Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
Clues to a defect in primary hemostasis
|
Immediate bleeding
Mucosal bleeding Menorrhagia Epistaxis Easy bruising |
|
|
Clues to a defect in secondary hemostasis
|
Delayed bleeding
Bleeding into joints and soft tissue |
|
|
Bernard-Soulier Syndrome
|
AR
Giant platelets Defect in GLYCOPROTEIN 1b/9 (plt receptor for vWF) does NOT aggregate in response to ristocetin |
|
|
How to distinguish BS from vWD?
|
Both will NOT aggregate in response to ristocetin
BUT with the addition of normal plasma, vWD will aggregate. BS won't. |
|
|
What other diseases are associated with GP1b/9?
|
ITP!
60% of cases of ITP have an autoantibody, usually to GP1b/9 or GP2b/3a Velocardiofacial syndrome: microdeletion 22q11 |
|
|
What is the treatment for ITP?
|
NOT PLATELETS
Steroids are first line |
|
|
Glanzmann's thrombasthenia
|
AR or autoimmune
Defect in glycoprotein 2b/3a Causes problems with platelet aggregation Will NOT show aggregation by ADP, epinephrine, collagen, TXA2 or thrombin. WILL aggregate with ristocetin (through vWF) |
|
|
What does glycoprotein 2b/3a do?
|
it is an integrin on the platelet surface that acts as a receptor for fibrinogen. 2b & 3a come together in the presence of calcium
|
|
|
Platelet receptors
|

|
|
|
Coagulation cascade
|

|
|
What conditions will you have this abnormality in platelet aggregation studies?
|
Bernard-Soulier
vWD = Abnormal aggregration in response to ristocetin. (Ristocetin causes vWF to bind to gp1b receptor) |
|
|
What is ristocetin?
|
Was used as an antibiotic, but caused clotting. Now only used in vitro. Enhances binding of vWF to platelet receptor gp1b, in an unknown fashion.
|
|

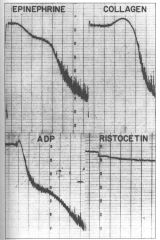
What is shown in this platelet aggregation study?
|
NORMAL platelet aggregation :-)
ADP and epinephrine exhibit two waves of aggregation, primary and secondary . The secondary wave is due to release of endogenous ADP. |
|
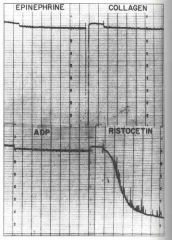
Disease?
|
Glanzmann's thrombasthenia
|
|
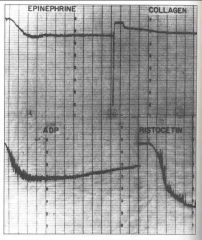
Disease?
|
Storage pool disease or defective release of storage pool contents (aspirin-like defect)
**Secondary waves to ADP and epinephrine absent |
|
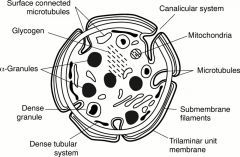
What are in the granules of platelets?
|
Dense granules: ADP, Ca, Serotonin
Alpha granules:growth factors, Platelet factor 4, fibronectin, Beta Thromboglobulin, von Willebrand Factor, Fibrinogen and Coagulation factors V and XIII Lambda granules: similar to lysosomes and contain several hydrolytic enzymes. |
|

pattern?
|
Abnormal response to ADP, epi, collagen.These are all dependent on binding to the ADP receptor (specifically P2Y12).
This pattern of abnormalities suggest either an abnormality of the P2Y12 receptor [rare] or a drug effect such as Clopidogrel [common.] If bleeding, give platelets. |
|

These aggregation traces were obtained from a 33-year-old woman referred for investigation of life-long menorrhagia and prolonged bleeding after dental surgery. There was a family history suggestive of a bleeding disorder but no conclusion had ever been reached.
|
The obvious abnormalities in these series of aggregation traces are the lack of second wave aggregation with ADP and adrenaline [remember these are weak agonists] but in addition the aggregation with collagen and ristocetin is abnormal [reduced.]
This suggests either platelet storage pool disorder or an abnormality of platelet granule release. |
|

These aggregation traces were obtained from an 18-year-old student under investigation for easy bruising. She had a prolonged closure time of >300s with PFA100
|
The obvious abnormalities are an absent response to arachidonic acid and reduced secondary wave aggregation with ADP and Adrenaline. Collagen is also reduced.
These findings suggest a defect in the Thromboxane A2 pathway. Possibilities include drugs such as aspirin, NSAIDs, food stuffs that contain salicylates or a true defect in the TxA2 pathway. |
|
|
Clinical clues to dx of vWD
|
Easy bruising
Nose bleeds Menorrhagia Jt bleeding uncommon; possibly type 3 |
|
|
Lab test abnormalities in vWD
|
Low F8
PT: normal PTT: prolonged Plt agg: abnormal response to ristocetin; normal responses to others. PFA: abnormal collagen/adrenaline closure time and in most cases (but not all) a normal collagen/ADP time. |
|
|
Type 1 vWD
|
Most common; mildest; may be asx
HETEROZYGOUS (homoz is type3) Quantitative defect |
|
|
Type 2 vWD
|
20%
AD Qualitative defect Normal levels but structurally abnormal FOUR SUBTYPES: A B M N |
|
|
Type 2A vWD
|
Decreased ability to bind GP1 receptor
Decreased plt adhesion & aggregation Low ristocetin cofactor activity Cannot form large multimers |
|
|
Type 2B vWD
|
GAIN OF FUNCTION
Enhanced binding to GP1 = spontaneous binding to platelets --> rapid clearance of plts & lrg multimers So may have thrombocytopenia & lack large multimers *** Pt plt-poor plasma + formalin donor plts: low ristocetin activity Pt plt-rich plasma: Abnormally LOW levels of ristocetin cause aggregation. Because large multimers are bound to platelets. CANNOT use desmopressin as a treatment for bleeding as can lead to clots & low plts |
|
|
Type 2M vWD
|
Decreased ability to bind GP1 (thus low activity with ristocetin) but has NORMAL large multimers
|
|
|
Type 2N vWD
Normandy |
Abnormal binding to F8
Normal vWF levels Normal ristocetin activity DECREASED F8 to levels seen in hemophilia A |
|
|
Type 3 vWD
|
Most severe (HOMOZYGOUS)
NO vWF production Extremely low F8 levels, to those seen in hemophilia A (Hemophilia A is XR, Type3vWD is AR) |
|
|
Platelet-type vWD
Pseudo-vWD |
AD defect in platelet
GP1 receptor on plt membrane increased affinity for vWF plt aggs + lrg multimers removed from circulation causing thrombocytopenia and low multimer levels SIMILAR FINDINGS TO TYPE 2B |
|
|
Acquired vWD
|
Autoantibodies
A form of vWD occurs in patients with aortic valve stenosis, leading to gastrointestinal bleeding (Heyde's syndrome). Acquired vWD has also been described in the following disorders: Wilms' tumour, hypothyroidism |
|
|
Which ABO blood group has normally LOW levels of vWD and may be misdiagnosed with Type 1 vWD?
|
O
|
|
|
When is desmopressin useful in treating vWD?
|
Type 1, Type 2A
Desmopressin (DDAVP) stimulates release of von Willebrand factor from the Weibel Palade bodies of endothelial cells and increases the levels of vWF as well as coagulant Factor VIII. CONTRAINDICATED in Type 2B; ineffective in others |
|
|
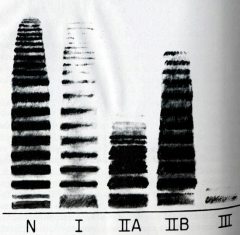
describe pattern of vWF multimers in type 1, 2a, 2b, 3
|
|
|
|
What 2 vWD have an increased RIPA test?
|
2B (gain of fxn gp1b/9)(decreased large forms)
Plt type (gain of fxn gp1b/9 for vWF)(decreased large forms)(Mimics 2B but needs higher ristocetin level, and also aggregates with cryo) |
|
|
What vWD type mimics hemophilia A? Why? How to tell apart?
|
vWD 3. most severe form of vWD. No vWd and therefore looks like no F8 either.
But type 3 vWD is AR vs. XR in hemophilia. So they could give you a picture that looks like hemophilia, but in a female. |
|
|
genetic defect hemophilia A?
|
xq28 inversion intron 22
|
|
|
What is it in EDTA that causes platelet clumping and pseudothrombocytopenia?
|
antibodies to gp2b/3a! (what usu binds to fibrinogen)
|
|
|
how can you tell DIC from TTP/HUS based on labs?
|
DIC has low fibrinogen
|
|
|
mutation in factor V leiden?
|
Arg --> Gln @ 506
|
|
|
mutation facrot V cambridge?
|
Arg --> thr @ 306
|
|
|
Mutation sickle cell dz?
|
Glu --> Val on 11 (Beta chain gene)
|
|
|
test results for antiphospholipid syndrome
|
elevated PTT
|
|
|
2 diseases with low platelets AND thrombosis
|
APLS
HIT |
|
|
treatment of HIT
|
Stop heparin
DO NOT give platelets DO NOT give warfarin DO give thrombin inhibitors, and monitor with PTT |