![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
253 Cards in this Set
- Front
- Back
|
What is the NT-pro-BNP assay |
B-typenatriuretic peptide (BNP) is a prohormone secreted from atrial and ventricularmyocardial cells in response to increased plasma volume, vasoconstriction, andactivation of RAAS - hormone released as result of of cells being stretched |
|
|
What is the NT-pro-BNP assay most helpful for? |
-Helpful with catsin determining benign vs pathologic murmurs - **Useful in discerning if dyspneicpatient is due to primary respiratory disease or cardiac |
|
|
Why is congenital heart disease important even though it only makes up <1% of cases |
important to not breed animals with congenital heart disease and to no longer breed the pair of parents that created the affected offspring as well |
|
|
what are the 3 most common congenital heart diseases of dogs |
•Aortic stenosis (AS) •Pulmonic stenosis (PS) •Patent Ductus Arteriosus (PDA) |
|
|
What is the most common congenital heart disease in cats? |
•atrioventricular (AV) septal defects(including ventricular septal defect, atrial septal defect) •AV valve dysplasia •endocardial fibroelastosis •PDA •aortic stenosis •Tetralogy of Fallot |
|
|
What are the most common congenital heart diseases of large animals? |
•cattle—ventricular septal defect, ectopicheart, and ventricular hypoplasia •sheep—ventricular septaldefect •pigs—tricuspid valvedysplasia, atrial septal defect, and subaortic stenosis •horses—ventricular septaldefect, PDA, tetralogy of Fallot, and tricuspid atresia. |
|
|
What breed of horse is particularly susceptible to congenital heart disease |
Arabian horses |
|
|
what are clinical signs of congenital heart disease |
•Failure to grow •Dyspnea •Weakness •Syncope •Cyanosis •Seizures •Sudden death |
|
|
what are causes of congenital heart disease |
•Genetic •Environmental •Infectious •Nutritional •Drug related |
|
|
What is PatentDuctus Arteriosus? |
•Ductus arteriosus fails to close duringparturition •Blood is shunted from systemiccirculation to the pulmonary artery •Normally closes 12-14 hours after birth •Left side volume overload |
|
|
What is the best diagnostic tool for a PDA? what is treatment? |
Echo Tx: surgery to ligate vessel, good prognosis with surgery |
|
|
what are Atrialand Ventricular Septal Defects |
•Openings in septa allow right-to-leftshunting in fetus •Openings fail to close properly •Atrial septal defect shunts left to right= R side overload •Ventricular septal defects shunt = left side overload and enlargement |
|
|
How do you treat Atrialand Ventricular Septal Defects |
surgical closure of the opening in the septa, treatment of CHF |
|
|
what is pulmonary stenosis |
•pulmonic valves are dysplastic ormalformed -outflow tract from the right ventricleis narrowed -increased ventricular systolic pressure -rightventricular hypertrophy and right atrial enlargement. -In severe cases cardiacoutput is limited during exercise |
|
|
what are clinical signs of pulmonary stenosis |
•Older than 1 year •Syncope •Tiring with exercise •Right sided heart disease •Jugular pulse •Left base murmur |
|
|
what is the best diagnostic tool for pulmonary stenosis and how do you treat? |
dx: echo tx: Balloon valvoplasty (stretch valve open), Valvulectomy or valvulotomy toopen the outflowtract, Medial management of CHF |
|
|
what is aortic stenosis |
•SAS = subaortic stenosis •Thickening of endocardial tissue justbelow the aortic valve •Obstruction to left ventricular outflow = left ventricular hypertrophy and aorticdilation •May affect coronary artery circulation •Severe disease can lead to left-sided CHFor sudden death |
|
|
what are clinical signs of aortic stenosis |
•Soft to moderate ejection murmur 4th left ICS -Tiring with exertion •Syncope •Left CHF •Sudden death |
|
|
how do you treat aortic stenosis |
•Restrict exercise •Balloon catheter dilation •Atenolol for pressures |
|
|
what are the four Tetralogyof Fallot ? |
-genetically transmitted heart malformation involving 4 heart defects: 1.PulmonicStenosis with 2.2° rightventricular hypertrophy 3.Subaortic VSD 4.Overridingaorta •Combination results in right-to-leftshunting •Deoxygenated blood from RV enters VSD andmixes with LV blood |
|
|
what are clinical signs of tetralogy of fallot |
•Failure to grow •Hypoxemia / cyanosis •Exercise intolerance; shortness of breath •Weakness •Syncope •Seizures •Sudden death •Adverse response tosedatives/tranquilizers |
|
|
What is treatment for tetralogy of fallot |
•Surgical: Create a systemic to pulmonary shunt•Medical: Phlebotomy – keep PCV 62-68% and replacewith crystalloids, Cage rest, oxygen |
|
|
what is persistent right aortic arch? |
PRAA •Persistence of the right 4th aortic arch •Constricts the esophagus, so once pups begin eating solid food, they regurgitate (megaesophagus) |
|
|
what are clinical signs of persistent right aortic arch and how is it diagnosed |
-regurgitation of solid food at weaning - aspiration pneumonia - weight loss -diagnosed with barium swallow or fluoroscopy |
|
|
what is the sinoatrial (SA) node |
pacemaker of the heart |
|
|
what is the atrioventicular (AV) node |
ventricular myocardium is electrically separated from atrial myocardium |
|
|
what is the impulse conduction through the heart |
-SA node in right atrium initiates impulse -AV node -downbundle of His; left and right branches -thruventricular muscle via Purkinje fibers |
|
|
how are myocardial cells connected |
viaintercalated discs which allows rapid transmission of impulses throughout wholemyocardium |
|
|
what are cardiac arrhythmias |
•Deviations from the normal heart raterhythm or rhythms originating from abnormal locations •May be no abnormal visible anatomicpathology |
|
|
why do arrhythmias occur |
1.Abnormalimpulse formation: ischemia, Hypocalcemia or hypercalcemia,Cardiomyopathy, Excess catecholamines, Reperfusion injury2.Abnormalimpulse conduction: Development of abnormal depolarizationpathways **or both** |
|
|
What are the different arrhythmias and what causes them? |
•Increasedexcitability:tachycardia or extrasystole •Reducedexcitability: bradicardia orasystole •Conductiondisturbance: blocks to different degrees |
|
|
when are arrhythmias an emergency? |
•Depress cardiac output: circulatory collapse or heart failure •Cardiac and non-cardiac disease •Detect and treat underlying disease iscrucial |
|
|
do arrhythmias always need to be treated? why? |
•Depends upon hemodynamic status
•Weak peripheral pulse, pale mucousmembranes, prolonged crt •Clinical signs •Weakness, collapse, exercise intolerance •Malignancy •Dangerous heart rate, frequency (treatment goal is to treat underlying disease) |
|
|
how much do arrhythmias affect hemodynamics and decrease cerebral blood flow |
8-75% |
|
|
many arrhythmias can be asculted and confirmed by.... |
ECG/EKG |
|
|
the sites of problems for arrhythmias are either
|
supraventricular (above the ventricles-atria) ventricular |
|
|
what are supraventricular arrhythmias? |
•Supraventricular Arrhythmias •Supraventricular tachycardia (SVT) •Atrial premature contractions (APC) •Atrial fibrillation (AF) “a-fib” (emergency) QRScomplexes appear normal…..problemis with the p wave |
|
|
what is supra ventricular tachycardia |
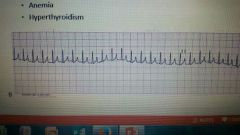
- high HR exceeds 160-180in the dog -p-qrs-t complexes are normal -causes: fear, excitement, exercise, anemia, hyperthyroidism |
|
|
what are atrial premature contractions (apcs) |

-HR normal - P wave occurs earlier than normal, impulse originates from other than SA node followed by normal QRS - asymptomatic, may hear heart sound or palpate pulse deficit - may progress to a fibb -causes: LA enlargement, atrial disease, electrolyte imbalance, drug rx |
|
|
what is atrial fibrillation? |
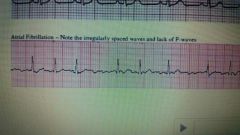
•Occurs when there is no organized atrialcontraction •Cardiac output declines •No atrial push and rapid heart rate>180 bpm dog; >240 bpm cat •Irregular rhythm •No P waves – small fibrillatorywaves instead •Causes: Enlarged hearts |
|
|
what are the 3 signs an EKG is in a-fib |
-tachycardia - no p wave - irregular rhythm |
|
|
Clinical signs of a-fib |
- weakness, syncope - cat-dyspnea - collapse - rapid, irregular HR ***calcium channel blockers to treat*** |
|
|
what are ventricular arrhythmias |
- ventricular tachycardia - ventricular fibrillation - impulse originates in the ventricles instead of the SA node of the atrium -QRS waves are wide and bizarre andmay not be associated with the P-wave |
|
|
what is ventricular tachycardia? |
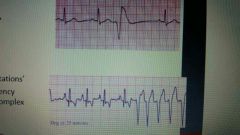
•Impulse originates from somewhere inventricle NOT in response to atrial impulse =ventricular premature contraction (VPC) •Wave is wide and bizzare •Can be isolated with relatively normal HR •Can be in runs •Decreased fill time=decreasedcardiac output •May progress to ventricular fibrillation |
|
|
what are clinical signs of v-tach |
-weakness, collapse, syncope - sudden death - CHF |
|
|
when do you treat v-tach |
- > 25 vpc per min - HR > 130 per min - at-risk breed - if clinical symptoms exist |
|
|
what is ventricular fibrillation |
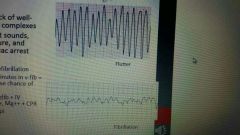
•Complete lack of well-defined QRScomplexes •Lack of heart sounds, blood pressure, andpulse = cardiac arrest |
|
|
How do you treat v-fib |
-electrical defibrillation - IV amiodarone - CPR - low dose epinephrine |
|
|
what are brady arrhythmias and which two are emergency situations? |
•HR <60 bpm dog; < 160 bpm cat inclinic •Emergency situation:Third degree AV block, Sick Sinus Syndrome |
|
|
what is sick sinus syndrome? |
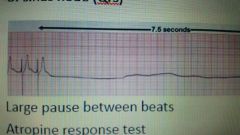
•Degeneration of conduction system •Sinus node dysfunction •Characterized by episodes of bradycardia(sinus arrest, AVB) •May be accompanied by short burst of SVT •Marked bradycardia leads to syncope •**High anesthetic risk - pause between HR complexes |
|
|
How do you treat bradycardias |
pacemaker |
|
|
what is 3rd degree av block |
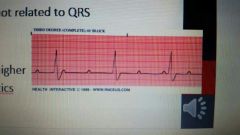
•Lack of relationship between Pwaves and QRS-T •Pathology of AV node or Bundle of His •QRS-T originate from ventricle •Medium-high risk of sudden death EKG: ventricular escape rhythm |
|
|
what is a disease associated with 3rd degree av block |
lyme disease (inflammation) |
|
|
what makes up the upper respiratory tract |
•Nasal cavity •Sinuses •Nasopharynx •Larynx |
|
|
what makes up the lower respiratory tract |
•Trachea •Bronchi •Lungs •Pleural cavity |
|
|
what are some upper respiratory diseases |
•Rhinitis •Nasal tumors •Epistaxis •Sinusitis •Tonsillitis •Laryngitis •Laryngeal paralysis |
|
|
What is rhinitis |
inflammation of the nasal cavity |
|
|
what are some causes (etiology) of rhinitis |
•Tooth root abscess •Viruses •Fungal:Aspergillus, Cryptococcus,Penicillin •Parasites: mites •Idiopathic inflammatoryrhinitis •Inflammatory polyp(cats) •Congenital abnormalities: cleft palate or primary ciliary dyskinesia •Foreign body: plantmaterial, awns •Allergicrhinitis •*Neoplasia – lymphoma,adenocarcinoma •Bacteria e.g. Bordetella |
|
|
What are the viruses that cause rhinitis in cats and dogs most commonly |
Feline: herpesvirus-I,calicivirus,chlamydia 90% rhinitis canine: distemper |
|
|
what are the two types of idiopathic rhinitis diseases |
lymphocytic plasmacyticrhinitis and chronic rhinosinusitis |
|
|
what happens with chronic rhinitis |
turbinate destruction and erosion of the mucosa |
|
|
what are the 3 types of nasal discharge and what are the terms used to define the sides it affects? |
serous, mucoid, mucopurulent unilateral, bilateral (both sides) |
|
|
if you have acute, unilateral nasal discharge what is your immediate suspicion |
foreign body |
|
|
what are signs of chronic rhinitis |
intermittent sneezing nasal depigmentation |
|
|
how do you diagnose rhinitis? |
-history, clinical signs - cult. and sens.: nasal sample, cytology - anesthesia: nasopharygeal exam, rhinoscopy, rads, CT, MRI, biopsy - nasal flush (foreign bodies, nasal plug) - periodontal probing - Secondary test: FeLV, FIV |
|
|
how do you treat rhinitis |
- treat underlying disease - cleanse nares - antimicorbials: if secondary bacteria infection - occasionally topical vasoconstrictive drugs: phenylephrine, ephedrine, can be irritating |
|
|
what are nasal tumors |
•Can occur in nasal passages or sinuses ofdogs and cats of all ages •Most are malignant (75-80%) Etiology: Dog: squamous cell carcinoma &adenocarcinoma > sarcomas Cat: lymphoma |
|
|
Possible causes of nasal tumors |
- predisposition:docliocephalic dogs - environmental exposure:tobacco - indoor coal or kerosene heater |
|
|
clinical signs of nasal tumors |
- unilateral or bilateral nasal discharge - sneezing, dypsnea, stertor, facial distortion, ocular discharge - dyspnea if obstructed |
|
|
more rostral tumors mean what |
unilateral, unless there is erosion into the other side |
|
|
more caudal tumors mean what |
bilateral even if unilateral in location since nares converge in rear of nasal passages |
|
|
how do you diagnose nasal tumor |
-rads - MRI & CT - rhinoscopy - nasopharyngoscopy - biopsy and histopathy for definitive diagnosis |
|
|
how do you treat nasal tumors |
- radiation (tx of choice) - surgery (no effective) - chemotherapy (no effective by itself, good with radiation) - supportive care (piroxicam-needs more study) |
|
|
what does epistaxis mean? |
bleeding from the nose |
|
|
what are some causes of epistaxis? |
- coagulopathys - local: trauma, fungal, bacterial, tumor |
|
|
what is sinusitis? |
inflammation of the sinuses - can be viral, bacterial, neoplasia - can be caused by dental disease and tooth root abscess |
|
|
what are clinical signs of sinusitis? what are diagnostic tools? treatment? |
- tooth root abscess (swelling under eye) , unilateral nasal discharge - rads, CT, dental exam, rhinoscopy, biopsy if mass -dental will treat if tooth root abscess, antibiotics to help before procedure for comfort |
|
|
what is tonsillitis? causes?clinical signs? diagnostic tool? treatment? |
- inflammation of the tonsils - infection, neoplasia - anorexia, salivation, pain in mouth - exam, history - antibiotics, soft food, sucrulfate (to coat), pain meds |
|
|
what is laryngitis? causes? signs? diagnosis? |
-inflammation of the larynx (acute or chronic) - allergies, aspiration, viruses, bacteria, chemical/smoke inhalation, excessive vocalization - inflammation/irratation of larynx, voice change, inspiratory effort increased, laryngospasm from swelling and edema - visualize tissue (anestetize patient), biopsy - treat underlying cause, debulk (mass), tracheostomy, glucocorticoids |
|
|
what is laryngeal paralysis? |
Failure of laryngeal musculature toproperly open and close the arytenoid cartilages |
|
|
what is GOLPP |
geriatriconset laryngeal paralysis and polyneuropathy |
|
|
what is laryngeal paralysis called in horses |
roaring |
|
|
Causes of lar par? |
- genetic/hereditary, iatrogenic (surgery), idiopathic (most common), myasthenia gravis, neoplasia, poly neuropathy, trauma |
|
|
what is the difference between lar par and GOLPP |
GOLPP also has appendicular weakness, dysphagia due to generalized neuropathy |
|
|
Treatment for larpar or GOLPP |
- use harness, avoid heat/humidity, tranquilize, doxopin (in study), in emergency: intubate, tracheostomy, sedation, steroids, oxygen - surgery for permanent treatment (tie back one side of arytenoid cartillages |
|
|
what are some diseases of the lower respiratory tract? |
- kennel cough - canine influenza - collapsing trachea - feline asthma - chronic bronchitis - heartworm disease (dogs & cats) - neoplasia - infectious (fungal/viral) |
|
|
what is infectious tracheobronchitis |
- kennel cough - highly contagious - involves multiple infectious agents (virus, bacteria, fungal) - predispostion: crowding, unsanitary conditions |
|
|
what is the difference between the mild and severe form of infectious tracheobronchitis |
- mild: accute onset of cough, fever, lethargy, inappetence not present, cough may last a week - severe: immunocompromised and puppies or other resp dz, bronchopneumonia, coughing, distress, anorexia, fever, depression |
|
|
what is the pathophysiology of infectious tracheobronchitis |
- virus may be initial invader w/ secondary bacteria - bordetella can attach and invade without co-infection, attach to cillia of bronchial epithelium and interfere with motility, also endotoxins and exotoxins - CPIV: few signs - CAV-2: mild, short acting |
|
|
what are clinical signs of infectious tracheobronchitis? |
- 4-10 days after exposure - coughing, +/- nasal discharge, gag and retch - anorexia, depression, fever - cough may become chronic due to damaged epithelium - bordetella organisms can persist 8-14 weeks |
|
|
how do you diagnose and treat infectious tracheobronchitis? |
- clinical signs/ history - tracheal/ bronchial wash - others: CBC, Rads, virus isolation, blood gas - treat: mild (self limiting, give supportive care), severe (systemic antibiotics, nebulized antibiotics, supportive), other: anti-tussives, glucocorticoids (decrease inflammation), bronchodilators |
|
|
with what form of infectious tracheobronchitis do you want to avoid cough suppressants?
|
the severe form, want a productive cough to remove bacteria and such
|
|
|
Canine influenza (CIV) (etiology, predisposition, transmission, pathophysiology) |
Etiology: H3N8/H3N2 Predisposition: Worldwide, dogs, some crossover to cats/ferrets, young and older moreseverity, Crowding, immunosuppressive drugs Transmission: aerosols, fomites, direct contact, occurs withinhours Pathophysiology: Virus replicates exclusively inepithelial cells lining respiratory tract, can take weeks to resolve (chronic coug) |
|
|
What percentage of dogs with respiratory disease where positive for H3N2? |
11% |
|
|
clinical signs of CIV |
May be clinically normal Severity variable, typically self-limiting and mild Mild cough, anorexia, lethargy, sneezing,nasal discharge, +/- dyspnea Low grade fever Cough persists 10-14 days, dry,non-productive Persistence may indicate pneumonia(tachypnea, dyspnea, crackles) |
|
|
What is the more severe strain of CIV |
H3N2 |
|
|
CIV diagnosis and treatment |
Diagnose: Sample from nasal, nasopharyngeal, ororopharyngeal , Lung tissue (necropsy), Acute and convalescent titers Other: CBC: leukocytosis with left shift (pneumonia), +/- tracheal or bronchial wash, Rads |
|
|
FelineInfluenza and Bordetella
|
•Cats can get Bordetella: Self-limiting in healthy patient, More severe in young or immunecompromised •Cats can get CIV: H7N2 avian influenza outbreak right nowin NYC shelters, somewhat rare |
|
|
Collapsing trachea |
Etiology/Pathophysiology: Decreased glycoprotein andglycosaminoglycan (Lose firmness, Collapses during resp) Progressive Clinical Signs: harsh, dry cough “goose honk”, Worse w/ excitement/exercise, heart disease Diagnosis: Rads, Bronchoscopy, Fluoroscopy Treatment: Symptomatic ( tranquilizers, O2, Glucocorticoids, Antitussives, Bronchodilators Surgical: External rings, Internal mesh stent |
|
|
Feline asthma (predispostion and etiology) |
Allergic bronchitis (type I) Predispostion: Siamese; 1-11 years of age (5.5y)Etiology/Pathophysiology: IgE mediated hypersensitivity, eosinophil and mast cell involvement, inflammation,mucous hypersecretion, bronchoconstriction, smooth muscle spasm, vascularleakage, and airway remodeling |
|
|
Feline asthma (signs, diagnosis, treatment) |
Clinical Signs: intermittent or seasonal, acute respiratory distress, Coughing, dyspnea, wheeze tachypnea, inspiratoryrattle Diagnosis: CBC: eosinophilia andhyperproteinemia, Rads (interstitial pattern, donuts,, hyperinflation / flattened diaphragm, heartworm, Baermann, NT-proBNP, Mycoplasma Treatment: Acute (Terbutaline IV, Dexamethasone, O2, Albuterol) Chronic(prednisolone Bronchodilators, inhaled steroids) |
|
|
what disease is a irreversible, slowly progressive inflammation of the bronchial mucosa, with coughing. Also can be initially infective as a bacteria or fungus, also sometimes associated with a foreign body |
chronic bronchitis (K9)
|
|
|
what are clinical signs of chronic bronchitis |
Cough worse with exercise, excitement, and uponwaking Exercise intolerance Increased effort for perceived level ofexertion +/- Concurrent obesity +/- Concurrent heart murmurs Crackles, wheezes, abdominal effort |
|
|
what respiratory disease causes epithelial edema, mucosal thickening and metaplasia (loss of ciliated epithelium with replacement of cuboidal cells) |
chronic broncitis (k9) |
|
|
How do you diagnose chronic bronchitis |
Diagnosis of exclusion* Steroid trial Rads: 3 view thorax: generalized increase in interstitial or peribronchialmarkings Cult/cyto of bronchoalveolarlavage Request Mycoplasma;not usually bacteria Bronchoscopy Echo: r/o heart dx, pulmonaryhypertension HW test and fecal exam |
|
|
Treatment for chronic bronchitis |
•Remove triggers •Corticosteroids •Metered Dose Inhalers •Oral ? Long-term •Cough Suppressants •Bronchodilators •Weight loss |
|
|
What are the 3 stages of feline heartworm disease |
•Stage 1:immature wormsarrive in pulmonary arteries, cause acute parenchymal inflammatory reaction •Stage 2:adult wormsstart to die, results in marked inflammatory response •Final stage: permanentlung damage that usually involves type II alveolar cell hyperplasia and chronicrespiratory disease |
|
|
in feline heartworm disease where does the worm reside |
pulmonary artery |
|
|
what is the usual worm burden in feline heartworm disease |
1-4 worms |
|
|
What disease is marked by pulmonaryvascular narrowing and tortuosity, thrombosis, and hypertension, smallnumber of worms which can lead to marked infarction, pulmonary edema,pneumonitis, and type II cellular proliferation |
feline heartworm disease |
|
|
clinical signs of feline heartworm disease |
•Vomiting •Cough, dyspnea •Weight loss anorexia, lethargy •Asymptomatic •Acute presentation: Salivation, tachycardia, dyspnea, Hemoptysis*, cough, CNS signs, sudden death |
|
|
How do you diagnose feline heartworm disease |
Microfilaremia israre Antigen: canmiss low worm burdens Antibody:indicates infection, past exposure Rads: enlarged pulmonary arteries, otherbased on severity Echo: may see in RV or PA |
|
|
How do you treat feline heartworm disease |
supportive care and prevention methods adulticide is not recommended |
|
|
what is the pathophysiology of caine heartworm disease |
1.Pulmonaryhypertension and pneumonitis: inflammation ofendothelium,dilation and tortuosity of the pulmonary arteries, pulmonary thrombosis, interstitial and alveolar lung disease 2.Right-sidedheart failure: high worm burdens, some backup into right ventricle; interfere with valve 3.Hepaticand renal disease: worms can reside in caudalvena cava; cause deposition of Ab-Ag complexes in kidneys 4.Cavalsyndrome: Hemolysis, shock, hypotension |
|
|
how do you diagnose canine heartworm disease |
HWantigen test Microfilariaexam CBC: r/o concurrent anemia, may seeeosinophilia, basophilia, monocytosis Chem: Increased globulins, azotemia Thoracicrads: Cardiomegaly, Pulmonary arterial enlargement,tortuosity, Pulmonary edema, infiltrates, Right atrial or ventricular enlargement Echo: “linear foreign body” in PA orright ventricle |
|
|
What are the 4 classes of canine heartworm disease |
Class 1: Dogs with either no clinical,radiographic or laboratory signs of disease, or very mild signs (cough) Class 2: moderate heartworm disease consisting of clinicalsigns (coughing, fatigue, weight loss), but no heart failure Class 3: Dogs with severe heartworm disease havea guarded prognosis Class 4: Dogs with CavalSyndrome |
|
|
what are the major clinical signs of class 3 heartworm disease |
cardiac cachexia,constant fatigue, persistent cough, dyspnea Right-sided CHF |
|
|
should you treat dogs with class 4 heartworm disease |
no, must have worms surgically removed |
|
|
what does a heart with heartworms look like |

Backwards D |
|
|
PleuralEffusion |
Build-up of fluid within the PLEURALSPACE |
|
|
PulmonaryEDEMA |
fluid within the lung interstitium |
|
|
Empyema |
purulent exudative fluid |
|
|
Chylothorax |
chylous fluid accumulates in pleural space |
|
|
Transudate pleural effusion is marked by: |
Mesothelial, macrophage Portal hypertension, mass, hypoalbuminemia |
|
|
Modified Transudate pleural effusion is marked by: |
Mesothelial, macrophage Rt side HF Mass |
|
|
Exudative pleural effusion is marked by: |
neutrophil Inflammation, septic or non-septic; irritant: bile, urine, chyle, foreign body; mass |
|

|
pulmonary edema |
|
|
what do fungal radiographs show |
Radiographs show a diffuse, nodularinterstitial pattern; lytic bone lesions |
|
|
Blastomycosis |
Clinical Forms: Primarypulmonary, Disseminated, Localcutaneous Clinical Signs: more in dogs, Anorexia, depression, wt. loss, Fever, cough, dyspnea, Ocular and nasal discharge, Wound exudate, Lymphadenopathy Not zoonotic but take precautions•Expensive; relapse common |
|

|
Blastomycosis |
|
|
Coccidioidomycosis |
Clinical Signs: May appear weeks/years afterexposure, Mild cough, Anorexia, weight loss, Mild fever, Lameness and pain if bone involvement, +/- lymphadenopathy |
|

|
Coccidioidomycosis |
|
|
Histoplasmosis |
Clinical Signs: 12-16 day incubation, GI disease as well ***, Cats: pulmonary signs, Dogs: GI signs - diarrhea Associated with bird and bat droppings prognosis poor for GI, good for pulmonary |
|

|
Histoplasmosis |
|
|
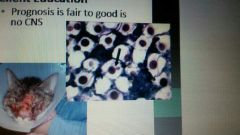
Cryptococcosis |
Most common systemic fungal disease incats! Organism grows in pigeon droppings Clinical Signs: Nasal cavity/sinus disease, chronicdischarge, 25% CNS disease, Ocular lesions, Mild fever, malaise, weight loss,anorexia, Dogs: CNS, skin |
|
|
Cryptococcosis |
|
|
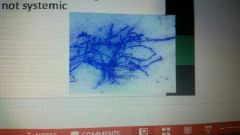
Aspergillosis |
In decaying vegetation, compost Predominantly nasal dz, Young to middle aged, Opportunistic, Chronic unilateral nasal discharge, Sneezing, stertor, pain Common in German shep 1-7 yrs |
|
|
Aspergillosis |
|

|
pulmonary neoplasia |
|
|
What is a highlycontagious systemic infection causedby an RNA virus Transmitted: Aerosols, Mother to fetus Clinical Signs: unvaccinated puppies, Fever, respiratory signs, hyperkeratosis of foot pads and nose(excess keratin)=hard pad, Vomiting and diarrhea, Enamel hypoplasia, Seizures: chewing gum, focal facialseizures |
Canine distemper virus |
|
|
Labile |
Easily killed in environment and with disinfectants |
|
|
What is a highlycontagious DNAvirus Transmitted: feces (dog,vector, fomite) Shed up to 3 days before clinical signs and 3 weeks after recovery Clinical signs: exhibited in 4-9 daysof exposure, replicates in lymphoid tissue, spreads to bloodstream, Attacks rapidly dividing cells, Destroys intestinal microvilli; bonemarrow cells |
Parvovirus |
|

|
canine parvovirus |
|
|
what is an infectious canine hepatitis of dogs, wild canids andbears, DNA virus Transmitted: Contact with infected urine,feces, saliva inenvironment, Virus replicates in tonsils and spreadsto lymph nodes, Continues via bloodstream to liver,kidney, spleen, eye |
canine adenovirus |
|
|
what disease has Clinical Signs that include, Subclinical infection, acute death, Fever, Hepatitis and necrosis, hepatic encephalopathy, seizures,ataxia, coagulopathy, DIC, icteric MM, serum,and urine, Can get pyelonephritis and chronic renaldisease, Can get uveitis and corneal edema |
canine adenovirus |
|
|
what is a Spirochete , passed via Ixodes tick Clinical Signs: Fever, lethargy, Anorexia, Episodic lameness, Lymphadenopathy, Rash, Myocarditis, nephritis |
Borreliosis (lyme disease) |
|
|
what is a Gram negative intracellular rickettsialorganism, passed via Ixodes tick Pathophysiology: bacteria binds to cell surface receptorsand is endocytosed into the cell, Inhibits neutrophil adherence andapoptosis Clinical Signs: Fever, lethargy, inappetence, Lameness, joint effusion, Lymphadenopathy, hepatomegaly,splenomegaly |
anaplasmosis |
|
|
What disease is a monocytic form vector is Rhipicephalussanguineus,brown dog tick Clinical Signs: Acute, Subclinical, and Chronic phases (Acute: Organisms multiply in spleen and liver; then to lungs, meninges, kidneys, Causes vasculitis Subclinical: not have any signs Chronic: bone marrow suppression, anemia, thrombocytopenia |
Ehrlichiosis- granulocytic |
|
|
what are the two different forms of ehrlishiosis granulocytic |
1.E.ewingii: Amblyomma americanumtickvector ( Sudden fever, lethargy, anorexia, Lameness (polyarthritis) and musclestiffness) 2.E.equi: Ixodesdamminitickvector (Fever, debilitating lethargy, anorexia) |
|
|
what is the disease Rickettsia rickettsia, Vector is Dermacentortick, Rhipicephalus Pathophysiology: Replicate in vascular endothelial cause inflammation,necrosis, and increased vascular permeability Clinical Signs: Fever, anorexia, deperession, Ocular discharge, Tachypnea, coughing, Vomiting, diarrhea, Muscle pain, CNS signs, Retinal hemorrhage, Scrotal edema, weight loss |
Rocky mountain spotted fever |
|
|
in what tick borne disease is the blood infectious |
rocky mountain spotted fever |
|
|
what vax was given to parvo dogs with the idea it would help prevent or make the disease less severe |
panleuk vax |
|

|
rocky mountain spotted fever |
|
|
what disease is Feline “distemper”, DNA virus in Parvoviridae Pathophysiology: virus replicatesin rapidly dividing cells (Neonatal brain, bone marrow, lymphoidtissue, intestinal lymphoid, Cells destroyed releasing largenumbers of virions) Clinical Signs: Young, unvax cats, Fever, depression, anorexia, Vomiting, fetid diarrhea, Dehydration, Fetal death, abortion, resorption, Cerebellar hypoplasia*, retinal defects |
panleukopenia |
|
|
what disease is Feline viral rhinotracheitis(FVR), contagious upper resp disease with high morbidity, moderate mortality, transmitted via aerosol and directcontact Clinical Signs: Acute onset sneezing, ulcerated nasal planum: Severe conjunctivitis,ulcers, Rhinitis withmucopurulent discharge, salivation, Fever, depression, anorexia, |
FelineHerpesvirus |
|
|
is FelineHerpes virus ever cured |
no |
|
|
what is an acute, highly contagious upperrespiratory tract disease with High morbidity, low mortality Transmitted by direct contact Clinical Signs: Fever, Serous ocular or nasal discharge, oral ulceration, salivation, Pneumonia, arthritis, diarrhea |
Feline calicivirus |
|
|
what medication does DR.A like with ulcers associated with feline calicivirus |
sucralfate |
|
|
what is Hemorrhagic calicivirus, Almost exclusively in group housed cats with 60% mortality that is Acute, severe systemic form, Acute respiratory disease, Vasculitis, Facial and limb edema, Skin ulcers, Organ failure, DIC Hemorrhagic Calicivirus |
VirulentSystemic Calici
|
|
|
what is an enteric coronavirus , highlycontagious and spread through feces, urine, saliva Transmitted: via inhalation oringestion, fomites, direct contact, Virus replicates in intestinalepithelium; enters macrophages and spreads systemically, extreme inflammation, Form granulomas in target organs (CNS,eyes, other) |
Feline infectious peritonitis (FIP) |
|
|
Clinical signs of the wet form of FIP include |
WetForm (Effusive) •Develops rapidly •Ascites and pleural effusion secondary tovasculitis •Anorexia, depression, weight loss •Dehydration •+/- fever |
|
|
Clinical signs of the dry form of FIP include |
DryForm (Non-effusive) •More chronic •Fever •Anorexia, depression, weight loss •Ocular lesions: uveitis, retinal lesions •Neurologic lesions •seizures |
|
|
is FIP easy or difficult to diagnose and what is the prognosis |
difficult, usually have to rule out other disease to determine poor prognosis |
|
|
what are the 2 treatment option for FIP |
Supportive care: Centesis, Steroids – immune suppression, Antibiotics Immunotherapy: Interferon, Polyprenyl Immunostimulant (PI), Experimental, good results for dryform (UT-CVM), Immunoregulin –non-specific immunostimulant |
|
|
what is a Retrovirus causing major mortality incats due to immunosuppression, anemia, and neoplasia Transmitted via contact with secretions, urine, feces, tears; fighting, grooming, fomites, in utero and duringnursing |
Feline Leukemia Virus |
|
|
What are the 3 possible sequelea of feline leukemia infection |
1.Regressiveinfection: cat has transient viremia, then clears it 2.Progressiveinfection: persistent viremia (bone marrow), Anemia,immune suppression, enteritis 3.Activeinfection: exhibit clinical signs, Fever, lethargy, lymphadenopathy, bloodcell deficiencies |
|
|
what is Retrovirus causing bone marrowsuppression and immunodeficiency, is lifelong Transmitted: Saliva and bite wound |
Feline immunodeficiency virus (FIV) |
|
|
What are the 3 stage of FIV |
Acute: Fever, lymphopenia, neutropenia,lymphadenopathy, GI or skin infection, Virus in T-cells, spreading to lymphnodes Latentstage: normal overall with persistent lymphadenopathy Chronicstage: Severe immunosuppression, secondaryinfections (URI, GI, UTI, skin), Gingivitis, stomatitis, diarrhea,wasting, anemia |
|
|
what are causes of anemia |
Irondeficiency Hemorrhage Hemolysis Parasites Toxins IMHA |
|
|
what are clinical signs of anemia |
increased HR and RR pale MM weak lethargic increased CRT |
|
|
anemia is caused by 1 of 3 things |
Decreasedproduction Increaseddestruction Loss of redblood cells (hemorrhage) |
|
|
how do you identify if anemia is regenerative of non-regenerative |
reticulocyte count |
|
|
how do we diagnose anemia |
PCV |
|
|
what are signs to look for with clotting issues |
Petechia, ecchymoses |
|
|
what anemia is Secondary tochronic blood loss (Fleas, GI bleed(ulcer), GI parasites, Neoplasia) Lose iron andhemoglobin(Microcytic,hypochromic red bloodcells (decreased MCV and MCHC)) |
Iron deficiency anemia |
|
|
what type of anemia is when immunecomplexes attach to rbc’s and body tries to remove them Dogs occurssecondary to inflammatory diseases TX: immune suppression Cats: occurssecondary to hemobartonellosis (Mycoplasma), FeLV TX:Transfusion, docy |
Hemolysis anemia |
|
|
Rememberneonatal isoerythrolysis? |
Dam passesantibodies to the neonate’s rbc in colostrum |
|
|
what type of anemia is: Mycoplasma hemofelis (Bacteriaattaches to rbc membrane, increased destruction, Anorexia,fever, weight loss, hepatosplenomegaly) Cytauxzoon felis (Protozoalorganism, Intracellular- anemia, Extracellular-macrophage involvement and creates vascularobstruction) Babesia (viabrown dog tick, Infects rbc’s, causeshemolysis, Hemoglobinuria,fever, anorexia, depressio) |
Blood- borne parasites |
|
|
What anemia is caused by oxidants where Hemoglobindenatures and forms Heinz body aggregates (Cats moresusceptible, Dog – onions!) or caused by Drugs (Acetaminophen: Causes methemoglobinemia, Methylene blue) |
Toxins / HeinzBody Anemia |
|
|
In what anemia do antibodiesattach to rbc membrane, accelerate their destruction and removal, complementsystem activated causing agglutination and destruction/macrophagesengulf and cleared in spleen Common in dogs 2-8 yrs, Breeds (Poodles, IrishSetter, Sheepdogs, Cockers, Females 4 xmore likely than males |
Immune mediated hemolytic anemia (IMHA) |
|
|
how do you treat IMHA |
Glucocorticoids Proton pumpinhibitors Heparin(thromboembolism, DIC) |
|
|
what is the prognosis for IMHA |
Guarded prognosis –30-40% will die. Relapses are common. |
|
|
What platelet disorder is when plateletsbecome coated in antibodies, abnormalplatelets destroyed by spleen/bone marrow/liver causes are drugs, toxins, infectious disease, females > males affected; 5-6 years old Clinical Signs: Petechia, ecchymoses, Epistaxis,hematemesis, hematochezia/melena, Weakness,lethargy, Hemorrhagewhen platelets < 30,000 |
Immune-mediatedThrombocytopenia |
|
|
How do you diagnose ITP (Immune-mediatedThrombocytopeni) |
Plateletcounts Bone marrowexam Clinical signsand response to treatment |
|
|
How do you treat ITP (Immune-mediatedThrombocytopeni) |
Glucocorticoids Vincristine Platelet –richplasma transfusion / whole blood Splenectomy inrefractory cases |
|
|
What is the prognosis for ITP (Immune-mediatedThrombocytopeni) |
Prognosis = guarded to good. May relapse. |
|
|
where are leukocytes formed |
Formed in bonemarrow, thymus, lymph system |
|
|
what are granulocytes |
Neutrophils,basophils, eosinophils |
|
|
what are agranulocytes |
Lymphocytes,monocytes -T-lymphocytes:recognize self, active in cell-mediated immunity (helper,natural killer, cytotoxic T cells) - B-lymphocytes (Humoralresponse (Ab), complement activation, opsonization) |
|
|
what are diseases of the leukocytes |
Ehrlichia FIV FeLV Lymphoma (Feline, Mediastinal, Alimentary, Multicentric, Canine) |
|
|
what disease accounts for90% of feline hematopoietic tumors, most inducedby FeLV - 70% felinelymphoma are positive for FeLV -Average age is 3 years - Average age in negative cats is 7 years - 80% of catswith multicentric LSA are FeLV positive |
Feline Lymphoma (Lymphosarcoma - LSA) |
|
|
What disease occurs in young FeLV cats Signsrelate to mass in mediastinum, Dyspnea, Tachypnea, Regurgitation, Cough, Anorexia,weight loss, depression, Pleuraleffusion |
Mediastinal LSA |
|
|
what disease occurs inolder cats, most FeLV negative Clinical signsrelate to intestinal mass, vomiting,diarrhea, Weight loss, obstruction |
Alimentary LSA |
|
|
what is the most commonform, most FeLV positive, ~ 4years old Clinical signsdepend on location (Asymptomatic, Anorexia,weight loss, lethargy, Enlargedperipheral lymph nodes, Anemia if FeLV +, Liver, GI: Vomiting, diarrhea, Lungs: Dyspnea, Renal:enlarged kidney, renal failure, Ocular:uveitis, blindness |
Multicentric LSA |
|
|
how do you diagnose multicentric LSA |
Diagnosed viacytology of mass or lymph node |
|
|
what is treatment for lymphoma |
Chemotherapy preferred :Remissionrates up to 80% reported, Remission lasts 42 days to 42 months Chemo sideeffects: Anorexia,vomiting, Leukopenia, Renal toxicity Localizedradiation can be helpful for some Will return remission average time is 5 months |
|
|
what is mostcommon hematopoeitic tumor of dogs, 85% involveregional or generalized lymphadenopathy Treatment: Chemotherapy, Prednisonetreatment alone = shorter survival Best rates arewith combination protocols Drug resistanttumor cells have emerged |
Canine Lymphoma |
|
|
what breeds are predisposed to Canine Lymphoma |
Boxers, Bullmastiffs, Bassets, Saint Bernards,Scotties predisposed |
|
|
Which congenital heart disease is where valves are dysplastic or malformed and outflow tract from the right ventricleis narrowed |
Pulmonic stenosis |
|
|
What arrhythmia is fast but normal? |
Supraventricular tachycardia (SVT) |
|
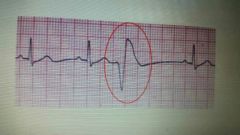
What is this complex called? |
VPC |
|
|
What is a clinical sign a pup with Persistent right aortic arch (PRAA)might show? |
Regurgitation |
|
|
Most common cause of sinusitis in dog? |
tooth root abscess |
|
|
Whichcongenital heart disease has excellent prognosis with surgicalcorrection60% fatality within 1 year without sx |
Patent ductus arteriosus (PDA) |
|
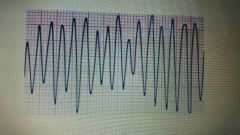
What arrhythmia? |
ventricular flutter/ fibrillation |
|
|
What arrhythmia has a lack of relationship between Pwaves and QRS-T, and treatment is with anticholinergics or sympathomimetics |
AV block |
|
|
Name two causes of rhinitis |
bacteria, virus, foreign body, fungus |
|
|
Name a type of nasal tumor |
Squamous cell carcinoma (SCC) Adenocarcinoma Lymphoma |
|
|
Which congenital heart disease is obstruction to left ventricular outflow, left ventricular hypertrophy and aorticdilation |
Subaortic stenosis |
|
|
Name a differential for bilateralepistaxis |
Coagulopathy Nasal tumor |
|
|
epistaxis is what |
nose bleed |
|
|
What type of arrhythmia has QRS complexes appear normal…..problemis with the p wave |
Supraventricular |
|
|
Which congenital heart anomaly causes megaesophagus? |
Persistent right aortic arch (PRAA) |
|
|
What arrhythmia has Pwaves occur earlier than normal; impulse originates from other than SA nodefollowed by normal QRS |
APC(atrial premature contraction) |
|
|
What is the cause of these signs in an older lab: - Stridor - Worsewith exercise, excitement, heat - Inspiratory dyspnea - Dysphonia |
LarPar (GOLPP: geriatric onset laryngeal paralysis and polyneuropathy) |
|
|
Organism that does the following: attach to cilia of bronchial epitheliumand interfere with motility; also endotoxins and exotoxins |
bordetella |
|

Edema or effusion? |
Effusion |
|
|
Two strains of canine influenza |
H3N8 H3N2 |
|
|
What disease? Losefirmness Collapsesduring respiration Progressive |
Collapsingtrachea |
|
Most likely disease? |
calicivirus |
|

What 2 possible diseases? |
Neoplasia ? |
|
|
Most common systemic fungal disease incats? |
cryptococcosis |
|

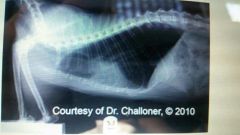
What likely disease? |
Heartworm disease |
|
|
What fungal disease? •Cats:pulmonary signs •Dogs:GI signs – diarrhea |
histoplasmosis |
|
|
What fungal disease? •Nasalcavity/sinus disease, chronic discharge •25%CNS disease •Ocularlesions |
cryptococcosis |
|
|
Three phases of leptospirosis? |
•Acute •Convalescent •Chronic |
|
|
What tick disease? •Replicate in vascular endothelial cellscausing inflammation,necrosis, and increased vascular permeability |
Rocky Mountain Spotted Fever (RMSF) |
|
|
What fungal disease? •Predominantlynasal dz •Youngto middle aged •Opportunistic •Chronicunilateral nasal discharge •Fromdecaying vegetation |
aspergillosis |
|

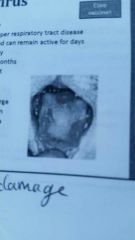
Most likely disease? |
Feline herpesvirus |
|
|
Two rickettsialdiseases: |
•Ehrlichia •RMSF |
|
|
What disease? •Destroysintestinal microvilli; bone marrow cells •Canget bacterial translocation and septicemia |
parvo |
|
|
What disease? •Maystart as tonsillitis but often goes unnoticed •Fever •Hepatitisand necrosis |
CAV |
|
|
What disease? •Spirochetebacteria •Many serovars: icterohemorrhagiae,canicola,pomona,grippotyphosa,bratislava,autumnalis |
Lepto |
|
|
What disease? •Organism enters through mucous membranes,abrasions, or ingestion of contaminated food/water |
lepto |
|
What lower respiratory disease? |
Feline asthma |
|
|
Name 2 tick diseases that cause lameness. |
•Lyme •Ehrlichia •Anaplasma |
|
|
What disease? •causing major mortality in cats due toimmunosuppression, anemia, and neoplasia |
FeLV |
|
|
What feline disease? •Cerebellar hypoplasia*, retinal defectswhen exposed in utero |
panleukemia |
|
|
What disease? •Serousocular or nasal discharge •**oralulceration**,salivation •Pneumonia,arthritis, diarrhea |
calici |
|
|
Treatment for most tick diseases? |
Doxycycline |
|
|
What are the forms of FIP? |
Dry Wet/effusive |
|
|
What disease? •Hyperkeratosis of foot pads and nose(excess keratin)=hard pad •Enamel hypoplasia |
Canine distemper virus (CDV) |
|
|
What is a regressive infection in Felv? |
•Cat clears viremia |
|
What disease? |
rabies |
|
|
What zoonotic disease? •Feline is definitive host but others canbe intermediate |
toxo |
|
|
What cause of anemia? •Antibodiesattach to the rbcmembrane which accelerates their destruction and removal•Complementsystem is activated causing agglutination and destruction, or•Macrophagesengulf and are cleared in the spleen |
IMHA |
|
|
What disease? •Virusreplicates in intestinal epithelium; enters macrophages and spreadssystemically •Causesextreme inflammation •Formgranulomas in target organs (CNS, eyes, other) |
FIP |
|
|
What test tells you if anemia isregenerative or not? |
•Reticulocyte count |
|
|
What type of anemia? •Microcytic, hypochromic redblood cells (decreased MCV and MCHC) |
•Iron deficiency |
|
|
What disease? •Plateletsbecome coated with antibodies or complement-Ab complexes •Abnormalplatelets are destroyed by the spleen, bone marrow, or liver |
ITP (Immune mediated thrombocytopenia) |
|
|
Accounts for 90% hematopoietic tumors incats? |
lymphoma |
|
|
Cause of 70% of lymphoma in cats? |
FeLV |
|
|
What disease in cats? •Once infected, virus reproduces in Tcells and spreads to other wbc’s and lymph nodes, salivary glands, CNS |
FIV |