![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
62 Cards in this Set
- Front
- Back
|
Mood disorders |
Psychological disorders characterized by prolonged and marked disturbances in mood that affect how people feel, what they believe and expect, how they think and talk, and how they interact with others. |
|
|
DSM-5 distinguishes between two categories of mood disorders: |
depressive disorders and bipolar and related disorders. |
|
|
DSM-5 defines three types of mood episodes as the foundations of mood disorders: |
major depressive episode, manic episode, and hypomanic episode (seeTABLE 5.1). |
|
|
Anhedonia |
A difficulty or inability to experience pleasure. |
|
|
Behavioral and Physical Symptoms of Depression |
more negative comments, make less eye contact, are less responsive, speak more softly, and speak in shorter sentences than people who are not depressed
|
|
|
vegetative signs |
Psychomotor retardation, along with changes in appetite, weight, and sleep, are classified as |
|
|
Hypersomnia |
should already know this |
|
|
depression is heterogeneous, how |
depression is heterogeneous, which means that people with depression experience these symptoms in different combinations. |
|
|
two types of depression: |
typical depression, people develop insomnia, lose weight, and their poor mood persists throughout the day, |
|
|
Prodrome |
A Prodrome is the early symptoms of a disorder or an episode, and the prodrome of an MDE may include anxiety or mild depressive symptoms that last weeks to months before fully emerging as a major depressive episode. |
|
|
Premorbid |
Referring to the period of time prior to a patient’s illness. |
|
|
What distinguishes depression from simply “having the blues”? |
#of symptoms |
|
|
“bereavement exclusion.” |
exclusion of ppl who grieve over a loved one, applies to dsm4, included in dsm 5 |
|
|
recurrent depression |
More than half of those who have had a single depressive episode go on to have at least one additional episode, noted as ... |
|
|
presenteeism |
being present but being less productive than normal |
|
|
seasonal affective disorder, variant of MDD |
Surveys find that approximately 4–6% of the general population experiences a winter depression, and the average age of onset is 23 years. The disorder is four times more common in women than in men |
|
|
Phototherapy (also called light-box therapy), |
reatment for depression that uses full-spectrum lights; also calledlight-box therapy |
|
|
Age cohort |
A group of people born in a particular range of years. |
|
|
peripartum onset |
In some cases, such as that of Marie Osmond in Case 5.2, depression emerges during pregnancy or within 4 weeks of giving birth |
|
|
Persistent depressive disorder |
(dysthymia), characterized by depressed mood and as few as two unknown. In addition, other depressive symptoms that last for at least 2 years and that do not recede for longer than 2 months at any time during that period |
|
|
Disruptive Mood Dysregulation Disorder |
is a depressive disorder in children characterized by persistent irritability and frequent episodes of out-of-control behavior. |
|
|
stress–diathesis model of depression |
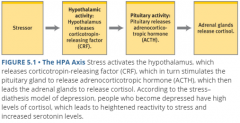
focuses on a part of the brain involved in the fight-or-flight response, the hypothalamic–pituitary–adrenal axis (HPA axis). Ppl with depression have higher amts of cortisol which makes them more reactive. |
|
|
negative triad of depression. |
Beck (1967) has suggested that people with depression tend to have overly negative views about: (1) the world, (2) the self, and (3) the future, |
|
|
internal attributional style |
People who consistently attribute negative events to their own qualities |
|
|
Three particular aspects of attributions are related to depression: |
whether the attributions are: stable (enduring causes) or unstable (local, transient causes), and People who tend to attribute negative events to internal, stable, and global factors have a negative attributional style |
|
|
attachment styles |
Secure attachment. Adults with this style generally display a positive relationship style. Avoidant attachment. Adults with this style are emotionally distant from others. Anxious-ambivalent attachment. Adults with this style chronically worry about their relationships. |
|
|
girls 2wice as likely to have depression vs. guys, why? 4 pts. |
-socialization of body dissatisfaction |
|
|
James Coyne’s interactional theory of depression |
someone who is neurologically vulnerable to depression (perhaps because of genes or neurotransmitter abnormalities) may, through verbal and nonverbal behaviors (psychological factor), alienate people who would otherwise be supportive (social factor |
|
|
Selective serotonin reuptake inhibitors |
SSRIs slow the reuptake of serotonin from synapses. Because these antidepressants affect only certain receptors, they have fewer side effects than other types of antidepressant medications, which can make people less likely to stop taking them |
|
|
Tricyclic antidepressants (TCAs), |
ed since the 1950s to treat depression and, until SSRIs became available, The side effects of TCAs differ from those of SSRIs: The most common side effects include low blood pressure, blurred vision, dry mouth, and constipation most common before SSRI's |
|
|
Monoamine oxidase inhibitors (MAOIs) |
Antidepressant medications that increase the amount of monoamine neurotransmitter in synapses. |
|
|
ECT electroconvulsive therapy |
A procedure that sends electrical pulses into the brain to cause a controlled brain seizure, in an effort to reduce or eliminate the symptoms of certain psychological disorders. ECT may be used when a patient: (1) has severe depression that has not improved significantly with either medication or psychotherapy, (2) cannot take medication because of side effects or other medical reasons, or (3) has a psychotic depression (depression with psychotic features) that does not respond to medication |
|
|
transcranial magnetic stimulation. |
A procedure that sends sequences of short, strong magnetic pulses into the brain via a coil placed on the scalp, which is used to reduce or eliminate the symptoms of certain psychological disorders. |
|
|
Behavior therapy , 2 ideas. (social learning) |
The form of treatment that rests on the ideas that: (1) maladaptive behaviors stem from previous learning, and (2) new learning can allow patients to develop more adaptive behaviors, which in turn can change cognitions and emotions. such methods focus on the ABCs of an unwanted behavior pattern:the antecedents of the behavior (the stimuli that trigger the behavior),the behavior itself, and the consequences of the behavior (which may reinforce the behavior). |
|
|
behavioral activation-how do you change behavior? What methods? |
Specific techniques to change such behaviors These techniques include self-monitoring (keeping logs of activities, thoughts, or behaviors), scheduling daily activities that lead to pleasure or a sense of mastery, and identifying and decreasing avoidant behaviors. |
|
|
Cognitive therapy |
The form of treatment that rests on the ideas that: (1) mental contents influence feelings and behavior; (2) irrational thoughts and incorrect beliefs lead to psychological problems; and (3) correcting such thoughts and beliefs will therefore lead to better mood and more adaptive behavior. |
|
|
cognitive restructuring, |
=behavioral activation |
|
|
Cognitive-Behavior Therapy |
The form of treatment that combines methods from cognitive and behavior therapies. CBT, particularly when it includes behavioral activation, is often about as successful as medication |
|
|
Interpersonal therapy (IPT) |
The form of treatment that is intended to improve the patient’s skills in relationships so that they become more satisfying. |
|
|
Systems therapy (family) |
Systems therapy is guided by the view that when one member changes (perhaps through therapy), change is forced on the rest of the system |
|
|
Diagnoses of bipolar disorders are based on three types of mood episodes. |
major depressive episode (which underlies MDD), manic episode, and hypomanic episode |
|
|
Manic episode |
A period of at least 1 week characterized by abnormally increased energy or activity and abnormal and persistent euphoria or expansive mood or irritability. |
|
|
Expansive mood |
A mood that involves unceasing, indiscriminate enthusiasm for interpersonal or sexual interactions or for projects. |
|
|
Flight of ideas |
thoughts that race faster than they can be said.something like watching two or three television programs simultaneously. |
|
|
hypomanic vs. manic |
same criteria as a manic episode, with two significant differences: the symptoms (1) don’t impair functioning, require hospitalization, or have psychotic features; and (2) they last a minimum of 4 days, not 1 week. Hypomania rarely includes the flight of ideas that bedevils someone in the grips of mania during hypomanic episodes people are uncritically self-confident but not grandiose. |
|
|
cyclothymia |
is characterized by symptoms of hypomania and depression that do not meet the criteria for either of the two types of bipolar disorder. cyclothymia is a more chronic but less intense version of bipolar II disorder - The main feature of Cyclothymic disorder is a chronic, fluctuating mood disturbance with numerous periods of hypomanic symptoms that alternate with depressive symptoms, each of which does not meet the criteria for its respective mood episodes. -These symptoms have been present for at least half of the time within a 2-year period and have not completely disappeared for more than 2 consecutive months |
|
|
bipolar I disorder vs. bipolar II disorder |
The types differ in the severity of the manic symptoms. To receive the diagnosis of the more severe bipolar I disorder, a person must have a manic episode; an MDE may also occur with bipolar I. Thus, just as an MDE automatically leads to a diagnosis of MDD, having a manic episode automatically leads to a diagnosis of bipolar I. manic episode=1week to be diagnosed with bipolar II disorder, a person must alternate between hypomanic episodes and MDEs |
|
|
rapid cycling |
Having four or more episodes that meet the criteria for any type of mood episode within 1 year. |
|
|
Fig. 5.4 Symptoms->disorder |

|
|
|
What neurological substructure is associated with bipolar? |
finding that the amygdala is enlarged in people who have been diagnosed with a bipolar disorder (Altshuler et al., 1998). Researchers have also found that the amygdala is more active in people who are experiencing a manic episode than it is in a control group of people who are not manic (Altshuler et al., 2005). |
|
|
neurotransmitters related to bipolar? |
There’s reason to believe that serotonin (Goodwin & Jamison, 1990) and norepinephrine have roles in bipolar disorders. For example, treatment with lithium (discussed shortly) not only lowers norepinephrine levels but also reduces the symptoms of a bipolar disorder (Rosenbaum, Arana, et al., 2005). |
|
|
neural communication/brainsystem of a manic patient |
researchers have also reported that the left frontal lobes of patients with mania produce too much of the excitatory neurotransmitter glutamate (Michael et al., 2003), |
|
|
twin studies of bipolar? |
If one monozygotic twin has a bipolar disorder, the co-twin has a 40–70% chance of developing the disorder if one dizygotic twin has the disorder, the co-twin has only about a 5% chance of developing the disorder, which is still over twice the prevalence in the population |
|
|
twin studies of general mood disorders w/ relation to genetics, i.e. Gene -> mood / bipolar even tho they're distinct disorders |
When a dizygotic twin has a bipolar disorder, the other twin has an 80% chance of developing any mood disorder |
|
|
what happens after a manic episode? |
Even after a mood episode is over, residual problems with cognitive functioning—which affect problem solving, planning, or decision making—can adversely influence the work and social life of a person with a bipolar disorder. -lower cognitive functioning, i.e. memory/executive functions |
|
|
Mood stabilizer |
A category of medication that minimizes mood swings. (The term mood stabilizer is sometimes used more broadly to include medications that decrease impulsive behavior and violent aggression.) Lithium; coordination problems, vomiting, muscular weakness, blurred vision, and ringing in the ears; |
|
|
interpersonal and social rhythm therapy(IPSRT |
As in IPT, IPSRT sessions focus on identifying themes of social stressors, such as a relationship conflict that arises because partners have different expectations of the relationship. IPSRT focuses on the timing of events (such as arranging weekend activities so that the patient wakes up at the same time each morning and goes to sleep at the same time each night |
|
|
Suicidal ideation |
Thoughts of suicide. |
|
|
The three most common types of disorders among those who commit suicide are (Brown et al., 2000; Duberstein & Con-well, 1997; Isometsä, 2000; Moscicki, 2001): |
major depressive disorder (50%), |
|
|
Bielau and colleagues (2005) theory |
reported a suggestive trend: People who committed suicide tended to have fewer neurons in the part of the brain that produces serotonin than did people who died of other causes |
|
|
long term suicide prevention 4 suggestions |
Thus, programs to prevent child abuse, to provide affordable access to mental health care (and so make it easier to obtain treatment for psychological disorders, in particular depression), to decrease substance abuse, and to increase employment may all help prevent suicides in the long term. |
|
|
Deliberate but nonlethal self-harming suicide attempts are referred to as _____ behavior. |
parasuicidal |