Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
528 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Define ligament.
|
fibrous connective tissue connecting bone to bone
|
|
|
|
Define tendon.
|
fibrous connective tissue connnecting muscle to bone
|
|
|
|
Define fascia.
|
fibrous connective tissue connecting muscle to muscle (and other structures)
|
|
|
|
What are the four muscles that make up the rotator cuff?
|
SITS = supraspinatus, infraspinatus, teres minor, subscapularis
|
|
|
|
Define thenar eminence.
|
muscles found on palmar surface at base of thumb
|
|
|
|
Define hypothenar eminence.
|
muscles found on palmar surface at base of little finger
|
|
|
|
What equipment is needed for the musculoskeletal exam?
|
skin-marking pencil
tape measure reflex hammer optional: goniometer |
|
|
|
What causes muscle wasting?
|
trauma resulting in limited use of arm due to pain
muscle problem nerve problem |
|
|
|
Define spasticity.
|
increase in muscle tone
|
|
|
|
List the grading scale for muscle strength.
|
5 = full ROM against gravity, full resistance
4 = full ROM against gravity, some resistance 3 = full ROM against gravity, no resistance 2 = passive ROM 1 = trace movement 0 = no movement |
Mosbys p707
|
|
|
Describe the steps of the musculoskeletal exam.
|
1. inspection → gait and posture
2. inspection → symmetry, contour, discoloration, swelling, masses 3. palpation -all muscles, bones, joints -warmth, swelling, crepitus, fluctuation of a joint (associated with effusion), resistance to pressure, tenderness 3. ROM |
|
|
|
What is the ddx for crepitus?
|
rubbing of bones (moving joint, broken bone)
tenosynovitis |
Mosbys p707
|
|
|
When should you use a goniometer?
|
when increase or limitation in ROM; begin with joint fully extended and then flex it; meausure angles of greatest extension and flexion and compare with expected values
|
Mosbys p707
|
|
|
What are you evaluating when you ask patient to clench teeth?
|
temporalis and masseter muscles → motor function of trigeminal nerve
|
Mosbys p707
|
|
|
Define cubitus valgus.
|
lateral carrying angle >15 degrees
|
|
|
|
What is a normal carrying angle?
|
5-15 degrees
|
|
|
|
Define cubitus varus.
|
medial carrying angle
|
|
|
|
Define fracture.
|
broken bone
|
|
|
|
Define myopathy.
|
disorder of muscle
|
|
|
|
Define neuropathy.
|
disorder affecting single peripheral nerve
|
|
|
|
Define polyneuropathy.
|
disorder affecting multiple peripheral nerves
|
|
|
|
What is another name for cubitus varus?
|
gunstock deformity
|
|
|

|
cubitus varus
|
|
|
|
cubitus valgus
|
|
|
|
What is a swan neck deformity?
|
hand deformity characterized by hyperextension of PIP joint and hyperflexion of DIP joint
|
|
|
|
What is the ddx for swan neck deformity?
|
congenital
trauma RA |
|
|

|

|
|
|
|
What are possible problems of the elbow joint?
|
dislocation
fracture tendonitis arthritis infection |
|
|
|
What is the purpose of Adson's Test?
|
suspected thoracic outlet syndrome
|
|
|
|
How do you perform Adson's test?
|
1. ask patient to stand
2. palpate radial pulse while pulling arm backward (abduction, external rotation, hyperextension) 3. ask patient to rotate head to involved side, take deep breath and hold it 4. positive for thoracic outlet syndrome if diminished or absent radial pulse |
|
|
|
What is thoracic outlet syndrome?
|
disorder involving compression of the neurovascular bundle passing between the anterior and middle scalene muscles at the superior thoracic outlet
|
|
|
|
What are the types of thoracic outlet syndrome?
|
1. neurogenic TOS → compression of brachial plexus
2. arterial TOS → compression of subclavian artery 3. venous TOS → compression of subclavian vein |
|
|
|
What does TOS stand for?
|
thoracic outlet syndrome
|
|
|
|
What is the purpose of Yergason's test?
|
suspected
1. bicipital tendonitis 2. laxity or tear of transverse humeral ligament → instability of long head of the biceps brachii tendon in bicipital groove |
|
|
|
How do you perform Yergason's test?
|
1. ask patient to sit or stand
2. adduct arm, flex arm to 90°, and place forearm in neutral position (thumb facing upward) 3. stabilize elbow inferiorly and grasp forearm with other hand 4. move glenohumeral joint into external rotation and proximal radioulnar joint into supination 5. positive if pain or snapping in bicipital groove OR 1. ask patient to sit or stand 2. adduct arm, flex elbow to 90°, and pronate forearm 3. place thumb in bicipital groove while grasping forearm with other hand 4. ask patient to move glenohumeral joint into external rotation and proximal radioulnar joint into supination while you provide resistance 5. positive if bicipital tendonitis or laxity/tear of pain or snapping in bicipital groove |
|
|
|
What is the function of the tranverse humeral ligament?
|
secures long head of the bicep tendon in bicipital groove
|
|
|
|
What is the purpose of the apprehension test?
|
suspected dislocation or dislocatability of shoulder
|
|
|
|
How do you perform the apprehension test?
|
1. patient may be standing, sitting, or supine
2. flex elbow 90° and abduct arm 90° 3. externally rotate arm 4. positive for dislocation or dislocatability if look of apprehension on patient's face |
|
|
|
What is the purpose of the drop arm test?
|
suspected rotator cuff tear
|
|
|
|
How do you perform the drop arm test?
|
1. passively abduct arm 90°
2. ask patient to slowly lower arm 3. positive for rotator cuff tear if pain + difficulty in lowering arm smoothly |
|
|
|
What is the most common type of rotator cuff tear?
|
supraspinatus tear
|
|
|
|
How do you test for medial epicondylitis (golfer's elbow)?
|
1. flex wrist
2. palpate medial epicondyle → origin of common flexor tendon 3. positive if pain |
|
|
|
How do you test for lateral epicondylitis (tennis elbow)?
|
1. extend wrist
2. palpate lateral epicondyle → origin of common extensor tendon 3. positive if pain |
|
|

|
olecranon bursitis
|
|
|
|
Which is more common, anterior or posterior shoulder dislocation?
|
anterior (98%)
|
|
|
|
How do you perform the valgus stress test for the knee?
|
1. flex knee 15°
2. place one hand on lateral knee so thenar eminence is against fibular head 3. place other hand on medial ankle 4. push medially against knee and laterally against ankle 5. palpate medial joint line for gapping indicative of MCL joint instability |
Hoppenfeld p185
|
|
|
What is the purpose of the valgus stress test of the knee?
|
suspected MCL joint instability
|
Hoppenfeld p185
|
|
|
How do you perform the varus stress test for the knee?
|
1. flex knee to 15°
2. place one hand on medial knee so thenar eminence is against tibia 3. place other hand on lateral ankle 4. push laterally against knee and medially against ankle 5. palpate lateral joint line for gapping indicative of LCL joint instability |
Hoppenfeld p185
|
|
|
What is the purpose of the varus stress test of the knee?
|
suspected LCL joint instability
|
Hoppenfeld p185
|
|
|
Which is more common, MCL injury or LCL injury?
|
MCL injury
|
Hoppenfeld p185
|
|
|
Which is worse, an MCL or LCL tear?
|
MCL tear → MCL is crucial to joint stability whereas an LCL tear may have little to no effect on stability
|
Hoppenfeld p185
|
|
|
What is the function of the ACL and PCL?
|
prevention of anterior and posterior dislocation of the tibia
|
Hoppenfeld p185
|
|
|
How do you perform the anterior/posterior drawer sign?
|
1. have patient lie supine
2. flex knees 90° 3. stabilized patient's foot by sitting on it 4. place fingers on insertion of medial and lateral hamstrings 5. place thumbs on medial and lateral joint lines 6. pull tibia anteriorly to perform anterior drawer sign 7. positive if tibia slides anteriorly 8. indicative of possible ACL tear 9. push tibia posteriorly to perform posterior drawer sign 10. positive if tibia slides posteriorly 11. indicative of possible PCL tear |
Hoppenfeld p186
|
|
|
What is the purpose of the anterior/posterior drawer sign?
|
anterior drawer sign → suspected ACL instability/injury
posterior drawer sign → suspected PCL instability/injury |
Hoppenfeld p186
|
|
|
Which is more common, ACL or PCL tear?
|
ACL tear
*PCL is rare |
Hoppenfeld p186
|
|
|
Which is more accurate, anterior drawer test or Lachman's test?
|
Lachman's test
|
|
|
|
How do you perform Lachman's test?
|
1. have patient supine
2. flex knee 20° 2. place one hand behind femur 3. place other hand behind tibia 4. pull tibia anteriorly 5. positive if anterior displacement of tibia or soft endpoint 6. indicative of ACL injury |
|
|
|
What is the purpose of Lachman's test?
|
suspected ACL instability/injury
|
|
|
|
What is the purpose of McMurray's test?
|
suspected medial meniscus tear
|
|
|
|
How do you perform McMurray's test?
|
1. have patient supine
2. place one hand on heel and flex leg fully 3. place other hand with thumb on lateral joint line of knee and fingers on medial joint line 4. push on lateral knee, externally rotate leg, and flex/extend leg 5. positive if palpable or audible "click" within joint 7. indicative of probable medial meniscus tear |
Hoppenfeld p191
|
|
|
What is the purpose of Aply's grinding test?
|
suspected meniscus tear
|
|
|
|
How do you perform Aply's grinding test?
|
1. have patient lie prone
2. flex knee 90° 3. place your knee on patient's thigh to stabilize it 4. push down on heel and rotate tibia internally and externally 5. positive if pain 6. if pain on medial side → indicative of medial meniscal tear 6. if pain on lateral side → indicative of lateral meniscal tear |
Hoppenfeld p191
|
|
|
What is the purpose of Allen test?
|
suspected arterial insufficiency or prior to performing ABG
|
|
|
|
What is the purpose of Apley's distraction test?
|
to distinguish between meniscal injury and ligament injury of knee
|
|
|
|
How do you perform Apley's distraction test?
|
1. have patient lie prone
2. flex knee 90° 3. place your knee on patients femur to stabilize it 4. pull up on ankle 5. internally and externally rotate tibia 6. pain indicative of ligament injury 7. pain should not occur if meniscal injury |
Hoppenfeld p193
|
|
|
How do you perform the Allen test?
|
1. compress radial and ulnar arteries
2. ask patient to clench and unclench fist several times 3. patient's hand should appear blanched 4. release compression of ulnar artery 5. patient's hand should "blush" within 5-10 sec 6. positive if blushing does not occur within 5-10 sec 7. if positive, do not perform ABG or cannulation since ulnar arterial supply to hand is not sufficient |
|
|
|
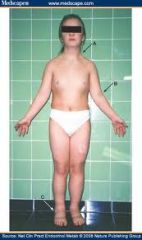
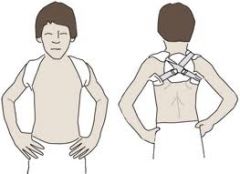
What is scoliosis?
|
lateral curvature of the spine associated with rotation of involved vertebrae (usually thoracic or lumbar, rarely cervical)
|
Orthopedics p158
Current Pediatrics |
|
|
What is the etiology of scoliosis?
|
if structural (i.e.fixed, fail to correct with lateral flexion) → usually idiopathic, but also congenital abnormalities, neurofibromatosis, neurologic or myopathic conditions
if non-structural (i.e. flexible, correct with lateral flexion) → compensatory mechanism secondary to leg length discrepancy, acute lumbar disc disease, or local inflammation 6x more common in females than males usually occurs between 8-13y/o infantile scoliosis may occur between 2-4y/o |
Orthopedics p158
Current Pediatrics |
|
|
What is the clinical presentation of scoliosis?
|

asymptomatic
lateral curvature of the spine assymmetry of the heights of the ribs or paravertebral muscles right thoracic curves most common |
Orthopedics p158
|
|
|
What is the diagnostic workup of scoliosis?
|

standing radiograph of the spine
|
Orthopedics p158
|
|
|
What is the management of scoliosis?
|
if nonstructural:
1. treat primary cause if structural: 1. refer to specialist 2. if <20 degrees → frequent observation 3. if >20 degrees → spinal bracing via Miwaukee brace or thoracolumbosacral orthotic 4. brace worn 23 hours per day 5. exercises performed in brace 6. if >45 degrees → surgery |
Orthopedics p158
|
|
|
What are the complications of scoliosis?
|
pain, deformity, disability, cardiopulmonary compromise
|
Orthopedics p160
|
|
|
What is the patient education for scoliosis?
|
1. spinal brace may have to be worn for >2 years
2. bracing does not eliminate curve but prevents progression 3. surgery may cause loss of spine motion 4. if >25 degree curve + pregnant → curve may increase |
Orthopedics p161
|
|
|
What is the etiology of genu varum and genu valgum in children?
|
normal variant
genu varum → normal from infancy to 2 years genu valgum → normal from 2-8 years |
|
|
|
When are genu varum and genu valgum normal?
|
genu varum → normal from infancy to 2 years
genu valgum → normal from 2-8 years |
Peds Current
|
|
|
What is the clinical presentation of genu varum and genu valgum?
|
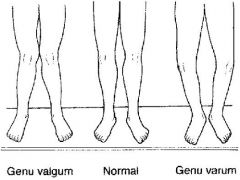
genu varum → bow-legged
genu valgum → knock-kneed |
Peds Current
|
|
|
When is the management for genu varum and genu valgum?
|
refer to orthopedist if:
bowing persists beyond 2/yo bowing increases rather than decreases bowing is unilateral knock-knees associated with short stature |
Peds Current
|
|
|
What are the complications of genu varum and genu valgum?
|
failure to straighten in appropriate time frame
genu varum → normal from infancy to 2 years genu valgum → normal from 2-8 years |
|
|

|
genu varum
|
|
|

|
genu valgum
|
|
|
|
What is the common name for talipes equinovarus?
|
clubfoot
|
|
|
|
What is the etiology of talipes equinovarus?
|
1. idiopathic (hereditary)
2. neurogenic 3. associated with a disorder (arthrogryposis, Larsen syndrome) occurs in 1:1000 live births |
Peds Current
|
|
|
What is the clinical presentation of talipes equinovarus?
|

1. plantar flexion of foot at ankle joint (equinus)
2. inversion of heel (varus) 3. medial deviation of forefoot (varus) |
Peds Current
|
|

|
talipes equinovarus
|
|
|
|
What is the management of talipes equinovarus?
|
1. immediate manipulation of foot following birth
2. splint to hold foot in correct position 3. once full correction obtained, long-term night brace 4. if resistant to manipulation and casting → surgery |
Peds Current
|
|
|
What is the etiology of metatarsus varus?
|
congenital
usually 2° to positioning in uterus |
Peds Current
|
|
|
What is the clinical presentation of metatarsus varus?
|

medial deviation of the forefoot
angulation at base of 5th metatarsal vertical crease in arch if rigid form |
Peds Current
|
|
|
What is the management of metatarsus varus?
|
if flexible → resolve spontaneously
if rigid → cast changed at intervals of 2 weeks |
Peds Current
|
|
|
What conditions are commonly associated with congenital hip dysplasia?
|
torticollis
metatarsus varus |
Peds Current
|
|
|
Define dysplasia.
|
abnormal growth or development
|
|
|
|
How do you perform the Ortolani and Barlow maneuvers?
|
place infant on back
obtain complete relaxation of infant ORTOLANI: place long finger over greater trochanter and thumb over inner side of thigh flex hips to 90° slowly abduct from midline one hip at a time attempt to lift greater trochanter forward feeling of slipping as head relocates is sign of instability BARLOW: apply pressure with thumb over inner side of thigh adduct thigh attempt to slip hip posteriorly eliciting a jerk as hip dislocates is sign of instability |
|
|
|
CONGENITAL DYSPLASIA OF THE HIP:
|

ETIOLOGY:
congenital → both acetabulum and femur underdeveloped occurs in 1:1000 live births CLINICAL PRESENTATION: abnormal relationship between proximal femur and acetabulum (dysplasia, subluxable hip, dislocatable hip, dislocated hip) Ortolani and Barlow reveal instability (signs of instability less evident after 1 m/o) if abduction limited to <90° → contracture around hip joint if knees unequal heights when hips and knees flexed → dislocated hip on side of lower knee if walking → painless limp, lurch to affected side, standing on affected leg results in dip in pelvis of opposite side d/t weakness of gluteus medius muscle (Trendelenburg sign) if bilateral dysplasia → waddling gait, widened perineum, lumbar lordosis MANAGEMENT: 1. completely reversible if corrected within first few weeks of life 2. if <4 m/o → manual reduction by flexion and abduction of hip, then pavlik harness to maintain reduction 3. if > 4m/o → traction x 2-3 weeks, then reduction under general anesthesia, then hip spica x 6 months 4. if unstable after closed reduction → open reduction 5. if older age → open reduction + correction of deformity COMPLICATIONS: if not corrected → dysplasia will be become progressive and irreversible and deformity will worsen, especially after walking age |
|
|
|
What is the etiology of tibial torsion?
|
if <16-18 months → normal variant
if persists beyond 16-18 months → sleeping with feet turned in |
Peds Current
|
|
|
What is the management of tibial torsion?
|
self-limiting → resolves by 16-18 months
if persists beyond 16-18 months → external rotation splint worn nightly |
Peds Current
|
|
|
What is the clinical presentation of tibial torsion?
|

internally rotated tibia
usually 20° sometimes accentuated by laxity of knee ligaments |
Peds Current
|
|
|
What is the clinical presentation of femoral anteversion?
|

internally rotated femur
|
Peds Current
|
|
|
What is the management of femoral anteversion?
|
returns to neutral by 6-8y/o
encourage external rotation exercises → bike riding, skating refer to orthopedist if no external rotation of hip in extension |
Peds Current
|
|
|
What are the disorders associated with "in-toeing"?
|
metatarus varus
tibial torsion femoral anteversion |
|
|
|
What does SCFE stand for?
|
slipped capital femoral epiphysis
|
|
|
|
Where does SCFE often refer?
|
knee
|
|
|
|
What is a SCFE?
|
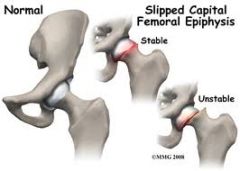
displacement of proximal femoral epiphysis
usually displaced medially and posteriorly relative to femoral neck |
PEDs Current
|
|
|
What is the etiology of a SCFE?
|
displacement of proximal femoral epiphysis d/t disruption of growth plate
cause unknown may be d/t weakness associated with hormonal changes associated with: obesity trauma hypothyroidism most common in obese adolescent males |
PEDs Current
|
|
|
What is the clinical presentation of a SCFE?
|
pain and limp
referred pain to thigh and medial knee (knee pain may be only complaint) limited internal rotation of hip stable if able to bear weight unstable if unable to bear weight |
PEDs Current
|
|
|
What is the diagnostic workup of a SCFE?
|
AP and lateral radiographs of the hip
|
PEDs Current
|
|
|
What is the management of a SCFE?
|
crutches for non-weight bearing
immediate referral to orthopedics for surgical fixation |
PEDs Current
|
|
|
What are the complications of a SCFE?
|
AVN
premature degenerative arthritis |
|
|
|
What is another name for Legg-Calves-Perthes disease?
|
avascular necrosis of proximal femur
|
|
|
|
LEGG-CALVES-PERTHES DISEASE:
|
ETIOLOGY:
idiopathic osteonecrosis of capital femoral epiphysis usually occurs between 4-8 y/o CLINICAL PRESENTATION: persistent pain in hip or groin referred mild or intermittent pain in thigh or knee atrophy of thigh 2° to disuse ↓ internal rotation and abduction limping gait MANAGEMENT: 1. radiograph of hip 2. protect hip joint and maintain normal joint motion to prevent degenerative arthritis 3. little benefit from bracing and surgery controversial COMPLICATIONS: poorer prognosis if metaphysical defects, complete involvement of femoral head, or late childhood onset |
|
|
|
What is nursemaid's elbow?
|
subluxation of radial head from annular ligament
|
PEDS Current
|
|
|
What is the etiology of nursemaid's elbow?
|
being lifted or pulled by the hand
consider abuse! |
PEDs Current
|
|
|
What is the clinical presentation of nursemaid's elbow?
|
painful fully pronated elbow
complaint that elbow will not bend radial head tenderness |
PEDs Current
|
|
|
What is the diagnostic workup of nursemaid's elbow?
|
radiographs normal
|
PEDs Current
|
|
|
What is the management of nursemaid's elbow?
|
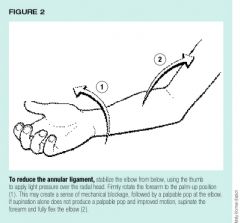
1. reduction → fully supinate arm and move from full extension to full flexion, will often hear click, and child will immediately feel better
2. sling x few days |
PEDs Current
|
|
|
What is the most common cause of septic arthritis?
|
staph aureus
|
Current p777
|
|
|
What is the diagnostic workup of septic arthritis?
|
synovial fluid:
cell count >50,000 cells/mcL differentail >90% PMNs gram stain culture BC positive in 50% of cases |
Current p777
|
|
|
SEPTIC ARTHRITIS:
|

ETIOLOGY:
source varies according to age: infant → usually d/t adjacent osteomylelitis child → usually isolated infection without bone involvement teenager → usually organism with affinity for joints (gonococcus) or underlying systemic infection organism varies with age: <4 m/o → group B strep, staph aureus 4 m/o to 4 y/o → staph aureus, h. flu (less common d/t immunizations) >4 y/o → staph aureus, staph pyogenes CLINICAL PRESENTATION: inflammatory monoarticular arthritis commonly affects knee, hip, wrist, shoulder, or ankle acute pain, swelling, warmth worsens over hours joint effusion infant → suspect if irritable, poor feeding, decreased abduction; paralysis of limb d/t inflammatory neuritis child → fever, malaise, vomiting, restriction of motion MANAGEMENT: 1. joint aspiration → WBC count >50,000 2. hospitalization and surgical drainage 3. empiric antibiotic therapy → nafcillin or oxacillin + 3rd generation cephalosporin 4. narrow-spectrum antibiotic therapy → selected based on age, gram stain, culture; 3 weeks for staph infection, 2 weeks for other infections COMPLICATIONS: if not detected before 24 hours, destruction of joint cartilage occurs, followed by arthrosis and fibrosis damage to growth plate may also occur |
|
|
|
Define torticollis.
|
stiff neck
|
|
|
|
What is a ganglion cyst?
|
soft tissue lesion found adjacent to a joint or tendon sheath
|
Orthopedics p111
|
|
|
What does the term "Bible bump" refer to and why?
|
refers to a ganglion cyst because common treatment in the past consisted of hitting the cyst with a bible (a book that most people possessed), causing it to rupture and drain
|
|
|
|
What is a Colles fracture?
|
fracture of the distal radius with fragment displaced dorsally
|
Orthopedics p125
|
|
|
What is the etiology of a Colles fracture?
|
fall onto extended wrist (i.e. outstretched hand)
|
Orthopedics p125
|
|
|
What is the clinical presentation of a Colles fracture?
|

history of fall on outstretched hand
acute pain, swelling, and tenderness of wrist dinner-fork (or silver-fork) deformity |
EOMC p350
|
|

|
dinner fork deformity → colles fracture
|
|
|
|
What is the diagnostic workup of a Colles fracture?
|

AP and lateral radiographs of forearm and wrist → dorsal angulation, radial deviation, and shortening of distal radial fragment
possible associated injury to ulnar styloid or ulnar collateral ligament |
Orthopedics p124
EOMC p350 |
|
|
What is the management of a Colles fracture?
|
1. reduction
2. short arm cast x 6 weeks 3. repeat radiographs immediately following reduction 4. repeat radiographs in 7-10 days 5. once cast removed, splint x 3 weeks 6. gentle exercises → shoulder, elbow, fingers |
Orthopedics p124
EOMC p350 |
|
|
What are the complications of a Colles fracture?
|
deformity, malunion, loss of wrist or finger motion, wrist arthritis, carpal tunnel syndrome, compartent syndrome, parasthesias
|
EOMC p350
|
|
|
What is a Smith's fracture?
|
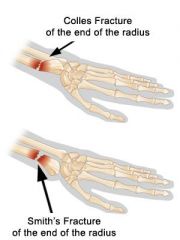
fracture of distal radius with fragment displaced ventrally (i.e. reverse Colles fracture)
|
|
|
|
What is the etiology of a Smith's fracture?
|
fall onto flexed wrist
|
|
|
|
What is the difference between a Colles fracture and a Smith's fracture?
|
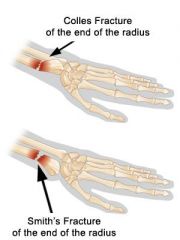
both are fractures of the distal radius
Colles → radial fragment displaced dorsally Smith's → radial fragment displaced ventrally (volarly) |
|
|
|
What is a boxer's fracture?
|
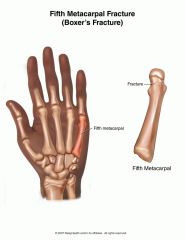
fracture of the distal metaphysis of the 5th metacarpal
|
Orthopedics p132
|
|
|
What is the etiology of a boxer's fracture?
|
usually fist fight
|
Orthopedics p132
|
|
|
What is the clinical presentation of a boxer's fracture?
|

history of fist fight
acute pain, swelling, and tenderness depression of knuckle of affected finger decreased ROM |
EOMC p355
|
|

|
depression of 5th "knuckle" → boxer's fracture
|
|
|
|
What is the diagnostic workup of a boxer's fracture?
|

AP, lateral and oblique radiographs of the hand
|
EOMC p355
|
|

|
boxer's fracture → fracture of distal metaphysis of 5th metacarpal
|
|
|
|
What is the management of a boxer's fracture?
|

1. if stable + minimal angulation → compression dressing x 1 week, gradual exercise, repeat radiographs after 1 week
2. if unstable + minimally angulated → ulnar gutter splint x 2-3 weeks 3. if >25 degrees angulation → reduction + plaster or fiberglass splint x 4 weeks |
Orthopedics p132
EOMC p355 |
|
|
What is the patient education for a boxer's fracture?
|
if adult, knuckle will always be less prominent when fist made
|
Orthopedics p132
|
|
|
What is a Bennett's fracture?
|
oblique fracture of the base of the 1st metacarpal that enters the carpometacarpal (CMC) joint
|
Orthopedics p132
|
|
|
What is the etiology of a Bennett's fracture?
|
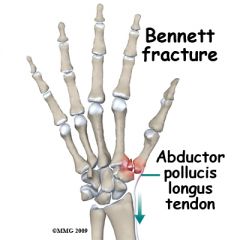
abductor pollicis longus tendon pulled proximally → causing 1st metacarpal to be displaced proximally while small medial fragment of 1st metacarpal remains attached to volar oblique ligament
|
EOMC p348
|
|
|
What is the clinical presentation of a Bennett's fracture?
|
pain, swelling, and ecchymosis at base of thumb
limited ROM |
EOMC p348
|
|
|
What is the diagnostic workup of a Bennett's fracture?
|

AP and lateral radiographs of thumb
|
EOMC p348
|
|
|
What is the management of a Bennett's fracture?
|
1. if non-displaced → thumb spica cast x 4 weeks
2. if displaced → reduction + surgical fixation *most Bennett's fractures usually requires surgery |
Orthopedics p132
EOMC p348 |
|
|
What is paronychia?
|

infection of the distal phalanx that occurs along the edge of the nail
|
Current p141
Orthopedics p122 |
|
|
What is the etiology of paronychia?
|
local trauma resulting in infection (bacterial or fungal)
if acute → think staph if chronic → think candida associated with: biting nail picking hangnail trimming cuticle onychomycosis diabetes people who have hands in water for long periods of time |
Orthopedics p122
|
|
|
What is the diagnostic workup of paronychia?
|
bacterial or fungal culture
|
|
|
|
What is a felon?
|
infection of the closed space of the pad of the distal phalanx
|
Orthopedics p122
|
|
|
What is the etiology of a felon?
|
infection of the fingertip pulp → usually staph aureus
associated with: wooden splinters minor cuts complication of paronychia |
Orthopedics p122
|
|
|
What is the clinical presentation of a felon?
|
rapidly increasing pressure and pain
erythema, swelling, and tenseness of fingertip cellulitis → tight prickling pain → abscess formation → throbbing pain, edema, increased pressure → compromised blood flow → possible necrosis |
Orthopedics p122
|
|
|
What is the clinical presentation of paronychia?
|
erythema, swelling, and tenderness of finger
|
Orthopedics p123
|
|
|
What is the management of paronychia?
|
If acute:
1. oral antibiotics 2. if abscess → I&D If chronic: 1. oral antifungals |
Orthopedics p123
|
|
|
What is the management of a felon?
|
1. early I&D
2. antibiotics for S. aureus |
Orthopedics p122
|
|
|
What are the complications of humeral shaft fracture?
|
-radial nerve injury
-brachial plexus injury -vascular injury -persistent stiffness of shoulder/elbow |
|
|
|
What is the etiology of humeral shaft fracture?
|
-acute trauma (MVA, fall on outstretched hand)
|
|
|
|
What are the symptoms/signs of humeral shaft fracture?
|
-severe pain, swelling
-deformity if displaced |
|
|
|
What diagnostics should be ordered if suspected humeral fracture?
|
-AP and lateral radiographs
-include shoulder and elbow joints |
|
|
|
What are the symptoms/signs of radial nerve injury?
|
-weakness in wrist and finger extension
-numbness in first dorsal webspace |
|
|
|
Proximal humeral fractures are most commonly seen in what patient population?
|
elderly w/ osteoporosis (especially women)
|
|
|
|
What is the etiology of radial head fracture?
|
fall on outstretched hand while elbow extended
|
|
|
|
What are the symptoms/signs of radial head fracture?
|
-pain, swelling, tenderness over radial head
|
|
|
|
What are the physical exam findings in radial head fracture?
|
-pain elicited on flexion/extension
-limited passive forearm rotation |
|
|
|
What diagnostics should be ordered for suspected radial head fracture?
|
-AP and lateral radiographs
-nondisplaced/minimally displaced fractures difficult to see on radiographs, but treat empirically if high index of suspicion |
|
|
|
What are the complications of radial head fracture?
|
-loss of extention (especially last 10-15°)
-traumatic arthritis |
|
|
|
What is the differential diagnosis of radial head fracture?
|
-elbow dislocation - diffuse pain, deformity
-olecranon process fracture of ulna -supracondyle ridge fracture of humerus |
|
|
|
What are the types of radial head fracture?
|
type I - nondisplaced/minimally displaced
-type 2 - displaced > 2mm -type 3 - comminuted |
|
|
|
What is the treatment for radial head fracture?
|
-type 1 - sling or splint for 7-10 days, early active motion
-type 2 - aspiration -> if no mechanical block to forearm rotation, treat like type I; if block, open reduction -type 3 - early excision of radial head fragments |
|
|
|
What are the associated injuries of radial head fracture?
|
-hemarthrosis
-dislocation -associated forearm/wrist injury |
|
|
|
What muscle is most commonly torn in rotator cuff tear?
|
supraspinatus
|
|
|
|
What is fat pad sign?
|
sign seen on lateral elbow radiograph
indicative of intra-articular hemorrhage which is often associated with radial head fracture |
|
|

|
fat pad sign → intra-articular hemorrhage → possible occult radial head fracture
|
|
|
|
What is the mechanism of injury for anterior/posterior shoulder dislocation?
|
anterior → fall on externally rotated, abducted arm
posterior → force directed against internally rotated arm; seizure |
Orthopedics p70
|
|
|
What is the clinical presentation of anterior/posterior shoulder dislocation?
|

prominent acromion
absence of normal fullness of humeral head severe pain upon movement anterior → anterior shoulder full, arm externally rotated, internal rotation painful posterior → anterior shoulder flat, arm internally rotated, external rotation painful |
Orthopedics p70
|
|
|
What is more common, anterior or posterior shoulder dislocation?
|
anterior (95%)
|
Orthopedics p70
|
|
|
What is a bankart lesion?
|
tear in labrum due to anterior shoulder dislocation
|
Orthopedics p72
|
|
|
What is the diagnostic workup of anterior/posterior shoulder dislocation?
|
AP and lateral radiographs
|
|
|

|
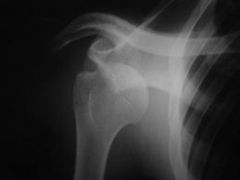
anterior shoulder dislocation
|
|
|
|
What is the management of anterior/posterior shoulder dislocation?
|
1. reduction
2. sling x few days 3. gradual active motion 4. rehabilitation exercises 5. avoid positions of known instability |
Orthopedics p74
|
|
|
After initial shoulder dislocation, in what percent of young males does redislocation occur?
|
60-80%
|
|
|
|
What is the mechanism of injury for AC joint separation?
|
fall on shoulder or direct blow to top of shoulder → driving acromion away from clavicle
|
Orthopedics p75
|
|
|
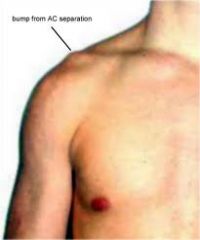
What is the clinical presentation of AC joint separation?
|
lateral clavicle elevated
swelling and tenderness over AC joint |
Orthopedics p75
|
|
|
What is the diagnostic workup of AC joint separation?
|

AP radiograph
|
Orthopedics p75
|
|

|
AC joint separation
|
|
|
|
What is the management of AC joint separation?
|
1. graded I-V where:
I = AC contusion or strain II = rupture of AC ligaments III = rupture of coracoclavicular ligaments IV and V = significant displacement 2. if incomplete separation → sling x few days + active shoulder motion as soon as tolerated 3. if grade IV or V → surgery |
Orthopedics p75
|
|
|
What is the etiology of clavicular fracture?
|
trauma
|
|
|
|
What is the clinical presentation of clavicular fracture?
|
clavicular deformity, skin tenting, tenderness
|
Orthopedics p79
|
|

|
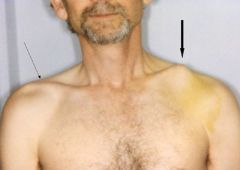
clavicle fracture
|
|
|
|
skin tenting → fracture of LT clavicle
|
|
|
|
What is the diagnostic workup of clavicular fracture?
|
AP and lateral radiograph
|
|
|

|
clavicle fracture
|
|
|
|
What is the management of clavicular fracture?
|
1. immobilization via figure-8 splint or simple sling x 4-5 weeks for child and 8 weeks for adult
2. splint must be periodically retightened 3. splint discomfort can be relieved by lying down and abducting arms 4. if fracture lateral to coracoclavicular ligament + minimal displacement → only use sling 5. if fracture lateral to coracoclavicular ligament + displacement → refer to orthopedic specialist due to high rate of nonunion 6. prominence at fracture site often persists in adult but nonunion rare |
Orthopedics p79
|
|
|
What is the common name for medial epicondylitis?
|
golfer's elbow
|
|
|
|
What is the common name for lateral epicondylitis?
|
tennis elbow
|
|
|
|
What is the etiology of medial/lateral epicondylitis?
|
unknown
direct blow overuse → repetitive use of flexors or extensors of forearm leads to degeneration (tendinosis) |
Orthopedics p92
|
|
|
What is the clinical presentation of medial/lateral epicondylitis?
|
gradual onset, dull ache, pain with rotation
medial epicondyltis → pain at common flexor tendon, increases with flexion of hand against resistance lateral epicondylitis → pain at common extensor tendon, increases with extension of hand against resistance |
Orthopedics p92
|
|
|
What is the diagnostic workup of medial/lateral epicondylitis?
|
none
|
|
|
|
What is the management of medial/lateral epicondylitis?
|
1. usually self-limited
2. NSAIDs 3. rest 4. ice after activity 5. avoid offending activity 6. exercise program of gentle stretching and strengthening as pain subsides 7. steroid/lidocaine injection usually provides permanent or long-lasting relief 8. surgery if refractory to treatment |
Orthopedics p92
|
|
|
What test would you perform for suspected anterior/posterior shoulder dislocation?
|
apprehension sign → positive if look of apprehension
|
|
|
|
What is gamekeeper's thumb?
|
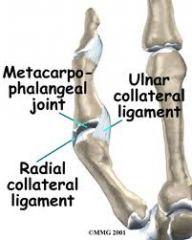
chronic injury to ulnar collateral ligament (UCL) connecting 1st metacarpal to proximal phalanx
|
Orthopedics p331
|
|
|
What is the mechanism of injury for gamekeeper's thumb?
|
acute → fall on hand → forced abduction or hyperextension of proximal phalanx; skiers
chronic → repeated hyperabduction; gamekeepers may cause torn UCL or avulsion fracture |
Orthopedics p331
|
|
|
What is the clinical presentation of gamekeeper's thumb?
|
chronic:
history of instability MCP joint effusion, tenderness weakness with pinch |
Orthopedics p331
|
|
|
What is the diagnostic workup of gamekeeper's thumb?
|

thumb radiograph to R/O avulsion fracture
|
Orthopedics p331
|
|
|
What is the management of gamekeeper's thumb?
|
Acute:
1. if partial tear or non-displaced avulsion fracture → cast x 5 weeks 2. if complete tear → surgery Chronic: 1. if associated with traumatic arthritis → ligament reconstruction 2. if associated with degenerative arthritis → arthrodesis |
Orthopedics p331
|
|
|
What is the name for acute gamekeeper's thumb?
|
skier's thumb
|
Orthopedics p331
|
|
|
What is another name for mallet finger?
|
baseball finger
|
Orthopedics p327
|
|
|
What is mallet finger?
|
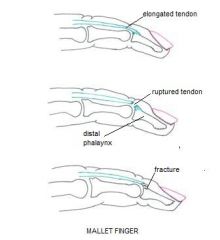
avulsion of the extensor tendon where it inserts at the base of distal phalanx (or possibly associated avulsion fracture)
|
Orthopedics p327
|
|
|
What is the mechanism of injury for mallet finger?
|
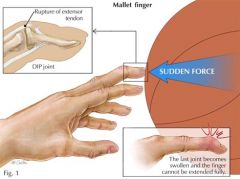
blow to tip of extended finger → forced flexion of DIP joint
|
Orthopedics p327
|
|
|
What is the clinical presentation of mallet finger?
|

flexed distal phalanx
swelling and tenderness of dorsal DIP joint lost of active extension of distal phalanx if long-standing injury, hyperextension of PIP joint may occur → swan neck deformity |
Orthopedics p327
|
|
|
What is the diagnostic workup of mallet finger?
|
finger radiograph to R/O avulsion fracture
|
Orthopedics p327
|
|
|
What is the management of mallet finger?
|

1. if no avulsion fracture or small avulsion fracture → splint x 5 weeks with slight hyperextension of DIP
2. if large displaced fracture + joint stability → same treatment as above 3. if large displaced fracture + instability → surgery 4. redness, swelling, and tenderness may last 2-3 months |
Orthopedics p327
|
|

|
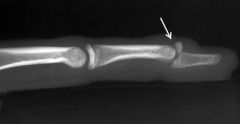
mallet finger
|
|
|
|
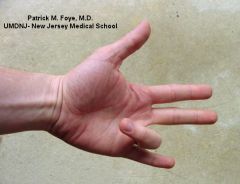
What is trigger finger?
|
catching, locking or snapping of involved finger flexor tendon
|
|
|
|
What is the mechanism of injury for trigger finger?
|
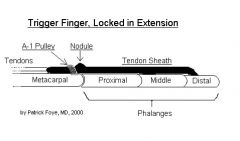
swelling of flexor tendon and sheath
if child + thumb → think congenital if multiple fingers → think rheumatoid disease |
Orthopedics p114
|
|
|
What is the clinical presentation of trigger finger?
|
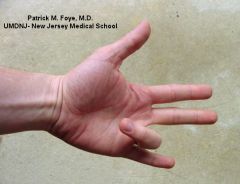
nodular thickening, swelling and tenderness near MCP joint
finger may lock in flexion or extension if locked in flexion, manipulation to unlock it may produce palpable snap worse with rest, better with activity |
Orthopedics p114
|
|
|
What is the diagnostic workup of trigger finger?
|
none
|
|
|
|
What is the management for trigger finger?
|
1. often self-limiting
2. splinting of DIP 3. surgical release |
Orthopedics p115
|
|
|
trigger finger
|
|
|
|
What is the etiology of frozen shoulder?
|
cause unknown
may be associated with rotator cuff tendinitis, bicipital tendonitis, reflex symphathetic dystrophy associated with ischemic heart disease, lung disease, and thyroid disease more common in women and diabetics |
|
|
|
What is the clinical presentation of frozen shoulder?
|
insidious onset of pain in 5th decade
restriction ROM 3 stages: 1. freezing 2. frozen 3. thawing tenderness around rotator cuff LOSS OF INTERNAL ROTATION (active and passive) |
|
|
|
What is the diagnostic workup of frozen shoulder?
|
radiograph to R/O posterior shoulder dislocation
|
|
|
|
What is the management of frozen shoulder?
|
1. pain relief
2. restoration of motion 3. moist heat 4. analgesics 5. sedation 4. injection of steroid 5. exercises on hourly basis 6. recovery usually takes >6 months |
|
|
|
What is another name for frozen shoulder?
|
adhesive capitulitis
|
|
|
|
What is frozen shoulder?
|
shoulder disorder characterized by insidious onset of pain and restriction of motion
|
|
|
|
What is the etiology of navicular fracture?
|
fall on outstretched hand → hyperextension of wrist
|
|
|
|
What are the complications of navicular fracture?
|
AVN → arthritis
|
|
|
|
What is the clinical presentation of navicular fracture?
|
pain in anatomical snuffbox
|
|
|
|
What is a tuft fracture?
|
fracture of distal phalanx
usually caused by crush injury |
|
|
|
What is the most common complication of a humeral fracture?
|
radial nerve injury
|
|
|
|
What is hallux valgus?
|
lateral deviation of great toe at MTP joint
|
Orthopedics p260
|
|
|
What is a bunion?
|
bony and soft tissue enlargement over medial aspect of head of 1st MTP associated with hallux valgus
|
Orthopedics p260
|
|
|
What is the etiology of hallux valgus?
|
cause unknown
associated with: hereditary factors tight-fitting shoes high heels |
Orthopedics p260
|
|
|
What is the clinical presentation of hallux valgus?
|
affects women 10x more than men
1st MTP joint: pain and tenderness when wearing tight-fitting shoes or high-heels erythema bunion → bony and soft tissue enlargement over medial aspect of head of 1st MTP lateral deviation of great toe at MTP joint possible hyperextension and callus formation on 2nd toe |
Orthopedics p260
|
|

|
hallux valgus
|
|
|

|
hallux valgus → with hyperextension of 2nd toe
|
|
|
|
What is the diagnostic workup of hallux valgus?
|
AP radiograph →
lateral displacement of proximal phalanx of great toe medial exostosis of head of 1st metatarsal possible degeneration of MTP joint |
Orthopedics p260
|
|

|
hallux valgus
|
|
|
|
What is the management of hallux valgus?
|
1. goal → relieve pressure over bunion
2. do not wear tight-fitting shoes, high-heels, or tight-fitting stockings 3. if hyperextended 2nd toe → wear "extra-depth" shoe or use splint to separate 1st and 2nd toes 4. if acute pain → rest and moist heat 5. if disabling pain with deformity → surgery with realignment of great toe and excision of exostosis |
Orthopedics p260-261
|
|
|
What is the patient education for hallux valgus?
|
1. >50% of cases respond by changing shoes
2. requires permanent lifestyle change if not surgical treated 3. do not wear tight-fitting shoes, high-heels, or tight pantyhoes |
Orthopedics p261
|
|
|
What is morton's neuroma?
|
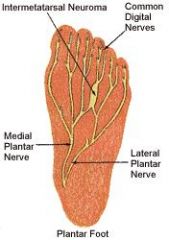
perineural fibrosis of the plantar nerve where the medial and lateral plantar branches communicate between 3rd and 4th metatarsals → painful fusiform (spindle-like) swelling of plantar nerve
|
Orthopedics p258
|
|
|
What is the etiology of morton's neuroma?
|
cause unknown
associated with: repetitive trauma wearing tight shoes |
Orthopedics p258
|
|
|
What is the clinical presentation of morton's neuroma?
|
burning pain between 3rd and 4th metatarsals (sometimes 2nd and 3rd)
possible numbness aggravated by tight shoe alleviated by removing shoe and massaging foot tenderness on pressure between 3rd and 4th metatarsals or transvere compression of forefoot possible decreased sensation |
Orthopedics p258
|
|
|
Where is morton's neuroma most commonly found?
|
between 3rd and 4th metatarsals
|
|
|
|
What is the diagnostic workup of morton's neuroma?
|
none → diagnosis made clinically
|
Orthopedics p258
|
|
|
What is the management of morton's neuroma?
|

1. for symptomatic relief → NSAIDs or local injection of lidocaine/steroid into web area from dorsal approach
2. pad separating 3rd and 4th metatarsals 3. do not wear tight-fitting shoes 4. surgical removal often necessary |
Orthopedics p258
|
|
|
What is the patient education for morton's neuroma?
|
do not wear tight-fitting shoes
|
Orthopedics p258
|
|
|
What is the plantar fascia?
|
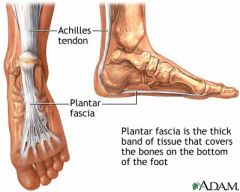
thick band of connective tissue extending from calcaneus to proximal phalanges; involved in gait
|
Orthopedics p253
|
|
|
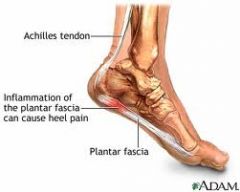
What is the plantar fasciitis?
|
inflammation of plantar fascia
|
|
|
|
What is the etiology of plantar fasciitis?
|
probable overuse with development of degeneration and microtears
associated with: tight heel cords (i.e. reduced dorsiflexion) obesity running |
Orthopedics p253
|
|
|
What is the clinical presentation of plantar fasciitis?
|
affects men and women equally
pain → usually at medial tubercle of calcaneous where plantar fascia originates but sometimes along medial longitudinal arch aggravated with first steps of morning or after prolonged sitting or after weight-bearing activities tenderness with direct pressure or sometimes dorsiflexion if bilateral → may be associated with RA, gout, AS |
Orthopedics p253
|
|
|
List disorders associated with bilateral plantar fasciitis.
|
RA
gout ankylosing spondylitis |
Orthopedics p253
|
|
|
What is the diagnostic workup of plantar fasciitis?
|
radiographs →
often normal possible osteophyte on calcaneous (but not cause of pain) |
Orthopedics p254
|
|
|
What is the management of plantar fasciitis?
|
1. for symptomatic relief → ice, NSAIDs, lidocaine/steroid injection
2. taping and pads slightly beneficial 3. cast x 6 weeks very beneficial 4. night splint holding foot in dorsiflexion if refractory 5. exercises to stretch heel cord and plantar fascia 6. if refractory after 6-12 months → surgery with detachment of plantar fascia at calcaneous |
Orthopedics p254
|
|
|
What is the patient education of plantar fasciitis?
|
1. medical treatment effective in 95% of cases
2. improvement may take up to 1-2 years 3. OTC orthoses are as effective as more expensive ones 4. do not perform exercises if in acute pain |
Orthopedics p255
|
|
|
Name the bones of the foot.
|

calcaneous
talus navicular cuboid medial cuneiform intermediate cuneiform lateral cuneiform metatarsals phalanges |
|
|
|
What is another name for onychocryptosis?
|
ingrown toenail
|
|
|
|
What is the etiology of calcaneous fracture?
|
usually fall on heel
|
Orthopedics p268
|
|
|
What is the clinical presentation of calcaneous fracture?
|
severe pain and swelling of heel
swelling may lead to blistering and skin necrosis |
Orthopedics p269
|
|
|
What is the diagnostic workup of calcaneous fracture?
|
radiograph → AP and lateral of hindfoot; AP and mortise of ankle
usually crushed displacement of fragments varies |
Orthopedics p269
EOMC p633 |
|
|
What is the management of calcaneous fracture?
|
Initial management to control swelling and hemorrhage:
1. compression dressing, ice, elevation 2. do not apply cast immediately after injury → only intensifies pain and swelling Later management: 1. if minimally displaced → cast x 2-3 weeks + immobilization or crutches 2. remove cast ASAP but do not allow weight bearing for 6-8 weeks 3. eversion and inversion exercises 4. prolonged immobility is not advised 5. if displaced → same treatment as above or open/closed reduction 6. if symptoms persist → surgery |
Orthopedics p269
|
|
|
What is the patient education for calcaneous fracture?
|
1. temporary disability may persist 1-2 years
2. some permanent impairment common → often widening of heel; some restriction of eversion and inversion |
Orthopedics p269
|
|
|
What disorder occurs in 10% of calcaneous fractures?
|
compression fracture of lumbar spine
palpate spine for tenderness if tenderness → order AP and lateral spinal radiographs |
EOMC p633
|
|
|
What is the etiology of phalangeal fractures?
|
direct trauma to phalange
|
EOMC p639
|
|
|
What is the clinical presentation of phalangeal fracture?
|
pain, swelling, ecchymosis
|
EOMC p639
|
|
|
What is the diagnostic workup of phalangeal fracture?
|
AP radiograph
|
EOMC p639
|
|

|
fracture of 5th proximal phalanx
|
|
|
|
What is the management of phalangeal fractures?
|
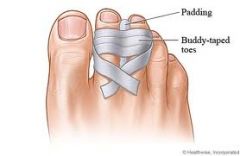
1. if undisplaced → place gauze pad between injured toe and medially adjacent toe and buddy tape them together x 3-4 weeks (change as often as needed)
3. closed or open reduction rarely necessary → but consider for markedly angulated fractures, fractures involving MTP joints, fractures involving interphalangeal joints of great toe |
Orthopedics p271
EOMC p639 |
|
|
What is the etiology of onychocryptosis?
|
soft tissue overgrows and obliterates nail sulcus
associated with: improper nail trimming → small nail spike irritates soft tissue → infection cleaning nail with tools that penetrate skin tight-fitting shoes and stockings bony deformities |
Orthopedics p263
|
|
|
What is the clinical presentation of onychocryptosis?
|
usually affects great toe
soft tissue overgrowth + normal nail pain, inflammation, pus |
Orthopedics p263
|
|
|
What is the diagnostic workup for onychocryptosis?
|
none
|
Orthopedics p263
|
|
|
What is the management of onychocryptosis?
|

1. antibiotics
2. soak nail 3. elevate nail edge with cotton wad until grows beyond soft tissue reaction → must be patient since takes 3 months for nail to grow 1 cm 4. if refractory → surgery usually by removing one or both nail margins |
Orthopedics p263
|
|
|
What is the patient education for onychocryptosis?
|
for prevention:
1. use proper nail-trimming technique → always trim nail straight across, do not round or cut too short 2. wear properly fitted shoes and stockings |
Orthopedics p263
|
|

|
onychocryptosis
|
|
|
|
What are the Ottowa rules for ordering ankle radiographs?
|
Unable to bear weight for 4 steps + one of the following:
1. bony tenderness at posterior edge of medial malleolus 2. bony tenderness at posterior edge of lateral malleolus |
|
|
|
What are the Ottowa rules for ordering foot radiographs?
|
Unable to bear weight for 4 steps + one of the following:
1. bony tenderness over the navicular 2. bony tenderness over the base of the 5th metatarsal |
|
|
|
|
|
|
|
What are the Ottowa rules for ordering knee radiographs?
|
Any of the following:
1. >55y/o 2. inability to bear weight for 4 steps following injury and in ER 3. patellar tenderness 4. fibular head tenderness 5. inability to flex knee to 90 degrees |
|
|
|
What is another name for chondromalacia patella?
|
patellofemoral pain syndrome
|
Orthopedics p227
|
|
|
Waht is chondromalacia patella?
|
pain over anterior aspect of knee in absence of other identifiable pathology (i.e. diagnosis of exclusion)
|
Orthopedics p227
|
|
|
What is the clinical presentation of chondromalacia patella?
|
usually affects teenagers and young adults
pain near or beneath patella worse when walking stairs, prolonged sitting with knee flexed often bilateral crepitus |
Orthopedics p227
|
|
|
What is the etiology of chondromalacia patella?
|
unknown cause
associated with: any anatomic abnormality or injury causing irregular movement of patella quadriceps imbalance high-riding patella genu valgum direct trauma vigorous squatting overuse |
Orthopedics p226
|
|
|
What is the management of chondromalacia patella?
|
1. reassure patient that problem is benign
2. treat underlying cause if present 3. avoid flexion load 4. NSAIDs 5. ice after activity 6. moist heat 7. exercise program 8. often resolves spontaneously |
Orthopedics p226
|
|
|
What is a Baker's cyst?
|
enlargement of semimebranous bursa normally present in medial aspect of popliteal fossa
|
Orthopedics p220
|
|
|
What is the etiology of a Baker's cyst?
|

if child → primary
if adult → secondary to intra-articular knee disorder (posterior tear of medial meniscus, OA, or RA) which causes increase in joint fluid → fluid fills bursa |
Orthopedics p220
|
|
|
What is the clinical presentation of Baker's cyst?
|

cyst in medial aspect of popliteal fossa
associated knee effusion if ruptures, may resemble thrombophlebitis or venous thrombosis! |
Orthopedics p220
|
|
|
What is the diagnostic workup of a Baker's cyst?
|
radiographs normal
ultrasound studies confirm benign cyst |
Orthopedics p221
|
|
|
What is the management of a Baker's cyst?
|
1. if child → self-limited in 1-2 years
2. if adult + asymptomatic → observation 3. if adult + symptomatic/burst → aspiration +/- injection of triamcinolone 20-40mg anteriorly, rest, elevation |
Orthopedics p221
|
|
|
What is Osgood-Schlatter's syndrome?
|
disorder involving growing tibial tuberosity
|
Orthopedics p231
|
|
|
What is the etiology of Osgood-Schlatter's syndrome?
|
cause unknown
traumatically produced lesion that occurs at attachment of patellar tendon to tibial tuberosity affects adolescents, 3x more males than females, usually evident between 8-15y/o |
Orthopedics p231
|
|
|
What is the clinical presentation of Osgood-Schlatter's syndrome?
|
local pain, swelling and tenderness over tibial tubercle
pain worsened by activity, walking stairs, squatting, knee extension against resistance |
Orthopedics p231
|
|
|
What is the diagnostic workup of Osgood-Schlatter's syndrome?
|
knee radiograph usually normal
possible separation and fragmentation of proximal tibial epiphysis |
Orthopedics p231
|
|
|
What is the management of Osgood-Schlatter's syndrome?
|
1. self limited → resolving with closure of proximal tibial growth plate
2. remove stress on tendon 3. stretching, ice, and NSAIDs after activity 4. if refractory → knee splint and temporary immobilization |
Orthopedics p231
|
|
|
What is the etiology of pre-patellar bursitis?
|
direct trauma
recurrent trauma → kneeling (housemaid's knee) |
Orthopedics p234
|
|
|
What is the clinical presentation of pre-patellar bursitis?
|

swelling around patella
|
|
|
|
What is the diagnostic workup of pre-patellar bursitis?
|
none
|
|
|
|
What is the management of pre-patellar bursitis?
|
If acute:
1. rest 2. aspiration for pain relief or suspected infection 3. repeated aspirations since fluid often returns Chronic: 1. possible excision |
Orthopedics p234
|
|
|
What is a Jones fracture?
|
fracture in proximal 1/3 of 5th metatarsal
|
Approach To The Orthopedic Patient handout
|
|
|
What is a Dancer's fracture?
|
avulsion fracture of the 5th metatarsal
|
|
|
|
What are the complications of a Jones fracture?
|
high rate of non-union due to lower vascularity → treat aggressively!
|
Approach To The Orthopedic Patient handout
|
|
|
What is a boxer's fracture?
|
fracture of proximal metacarpal → usually 5th metacarpal
|
|
|
|
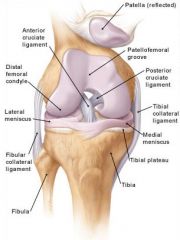
What are the medial and lateral meniscus of the knee made of?
|
fibrocartilage
|
|
|
|
What are 4 important ligaments of the knee?
|
medial collateral ligament (MCL)
lateral collateral ligament (LCL) anterior cruciate ligament (ACL) posterior cruciate ligament (PCL) |
|
|
|
What test is performed for suspected achilles tendon rupture?
|
Thompson's test → positive if squeezing calf does not produce plantar flexion of foot
|
|
|
|
What is the mechanism of injury for achilles tendon rupture?
|
spontaneous rupture due to gradual degeneration of achilles tendon → often caused by jumping, pushing off forefoot
high incidence if taking quinolones |
Orthopedics p257
|
|
|
What is the clinical presentaiton of achilles tendon rupture?
|
hear "pop"
walk flat footed; unable to stand on ball of foot hemorrhage palpable sulcus at rupture site tenderness excessive passive dorsiflexion positive Thompson's test |
Orthopedics p257
|
|
|
What is the diagnostic workup of achilles tendon rupture?
|
none
|
|
|
|
What is the management of achilles tendon rupture?
|
1. refer to orthopedist immediately for surgery
2. refrain from excessive activity for 1 year 3. recurrence common |
Orthopedics p257
|
|
|
What is the mechanism of medial/lateral meniscus tear?
|
flexion with external rotation or extension with internal rotation
|
Orthopedics p217
|
|
|
What is the clinical presentation of medial/lateral meniscus tear?
|
history of twisting injury to knee with foot in weight-bearing position
popping or tearing sensation severe pain localized medially or laterally depending on meniscus injured joint effusion occurs gradually over several hours acute symptoms replaced by intermittent locking, buckling, giving out, swelling, and mild pain difficulty walking stairs or squatting pain at joint line limited ROM positive McMurray test |
Orthopedics p217
|
|
|
What is the diagnostic workup of medial/lateral meniscus tear?
|
radiograph to R/O fracture
|
Orthopedics p218
|
|
|
What is the management of medial/lateral meniscus tear?
|
1. conservative treatment initially
2. RICE -Robert Jones compression dressing 3. crutches 4. quadricep-strengthening exercises x 2-4 weeks 5. gentle ROM exercises after 2-3 days (swimming is excellent) 6. resume weight-bearing as pain subsides 7. MRI is continued pain 8. surgery is continued pain or irreducible locking |
Orthopedics p218
|
|
|
Which is more common, medial or lateral meniscus tear?
|
medial meniscus
10x more common because its more firmly attached |
Orthopedics p217
|
|
|
What is the most common knee injury?
|
meniscus tear
|
|
|
|
What is the mechanism of injury for ACL/PCL sprain?
|
twisting injuries
|
Orthopedics p222
|
|
|
What is the mechanism of injury for MCL/LCL sprain?
|
MCL → valgus stress against the knee
LCL → varus stress against the knee |
Orthopedics p222
|
|
|
What is the clinical presentation of ACL/PCL sprains?
|
popping or tearing sensation
inability to bear weight immediate swelling due to hemorrhage positive anterior drawer sign or lachman test if ACL tear positive posterior drawer sign if PCL tear |
|
|
|
What is the clinical presentation of MCL/LCL sprains?
|
inability to bear weight
ecchymosis within few days positive valgus stress test if MCL tear positive varus stress test if LCL tear |
Orthopedics p223
|
|
|
Which is more painful, incomplete or complete knee ligament tears?
|
incomplete
|
Orthopedics p223
|
|
|
What is the diagnostic workup of ACL/PCL and MCL/LCL sprains?
|
radiograph of knee to R/O fracture/avulsion fracture
|
Orthopedics p223
|
|
|
What is the management for ACL/PCL sprains?
|
1. dependent on age and lifestyle of patient
2. if minor sprain → ice, compression dressing, elevation x 2-3 days, then exercises 3. if highly active → surgery |
Orthopedics p223
|
|
|
What is the management for MCL/LCL sprains?
|
1. rest, ice, compression dressing
2. hinge brace 3. early rehabilitaiton 4. if complete LCL tear → surgery |
Orthopedics p223
|
|
|
What is the mechanism of injury for patellar dislocation?
|
lateral dislocation can occur if sudden valgus stress to knee or direct blow to medial aspect of patella
|
Orthopedics p229
|
|
|
What is the clinical presentation of patellar dislocation?
|

laterally displaced patella
|
Orthopedics p229
|
|
|
What is the diagnostic workup of patellar dislocation?
|

knee radiograph to R/O fracture
|
Orthopedics p229
|
|
|
What is the management of patellar dislocation?
|
1. reduction → lift heel of leg off examining table + gentle pressure against patella
2. knee immobilizer x 2-3 weeks 3. quadriceps exercises ASAP |
Orthopedics p229
|
|
|
Twisting knee injury + acute hemarthrosis usually indicates?
|
ACL tear
|
Orthopedics p229
|
|
|
What is the mechanism of injury for a patella fracture?
|
fall onto knee or direct blow
|
Orthopedics p236
|
|
|
What is the management of a patella fracture?
|
Undisplaced:
1. compression dressing 2. splint or cast x 5-6 weeks 3. exercise program Displaced → surgery |
Orthopedics p236
|
|
|
What is the diagnostic workup of patellar fracture?
|

AP and lateral radiographs of knee
|
|
|
|
What is the most common cause of kyphosis/gibbus?
|
compression fractures from osteoporosis
|
Mosbys p708
Orthopedics p161 |
|
|
Where do 95% of lumbar disc lesions occur?
|
L4 and L5 disc spaces
|
Orthopedics p145
|
|
|
List the parts of an intervertebral disc.
|
outer portion → annulus fibrosus
inner portion → nucleus pulposus |
|
|
|
Does a lumbar disc herniation affect the spinal root above or below it?
|
below
|
Orthopedics p146
|
|
|
Which part of the annulus fibrosus is most susceptible to nucleus propulsus herniation?
|
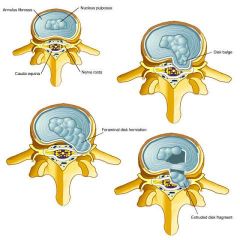
posterolateral
|
Orthopedics p145
|
|
|
What is the clinical presentation of lumbar disc herniation?
|
lower back pain → localized near disc, one-sided, deep, aching, may refer to iliac crest or buttock, exacerbated with lateral flexion toward affected side
if nerve root compression, radicular pain → radiates over buttock, down posterior or posterolateral leg |
Orthopedics p147
|
|
|
List 5 types of lumbar disc disease.
|
1. herniation without compression of nerve root
2. herniation with compression of nerve root 3. cauda equina syndrome 4. chronic degenerative disease with or without leg symptoms 5. spinal stenosis |
Orthopedics p147
|
|
|
How can you differentiate back pain due to muscle strain and back pain due to intervertebral disc disease?
|
during lateral flexion:
if muscle strain → pain increases with flexion away from affected side if intervertebral disc disease → pain increases with flexion toward affected side |
Orthopedics p144
|
|
|
If back pain or radicular pain does not improve with bed rest, what should be considered?
|
spinal cord tumor
|
Orthopedics p147
|
|
|
What is the treatment for lumbar disc disease?
|
1. NSAIDs, analgesics, and moist heat as needed
2. if radicular pain → best rest x 5-10 days 3. careful exercise program 4. physical therapy 5. if severe or progressive neurological deficits or refractory to treatment after 6 weeks → surgery |
Orthopedics p149
|
|
|
What is the treatment for chronic degeneration of lumbar disc?
|
1. NSAIDs, analgesics, moist heat, rest
2. lumbrosacral corset 3. postural training 4. exercise program or physical therapy |
Orthopedics p151
|
|
|
What is the etiology of acute lumbosacral strain?
|
trauma
if chronic back pain, consider risk factors |
|
|
|
What is the clinical presentation of acute lumbosacral strain?
|
pain and tenderness over affected area
|
Orthopedics p153
|
|
|
What are the risk factors for chronic lumbar back pain?
|
poor muscular tone
obesity smoking lack of daily exercise incorrect postural and lifting habits high-heels |
Orthopedics p153
|
|
|
What is the treatment for acute lumbosacral strain?
|
If simple:
1. rest x 1-2 days followed by physical activity 2. mild analgesics 3. proper lifting and bending habits If complicated: 1. encourage weight loss, smoking cessation 2. daily postural exercises 3. exercise program *treatment based on symptoms not radiographs |
Orthopedics p153
|
|
|
What is "bamboo spine"?
|
complication of ankylosing spondylitis characterized by fusion of vertebrae
|
|
|
|
List the number of each type of vertebra.
|

cerivcal → C1-C7 (C1 atlas, C2 axis, C7 vertebra prominens)
thoracic → T1-T12 lumbar → L1-L5 sacral → S1-S5 (fused) coccyx |
|
|

|
spondylolisthesis (at L4-L5)
|
|
|
|
What is spondylitis?
|
inflammation of the vertebrae
|
|
|
|
What is spondylolysis?
|
stress fracture of pars interarticularis
|
|
|
|
What is spondylolisthesis?
|
anterior displacement of a vertebra in relation to the one below
|
|
|
|
What is the etiology of spondylolysis?
|
hereditary predisposition → thin vertebral bone
sports (especially gymnastics and football) → impact loading and hyperextension of lumbar spine → stress fracture of pars interarticularis |
Orthopedics p154
|
|
|
What is the etiology of spondylolisthesis?
|
spondylolysis
congenital traumatic degenerative pathologic → metabolic bone disease, tumor |
Orthopedics p154
|
|
|
What is the most common cause of spondylolisthesis?
|

bilateral stress fracture of pars interarticularis → spondylolysis → spondylolisthesis
|
Orthopedics p155
|
|
|
What is the clinical presentation of spondylolysis and spondylolisthesis?
|
often asymptomatic
pediatric: often no pain paraspinal muscle spasm → hamstring tightness → postural deformity and gait abnormality adult: low back pain increased lordosis palpable step-off tenderness in affected area neurologic deficits rare |
Orthopedics p155
|
|
|
Where does spondylolisthesis most commonly occur?
|
L5-S1
|
Orthopedics p154
|
|
|
What is the diagnostic work-up of spondylolisthesis?
|
lateral radiograph of lumbosacral spine
|
|
|
|
What is the grading scale for spondylolisthesis?
|
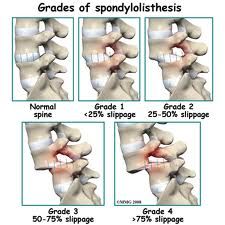
Grade 1 → <25% anterior displacement
Grade 2 → 25-50% anterior displacement Grade 3 → 50-75% anterior displacement Grade 4 → >75% anterior displacement |
Orthopedics p154
|
|
|
What are the complications of spondylolysis?
|
spondylolisthesis
|
Orthopedics p154
|
|
|
What are the complications of spondylolisthesis?
|
nerve compression
spinal stenosis |
|
|
|
What is the treatment for spondylolysis and spondylolisthesis?
|
pediatric:
1. goal → heal stress fracture 2. restrict activity for several months 3. back brace adult or nonunion: 1. NSAIDs 2. rest 3. weight loss 4. exercise program → hamstring exercises 5. intermittent use of back brace 6. if refractory or progressive → surgery |
Orthopedics p154
|
|
|
What is the patient education for work-related low back pain?
|
1. few days rest
2. mild analgesics 3. educate about proper posture, bending, and lifting 4. use chair with good lumbar support and armrests; temporarily avoid bending and lifting 5. encourage early exercise → walking, biking, swimming followed by exercise program 7. avoid passive treatment → heat, massage 8. encourage return to work 9. if refractory to treatment after 6-8 weeks → refer to specialist |
Orthopedics
|
|
|
What is diagnostic workup of Reiter's syndrome?
|
HLA-B27 antigen → positive 85%
ESR → elevated |
Orthopedics p167
|
|
|
What is ankylosing spondylitis?
|
type of seronegative spondyloarthopathy
chronic arthritis of axial skeleton |
|
|
|
What is costochondritis?
|
inflammation of the junctions where cartilage connects ribs to sternum
|
|
|
|
What is the clinical presentation of costochondritis?
|
chest pain → musculoskeletal chest pain localized near sternum → pain on palpation of chest wall that increases with breathing/movement
|
|
|
|
What is the management of costochondritis?
|
self-limited
NSAIDs ice/heat avoid exacerbating activities |
|
|
|
What is the etiology of costochondritis?
|
usually idiopathic
chest wall trauma viral infection arthritis → ankylosing spondylitis, psoriatic arthritis fibromyalgia common cause of chest pain in adolescents |
|
|
|
What is the diagnostic workup of costochondritis?
|
R/O other causes of chest pain
|
|
|
|
What is the difference between costochondritis and Tietze's syndrome?
|
Tietze's syndrome is a more severe form of costochondritis that is characterized by SWELLING of the costal cartilages
|
|
|
|
What is the etiology of rib fracture?
|
usually MVA causing blunt thoracic trauma
|
EMED Current
|
|
|
What is the clinical presentation of rib fracture?
|
localized pain
pain with inspiration crepitus |
EMED Current
|
|
|
What is the diagnostic workup of rib fracture?
|
PA and lateral CXR
*though 50% aren't detected on CXR |
EMED Current
|
|
|
What are the complications of rib fracture?
|
pneumothorax
hemothorax hypoventilation atelectasis pneumonia |
EMED Current
|
|
|
What is the management for rib fracture?
|
1. rapid mobilization
2. respiratory support 3. pain management |
EMED Current
|
|
|
What is scoliosis?
|
lateral curvature of the spine
|
Orthopedics p158
|
|
|
What is the etiology of scoliosis?
|
if structural (i.e.fixed, fail to correct with lateral flexion) → usually idiopathic, but also congenital abnormalities, neurofibromatosis, neurologic or myopathic conditions
if non-structural (i.e. flexible, correct with lateral flexion) → compensatory mechanism secondary to leg length discrepancy, acute lumbar disc disease, or local inflammation 6x more common in females than males usually occurs between 10-13y/o |
Orthopedics p158
|
|
|
What is the management of scoliosis?
|
if nonstructural:
1. treat primary cause if structural: 1. refer to specialist 2. if <20 degrees → frequent observation 3. if >20 degrees → spinal bracing via Miwaukee brace or thoracolumbosacral orthotic 4. brace worn 23 hours per day 5. exercises performed in brace 6. if >45 degrees → surgery |
Orthopedics p158
|
|
|
What is the clinical presentation of scoliosis?
|

asymptomatic
lateral curvature of the spine right thoracic curves most common |
Orthopedics p158
|
|
|
What is the diagnostic workup of scoliosis?
|

standing radiograph of the spine
|
Orthopedics p158
|
|
|
What are the complications of scoliosis?
|
pain, deformity, disability, cardiopulmonary compromise
|
Orthopedics p160
|
|
|
What is the patient education for scoliosis?
|
1. spinal brace may have to be worn for >2 years
2. bracing does not eliminate curve but prevents progression 3. surgery may cause loss of spine motion 4. if >25 degree curve + pregnant → curve may increase |
Orthopedics p161
|
|
|
What is kyphosis?
|
posterior curvature of the spine
|
Orthopedics p161
|
|
|
What is the etiology of kyphosis?
|
diseases of disc and vertebral bodies
compression fractures from osteoporosis congenital (rare) trauma radiation surgery if senile kyphosis → thoracic disc degeneration → wedging if adolescent → often minor muscle imbalance and weakness |
Orthopedics p161
|
|
|
What is the clinical presentation of kyphosis?
|
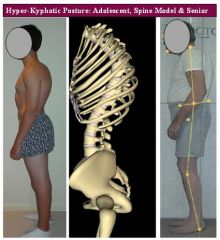
poor posture
fatigue pain posterior curvature of spine local tenderness |
Orthopedics p161
|
|
|
What is the diagnostic workup of kyphosis?
|
lateral radiograph of spine
|
Orthopedics p161
|
|
|
What is the management of kyphosis?
|
if adolescent:
1. full time brace x 1 year then night brace x 1 year 2. postural exercises → hamstrings, pelvic tilt if any age: 1. if severe deformity with pain or neurological symptoms → surgery |
Orthopedics p161
|
|
|
What is the common name for hyperextension/hyperflexion of the cervical spine?
|
whiplash
|
|
|
|
What is the etiology of whiplash?
|
usually MVA causing sudden hyperextension of neck
|
EMED Current
|
|
|
What is the clinical presentation of whiplash?
|
neck pain, muscle spasm, HA, hoarseness, dysphagia 12-24 hours following trauma
neck tenderness and limited ROM |
EMED Current
|
|
|
What is the diagnostic workup of whiplash?
|
AP and lateral radiographs of cervical spine
|
EMED Current
|
|
|
What is the management of whiplash?
|
1. if persistent cervical spine tenderness along midline (i.e. possible ligament instability) → rigid cervical collar 24 hours/day x 7-10 days
2. analgesics 3. muscle relaxants 4. heat 5. re-examination in 7-10 days |
EMED Current
|
|
|
What is the clinical presentation of spinal fracture?
|
if no spinal cord injury:
focal pain and tenderness over vertebral column no neurological deficits If spinal cord injury: neurological deficits |
EMED Current
|
|
|
What is the diagnostic workup of spinal fracture?
|
AP and lateral radiographs of spine
|
EMED Current
|
|
|
What is the management of spinal fracture?
|
1. immobilization on spinal board with cervical collar if being transported
2. analgesics 3. hospitalization |
EMED Current
|
|
|
How is most commonly affected by ankylosing spondylitis?
|
males between 20-40y/o
|
|
|
|
What drug is most commonly used to treat ankylosing spondylitis?
|
indomethacin
|
|
|
|
What is the clinical presentation of trochanteric bursitis?
|
pain over trochanter that radiates down iliotibial tract to lateral aspect of thigh and knee
local point tenderness pain with hip motion, especially internal rotation and abduction |
|
|
|
What is the diagnostic workup of trochanteric bursitis?
|
radiographs normal
|
Orthopedics p205
|
|
|
What is the management of trochanteric bursitis?
|
1. NSAIDs or steroid/lidocaine injection
2. moist heat 3. rest |
Orthopedics p205
|
|
|
What is the etiology of aseptic necrosis (AVN) of the hip?
|
idopathic in most cases
associated with: hip dislocation gout alcoholism chronic renal disease divers and workers who use compressed air long-term steroid therapy more common in men |
Orthopedics p204
|
|
|
What is the clinical presentation of aseptic necrosis of the hip?
|
gradual
pain slight limp progressively restricted ROM |
Orthopedics p204
|
|
|
What is the diagnostic workup of aseptic necrosis of the hip?
|
hip radiograph → increase in density in superior portion of femur
|
Orthopedics p204
|
|
|
What is the managment of aseptic necrosis of the hip?
|
1. goal → prevent collapse of femoral head and encourage repair of necrotic area
2. prolonged use of crutches 3. if collapsed → prosthetic replacement |
Orthopedics p204
|
|
|
What is aseptic necrosis of the hip?
|
infarction in the anteriosuperior weight-bearing portion of the femoral head →
bone necrosis → collapse → secondary degenerative arthritis |
Orthopedics p204
|
|
|
What is the etiology of hip dislocation?
|
posterior dislocation → blow to knee while hip and knee flexed
anterior dislocation → blow to knee while hip abducted |
Orthopedics p206
|
|
|
What is the clinical presentation of hip dislocation?
|
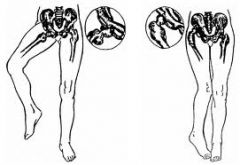
posterior dislocation → hip flexed and internally rotated
anterior dislocation → hip in external rotation |
Orthopedics p207
|
|
|
What are the complications of hip dislocation?
|
associated knee or acetabular fracture
AVN |
Orthopedics p206
|
|
|
Which is more common, anterior or posterior hip dislocation?
|
posterior
|
Orthopedics p206
|
|
|
What is the management of hip dislocation?
|
EMERGENCY!!!
1. reduce immediately to prevent AVN 2. prohibit weight-bearing |
Orthopedics p207
|
|
|
What is the diagnostic workup of hip dislocation?
|

AP and lateral hip radiograph
*posterior hip dislocation pictured above |
|
|
|
What is a giant cell tumor?
|
benign vascular lesion in bone but may transform into malignancy
|
Orthopedics p386
|
|
|
What is the etiology of giant cell tumor?
|
spontaneous
associated with hyperparathyroidism rare usually occurs between 20-40y/o rare in children and elderly |
|
|
|
What is the clinical presentation of a giant cell tumor?
|
bone pain usually affecting distal metaphysis and epiphysis of femur
possible pathologic fracture |
|
|
|
What is the diagnostic workup of a giant cell tumor?
|
AP and lateral radiographs of femur → "soap bubble" appearance
|
Orthopedics p386
|
|
|
What is the management of a giant cell tumor?
|
surgical removal
|
|
|
|
List types of bone tumors and their characteristic radiographic appearance.
|
osteosarcoma → sunburst appearance
ewing's sarcoma → onion skin appearance giant cell tumor → soap bubble appearance |
|
|
|
Benign and malignant lesions typically develop in which part of a long bone?
|
metaphysis
|
|
|
|
What percent of 2° bone tumors affect the spine?
|
40%
*spine = most common site for bone metastasis |
Orthopedics p356
|
|
|
What is an enchondroma?
|
benign bone tumor originating from cartilage (i.e. cartilage cyst)
|
Orthopedics p446
|
|
|
What is the clinical presentation of enchondroma?
|
usually occurs between 10-50 y/o
nonspecific symptoms no pain usually in small bones of hands and feet discovered incidentally or following pathologic fracture enlarged fingers deformities |
Orthopedics p446
|
|
|
Where do enchondromas most commonly occur?
|
small bones of hands and feet
|
Orthopedics p446
|
|
|
What is the diagnostic workup of enchondroma?
|
radiograph
usually located centrally in bone |
|
|
|
What is the management of enchondroma?
|
1. observation → periodic radiographs
2. if diagnosis uncertain → surgery to R/O chondrosarcoma 3. if recurrent fracture → surgery |
Orthopedics p446
|
|
|
How do you distinguish between enchondroma and chondrosarcoma?
|
enchondroma → painless
chondrosarcoma → painful, bone erosion |
|
|

|
enchondroma (of 5th metacarpal)
L: radiograph R: MRI |
|
|
|
What is an osteochondroma?
|
classified as benign bone tumor but thought to be a developmental abnormility where part of physis forms outgrowth on bone surface
|
Orthopedics p446
|
|
|
What is the clinical presentation of osteochondroma?
|
painless mass
usually occurs at distal metaphysis of femur or proximal metaphysis of tibia growth ceases with skeletal maturity |
Orthopedics p446
|
|
|
What is the management of osteochondroma?
|
1. observation → periodic radiographs → often regresses once reach skeletal maturity
2. if symptoms (pain, blood vessel or nerve compromise, large cartilage cap) → surgical removal once reach skeletal maturity |
Orthopedics p446
|
|
|
What is the diagnostic workup of osteochondroma?
|
radiograph →
sessile or pedunculated lesion continuous with cortex and marrow cavity small cartilage cap |
|
|

|
pedunculated osteochondroma of distal femur + associated fracture
|
|
|
|
What is chondrosarcoma?
|
malignant cartilage tumor
primary or secondary from enchondroma |
Orthopedics p448
|
|
|
What is the clinical presentation of chondrosarcoma?
|
occurs >40 y/o
shoulder girdle, pelvis, proximal femur painful swelling |
Orthopedics p448
|
|
|
What bone tumor presents at the diaphysis?
|
Ewing's sarcoma
|
Orthopedics p448
|
|
|
What is the diagnostic workup of chondrosarcoma?
|
radiograph → speckled calcifications in destructive radiolucent lesion
|
Orthopedics p449
|
|

|
bone destruction + sunburst pattern → osteosarcoma (of proximal fibula)
|
|
|

|
chondrosarcoma of inferior ramus of pubis
|
|
|

|
Ewing's sarcoma (of femur)
|
|
|
|
What is the management for chondrosarcoma?
|
1. refer to orthopedic specialist
2. surgical resection 3. NOT sensitive to chemotherapy or radiation |
Orthopedics p449
|
|
|
What is the most common tumor of the hand?
|
enchondroma
|
|
|
|
What is multiple myeloma?
|
neoplastic proliferation of plasma cells of bone marrow
|
Orthopedics p168
|
|
|
What is the difference between raynaud's disease and raynaud's phenomenon?
|
raynaud's disease = primary
raynaud's phenomenon = secondary |
Current p756
|
|
|
What is the etiology of raynaud's disease/phenomenon?
|
paroxysmal digital ischemia caused by exaggerated response to cold or emotional stress
may be primary or secondary primary usually affects young women 15-30y/o |
Current p756
|
|
|
What is the clinical presentation of raynaud's disease/phenomeon?
|
paroxysmal well-demarcated digital pallor or cyanosis followed by rubor
precipiated by cold or emotional stress relieved spontaneously or by warm room or warm water |
Current p756
|
|
|
What is the ddx for raynaud's?
|
primary
secondary: scleroderma SLE mixed connective tissue disease |
Current p757
|
|
|
What is the diagnostic workup?
|
if primary → none
if secondary → dependent on suspected cause |
|
|
|
What is the management of raynaud's?
|
keep body warm
protect hands from injury → since wound heal slowly and are difficult to control apply lotion to hands frequently stop smoking if severe symptoms or tissue injury → calcium channel blockers, sympathectomy |
Current p757
|
|
|
What are the differences between primary and secondary raynaud's?
|
primary → symmetric, benign
secondary → may lead to digital pitting, ulceration, and gangrene |
Current p756
|
|

|
raynaud's disease/phenomenon
|
|
|
|
What is polyarteritis nodosa?
|
necrotizing arteritis of medium-sized arteries
|
Current p765
|
|
|
What is the etiology of polyarteritis nodosa?
|
unknown
10% associated with hepB where presentation occurs within 6 months of hepB infection |
Current p765
|
|
|
What is commonly associated with polyarteritis nodosa?
|
hepB
|
Current p765
|
|
|
What is the clinical presentation of polyarteritis nodosa?
|
dependent on vessels affected
insidious onset fatigue, fever, weight loss livedo reticularis abdominal pain arthralgia, myalgia, neuropathy mononeuritis multiplex → manifests as foot drop |
Current p765
|
|
|
What is the diagnostic workup of polyarteritis nodosa?
|
anemia
leukocytosis elevated ESR and CRP negative ANCA hepB angiogram or tissue biopsy |
Current p765
|
|
|
What is the management of polyarteritis nodosa?
|
high dose corticosteroids
if severe → immunosuppressants if hepB → corticosteroids + antiviral therapy + plasmapheresis |
Current p765
|
|
|
What is giant cell arteritis?
|
systemic arteritis affecting medium and large-sized vessels
|
|
|
|
What is the clinical presentation of giant cell arteritis?
|
HA, visual changes, jaw claudication, throat pain polymyalgia rheumatica (50%)
|
Current p767
|
|
|
What is the clinical presentation of polymyalgia rheumatica?
|
pain and stiffness of shoulders and hips without other explanation
|
Current p767
|
|
|
What are the major differences between polymyalgia rheumatica and giant cell arteritis?
|
polymyalgia rheumatica:
does not cause blindness responds to low dose corticosteroids giant cell arteritis: can cause blindness requires high dose corticosteroids |
Current p767
|
|
|
What is the diagnostic workup of giant cell arteritis?
|
elevated ESR and CRP
|
Current p767
|
|
|
What is the management of giant cell arteritis?
|
1. immediate high-dose prednisone
2. temporal artery biopsy |
Current p767
|
|
|
What is the management of polymyalgia rheumatica?
|
low-dose prednisone
|
Current p767
|
|
|
What is Behcet's syndrome?
|
vasculitis involving small, medium, and larger arteries and veins
|
Current p772
|
|
|
What is the etiology of Behcet's syndrome?
|
unknown
tends to effect people with Asian, Turkish, Middle Eastern descent |
Current p772
|
|
|
What is the clinical presentation of Behcet's syndrome?
|

recurrent aphthous ulcers of mouth (>3/year)
aphtous ulcers of genitals erythema nodosum-like rash folliculitis uveitis -if anterior → photophobia, red eye, hypopyon -if posterior → symptoms manifest late nonerosive arthritis of knees and ankles neurologic lesions that mimic MS |
Current p772
|
|
|
What is the diagnostic workup of Behcet's syndrome?
|
elevated ESR and CRP
pathery test → prick skin; positive if sterile pustule formation within 24-48 hours |
Current p772
|
|
|
What is the management of Behcet's syndrome?
|
corticosteroids → prednisone
|
Current p772
|
|
|
What is pathery and what disease is it associated with?
|

formation of sterile pustule at site of needle stick associated with Behcet's syndrome
|
Current p773
|
|
|
What is the workup of fibromyalgia?
|
9x more common in women than men
between 3-50y/o multiple trigger points chronic (>3 months) diffuse pain vague aching joints, especially spine, shoulder, hips vague symptoms → fatigue, HA, stiffness, abdominal symptoms, sleep disorders depression radiographs normal R/O other more likely causes of pain |
Orthopedics p301
|
|
|
What is the diagnostic criteria for fibromyalgia?
|
1. history of chronic widespread pain
2. >3 months in duration 3. pain in 11 of 18 characteristic trigger points 4. all 4 body quadrants affected |
Orthopedics p302
|
|
|
What is the management of fibromyalgia?
|
1. treat empirically and symptomatically
2. all treatments have uncertain success rates 3. NSAIDs, muscle relaxants, trigger point injections, antidepressants, aerobic fitness programs, physical therapy, acupuncture, transcutaneous nerve stimulation 4. address social and environmental factors 5. recommend self-education and management, support groups 7. prognosis uncertain → symptoms may come and go for years despite tx approach |
Orthopedics p302
|
|
|
What percent of the general population is affected by fibromylagia?
|
2-3%
|
Orthopedics p301
|
|
|
What is another name for reflex sympathetic dystrophy (RSD)?
|
complex regional pain syndrome
|
Orthopedics p441
|
|
|
What is the workup of reflex sympathetic dystrophy?
|
unknown cause
relatively minor injury → sympathetic nervous sytem disturbance → symptoms pain → burning, throbbing, shooting hyperalgesia, allodynia, hyperpathia stiffness, edema atrophy of skin, hair, and nails autonomic dysfunction → anhidrosis or hyperhydrosis, heat and cold insensitivity affects extremities |
Orthopedics p441
RSD lecture |
|
|
Define hyperalgesia.
|
increased sensitivity to pain
|
|
|
|
Define allodynia.
|
pain from a stimulus that normally does not cause pain
|
|
|
|
Define hyperpathia.
|
abnormally painful reaction to a stimulus
|
|
|
|
What is the management of regional sympathetic dystrophy?
|
1. prevention → immediate attention to injury, control of pain and swelling (elevation of extremity), active use of extremity despite pain, no smoking
2. early → corticosteroids, pain meds, mobilization 3. intermediate → sympathetic block, calcitonin, pain meds, mobilization 4. late → pain meds, physical therapy |
Orthopedics p441
RSD lecture |
|
|
What is osteomyelitis?
|
infection of the bone
|
|
|
|
What is the etiology of osteomyelitis?
|
bone infection caused by either:
1. adjacent infection 2. dissemination in blood → elderly, sickle cell, IV drug abuse 3. skin breakdown due to vascular insufficiency if sickle cell → think salmonella if IV drug abuse → think s. aureus if adjacent joint → think s. aureus or staph epidermidis |
Current p780
|
|
|
What is the diagnostic workup of osteomyelitis?
|
ESR → extremely high (>100mm/h)
bone biopsy culture from bone biopsy radiographs: if early → soft tissue swelling, periarticular demineralization if >2 weeks → bone erosion |
Current p780
|
|
|
What is the clinical presentation of osteomyelitis?
|
fever, chills, bone pain and tenderness
if adjacent infection → inflammation, lower fever if skin breakdown → ulcer, absent fever |
Current p780
|
|
|
What is the management of osteomyelitis?
|
1. debridement of necrotic bone
2. prolonged antibiotics x 6-8 weeks |
Current p780
|
|
|
What are the indications for aspirin?
|
analgesic
antipyretic anti-inflammatory anti-platelet → prevention of MI, TIA, CVA; current MI; post-MI; revascularization procedures |
Pharmacology p504
|
|
|
What is the mechanism of action of aspirin?
|
IRREVERSIBLY inhibits COX-1 → preventing thromboxane A2 production
COX-1 normally converts arachidonic acid to prostaglandin H2 → prostaglandin is converted to thromboxane A2 |
Pharmacology p233, 502
|
|
|
What are the adverse effects of aspirin?
|
prolonged bleeding time
GI problems → distress, ulcer, hemorrhage, iron-deficiency anemia sodium and water retention → edema, hyperkalemia hemorrhagic stroke |
Pharmacology p233, 502
|
|
|
Why may aspirin cause GI bleeding?
|
↑ gastric acid secretion
↓ mucus production |
Pharmacology p502
|
|
|
If an NSAID causes GI bleeding, and continued NSAID treatment is necessary, what should you prescribe?
|
proton pump inhibitor (PPI) or misoprostol
|
Pharmacology p502
|
|
|
Toxic doses of aspirin cause?
|
respiratory depression
|
|
|
|
What are the symptoms of aspirin toxicity?
|
HA, dizziness, nausea, vomiting, mental confusion, tinnitus, hyperventilation → restlessness, delirium, hallucinations, convulsions, coma, respiratory and metabolic acidosis, death from respiratory failure
|
Pharmacology p505
|
|
|
What are the contraindications for aspirin?
|
<15y/o
pregnancy and breast-feeding surgery within 1 week probenecid, sulfinpyrazone increase uric acid secretion (whereas aspirin decreases uric acid secretion) |
Pharmacology p505, 506
|
|
|
Why must aspirin be avoided in adolescents <15y/o?
|
aspirin + viral infection = potential Reye's syndrome
|
Pharmacology p504
|
|
|
What is the patient education for aspirin?
|
1. take with fluids and food to decrease dyspepsia
2. do not take concurrently with other salicylates 3. do not take 1 week prior to surgery 4. do not take with probenecid or sulfinpyrazone 5. may need to lower warfarin, phenytoin, or valproic acid etc. since aspirin causes higher plasma concentrations of those drugs |
Pharmacology p233, 506
|
|
|
What is the dosing for aspirin?
|
prevention of MI → 81-162 mg/d
prevention of stroke → 50-325 mg/d acute MI → 162-325mg OA or RA → 3g/d |
Pharmacology p505
|
|
|
What type and dose of aspirin should be given for acute MI?
|
162-325mg of nonenteric coated aspirin chewed and swallowed immediately
|
Pharmacology p505
|
|
|
What are the indications for ibuprofen?
|
analgesic
antipyretic anti-inflammatory anti-platelet |
Pharmacology p507
|
|
|
What is the mechanism of action for ibuprofen?
|
REVERSIBLY inhibits COX-1 → preventing synthesis of prostaglandins (but not leukotrienes)
|
Pharmacology p507
|
|
|
What are the adverse effects of ibuprofen?
|
GI → dyspepsia, bleeding
CNS → HA, dizziness, tinnitus |
Pharmacology p507
|
|
|
What is the mechanism of action for indomethacin?
|
REVERSIBLY inhibits COX-1
|
Pharmacology p507
|
|
|
What are the indications for indomethacin?
|
OA of hip
ankylosing spondylitis acute gout *analgesic, antipyretic, and anti-inflammatory effects but use limited to above conditions due to toxicity |
Pharmacology p507
|
|
|
What are the indications for meloxicam?
|
OA
RA ankylosing spondylitis |
Pharmacology p507
|
|
|
What are the indications for ketorolac?
|
potent analgesic → short-term relief of moderate to severe pain up to 5 days after first dose administered via IV or IM
*only moderate anti-inflammatory |
Pharmacology p508
|
|
|
What are the contraindications for ketorolac?
|
pediatrics
|
Pharmacology p508
|
|
|
What are the adverse effects of ketorolac?
|
GI bleeding
stomach or intestinal perforation fatal peptic ulcer |
Pharmacology p508
|
|
|
What is the patient education for ketorolac?
|
if mild or chronic pain → do not exceed 40mg/d
|
Pharmacology p508
|
|
|
What is the mechanism of action for celecoxib?
|
reversible inhibition of COX-1 but mostly COX-2
|
Pharmacology p508
|
|
|
What are the indications for celecoxib?
|
pain
OA RA *no anti-platelet function |
Pharmacology p508
|
|
|
What are the adverse effects of celecoxib?
|
HA, dyspepsia, abdominal pain, diarrhea
*less GI bleeding than aspirin |
Pharmacology p508
|
|
|
What are the contraindications for celecoxib?
|
sulfonamide allergy
severe heart disease severe hepatic disease severe renal disease may increase levels of some B-blockers, antidepressants, antipsychotics |
Pharmacology p509
|
|
|
What is the generic name for Motrin?
|
ibuprofen
|
|
|
|
What is the generic name for Vicodin?
|
hydrocodone
|
|
|
|
What is the generic name for Valium?
|
diazepam
|
|
|
|
What is the generic name for Percocet?
|
oxycodone
|
|
|
|
What is the generic name for Demerol?
|
meperidine
|
|
|
|
What are the indications for acetominophen?
|
analgesic → pain, OA
antipyretic *no anti-inflammatory effects |
|
|
|
What are the adverse effects of opioids?
|
sedation
respiratory depression constipation tolerance withdrawal addiction |
|
|
|
What are the contraindications for morphine?
|
respiratory depression
renal failure |
|
|
|
What is the MOA of colchicine?
|
1. bind and depolymerizes tubulin, a protein involved in mobilization of neutrophils → decreasing their accumulation in gout affected sites
2. blocks cell division by binding to myotic spindles 3. inhibits leukotriene synthesis |
|
|
|
What are the indications for colchichine?
|
pain relief in acute gout
prevention of acute gout attacks |
Pharmacology p516
|
|
|
What are the contraindications for colchicine?
|
pregnancy
|
|
|
|
What are the adverse effects of colchicine?
|
nausea, vomiting, diarrhea, abdominal pain
|
|
|
|
List ucosuric medications.
|
probenecid
sulfapyrazone |
|
|
|
What is the MOA of ucosurics (probenecid and sulfapyrazone)?
|
inhibits urate-anion exchanger in proximal tubule → inhibiting resorption → increasing renal clearance of uric acid
|
|
|
|
What are the indications for probenecid or sulfapyrazone?
|
prevention of gout where uric acid is undersecreted
|
|
|
|
What are the contraindications for probenecid or sulfapyrazone?
|
renal insufficiency
kidney stones high dose aspirin therapy |
|
|
|
List xanthine oxidase inhibitors.
|
allopurinol
|
|
|
|
What is the MOA of allopurinol?
|
inhibits xanthine oxidase which normally catalyzes uric acid synthesis
|
|
|
|
What are the indications for allopurinol?
|
prevention of chronic gout if:
1. overproducer of uric acid 2. undersecreter of uric acid + renal insufficiency |
|
|
|
List natural, semi-synthetic, and synthetic opiods.
|
natural → morphine, codeine
semi-synthetic → hydromorphone, hydrocodone, oxycodone synthetic → tramadol, methadone, meperidine |
|
|
|
List the indications for opioid analgesics.
|
mild to moderate pain → tylenol with codeine,
moderate to severe pain → morphine, hydromorphone, hydrocodone, oxycodone, meperidine, tramadol opioid detox → methadone |
|
|
|
What are the most common adverse effects of opioids?
|
constipation, sedation, respiratory depression
|
|
|
|
Urinary retention is a common side effect of meperidine (demerol), true or false?
|
true
|
|