![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
51 Cards in this Set
- Front
- Back
|
amniotic fluid is produced by |
fetal kidney, skin, lungs, umbilical cord, membranes |
|
|
in 2nd and 3rd trimesters what accounts for 2/3 of AFI |
fetal urination after 16 wks most of the fluid is produced by the fetal urinary system amniotic fluid is absorbed by fetal swallowing and gastrointestinal absorption |
|
|
functions of the amniotic fluid |
cushion fetus allows for fetal movement or activity prevents adherence of amnion to embryo promotes lung growth regulates temp |
|
|
amount of fluid is directly related to less than 15 wks |
AFI is from amnion: diffusion of maternal plasma through chorionic plate; exchange of fluids through fetal maternal circulation
|
|
|
amount of fluid is directly related to 15-30 wks |
fetal kidneys and skin diffusion if abnormality/absence of fetal kidneys, AFI is directly impacted |
|
|
amount of fluid is directly related to greater that 30 wks |
skin diffusion decreases; renal function and urine output increases |
|
|
1st trimester: fluid is regulated through |
membranes, fetal lungs, and skin |
|
|
2nd/3rd trimester fluid is regulated through |
urine and fetal swallowing |
|
|
normal levels based on GA 10wks |
30mL |
|
|
normal levels based on GA 20 wks |
300mL
|
|
|
normal levels based on GA 30 wks |
600mL |
|
|
normal levels based on GA 36wks |
1000mL |
|
|
normal levels based on GA 38-42 wks |
600mL |
|
|
subjective observation |
sonographer eye-balls amount |
|
|
subjective observation 20-30 wks |
AFI appears generous but normal amount |
|
|
subjective observation end of prgnancy |
AFI appears minimal with a single larger pocket of fluid within uterus |
|
|
assessment of amniotic fluid volume maximum vertical pocket |
measure largest pocket found measure anterior to posterior MVP of 8cm or greater is considered polyhydramnnios |
|
|
don't measure fluid where |
loops of cord are present
can use color/power to obtain a more accurate fluid volume assessment |
|
|
amniotic fluid can be assessed subjectively or |
quantified with the four-quadrant method or single largest vertical pocket method
|
|
|
amount of fluid correlates with fetal and placental weight |
small for age fetus - low AFI large for dates fetus - high AFI |
|
|
amniotic fluid u/s |
appears anechoic but some particulate matter may appear further along in the pregnancy |
|
|
vernix |
fatty material of fetal skin may be visualized in amniotic fluid later in pregnancy |
|
|
subjective assessment; sonographer should |
visually assess fetal lie and placental position |
|
|
decreased AFI |
sonographer feels there is an overall crowding of fetal parts and unable to visualize any significant pockets of fluid within entire uterus |
|
|
increased AFI |
overall appearance of an excess of fluid (more accurate with experienced sonographers) |
|
|
Four-Quadrant Method (amniotic fluid index) |
divide iterus into 4 quadrants and measure largest vertical pocket (absent of fetal parts) in each quadrant - then total them up |
|
|
normal AFI measurement (4 quad) |
8-22 cm |
|
|
decreased AFI measurement ( 4 quad) |
less than 5 cm |
|
|
increased AFI measurement (4 quad) |
greater than 22cm |
|

4 quadrant method |
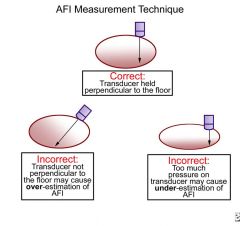
correct transducer placement |
|
|
AFI pitfalls |
be sure NOT to include uterine wall transducer is perpendicular in relation to table gain to low: could miss fetal part, could include uterine wall gain to high: make fluid appear to echogenic use of color Doppler will assist in identifying portion of umbilical cord present |
|
|
single pocket assessment |
identify largest pocket (must be more than 1 cm) without fetal parts and measuring depth
|
|
|
single pocket less than 2cm |
oligohydraminos |
|
|
single pocket 2-8 cm |
normal |
|
|
single pocket greater that 8 cm |
polyhydraminos |
|
|
polyhydraminos |
amniotic fluid volume greater than 2000mL at term largest pocket greater than 8cm |
|
|
polyhydramnios - etiology |
increased secretion of amniotic fluid by large placenta or fetal malformation which prevents swallowing or absorption 60% idiopathic 20% due to maternal disease 20% due to fetal structure anomaly |
|
|
polyhydramnios |
can put too much pressure on baby ; can cause congestive heart failure, puts stress on lungs |
|
|
polyhydramnios - S/S |
sudden maternal weight gain patient large for dates maternal lower limb adema "distant fetal parts and heart tones" clinical quotes |
|
|
polyhydrmnios - u/s |
large amount of amniotic fluid exceptional visualization of fetal parts/details placenta may appear thin (compressed from excessive fluid) |
|
|
seven fetal assessments to be made when examining a fetus with polyhydramnios |
1.assess the head - is there a brain malformation 2. assess the neck and mouth - is there obstuction 3. assess the heart - is there heart failure 4. assess the chest - is there compression 5. assess the esophagus - is the stomach seen 6. assess the upper gastrointestinal tract - obstruction 7. assess the fetus neurologically - is there poor tone |
|
|
oligohydramnios |
abnormally small amount of fluid less than 400-500mL at birth mild - pocket <2 cm but >1cm Oligo - pocket is < 1 cm |
|
|
oligohydramnios - etiology |
fetal demise IUGR (cause or result) placental vascular insufficency PROM fetal renal anomilies |
|
|
Oligohydramnios AFI |
AFI <5-8 cm 16-34 wks AFI less than 8 cm is termed oligo or decreased amniotic fluid volume beyond 34 wks fluid is decreasing and one should see at least a 2 x 2 pocket |
|
|
organs to assess if oligohydramnios is not the result of PROM |
demise D renals R IUGR I PROM P Trisomies T twin to twin transfusion |
|
|
Oligohydramnios S/S |
lack of normal materna weight gain small for dates |
|

Oligohydramnios U/S |
reduced amount of amniotic fluid poor image detail due to lack of tissue-fluid interface crowding of fetal parts decreased in number of pockets of fluid |
|
|
oligohydramnios - prognosis |
fetal risks are dependent of severity and time of onset of oligo skeletal and facial deformities pulmonary hypoplasis under developed lungs, no fluid to develop them |
|
|
polyhydraminos - prognosis |
increased risk of preterm labor (more pressure) pregnancy induced hupertension postpardium hemorrage |
|

echogenic fluid |
amniotic fluid with sludge, patients with preterm labor have an increased risk of infection and preterm delivery |
|
|
3rd trimester echogenic particle most likely represent |
vernix |