|
primary restraint to distraction forces in full extension in elbow? |
capsule |
|
|
|
secondary stabilizer to varus force in elbow? |
- aconeus, |
|
|
|
- most important to provide 30% of valgus stability in elbow?- |
- radial headand lateral capsule |
|
|

-other STx for young high demand patients with DJD elbow?MC complication? |
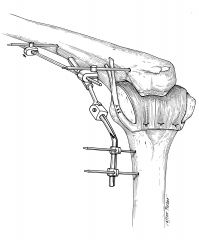
ulnohumeral distraction interposition arthroplasty- ulnar nerve dysfunction |
|
|

MC pt population affected what is dx? -who is affected? -stx if incompetent elbow ligaments |
-primary arthritis elbow -in middle-aged male laborers -constrained TEA |
|
|
|
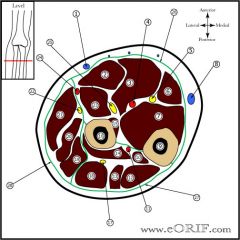
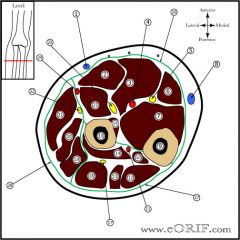
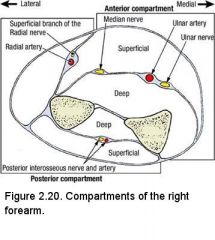
1. Cephalic vein 2. Flexor carpi radialis(FCR) 3. FDS 4. Ulnar artery 5. Ulnar nerve 6. Flexor carpi ulnaris(FCU) 7. FDP 8. Basilic vein 9. Ulnar Shaft 10. APL 11. Posterior Interosseous artery 12. Ext. Carpi ulnaris (ECU) 13. Extensor digiti minimi 14. Supinator 15. Flexor pollicis longus 16. Radial Shaft 17. Deep branch of Radial nerve 18. Extensor digitorum 19. ECRB 20. ECRL 21. Brachioradialis 22. Superficial branch of Radial nerve 23. Pronator teres 24. Radial artery 25. Median nerve 26. Volar (flexors) 27. Dorsal (extensors) 28. Mobile wad(Brachioradialis,ECRL, ECRB) |
|
|
|
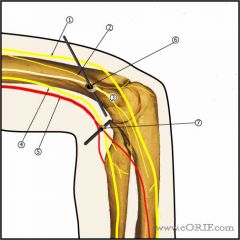
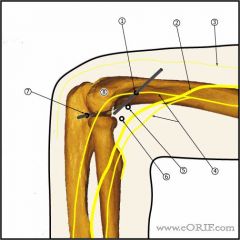
1. Ulnar nerve 2. Medial antebrachial cutaneous nerve 3. Medial epicondyle 4. Median nerve 5. Brachial artery 6. Superomedial portal (proximal anteromedial portal): anteriorto the intermuscular septum, 2cm proximal to the medial epicondyle. Must stayanterior to the medial intermuscular septum to aboid ulnar nere injury. 7. Anteromedial portal: generally used to augment superomedial portal.Ensure ulnar nerve is not subluxed before establishing anteromedial portal.Generally 2cm distal and 2 cm anterior to the medial epicondyle. Risks: ulnarnerve, medial antebrachiocutaneous nerve. |
|
|
|
|
|
|

A 3-year-old male has decreased use of his left elbow after his mother grabbed his arm and attempted to lead him across the street. Physical exam demonstrates guarding of the extremity with a slightly flexed and pronated arm, elbow swelling, and focal tenderness. A lateral radiograph is shown in Figure A. What is the most appropriate first step in management? -dx? -MC age effected & MoI? |
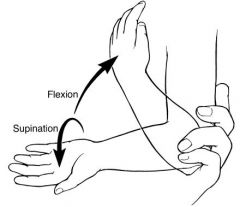
Closed reduction via supination and flexion - nursemaids elbow - children under 5 years of age as a result of a quick pull on an extended and pronated arm and results in subluxation of the annular |
|
|

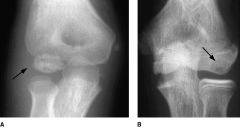
A 2-year-old is brought to the emergency room with reports of acute elbow pain and limited use of the left upper extremity. The patient is neurovascularly intact and is afebrile. Examination reveals that the elbow is in slight flexion and the forearm pronated but further examination is limited secondary to pain. AP and lateral radiographs are shown in Figures A and B. What is the next best step in management? -what is NOT necessary x2? -DX |
-Supination and flexion reduction maneuver - no radiographic & No Cast -radial head subluxation or “nursemaid’s elbow”. |

|
|
|
MC complication with nurse maids elbow? |
Recurrenceoccurs in 5% to 39% of cases, but generally ceases after 5 years of age. |
|
|
|
An 11-year-old boy sustains an elbow injury. Which of the following injuries could be appropriately managed with a long arm posterior splint for 8-12 days, followed by protected range of motion exercises? 1. Nondisplaced lateral condyle fracture 2. Acutely reduced elbow dislocation 3. Ulnar collateral ligament sprain 4. Gartland type I supracondylar fracture 5. Minimally displaced olecranon fracture |
2 -Acute elbow dislocations can be appropriately treated with a long arm posterior splint for 10 days, followed by protected range of motion exercises.Acute pediatric elbow dislocations are most common in 10-15 year-olds. They are classified according to the position of the proximal radio-ulnar joint in relation to the distal humerus. Posterior dislocations are most common. Treatment involves closed reduction, verification of stability, then brief immobilization with early range of motion. Operative treatment is usually indicated in open dislocations and incarcerated medial epicondyle fragments. |
|
|

-Dx? -associated conditions? -Stx-indication? -MC complicatioon? |
-Elbow dislocation - PL -look for fractures of medial epidcondyle, coronoid, proximal radiushigh index of suspicion for transphyseal (distal humerus epiphyseal separation) fractures in very young children (<3 years old) -incarcerated medial epicondyle or coronoid process in the joint -Stiffness |
|
|

-Dx- -MC neurapathy? -MC assocated FX? -Mc age effected? Moi? |
--Elbow dislocation - PL -avulsion of the medial epicondyle -ulnar N, at risk with associated medial epicondyle avulsions -most common in 10-15 year oldsvery rare in younger children< 3 years old Moi=Foosh=fall onto an outstretched hand |
|
|

- When comparing ORIF with a plate to a percutaneous technique using intramedullary nails (IMN), -what is MC finding with 2 tx techniques? -what is optimal fracture patterns for IMN technique are? -MC compliction w/this fx? |

- Restoration of radial bow is similar in both groups - midshaft pediatric both bone forearm fractures with minimal comminution in transverse and oblique patterns and acutely after injury prior to the presentation of fracture callus -Refractureoccurs in 5-10% following both bone fractures |
|
|

An 11-year-old boy fell on his outstretched right hand. He has a closed injury and is neurovascularly intact. Injury films are shown in Figures A and B. The patient undergoes an anatomic closed reduction in the emergency department and the fracture is stable under fluoroscopic imaging. What would be your next step in management? -Surg Indications for this fx? |
-Short-arm cast SI=unacceptable alignment following closed reduction
|
|
|
apex volar fractures (supination injuries)may be treated and reduced by forearm ____ apex dorsal fractures (pronation injuries)may be treated and reduced by forearm ____? |
-pronation -supination |
|
|
|
A 12-year old boy fell sustaining a both bone forearm fracture. When properly reduced what is radiographic assessment of anatomic forearm alignment after reduction?(AP &L ) |

AP radiograph demonstrates the radial styloid and biceps tuberosty 180 degrees apart (Illustration A). On the lateral, the coronoid process and ulnar styloid will be 180 degrees apart. |
|
|

bayonet apposition ok if ___years |
<10 |
|
|

MC complication if multiple attempts at reduction and rod passage? -MC PE finding that can often be missed if not evaluated by an orthopaedic surgeon |

-compartment syndrome - subtle poke-holes=open fx=Surgery |
|
|
|
what is the most common fracture in children <16 years old? MC complication tx of this fx? MC complication with SAC resulting in displacement? |
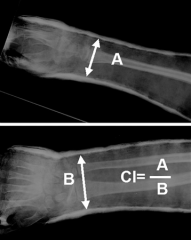
-Forearm Fractures - -Casting Thermal Injury - Cast index greater than 0.85 was associated with a significantly higher rate of displacement (26%) |
|
|
|
An 11-year old boy presents to fracture clinic 1 week after sustaining a displaced metaphyseal distal radius fracture that was managed with closed reduction and cast application. While the initial post-reduction radiographs showed near anatomic alignment with a well molded cast, radiographs 1 week later show 22 degrees of apex volar angulation and dorsal re-displacement. What is the best management at this time? |
Closed reduction and percutaneous fixation |
|
|

Class/dx? -Acceptable Angulation for Closed Reduction in Pediatric Forearm Fractures ?8 vs 10 |
SH-2 -8 yrs/< 1 cm/15°shaft/45°rotation/30 dorsal angulation 10 yrs/< 1 cm/10°shaft/ 30°rotation/ 20 dorsal angulation |
|
|
|
) What is the most common fracture in children younger than 16-years-old? 2nd MC fx? 3rd MC fx? |
#1Distal radius 2- fractures of the phalanges of the hand #3- fractures of the carpal/metacarpal region |
|
|

Isolated pronation of the forearm will most likely achieve reduction of what type of fracture in a 7-year-old boy? |
Supination injury resulting in an apex-volar greenstick both bone forearm fracture |
|
|

if this fx which is better to reduce risk of loss of reduction SAC or LAC? - accepted angulation is dependent on what 3 factors? |
-no increased risk of loss of reduction with short arm vs. long arm casting -patient-age;location of the fracture;type of deformity (angulation, rotation, bayoneting). |
|
|
|
-name 2 fx with dislocatin? -name 2 fx of metaphysis? -name 2 fx of diaphysis? |
-dislocation=Monteggia’s fracture Galeazzi fracture -meta=distal radius fx (Colle's fx) Torus fx -both bone fx Greenstick fx |
|