![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
141 Cards in this Set
- Front
- Back
|
A patient undergoing liver surgery has a venous air embolism, what is the most appropriate position to place them in: |
B
Heart should be above level of surgical site, left lateral position (air-lock) |
|
|
Which of the following is NOT a side effect of cyclosporine
a. Alopecia b. Hypertension c. Renal impairment d. Gum hyperplasia |
A |
|
|
What is the half life of clopidogrel?
a. 6 hours b. 14 hours c. 24 hours d. 7 days |
A |
|
|
When administering adrenaline and atropine via ETT dose compared with IV should be |
B |
|
|
What splitting ratio gives a 3% concentration of isoflurane |
C |
|
|
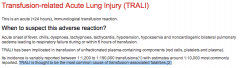
What transfusion related complication is the commonest cause of mortality |
B |
|
|
Which of the following is not included in the CHADS2 AF thromboembolic risk scoring system |
B
|
|
|
What is the ratio of breaths to compressions in neonatal resuscitation |
A
|
|
|
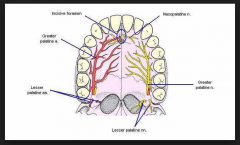
What is the innervation of the hard palate
a. Greater palatine and nasopalatine |
A |
|
|
Which of the following is suggesting of an inhaled foreign body in a child on chest x ray |
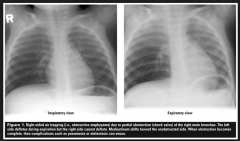
B |
|
|
What is the distance from the lips to the carina in an 70kg adult male in cm |
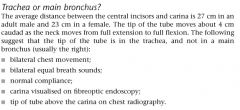
D |
|
|
What colour is the label for subcutaneously administered drugs
a. Pink b. Yellow c. beige d. Red e. Blue |
C |
|
|
How much air is the maximum to that should be used to inflate a 5 LMA classic cuff
a. 15 b. 20 c. 25 d. 40 e. 45 |
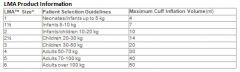
D
|
|
|
Where should the tip of an IABP lie
a. 2cm distal to the left subclavian b. 2 cm proximal to the left subclavian c. 2cm proximal to the renal artery d. 2 cm distal to the renal artery |

A |
|
|
A 60kg female is given 50 mg of rocuronium, she is unable to be intubated, what dose of sugamadex is required to reverse the rocuronium |
C |
|
|
In a penetrating chest injury what part of the heart is most likely to be injured |
B |
|
|
What is the maximum recommended dose of Intralipid in local anesthetic toxicity (ml/kg) |
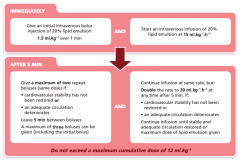
D |
|
|
What is a contraindication to an IABP? |
A
|
|
|
An infant is born with meconium stained liquor and is apnoeic and floppy… your first step should be |
C |
|
|
Central sensitization occurs due to
a. Primary events mediated by the NMDA receptor b. Alterations in gene expression c. Increased magnesium |
A |
|
|
What volume of FFP is required to increase fibrinogen level by 1g/L
a. 10-15ml/kg b. 30ml/kg |
B |
|
|
An epidural in a healthy individual causes all EXCEPT |
A |
|
|
In the Revised Trauma Score includes GCS, Blood pressure and what other parameter?
a. HR b. Saturation c. Respiratory rate d. Urine output |
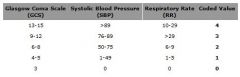
C |
|
|
Autologous transfusion results in less
a. Cost b. Blood waste c. Incompatible transfusion d. Unrequired transfusion |
C |
|
|
After an infusion of normal saline causing isovolumetric haemodilution what occurs?
a. Increased cardiac output b. Increase oxygen extraction c. Capillary vasodilatation |
A |
|
|
Bleeding in trauma has been shown to be reduced by
a. Tranexamic acid b. Recombinant factor VIIa c. DDAVP d. Prothrombinex |
A |
|
|
The time constant of the lung is calculated by
a. Compliance x resistance b. Compliance plus resistance c. Compliance /resistance d. Resistance/compliance |
A |
|
|
The commonest post operative complication in a patient with a # NOF is
a. UTI b. Pneumonia c. Delirium d. Myocardial infarction |
C
10-15% according to a BMJ article |
|
|
In an infant, the intercristine line is at the level of |
E |
|
|
Which of the following is a contra-indication to a left DLT
a. Left pneumonectomy b. Tumour in the left main stem bronchus |
B
Contraindications to a Left DLT • Intra-luminal tumour of l main bronchus • Left bronchial stent in situ • Left tracheo-bronchial disruption • Left pneumonectomy • Left lung transplant |
|
|
What is the commonest symptomatic cardiac condition in pregnancy
a. Mitral stenosis b. Aortic stenosis c. Eisenmengers d. Tetralogy of fallot |
A
Anaesthesia for Caesarean Section in Patients with Cardiac Disease. Journal of The Pakistan Medical Association “Rheumatic heart disease at present is the most common cardiac disorder in pregnancy, with mitral stenosis (MS) as a single most prevalent lesion” |
|
|
What is the ratio of MAC awake:MAC of sevoflurance
a. 0.2 b. 0.34 c. 0.5 |
B
Cerebral Awakening Concentration of Sevoflurane and Isoflurane Predicted During Slow and Fast Alveolar Washout. A & A November 1993 vol. 77 no. 5 1012-1017 Make awake value for sevo = 0.34 |
|
|
Pain from the uterus during labour is transmitted via |
C |
|
|
The features of Pierre Robin sequence include cleft palate, micrognathia and:
A. Glossoptosis B. Craniosynostosis C. Macroglossia D. Microstomia |
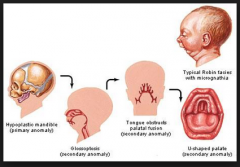
A |
|
|
A size C oxygen cylinder that reads 5000kpa contains approximately how many litres of oxygen
a. 100 b. 150 c. 200 d. 350 e. 600 |
B |
|
|
A patient having a craniotomy has the CVP/arterial transducers at the level of the right atrium. The head is 13cm above the level of the heart. If the MAP is 80mmHg and the CVP is 5mmHg what is the cerebral perfusion pressure in mmHg
a. 60 b. 62 c. 65 d. 70 e. 75 |
D |
|
|
After a procedure with an LMA in situ a patient complains of loss of sensation to the anterior part of the tongue. What nerve is likely damaged? |
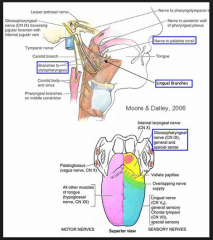
B |
|
|
What statistical test would be best to evaluate the effects of 2 drugs in patients at 3 different points in time |
A |
|
|
A man is working with electrical appliances at home with a residual current device. If he touches the active and the neutral (was it neutral or earth) wire he will suffer
a. A microshock b. A macroshock c. Nothing happens because the fuse blows d. The RCD will protect him from macroshock |
D
RCD will protect him from macroshock RCD will trip with a 30 mA leakage - works on principle that current flowing to and from an appliance (in live and neutral wires) is equal. Current of 100mA required to cause VF when applied to surface of body. Only 0.05 - 0.1 mA required to cause VF when applied directly to myocardium (=microshock) |
|
|
An infant with failure to thrive is noted to have an apical systolic murmur, weak pulses, with the femoral felt most easily. They most likely have
a. Patent ductus arteriosis b. Ventriculoseptal defect |
Neither seem quite right. Definitely not PDA though
Medscape – PDA “In the low birth weight premature infant, the classic signs of a patent ductus arteriosus (PDA) are usually absent. The classic continuous murmur is rarely heard. A rough systolic murmur may be present along the left sternal border, but a small baby with a large patent ductus arteriosus (PDA) and significant pulmonary overcirculation may have no murmur. In that case, typically, precordial activity is increased and peripheral pulses are bounding. The increased precordial activity is caused by the large left ventricular stroke volume. Bounding pulses are caused by the relatively low systemic arterial blood pressure due to the continuous runoff of blood from the aorta into the pulmonary artery.” Medscape – VSD “The characteristic harsh, holosystolic murmur is loudest along the lower left sternal border (LSB), and it is well localized” Can’t find anything about weak pulses |
|
|
Which radiological finding is most consistent with atlantoaxial instability in a patient with rheumatoid arthritis
a. A 9mm gap between the anterior arch of C1 and the odontoid peg |
A
Atlantoaxial subluxation occurs in 25% of patients with severe RA Maxiumum gap between odontoid and arch of the atlas is 3mm - more than this is significant |
|
|
What is the most accurate method of determining fetal heart rate in a neonate
a. Palpation of an umbilical vein pulse b. Auscultation with a stethoscope c. Palpation of femoral pulse d. Pulse oximetry |
B
ARC Neonatal Resuscitation • “Heart rate can be determined by listening to the heart with a stethoscope (most reliable) or in the first few minutes after birth, by feeling for pulsations at the base of the umbilical cord” • Pulse oximetry can provide and accurate and continuous display of the heart rate within about a minute of birth” ?more accurate than auscultation |
|
|
In acute liver injury what causes the highest risk of bleeding
a. Thrombocytopenia b. Coagulopathy c. Portal hypertension d. Platelet dysfunction e. |
?B
can’t find anything on this Miller • “Perioperative hemorrhage in patients with significant liver dysfunction may occur because of bleeding diatheses or the complications of portal hypertension (or both)” • Portal hypertension → splenomegaly → thrombocytopaenia • “In patients with acute liver failure, plasmapheresis may have potential benefit because it promotes rapid correction of coagulopathy while minimizing volume overload” |
|
|
A patient in recovery post op total hip replacement develops crushing central chest pain, ECG shows ST segment elevation (NB- no BP etc given, beta blockade was not an option). The most appropriate action is to give |
A
|
|
|
Stellate ganglion blockade causes |
A Decreased Axillary sweating only with thoracic sympathetic ganglion block (around T3), not covered by Stellate Ganglion (C6-T1) |
|
|
Features of ventricular tachycardia DO NOT include
a. Absence of p waves b. Monophasic waves c. Prominent R wave in V1 d. A-V dissociation |
A |
|
|
An inpatient becomes hyponatraemic 48 hours post op and has a seizure. The most appropriate treatment is
a. Fluid restriction b. Normal saline ?ml/hr c. Hypertonic saline d. Salt tables |
C
|
|
|
A child with 10% dehydration is likely to have
a. Bradycardia b. Rapid deep breathing |
B
RCH CPG Dehydration Moderate dehydration (4-6%) • Delayed CRT (> 2 secs) • Increased respiratory rate • Mild decreased tissue turgor Severe dehydration (>/= 7%) • Very delayed CRT > 3 secs, mottled skin • Other signs of shock (tachycardia, irritable or reduced conscious level, hypotension) • Deep, acidotic breathing • Decreased tissue turgor |
|
|
When stimulating the ulnar nerve with a nerve stimulator, which muscle do you see twitch? |
C |
|
|
When analyising a study containing a control and two test groups, the best statistical method to use is.... |
A |
|
|
Acromegaly due to excess of growth hormone. Why is it difficult to do a direct laryngoscopy?
A: Distorted facial anatomy B: Macroglossia C: Glottic stenosis D: Prognathe mandible E: Arthritis of the neck |
B |
|
|
Post CEA on ward, patient seizes. BP has been hard to control. What to do to prevent further seizures?
A: Add another antihypertensive B: Start antiplatelet drugs C: Start anticonvulsants D: Do angio and stent E: Nimodipine |
A
|
|
|
Main heat loss in anaesthetic for neonate
A. vasodilatation B. radiation C. convection D. conduction E. evaporative |
B
|
|
|
Patient with aortic stenosis, the signs indicate poor prognosis
A. Palpitation B. Radiation to carotid arteries C. Paroxysmal nocturnal dyspnoea D. Angina E. Syncope |
C
Evaluation and Management of Patients With Aortic Stenosis. Circulation. 2002; 105: 1746-1750 “Survival is nearly normal until the classic symptoms of angina, syncope, or dyspnea develop.1 However, only 50% of patients who present with angina survive 5 years, whereas 50% survival is 3 years for patients who present with syncope and 2 years for patients who present with dyspnea or other manifestation of congestive heart failure” |
|
|
Circuit disconnection during spontaneous breathing anaesthesia
A. will be reliably detected by a fall in end-tidal carbon dioxide concentration B. will be detected early by the low inspired oxygen alarm C. will be most reliably detected by spirometry with minute volume alarms D. may be detected by an unexpected drop in end-tidal volatile anaesthetic agent concentration E. can be prevented by using new, single-use tubing |
D
|
|
|
Which drugs below does not need dose adjustment in renal failure patient
A. Buprenorphine B. Morphine C. Tramadol D. ? E. ? |
A
|
|
|
Fat: blood coefficient- N2O, Desflurane, Sevoflurane, Isoflurane
A. N2O ~ D > S > I B. N2O > D > S > I C. D > N2O > S > I D. N2O > D > S ~ I E . D > N2O > I > S |
D
|
|
|
The average expected depth of insertion of an oral endotracheal tube, from the lip, in a normal newborn infant is
A. 7.5 cm B. 8.5 cm C. 9.5 cm D. 10.5 cm E. 11.5 cm |
C
Rule of 6 Depth of insertion = weight + 6 Term Neonate weight ~3.5kg |
|
|
What is the average distance from the lips to carina in an average 70kg adult male?
A. 21 cm B. 23 C. 25 D. 27 E. 29 |
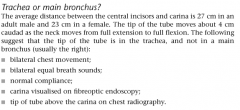
C |
|
|
Patient with severe Rheumatoid arthritis. Has C1/C2 instability. Most likely C-spine Xr finding would be
A. Anterior Atlantoodental interval >9 B. Increased sagittal diameter C. Posterior atlantodental interval >14 D. Midpart of C1 over C2 E. Tear drop sign of C2 |
A
Most common type of atlanto-axial instability is anterior AAS (80%), where C1 moves forward on C2 from destruction of transverse lig |
|
|
Which nerves need to blocked to anaesthetise the hard palate:
A. Superior labial nerve and greater palatine nerve B. Greater palatine nerve and nasopalatine nerve C. Inferior orbital nerve and nasopalatine nerve D. Glossopharyngeal nerve and… E. Anterior ethmoidal nerve and… |
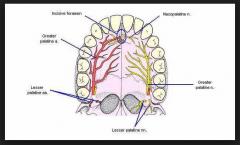
B |
|
|
Patient complains of numbness of the anterior third of his tongue following GA with LMA. Which nerve is involved?
A. Glossopharyngeal B. Facial nerve C. Superior vagus D Mandibular n. |
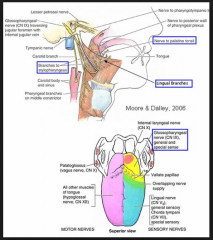
D |
|
|
Increased risk of post-partum haemorrhage in:
A. Nulliparous patient B. Patient < 20 years old C. Factor V Leiden deficiency D. Oligohydramnios E. Prolonged labour |
E
|
|
|
Chest Xray findings in a child who has inhaled a foreign body:
A. Opaque mass overlying the airway B. Hyper-expanded lung fields C. Unilateral pulmonary oedema D. Collapsed lung base E. Mediastinal shift |
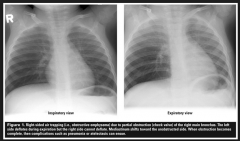
B |
|
|
Which of the following are feature of Conn’s syndrome?
A. Normoglycaemia, hypernatremia , hypokalemia B. Hypoglycaemia, hypernatremia, hypokalemia C. Hyperglycaemia, hyponatremia, hyperkalemia D. Normoglycaemia, hyponatremia, hyperkalemia E. Hypoglycaemia, hyponatremia, hyperkalemia |
A
|
|
|
Unequal consolidation on CXR can be caused by all except:
A. Pleural effusion B. Pulmonary infarction C. Pulmonary haemorrhage D. APO E. Pneumonia |
D
Nb Unilateral Pulmonary Oedema can occur with rapid reexpansion of one lung. |
|
|
What is the mechanism of central sensitisation?
A. Increased intracellular magnesium B. Antagonism of the NMDA receptor C. Glycine is the major neurotransmitter involved D. Recurrent a-delta fibre activation E. Alteration in gene expression |
E
|
|
|
What is the resus dose of atropine and adrenaline when given via ETT compared to IV
A. x 0.5 B. No change C. x 2 D. x 4 E. x 6 |
D |
|
|
A home handyman leaves his electricity turned on whilst fiddling with wires [repairing a power outlet]. He has a RCD. What happens if he touches the neutral and ground wires? |
A |
|
|
If a patient experiences parasthesia in the little finger during supraclavicular brachial plexus block, the needle is in proximity to the |
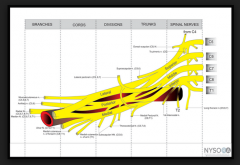
D
Supraclavicular Nerve Block performed at trunks |
|
|
What is the best predictor of severe bleeding in cirrhosis? |
A
A lot of other sites just say it is a multi-factorial process
In chronic liver disease and cirrhosis, more likely due to portal hypertension --> varices and local vascular factors rather than haemostatic factors. |
|
|
What is the dose of FFP required to increase fibrinogen levels by 1 g/L |
E |
|
|
FFP dose to increase fibrinogen by 1 mg/l
a. 10 mls/kg b. 20 mls/kg c. 30 mls/lg d. 40 mls/kg |
C |
|
|
What is the oxygen concentration in a standard bottle of heliox? |
Heliox 28% in Australia. 21% is available overseas
|
|
|
A C size oxygen cylinder (A size in New Zealand) reads 5000kPa. How much oxygen remains? |
B |
|
|
Patient undergoing partial hepatic resection develops Venous Air Embolism. Best position should be |
Left lateral to prevent air lock |
|
|
What is the ratio of compressions to breaths in neonatal resus?
A. 3:1 |
A
|
|
|
Which drug has the best evidence for reducing blood loss in trauma?
A. Aminocaproic acid B. Novo 7 C. Prothrombinex D. Tranexamic acid E. Aprotinin |
D
CRASH-2 Trial |
|
|
The pain of the first stage of labour is transmitted by:
A. Grey rami communicantes B. T10-L1 anterior roots C. The hypogastric plexus D. Inhibitory nerves to the internal vesical sphincter E. Parasympathetic nerves |
C |
|
|
You are asked by an Obstetrician to help relax a uterus in labour and deliver for manual removal of placenta. What is a safe and effective dose of IV GTN to be delivered?
A. 5 mcg B. 50 mcg C. 250 mcg D. 400 mcg E. 500 mcg |
B |
|
|
Dose of GTN IV to relax uterus?
a. 25 mcg b. 50 mcg c. 250 mcg d. 500 mcg e. 750 mcg |
B
ANZJOG Volume 37, Issue 1, pages 20–24, February 1997 : 50 - 200 mcg , 200mcg is mentioned a few places. I will check the O&G textbooks for a proper reference. --Methoxyflurane 06:45, 21 April 2012 (CDT) |
|
|
Middle-aged male with severe MS having general anaesthesia for repair of fractured ulna / radius. 10 minutes into the case you notice a tachyarrythmia with his HR 130 and BP 70. He is normally in sinus. What do you do? |
C |
|
|
The ratio of MAC to MAC Awake for sevoflurane is:
A. 0.22 B. 0.33 |
B
|
|
|
A lady with a Fontan’s circulation for tricuspid atresia presents for caesarian section. What is the best way of maintaining her cardiac output? |
D
Spontaneously breathing best with raised legs to maintain venous return.
If intubated and ventilated, shorten insp time to reduce effect of increased intrathoracic pressure on venous return. |
|
|
What is the cerebral perfusion pressure if MAP 80, CVP 5, both at the level of the RA with the tragus 13 cm above the RA?
A. 62 mmHg B. 65 C. 75 D. 80 |
B
1mmHg = 1.36cmH20 80 x 1.36 = 108.8cmH20 108.8 – 13 = 95.8cmH20 95.8/1.36 = 70.4mmHg (i.e. the MAP at level of the head) CPP = MAP-CVP CPP = 70-5 = 65mmHg |
|
|
What is the best way to measure neonatal heart rate during resus?
A. Palpate a femoral artery B. Palpate a carotid artery C. Auscultate the precordium D. Palpate the umbilical stump |
C
ARC Neonatal Resuscitation • “Heart rate can be determined by listening to the heart with a stethoscope (most reliable) or in the first few minutes after birth, by feeling for pulsations at the base of the umbilical cord” • Pulse oximetry can provide and accurate and continuous display of the heart rate within about a minute of birth” ?more accurate than auscultation |
|
|
A term primip with meconium-stained liquor has a caesarian section. On initial assessment the neonate if pale and floppy with a heart rate of 90 bpm. Initial treatment should be:
A. Positive pressure ventilation B. Dry and stimulate C. Suction the trachea D. Start CPR |
C
ARC Guidelines – Management of the Airway in the Presence of Meconium Stained Liquor • Suctioning before delivery makes no difference • Routine suctioning of babies who are vigorous no longer advocated (doesn’t improve outcomes) • No evidence to support or refute endotracheal suctioning in the non-vigorous neonate • If tracheal suctioning is performed it must be accomplished before spontaneous or assisted respirations have commenced… stimulation to breath should not be provided beforehand |
|
|
The most common clinically significant valvular lesion in pregnancy is:
A. MS B. MR C. AS D. AR E. TR |
A
|
|
|
During prolonged trendelenburg positioning there is:
A. No change in ICP B. No change in IOP C. Increased pulmonary compliance D. Increased myocardial work E. No increased pulmonary venous pressures |
D
|
|
|
How do you calculate the inspiratory time constant for lungs
A. resistance multiplied by compliance B. resistance divided by compliance C. compliance divided by resistance D. resistance minus compliance E. resistance plus compliance |
A
Lung Mechanics & Mechanical Ventilation - Lexington Pulmonary and Critical Care Mathematically, the time constant is defined as compliance multiplied by the airway resistance and the resulting value has units of seconds of time |
|
|
What is the best indicator of pending respiratory depression when using a morphine PCA
A. Respiratory rate B. Sedation score C. Reduced saturations |
B
|
|
|
A 60kg 17 year old female given 50 mg rocuronium for RSI. You can’t intubate or ventilate. What is the appropriate dose of sugammadex?
A. 300mg B. 600mg C. 920mg D. 1300mg |
C
Well actually 960mg Reversal of shallow neuromuscular = 2 mg/kg Reversal of profound neuromuscular blockade = 4 mg/kg Immediate reversal of neuromuscular blockade = 16 mg/kg |
|
|
What is the maximum dose of Intralipid during LA toxicity resus?
8ml/kg A. 10 B. 12 C. 16 |
B
Poisons Information Centre of Ireland “A recommended upper limit is 10mL/kg but no maximum dose has been established” Association of Anaesthetists Great Britain & Ireland (AAGBI) • Bolus 1.5ml/kg • Infusion 0.25ml/kg/min • Two further boluses 1.5ml/kg • Increase infusion to 0.5ml/kg/min |
|
|
What is the immediate compensation for the dilutional anaemia when 3 litres of normal saline is given at the start of a case?
A. Increased CO B. Capillary dilatation C. Increased oxygen delivery D. Right shift in the oxygen dissociation curve |
A
Though B too? Isovolaemic haemodilution leads to a decrease in [Hb]. Without a significant increase in either SaO2 or paO2 (not possible in the standard state at sea level and room air), the only way to return oxygen flux to normal is through an increase in CO. CO is a product of heart rate (HR) and stroke volume (SV), and is dependent upon preload, afterload and myocardial contractility. Increased CO occurs through several factors: 1. Decreased blood viscosity an increased tendency for venous return (VR) SV and thus CO. 2. Decreased blood viscosity SVR and afterload CO. Poiseuille's law shows resistance in a vessel is directly related to viscosity (and length, and inversely related to radius to the fourth power). 3. Metabolic Autoregulation - Local tissue factors lead to vasodilation in order to increase regional blood flow and restore oxygen delivery to normal. Increased regional blood flow tendency for VR CO. Any small decrease in systemic blood pressure (BP) due to the subsequent fall in SVR as regional circulations vasodilate, is quickly detected by the carotid and aortic baroreceptors, leading to an increased sympathetic outflow and thus increased HR, SV and subsequently CO. Increased tissue O2 extraction: Local factors independent of the increase in CO also assist in maintaining tissue oxygen supply despite a fall in oxygen flux. These adaptions occur to increase the oxygen extraction by tissues. An important mediator of this is a right-ward shift in the oxyhaemoglobin dissociation curve, increasing the p50 (normal 26.6 mmHg) and thus assisting the offloading of oxygen from Hb. Also, the lower pO2 places the tissues on a steeper position of the oxyHb dissociation curve, further facilitating oxygen unloading as greater amounts of O2 are off-loaded per unit drop in pO2 |
|
|
The following electrolytes are from an alcoholic 12 hours post laparotomy. What is the diagnosis? Na 141, K 4, Cl 114, HCO3 19
A. DKA B. Methanol C. Lactate D. NaCl resus |
D AG = 145 - 133 AG = 12 (normal anion gap) |
|
|
Alcoholic patient undergoes unremarkable anaesthesia for explorative laparotomy for investigation of abdominal pain. No pathology is found. However, in recovery the following electrolyte disturbances found: |
D |
|
|
The plasma half-life of clopidogrel is: |
A |
|
|
Isoflurane vaporiser giving 3%. What is the splitting ratio?
A. 1:3 B. 1:9 C. 1:13 D. 1:20 E. 1:27 |
C
Well, almost Dorsh & Dorsh “The ratio of bypass gas to gas going to the vaporizing chamber is called the splitting ratio and depends on the ratio of resistances in the two pathways” http://www.anesthesia2000.com/physics/Chemistry_Physics/physics17.htm Isoflurane 3% = 1:14 |
|
|
The line between the iliac crests in a neonate corresponds to: |
D |
|
|
In a neonate the main resistance in a circle system with CO2 absorber
A. APL valve B. Expiratory and inspiratory unidirectional valves C. tubing D. ETT E. HME filter |
D |
|
|
Blood flow across which of the following is used to estimate pulmonary artery pressures during echocardiography?
A. Tricuspid valve B. Pulmonary valve C. Mitral Valve |
A
|
|
|
Which patient do you not put a left-sided Robert-Shaw DLT into? |
B |
|
|
An infant born at 32 weeks gestational age comes at 6 weeks for elective bilateral inguinal hernia repair. The parents expect to take him home that day. What do you tell them? |
D |
|
|
A machine with a soda lime absorber was left on overnight with oxygen running at 6 litres per minute. In the morning a desflurane vaporiser is connected. What toxic substance may be produced? |
B |
|
|
A post-op child being given 2.5%D + 1/2NS on the ward seizes, is intubated and ventilated and transferred to ICU. Sodium is 116. What do you do? |
B |
|
|
Which is not a side effect of cyclosporine?
A. Alopecia B. Gingival hyperplasia C. Hypertension D. Renal impairment |
A |
|
|
New national labelling standards endorsed by ANZCA. What colour should the label on a subcutaneous ketamine infusion be?
A. Red B. Blue C. Beige D. Yellow E. Pink |
C
National Recommendations for User-applied Labelling of Injectable Medicines, Fluids and Lines Intra-arterial = Red Intravenous = Blue Epidural / Intrathecal / Regional = Yellow Subcutaneous = Beige 723 Other routes = Pink |
|
|
ANZCA professional documents, ketamine labels should be
A. Pink B. Green C. Grey D. Yellow E. Black |
D
National Recommendations for User-applied Labelling of Injectable Medicines, Fluids and Lines Intra-arterial = Red Intravenous = Blue Epidural / Intrathecal / Regional = Yellow Subcutaneous = Beige 723 Other routes = Pink |
|
|
Poor prognosis of AS
A. PND B. Chest pain C. Palpitation D. Syncope E. Malaise |
A
|
|
|
Required for diagnosis of Neuroleptic Malignant Syndrome
A. Diaphoresis B. ↑ CK C. Rigidity D. Hypertenion E. ↑ HR |
C |
|
|
2 yo 15kg child following seizure on surgical ward. Admitted with appendicitis and perforation. 60ml/hr of ½ N. Saline 5%dextrose
Na+ 119 K+ 4.5 HCO3- 19 Cl- 90 Best treatment would be A. Desmopressin B. Frusemide C. 3% normal saline D. Normal Saline E. Fluid restrict |
C
|
|
|
Atrial septal defect, where is the murmur heard the loadest? |
A |
|
|
Young infant with Failure to Thrive. Born on the 20th percentile now is on the 5th percentile. Found to have a systolic murmur, tachynpnoea with weak femoral pulse. The most likely diagnosis is |
A |
|
|
Myasthenia gravis, Eaton Lambert Syndrome What happens with exercise?
a. MG better, EL worse b. EL better, MG worse c. Both EL and MG get worse d. Both EL and MG get better |
B
|
|
|
Cephalothin doesn't cover:
a. Proteus b. E coli c. Staph d. Strep e. Pseudomonas |
E
|
|
|
Regarding PS9 safe provision of anaesthesia for Colonoscopy: |
A |
|
|
You see a man in his 60s in clinic 1 week prior to laparoscopic cholecystectomy. He has dilated cardiomyopathy with an ejection fraction of 30%, but does not get dyspnoeic with normal activities of daily living. What is the most appropriate management of his heart failure? |
C |
|
|
Young child with WPW undergoes general anaesthesia. Intra operatively developed tachycardia. HR 220, BP 80/40. Best drug to cardiovert |
B
|
|
|
Finding on haemophilia A patient
A. Female haemarthrosis B. Male haemarthrosis C. Normal PT, abnormal APTT D. Abnormal PT, normal APTT |
C
|
|
|
32 y/o male. Weakness distal and prox muscles, infection 10 days ago, no sensory involvement, temp 37.8, facial weakness. Cause:
A. Guillian Barre B. Myasthenia Gravis D. Poliomyelitis E. ?Acute encephalitis F. ?Polymyositis |
A
|
|
|
What gestation to monitor uteroplacental flow
A 20 weeks B 24 weeks C 28 weeks D 32 weeks E 36 weeks |
B
|
|
|
Cause of hypoxia in 1 lung ventilation?
A Blood to non-ventilated lung B V/Q mismatch in ventilated lung C ?hypoxic pulm vasoconstriction |
A
|
|
|
Endocarditis prophylaxis
A Bicuspid valve B Congenital repair > 12 months ago C Rheumatic heart valve D Uncorrected cyanotic heart disease E MVP + ?MR |
D
|
|
|
Area burnt in adult male - upper half of upper limb, anterior abdo, whole left leg:
A 23% [changed figure compared to prev years] B 32% |
B
Around 31.5% according to rule of 9’s technique (i.e 4.5 upper arm, 9 ant abdo, 18 whole leg) |
|
|
Best position for tip of IABP is 1-2 cm:
A Distal to Left subclavian artery B Proximal to Left subclavian artery |
A
|
|
|
VT features:
A monophasic V6 B QRS > 0.14 C Right axis deviation |
B
|
|
|
70 y/o postop in recovery following hip surgery. Develops severe chest pain, ST elevation. Immediate mx:
A Beta blocker B Aspirin C GTN infusion D Heparin infusion |
B
|
|
|
The muscles of the upper eyelid receive a somatic nerve |
B |
|
|
A line isolation monitor protects against microshock
A. only if the warning current is set at 10mA B. only if the warning current is set at 30mA C. under no circumstances D. only if the equipment used is grounded E. only if it monitors all the equipment in the region |
C
|
|
|
The commonest initial presenting feature in anaphylaxis is
A. coughing B. desaturation C. hypotension D. rash E. wheeze |
C
|
|
|
Following a left sided pneumonectomy, a left intercostal drain is placed and connected to an underwater drainage system. In the postoperative period: |
E
|
|
|
Most safe side to insert subtenon block |
A |
|
|
Levosimendin: |
C |
|
|
During scoliosis surgery with monitoring of somatosensory evoked potentials, which tract are they mainly monitoring? |
A |
|
|
What is the major cause of death in a patient with perforation of the pharynx, oesophagus or trachea? |
C
|
|
|
You are asked to see a 60-year-old male 2 days following a cervical laminectomy because he has new neurological symptoms in his right arm. The surgical team think these may be due to poor patient positioning. The sign that would most help differentiate a C8-T1 nerve root injury from an ulnar nerve injury is |
D |
|
|
An infant is anaesthetised and ventilated using an endotracheal tube and circle breathing system with CO2 absorber. The item which causes the most resistance to breathing is the |
C
|
|
|
When stimulating the ulnar nerve with a nerve stimulator, which muscle do you see twitch?
A. opponens abducens B. abductor pollicis brevis C. adductor pollicis brevis D. extensor pollicis E. flexor pollicis brevis |
C |
|
|
In congenital diaphragmatic hernia |
A |
|
|
What will not increase A-a gradient
a. decreased cardiac output b.. Increased FiO2 c. Decreased FiO2 d. increased shunt |
C
|
|
|
Wolf Parkinson White Syndrome:
a. PR interval lenghtened b. [Something about delta wave] c. DCR is less effective d. Central IV access may precipitate arrythmias |
D |