Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back

What is vernix caseosa?
When is epidermal maturation complete in the newborn? |
Vernix caseosa= layer covering newborn. desquamated cells, lanugo hairs, antimicrobials, sebaceous gland secretions. Sheds in a few days.
Maturation is completed by ~34 weeks |
|
|
Why should caution be exercised in using any topical substances in neonates?
|
1. ↑ surface area: body weight ratio
2.potentially increased permeability and abnormal barrier (esp. in those born with blistering disorders or erythroderma) |
|

What is the yellow color due to? What accounts for this appearance of the skin (note- this neonate is 6 hours old)?
|
Meconium
Normal skin looks wrinkled because baby was in warm, wet environment. |
|

What is this called? Where is the pigment located?
How can it be differentiated from bruising? What happens to the pigment? |
Mongolian spot aka. Dermal Melanosis.
Different from bruising- doesn't go through color changes of bruising. Regresses throughout life. |
|

What is this called? Does it fade over time?
|
Angel's kiss or "Nevus simplex" capillary stain
Around 50% persist throughout life. Can fade and return when baby becomes emotional/cries. Not bruises (eyelid bruising is rare in babies!) |
|

What is this called? How does it form?
|
Stork bite
It's a "Nevus Simplex" capillary stain (from dilated capillaries) |
|
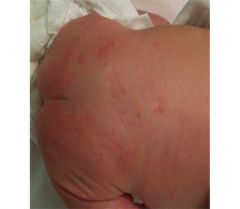
What is this common rash? When does it develop?
|
Erythema Toxicum (looks like flea bites or pustules)
Baby is a newborn (develops after birth). Benign. |
|

What is this called and in what demographic is it commonly seen? When does it develop?
|

Transient neonatal pustular melanosis
Develops in african american children IN UTERO. Sometimes see colarette of scale (from desquamation around lesion). |
|

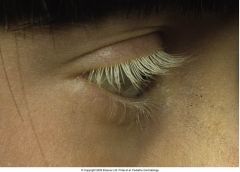
What is on the shoulder of this baby?
|
Lanugo hairs (common in babies, shed with the vernix caseosa) but can be seen in adults in certain malignant conditions.
|
|

What is this? What demographic is it typically seen in?
|

Hyperpigmentation
Typically seen in Indian, Asian, pigmented races. It will distribute over first couple of months of life. Babies are lighter at birth than later in life. |
|

What is the small lesion on the baby's right cheek?
|
Milia (mini epidermal inclusion cyst filled with keratin). It will desquamate/shed over time.
|
|

What is this condition (seen on nose)? What can it result from?
|
Sebaceous hyperplasia
Can result from maternal hormone stimulation. |
|

What is this condition? How can you make it go away?
|
Physiologic Cutis Marmorata (marbling of skin)
When child is cold, vasoconstriction results in this pattern. Will disappear by warming up child (place into isolette). |
|
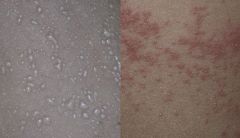
Name the normal neonatal lesions? In what climate does this condition show?
|
Miliaria crystallina (fragile, superficial)
Miliaria rubra (prickly appearance) Both transient and occurs when child is in warm environment. |
|

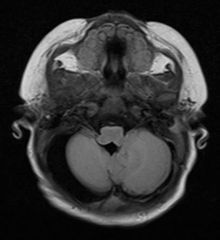
What is this? What is the word for failure to close?
|
Nasal encephalocele (pocket of brain tissue through an area of DYSRAPHISM).
|
|

What is the condition on the top left called? What about the bottom right? If you see a baby with either of these, what do you want to do?
|
Top left= midline hemangioma, Bottom right= "fawn tail" or hypertrichosis over midline. Both suggestive of occult spina bifida.
**work up the child because they can develop bladder spasticity early on. |
|

What is this lesion called? Why do we worry about it so much?
|
Dermoid cyst (contains hair, sebum, keratin, glands).
Dangerous because some can contain ostium that has a sinus tract with extension to CNS. Easy access for bacteria --> recurrent meningitis. |
|

What condition might this child be recurrently afflicted by? What do you have to do to treat this?
|
Recurrent meningitis (this is a dermal sinus that tracks to the meninges, and if bacteria enters it can cause infection).
Needs to be removed by neurosurgeon. |
|

What is this lesion called? If it occurs at the vertex/midline what can it be associated with?
|
Aplasia cutis congenita. (congenital absence of skin)
May not be associated with anomalies but if in midline, could be associated with underlying NEURAL TUBE DEFECT. Make sure to image! |
|

What would you be worried about in this child who also has a port wine stain?
|
This combination (hair collar + port wine) suggests an atreitic encephalocele. In general, you want to image these patients for possible underlying malformations.
Hair collar= ring of dark, coarse hair. |
|
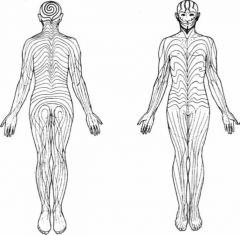
What is the name of the patterns shown here? Disorders that follow this pattern suggest what?
|

Lines of Blaschko (lines of skin embryogenesis)
Disease following the lines represent genomic/epigenomic MOSAICISM. ex: linear epidermal nevus |
|

What is this called?
|
Nevus sebaceous (organoid hamartoma). Overgrowth of sebaceous glands in the area of a nevus.
|
|

What is this lesion called? What does it tell you about the origin of the condition?
|
Hypomelanosis of Ito or mosaic hypopigmentation
Occurs in swirling pattern that tells you it's a Genetic Mosaicism. |
|

What is this spot?
|
An accessory nipple (occurs in the milk line). Might get mistaken for a nevus.
|
|
|
What does an epidermal melanin unit consist of?
|
Melanocyte + up to 30 keratinocytes (melanosomes which contain melanin pigment are discharged into keratinocyte)
|
|
|
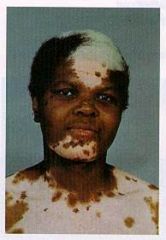
What is this condition called? Where on the body does it tend to present? When in life is it evident?
What other conditions might this person have? |
Vitiligo- presents on extensor surfaces mainly
Acquired disorder- presents later in life (one key difference from Piebaldism). Absence of melanocytes. Likely related to autoimmune mechanism so other autoimmune disorders may run in the family. |
|
What is this called? What is the treatment for vitiligo?
|

Poliosis (vitiligo involvement in hair)
Treatment = 1) corticosteroids- effects autoimmune mxn. 2) Repigmentation (via phototherapy)- because some pigment is preserved in these individuals. |
|

What might this person be affected with? How can you tell the difference between this and Vitiligo?
|
Post Inflammatory Hypopigmentation (pityriasis alba). Possibly the person has tinea versicolor infection.
Melanocytes are intact but defective transfer of melanosome to keratinocyte. Under Wood's lamp, vitiligo looks chalk white. |
|
This individual has what mutation/inheritance pattern? What is the difference between this and Vitiligo?
|
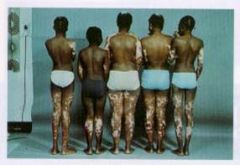
Mutation in cKIT proto-oncogene (Autosomal dominant).
This is congenital mutation (born with it). White forelock. Problem with production of pigment (melanocytes exist but pigment doesn't). |
|
|
How is melanin synthesized? What is the crucial enzyme in the synthesis of melanin?
|
L-phenylalanine is turned into L-dopa which eventually becomes Eumelanin (black pigment) or Pheomelanin (red pigment)
Tyrosinase= crucial enzyme(L-tyr to L-dopa, and L-dopa to dopaquinone) |
|
What is this condition called? What mutation does this individual have? What is their melanocyte count?
|

Oculocutaneous Albinism
OCA-1= tyrosinase negative, AR. Normal NUMBER of melanocyte. Note: translucent iris, burn easily. Nystagmus (vision problem). |
|

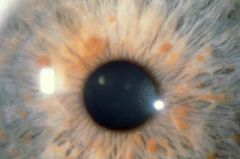
This is the fundus exam of a person with what condition? How can you tell? What would the person look like if you transiluminated their eye?
|

Oculocutaneous Albinism
You can make out choroidal circulation because they have a lack of pigment (it stands out). Red Iris Reflex is seen upon transilumination of eye. |
|
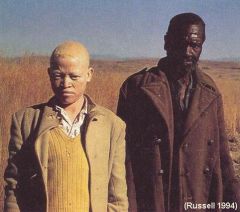
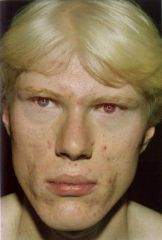
What condition does this individual have and how can you tell? What mutation does he have?
|
OCA-2 (they have more yellow/reddish hair).
Mutation in P-protein (which is responsible for transport of melanin). Often hunted and killed in Tanzania because believed to have magical body parts. |
|

What is this? Is it congenital?
What is the most significant predisposing factor for this type of lesion? |
Early hemangioma (looks flat, like a bruise). NOT congenital (though it can present early in life).
Predisposing factor= Low Birth Weight |
|

What is the typical course of this lesion? Should it be monitored or is it benign?
|
The lesion itself is benign and will regress over time. However this one is periocular and can compress eye causing amblyopia so should be monitored.
|
|

What is this? Is it problematic?
|
Hemangioma that is midline. Associated with occult spinal dysraphism (should get imaged).
|
|

What is this? Is it problematic?
|
Perineal/segmental hemangioma that can cause PELVIS syndrome (associated with painful ulcerations).
|
|

What is this? What might this child have in addition to this lesion?
|
PHACES syndrome- Posterior fossa abnormality, Hemangioma, Arterial abnormality, Coarctation of aorta, Eye anomalies, Sternal abnormalities
Upper segmental lesion associated with posterior fossa anomalies and arterial anomaly (she was missing R internal carotid). |
|
|
How do you treat hemangiomas?
|
No treatment (typically spontaneously involute).
If there is a high risk hemangioma (airway compromise, affects eye, etc.) you can treat with Propranolol or Systemic steroids (too thick for laser). Or surgery. |
|

This lesion is often confused with a hemangioma. What is it?
|
Pyogenic granuloma (often seen in sites of trauma or warts, friable and bleeds easily).
|
|

What is this called? If it was in the distribution of V1 (first branch of the trigeminal) what would it be called?
|
Port-Wine Stain- i.e. capillary malformation (if in V1 distribution, it would be Sturge Weber Syndrome).
|
|

What is this syndrome associated with (note- it is in the V1 distribution of the trigeminal nerve)? How does this lesion differ from a hemangioma?
|
Seizures and glaucoma (child has a glass eye). Differs from hemangioma because this is present AT BIRTH!
|
|
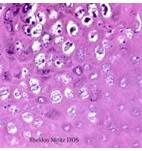
What is the causative agent seen in this pathology? What type of infectious agent is it and how is it transmitted?
|
Molluscusm Contagiosum (DNA poxvirus)
Spreads by fomite, autoinoculation (lives despite chlorine!) Virus (note inclusion bodies) |
|

What is the causative agent? Treatment?
|
Molluscum contagiosum (note umbillicated vesicles)
Treat with Cantharidin (extracted from beetles). Otherwise, you can open lesions but it is painful. |
|

What is the boggly plaque seen here called?
What is it associated with and how does it get transmitted? |
Boggy plaque = kerion (from inflammatory response)
Tinea Capitis is also seen (trasmit via shared hair brush, fomites). i.e. scalp ringworm |
|

What is the most common cause of tinea capitis? Second most common cause? How can you tell the difference between these two?
|

Trichophyton tonsurans = most common cause (seen in African Americans typically). Does not fluoresce.
Microsporum canis= 2nd most common *transmitted by infected cat/dog. Fluoresces blue/green under wood's lamp. |
|

How could you diagnose this causative agent in your office? What would you do to treat this?
|
This is microsporum canis, t. capitis (alopecia with broken hair often seen).
KOH prep: to show endothrix (t. tonsurans) or ectothrix (m. canis). *Treat with GRISEOFULVIN, or Terbinafine (of flucanazole) |
|
|
How are warts transmitted?
|
Skin-to-skin contact, fomites (locker room floor), autotransmission, vertical transmission at birth.
|
|
|
Name the wart:
1. common wart 2. flat wart 3. plantar warts (on feed) 4. anogenital or mucosal warts |

1. common = verrucae vulgaris
2. flat = verrucae plana 3. plantar= verrucae plantaris 4. genital = verruca acuminata |
|

What type of wart is this? what is the black dot?
|
Common wart = verrucae vulgaris
Black dot represents thrombosed capillaries |
|

What type of warts are seen here?
|
Verruca plana- flat warts
Flat top papules, can koebnerize to form linear arrangements due to scratching |
|
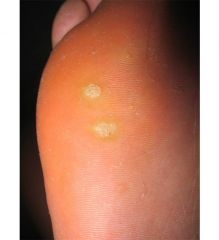
How do you distinguish these spots (are they warts or corns)?
|
Plantar warts (typically in weight bearing areas). Can become tender.
Warts, when shaved have small black dot appearance (whereas corns do not). Corns= pinpoint callus on foot. |
|

A child that is <2 years old has this presentation. What do you suspect is the causative agent and what is the mode of transmission?
|
<2= likely vertical transmission, Genital HPV (6,11)
2-8= likely from sexual abuse, Genital HPV 6,11 |
|
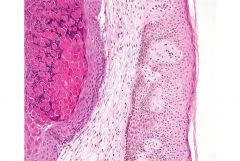
What is seen on this histopathology? How do you treat it?
|
HPV (note the halo around nucleus)
No specific antiviral treatment! Wait for it to regress, use keratolytics, cryosurgery, or podophyllin/trichloroacetic acid for condyloma acuminata. |
|

What infectious agent causes this disease? How was it transmitted? Is the child contagious?
|
Parvovirus B19-- causes fifth's disease (slap in the face appearance). Transmitted via respiratory route.
The child, one they have macular erythema rash, is not contagious. |
|

What is the condition seen here?
|
Irritant diaper dermatitis (note the sparing of the folds!).
Erythema, maceration, and scale from wetness, urinary contact. |
|

What condition is seen here? How do you know?
|

Candida diaper dermatitis. You can make it out because of the satellite lesions and colorette of scale.
Child might also have thrush (oral candidiasis) |
|

What condition is this? How does it differ from diaper dermatitis?
|
Napkin psoriasis (resembles seborrheic dermatitis). Well demarcated areas of erythema that INVOLVE the crease (unlike diaper dermatitis which spares the creases)
|
|

What is this condition called? How would the baby present? How would you treat it?
|

Acrodermatitis enteropathica
Baby may be irritable, have diarrhea, periorofacial/acral dermatitis, and alopecia Typically seen after weaning (lack of Zn from breast milk). GIVE ZINC! |
|

This child presents with a diaper dermatitis that is resistant to treatment. The rash is composed of brownish papules and purpura. This lesion is also found under the arms. What might it be?
|

Langerhans cell histiocytosis- refer to Hematology & get biopsy.
|
|

A child is found who has multiple lesions of this type. What else would seal the diagnosis of NF-1?
|
2+:
6+ cafe au lait Axillary freckling Plexiform neurofibroma Two or more lisch nodules of iris Optic nerve glioma family history |
|

What is the mutation in individuals with Neurofibromatosis 1?
What is the mode of transmission? |
Neurofibromin (gene on 17q). Encodes GTPase which acts as a tumor suppressor.
Mode of transmission = Autosomal Dominant |
|

This is subtle- but a child who has this condition in addition to multiple cafe-au-lait spots should be worked up for?
|

Tibial bowing (a skeletal dysplasia)- associated with NF-1.
Also note the plexiform neurofibroma that here mimics a necus. |
|

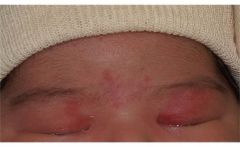
What does this little baby have? What is the major risk for the child?
|
Neonatal lupus erythematosus. Raccoon eyes= characteristic lesion.
Heart block (because antibodies can deposit in AV node and affect bundle of His) |
|

What is this condition primarily due to (what is the mode of transmission)?
|
Vertical transmission (transplacental transfer of IgG Anti-Ro SSA and Anti-La SSB antibodies).
*note: mom does not need to have active disease |
|

This 4.5 year old boy presents with a stubborn perianal rash that is not responding to topical steroid or nystatin. What is it?
|
Group A Beta-hemolytic strep infection
"strep tush" Tests positive for strep on throat culture |
|

What is this (note, the belt buckle)?
|
Nickel contact dermatitis
|