Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
167 Cards in this Set
- Front
- Back
|
What cells are located in the epidermis? |
-Keratinocytes
-Melanocytes -Langerhans cells -Merkel cells |
|
|
What structural elements are located with melanocytes
|
Produce melanin which gives us pigmentation and protects us from the sun
|
|
|
How many melanocytes for each keratinocyte?
|
1 melanocyte for each keratinocyte.
|
|
|
What are some important structures and facts about the basement membrane zone (BMZ) of the epidermis aka dermal-epidermal junction?
|
Structures
1. Lamina lucida 2. Basal lamina 3. Anchoring fibers Important fact: Many blistering diseases of the skin have their origin in the BMZ |
|
|
What is the main function of the dermis and its structures?
|
Support all dermal structures:
Dermal Structures: Blood vessels; nerves; sweat glands (apocrine and eccrine), sebaceous glands, hair follicles, nails, & matrix. |
|
|
What does the matrix of the dermis consist of?
|
Collagen, elastic fibers, & Ground substance.
|
|
|
What are the primary skin lesions?
|
-Macule
-Patch -Papule -Plaque -Pustule -Vesicle -Bullae |
|
|
What are the secondary skin lesions? |
-Scale
-Crust -Erosion -Ulceration -Fissure Atrophy -Scar |
|
|
What is a flat area of discoloration < 1cm?
|
Macule
|
|
|
What is a flat area of discoloration >= 1 cm? |
Patch
|
|
|
What is a raised palpable lesion < 1 cm?
|
Papule
|
|
|
What is a raised palpable lesion >= 1 cm?
|
Plaque
|
|
|
What is a raised fluid filled bump that is filled with pus?
|
Pustule
|
|
|
What is a raised fluid filled lesion < 1 cm that is filled with serous exudate (clear or cloudy)?
|
Vesicle
|
|
|
What is a raised fluid filled lesion >= 1 cm that is filled with serous exudate (clear or cloudy)
|
Bullae
|
|
|
What is a red plaque that is superimposed with stratum coreum that should not be there?
|
Scale
|
|
|
What is dried heme and exudates on a lesion called?
|
Crust aka scab
|
|
|
What is a circumscribed loss of epidermis called?
|
Erosion.
Note it is only epidermis |
|
|
What is a circumscribed area loss of epidermis & deeper layers called?
|
Ulceration
|
|
|
What is a circumscribed linear erosion/ulceration called?
|
Fissure
|
|
|
What is a circumscribed thinning of the skin called?
|
Atrophy
|
|
|
This is a hypertrophic area of the skin, which happens to be thicker than surrounding skin. What is this called?
|
Scar
|
|

What is this called?
|

Macule
|
|
What is this called?
|
Patch
|
|

What is there lesions called?
|

Papules and Plaques
|
|

What are these lesions called?
|

Vesicles and Bullae.
|
|

What are these lesions called?
|

Vesicles and Bullae
|
|

What are these lesions called?
|

Vesicles and Bullae
|
|

What is this?
|

Pustules
|
|

What is this?
|

Pustules
|
|

What is this?
|

Nodule
|
|

What is this?
|

Tumor (squamous cell carcinoma)
|
|

What is this?
|

Wheals (urticaria)
|
|

What is this?
|

Wheals (urticaria)
|
|

What is this?
|

Lichenification
|
|
What is this?
|
Lichenifaction
|
|
What is this?
|
Fissure
|
|

What is this?
|

Burrows
|
|

What is this?
|

Scale
|
|
|
What color does erythrasma fluoresce under wood's light?
|
Coral red color fluoresence under wood's light. See slide 27 of 74 in Office Procedures in Dermatology
|
|
|
What does KOH test for?
|
Fungi
|
|
|
What does Gram Stain test for?
|
bacteria
|
|
|
What does Scabies prep test for?
|
scabies
|
|
|
What does Tzanck smear test for?
|
Herpes Simplex Viruses. You are looking for multinucleated giant cells
|
|
|
What kind of conditions (_____alop:ecias) are the following
*Alopecia areata Telogen effluvium Androgenetic alopecia Trichotillomania |
Non-scarring alopecias
|
|
|
What alopecia disorder is associated with thyroid disease?
|
Alopecia areata
|
|
|
Does vitilago have an association with thyroid disease?
|
Yes
|
|
|
-Detachment of nail from its bed at distal/lateral attachments
-Creates a subungual space that collects dirt and keratinous debris Pseudomas can develop and cause a greenish discoloration |
Onycholysis
|
|
|
-Transverse line in nail, usually seen in all 20 nails and correlates to a form of systemic disease
-Occurs after any severe, sudden, acute, usually febrile illness -Correlates to telogen effluvium of the hair |
Onychoschizia-Beau’s Lines
|
|
|
Biting of the nails
|
Onychophagia
|
|
|
-Chronic infectious condition
--15-20% people 40-60 years old --90% of the elderly -Incidence has been rising due to: age, diabetes, immunosuppression, poor peripheral circulation, trauma -Can be portal of infection (diabetics) -Spreads to: other nails, skin, people -Socially unacceptable |
Onychomycosis
|
|
|
Premenopausal females are less likely to be infected- suggesting that estrogen may have a protective effect
Prepubertal children rarely affected-possibly due to faster growth of nails, less trauma |
Onychomycosis
|
|
|
Patterns of onychomycosis
|
-distal subungal onychomycosis
-superficial white onychomycosis -proximal subungal onychomycosis |
|
|
______ is the most common type of onychomycosis.
It is most often caused by Trichophyton rubrum or Trichophyton mentagrophytes. The manifestation of distal/lateral subungual onychomycosis begins with initial fungal penetration of the stratum corneum from the hyponychial area or from the nail fold. The disease is characterized by a yellow-brown discoloration of the nail plate, onycholysis, and subungual hyperkeratosis. |
Distal/lateral subungual onychomycosis
|
|
|
_______ _____onychomycosis
The fungi directly invade the nail plate. The most common causative agent is T. mentagrophytes. Species of Fusarium or Acremonium may also be the etiologic agents. Almost always found in toenails, superficial white onychomycosis is characterized by a white, crumbly, sometimes powdery, appearance. The initial lesions may be randomly dispersed but will eventually coalesce to include the entire surface of the nail. This infection is capable of producing progressive dystrophy of the nails. Superficial white onychomycosis may also be a sign of HIV infection. |
Superficial white onychomycosis
|
|
|
______ _______ onychomycosis Penetrates the proximal portion of the nail
Hallmark sign of HIV infection Occurs in both fingernails and toenails |
Proximal subungal onychomycosis
|
|
|
What is the disease based on the following:
Pitting Subungual hyperkeratosis Onycholysis Oil Spot- yellow spots under the nail plate Affects 25% of patients with psoriasis Most treatments are unsatisfactory |
Psoriatic Nail Disease
|
|
|
-Diabetic peripheral neuropathy
-Ulceration of 3rd toe from elongated, mycotic nail |
Onychogryphosis
|
|
|
Based on the following what is this?:
Epidermal tumors caused by the human papillomavirus (HPV) |
Verrucae
|
|
|
Based on the following what is this?
Common contagious tumors Seen most commonly in children, young adults Transmitted by direct human-to-human contact 3 common types of cutaneous warts: common, plantar, flat |
Verrucae
|
|
|
Self-limited epidermal viral infection
Flesh-colored to pink umbilicated papules, usually grouped Can have central keratotic plug Seen in children and sexually active adults. -Two separate diseases – 99% is classical condition in children (5 per week) -Second condition is rare 1 per year |
Molluscum Contagiosum
|
|
|
MCV is a pox virus
Transmitted via skin-to skin contact Can koebnerize Can be extensive in HIV+ patients Usually resolve in 6 months |
Mollusum Contagiosum
|
|
|
-As the viral lesions heal they tend to hypertrophy and crust over
-Represents ‘immune response’ to therapy -Some form of destruction -Drying agent -Irritate the lesion. Create an inflammatory response. The inflammatory response activates the Immune system response. This a sign of a Immature immune system. |
Molluscum Healing
|
|
|
What is the most prevalent STD?
|
Herpes Simplex...The gift that keeps on giving :-)
|
|
|
What is the prevalence of Herpes?
|
45 million people
|
|
|
What do Primary Care Physicians think about herepes with respect to their patient population?
|
Although Genital Herpes is one of the most common STDs, many primary care physicians believe it is virtually nonexistent in their patient population?
(50/300 = 15 %) ~ 1 in 6 patients |
|
|
What are group vesicles on erythematous base?
|
Herpes, Herpes, Herpes
Valtrex, Valtrex, Valtrex!!! |
|
|
What percent of adults are exposed to herpes simplex type 1?
|
85 %
|
|
|
Where do recurrent infections of Herpes occur?
|
mucocutaneous sites, oral mucosa are rarely involved.
|
|
|
What are these?
UV exposure, fever, colds, stress |
Precipitating factors for recurrent herpes infections.
|
|
|
Bullseye targetoid lesions are called?
|
Erythema Multiforme
|
|
|
What is the number one cause of Erythema Multiforme?
|
Herpes Simplex Virus
|
|
|
With Herpes Simplex Virus recurrence happen at the site of ________.
|
innoculation
|
|
|
At time of ___________, HSV ascends peripheral sensory nerves and enters sensory or autonomic nerve root ganglia where latency is established
|
innoculation
|
|
|
Any herpetic infection around the eye requires examination of the cornea.
|
Periocular herpes
|
|
|
Vesicles have dried up and erosions remain
______ should always be in your d/d when you see crusted erosions |
herpes
|
|
|
Most commonly associated with eczema but can be seen with other disorders
Associated with fever, malaise, irritability Lesions are not ‘grouped’ but disseminated (everywhere) |
Eczema Herpeticum
|
|
|
Initial lesions are usually papules and are not usually observed, quickly evolve into vesicles which appear as “dewdrops on a rose petal”
Vesicles umbilicate and rapidly evolve to pustules and crusts over 8-12 hours Lesions develop in crops and will be seen in all stages of evolution |
Varicella Zoster
|
|
|
Lesions first develop on face and scalp and spread inferiorly to trunk and extremities
Most profuse in areas least exposed to pressure Mucous membranes-including nose, conjunctiva, pharynx, larynx, trachea, Gi tract, urinary tract and vagina can be involved |
Varicella Zoster
|
|
|
Mortality rate in children is 1 per 50,000 cases or 100 deaths annually
Complications in children: bacterial superinfections, encephalitis, Reye’s syndrome Adults: Prolonged recovery, pneumonia (16%), encephalitis, arthritis, carditis, orchitis Mortality rate in adults is 15/50,000 cases |
Varicella Zoster
|
|
|
Varicella immunization is 80% effective in preventing primary VZV infection
Uncertain how long immunity lasts Zoster still occurs, rate is unknown |
Varivax
|
|
|
Reactivation of VZV
Unilateral pain and a vesicular eruption limited to a dermatome 70% of cases age>50 1/3 as contagious as varicella |
Herpes Zoster
|
|
|
Prodromal stage: Neuritic pain precedes eruption by 3-5 days
Active vesiculation: 3-5 days Crust formation: day 2 - 3 weeks Postherpetic neuralgia: months to years |
Zoster "Shingles"
|
|
|
Nasocilliary branch of the trigeminal nerve is involved
Refer to Ophthalmology |
Hutchinson’s Sign
|
|
|
Pain lasting> 30 days after lesions have cleared
Corticosteroids have been used with antivirals to reduce PHN Ticyclic antidepressants (nortriptyline) and gabapentin have been shown to be helpful Lidocaine patches and capsaicin cream Frequent contact with children seem to decrease the incidence of zoster |
Post herpetic Neuralgia
|
|
|
-Sites of predilection : Thoracic 50%, trigeminal 10-20%, lumbosacral/ cervical 10-20%
-7 times more common in immunocompromised patients, esp. HIV + |
Zoster
|
|
|
May 25, 2006 – The FDA approved the first vaccine for zoster
The agency cleared the vaccine -- known as Zostavax -- for use in adults age 60 and older: studies showed it prevents zoster roughly half the time. More than 1 million cases of Zoster yearly in US Vaccinated patients are 1/3 less likely to develop PHN, and have fewer lesions and pain |
Zostavax
|
|
|
What is this list:
Drug eruption Secondary syphillis (check RPR) Guttate psoriasis Eczema Parapsoriasis Erythema multiforme |
Pityriasis Rosea Differential Diagnosis
|
|
|
-Acute eruption with a distinctive morphology, and a characteristic course
-Starts with a primary or “herald” plaque usually on the trunk -1-2 weeks later a generalized secondary eruption develops in a typical pattern -Spontaneous remission in 6 weeks -Usually only MILDLY pruritic |
Pityriasis Rosea
|
|
|
Acute or chronic dermatosis involving skin and/or mucous membranes
Characterized by the “4 P’s” : Pruritic, Purple, Polygonal, Papules Typical distribution: flexor surfaces (wrists) lumbar region, eyelids, shins, scalp, penis Oral lesions typically show a lacy white reticular pattern on the buccal mucosa, can also be erosive |
Lichen Planus
|
|
|
Nails: can cause destruction of the nail fold and nail bed.
Scalp: scarring alopecia Koebner phenomenon May be associated with Hepatitis C |
Lichen Planus
|
|
|
-Sexually transmitted disease caused by Treponema pallidum
-Starts with a painless ulcer at site of innoculation -Goes on to become systemic with secondary and tertiary stages |
Syphillis
|
|
|
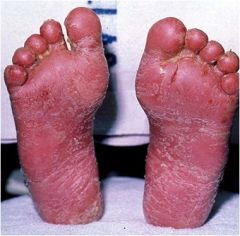
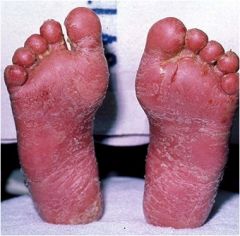
Teeming with spiroketes; palms & soles
|
Syphillis
|
|
|
Painless chancres at innoculation site; goes away
|
Syphillis
|
|
|
-Appears 2-6 months after primary infection and 2-10 weeks after appearance of primary chancre
-May have ‘acute illness syndrome’: fever, chills, arthralgia, myalgia, malaise -Skin lesions: macules & papules scattered over trunk, neck, palms and soles -Hair loss: ‘moth-eaten’ alopecia on scalp and beard areas -Condyloma Lata: Soft, flat-topped pink papules on perianal area |
Secondary Syphillis
|
|
|
-Aka: “The great imitator”……can look like any papulosquamous disease
-Lesions associated with secondary syphillis are ‘teeming with spirochetes |
Still Secondary Syphillis
|
|
|
-Develops 2-60 years after primary lesions
-Noduloulcerative: plaques and nodules with scars healed in the center -Gumma: rubbery lump or deep lesion found in subcutaneous tissue |
Tertiary Syphillis
|
|
|
Acne is a multifactorial inflammatory disease affecting pilosebaceous follicles
Pathogenesis is not completely understood Microcomedo is the primary acne lesion |
Acne Vulgaris
|
|
|
-Abnormal desquamation of follicular keratinocytes
-Sebum production -Proliferation of Propionibacterium acnes -Inflammation and immune response |
4 major factors in the etiology of acne vulgaris
|
|
|
What are the subtypes of hyperplasia
|
-Vascular
-Papulopustular -Sebaceous Hyperplasia -Ocular |
|
|
-Flushing and persistent central facial erythema, +/- telangiectasia
-Edema can develop from recurrent vasodilation |
Vascular Rosacea
|
|
|
What kind of Rosacea?
-Persistent facial erythema with transient papules and pustules -Not centered around a comedo -Keratinization defects play no role in rosacea |
Papulopustular Rosacea
|
|
|
What kind of Rosacea?
-Initial process is overgrowth of sebaceous glands -Skin appears thicker and smoother -Irregular surface enlargement and nodularities develop as fibrosis occurs |
Sebaceous Hyperplasia
|
|
|
What kind of rosacea?
-Occurs in up to 50% of rosacea patients -Foreign body sensation in the eyes, burning or stinging, dryness, itching, photosensitivity, recurrent styes, blurred vision, telangiectasia of the sclera, periorbital edema -Meiobian gland impaction-decreased lipid in tear film, greater tear evaporation, irritability of the eyes |
Ocular Rosacea
|
|
|
Characteristic
Papules and Pustules: Yes Erythema: yes Telangiectasia: yes Comedones: No Usually Age > 25-30: Yes |
Rosacea
|
|
|
Characteristics
Papules and Pustules: Yes Erythema: No Telangiectasia: No Comedones: Yes Usually Age < 25: Yes |
Acne
|
|
|
What are these lesions?
-Seborrheic keratosis -Cherry angioma -Spider angioma -Melanocytic nevus -Halo nevus |
Benign Tumors of the skin
|
|
|
What skin lesion?
-Most common benign epithelial tumor -Hereditary -Start at around age 30 -Can be few or multiple -Vary in morphology and color depending on location of body |
Seborrheic keratosis
|
|
|
What skin lesion?
-Very common, bright red to violaceous domed papules -Can thrombose and appear black -Most commonly on the trunk -Develop around age 30 -Can be multiple -Only a cosmetic nuisance |
Cherry angioma
|
|
|
What is this skin lesion?
-One of the most common lesions in Caucasians -Most adults have 20 -Appear in early childhood -Gradually involute around 60 |
Acquired Melanocytic Nevus
|
|
|
What is this skin lesion?
-Nevus surrounded by a halo of leukoderma or depigmentation -Immunologic phenomenon via action of cytotoxic lymphocytes -Nevus will usually disappear in months-years -Skin repigments in months-years -May occur on one or multiple nevi -Possible precursor to vitiligo |
Halo Nevus
|
|
|
What kind of tumors are the following lesions?
-Basal cell carcinoma -Squamous cell carcinoma -Malignant melanoma |
Malignant Tumors of the skin
|
|
|
What type malignant tumor?
-Most common type of skin cancer -Slow growing -Locally invasive and destructive but not metastatic -Usually in sun-exposed areas in fair-skinned people |
Basal Cell Carcinoma
|
|
|
What type of skin cancer is described?
-Typically looks like a ‘pearly’ shiny papule with overlying telangiectasia and rolled borders -Center may be ulcerative -Several variants: superficial, sclerosing, pigmented |
Basal Cell Carcinoma
|
|
|
What is this a description of ?
It can look like a shiny bump or nodule that is pearly or translucent and is often pink, red or white. In dark-haired people it can be tan, black or brown. |
Basal Cell Carcinoma
|
|
|
You are think you patient has eczema and your treat her with steroids. It does not clear. What does she have? What should you do?
|
Superficial Basal Cell Carcinoma (BCC);
Biopsy |
|
|
This is a common appearance of what?
-a pink growth with a slightly raised, rolled border and a crusted indentation in the center, similar to a donut with an indented center. |
Basal Cell Carcinoma
|
|
|
What are the three ways to prevent basal cell carcinoma?
|
hat, sunglasses, and sunscreen
|
|
|
Whatkind of cancer does the following describe?
-2nd most common type of skin cancer -Sun exposed areas in fair-skinned people -Erythematous, keratotic nodule, may ulcerate |
Squamous Cell Carcinoma
|
|
|
What type of cancer?
Can metastasize (3-4%) Most common skin cancer in black patients Can occur in burn scars-Marjolin’s ulcer- met rate is 20% |
Squamous Cell Carcinoma
|
|
|
What is the most common skin cancer in black patients?
|
Squamous Cell Carcinoma
|
|

What is this lesion?
|

Basal Cell Carcinoma
|
|

What is this lesion?
|

Basal Cell Carcinoma
|
|

What is this lesion?
|

Squamous Cell Carcinoma
|
|

What type of cancer? What disease do this boy has?
|

Squamous Cell Carcinoma. Xeroderma Pigmentosum
|
|

This is a seven-year-old girl. What disease does she have? What lesions do you see?
|

She has xeroderma pigmentosum. Multiple actinic keratoses & SCCs
|
|

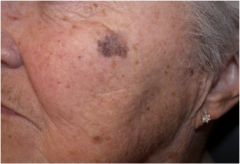
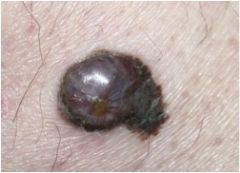
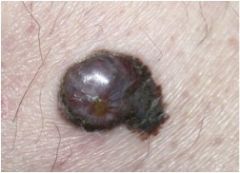
What is this?
|

Melanoma
|
|
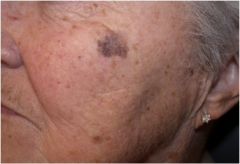
What is this?
|
melanoma
|
|

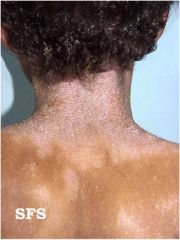
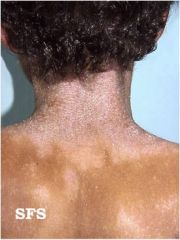
What is this?
|

melanoma
|
|
|
What are the ABC's of melanoma?
|
Asymmetry
Border irregularity Color Diameter Every type of change. |
|
|
What should you do with any type of change in the skin that doesn't go away in a timely manner?
|
Check it.
|
|
|
What is the most common dermatophyte.
|
T. rubrums
|
|
|
What is this most common candida pathogen?
|
C. Albicans
|
|
|
What conditions shows "spaphetti and meatballs" on KOH?
|
T. versicolr
|
|
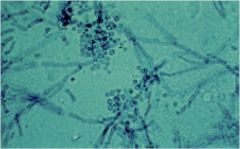
This slide prepared with KOH, shows "spaghetti and meatballs" What is the pathogen
|
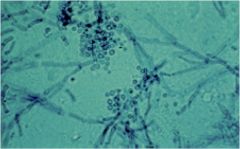
T. versicolor
|
|
|
Tinea capitis
|
Scalp
|
|
|
Tinea pedis
|
Feet (athletes foot)
|
|
|
Tinea manuum
|
Hands
|
|
|
Tinea cruris
|
Groin
|
|
|
Tinea barbae
|
Beard, hair
|
|
|
Tinea corporis
|
Body
|
|
|
Tinea unguium
|
Nails
|
|
|
Tinea unguium
|
(onychomycosis)
|
|
|
Etiologic agent is Phaeoannellomyces werneckii
Mostly seen in the tropics Brown to black lesion on hands and feet |
Tinea nigra
|
|
|
Dimorphic fungus
In soil and on plants (rosebushes and mulches) Worldwide Occupational disease of gardeners, florists, farmers etc. |
Sporothrix schenckii
|
|
|
Painless papule – enlarge then open sore – along lymphatic drainage you will nodules
See a case every few years |
Sporotrichosis
|
|
|
Genetic, environmental and immune factors
Genetics: risk of developing AD significantly higher if parents have an atopic disease Environmental: food/aeroallergens, various non-allergic factors, ie. Trauma, low humidity, sweating, emotional stress, any viral infection, xerosis Immune: Upregulation of interleukins, persistent monocyte activation, increased eosinophil infiltration in the skin and elevated serum levels of IgE |
Etiologic factors of atopic dermatitis
|
|
|
Which immunoglobulin is elevated in contact dermatitis?
|
IgE
|
|
|
Typically, Infantile eczema affects the facial areas
Teens and older children tend to develop it in the folds of the antecubital and popliteal fossae Adults tend to develop lesions on the hands, feet and trunk but this can vary greatly among individuals |
Presentation of Atopic dermatitis will vary with age.
|
|
|
These are ______________
Tachyphylaxis (diminishing efficacy) Skin side effects Atrophy, telangiectasia, striae, dyspigmentation HPA-axis suppression (reduced cortisol) A greater concern in children because: Higher body surface area (BSA) to weight ratios than adults Occlusion in diaper areas increases absorption Cushing’s syndrome and potential for growth retardation Risk of cataract and glaucoma |
Issues associated with treating the skin with topical steroids
|
|
|
Classic delayed cell-mediated hypersensitivity reaction
Sensitization can occur quickly with strong sensitizers, like poison ivy, or over years Antigen is absorbed in skin by Langerhans cells-processes antigen and takes it to lymph nodes and T cells-sensitized T cells then enter blood circulation-then all of the skin becomes hypersensitive to the allergen |
Etiology of contact dermatitis and sensitization.
|
|
|
Localized form of lichenification
Characteristic feature of AD but can occur independent of AD Results from rubbing and scratching at an area for months to years Often related to emotional stress Patients often say that the scratching becomes pleasurable and will scratch until it bleeds |
Lichen simplex chronicus
|
|
|
Occurs in the winter in elderly
Skin is dry, ‘cracked’, fissured with slight scaling Persists for months Due to too frequent bathing in hot water and too much heat in the house |
asteatotic eczema
|
|
|
Chronic, pruritic, inflammatory dermatitis occurring in the form of coin shaped plaques
Common on lower legs of elderly men in the winter months |
nummular eczema
|
|
|
Hypopigmented to slightly pink, lightly scaly plaques on face, trunk, arms
Associated with AD |
Pityriasis Alba
|
|
|
Chronic, self-limited dermatosis of the dermis
Annular plaques usually on hands and feet Common in children Disappears in 2 yrs in 75% of pts Recurrences are common Often dx as tinea |
granuloma annulare
|
|

What is this?
|

Lichenification
|
|
|
What is the target of biologic agents used for treatment of psoriasis
|
TNF
T-lymphocytes (T-cells) |
|
|
Major defect mediating psoriasis
|
TNF is a critical mediator of psoriatic inflammation, playing a central role in the inflammatory response
Psoriatic plaques have high levels of TNF |
|
|
TNF can trigger multiple destructive effects, including ____ levels in the skin causing epidermal _______.
|
excess;thickness.
|
|
|
List the biologic agents used to treat psoriasis.
|
Etanercept (Enbrel) -TNF
infliximab (Remicade) - TNF adalimumab (Humira) - TNF efalizumab (Raptiva) - T cells alefacept (Amevive) - T cells |
|
|
Definition of Psoriasis
|
Psoriasis is a systemic, chronic genetic disease that is not contagious. Psoriasis is characterized by raised, thick inflammed patches of skin that are covered by silvery-white scales and are associated with local itching or burning.
|
|
|
What is this a description of ?
Immune system is mistakenly triggered which speeds up the growth cycle of skin cells Normal cell matures and sheds in 30 days Psoriatic skin cell matures in 3-4 days Instead of shedding, the cells build up and form plaques |
Etiology of Psoriasis
|
|
|
Population affected: 7 million (2.6% of US population)
Gender: Equal distribution between men and women Age of onset: Mean 28 years New cases: Between 150,000 and 260,000 cases/year Undertreatment: 50% with active disease not currently treated Outpatient costs: $1.6 to $3.2 billion/year |
Psoriasis Statistics
|
|
|
Psoriasis on <5% of BSA
Does not Impact on patient’s quality life Treatment Moisturizers, OTC products, topical steroids, vitamin D3 and A derivatives Treatments have no known serious risks |
Clinical Definition of Psoriasis: Mild
|
|
|
Body surface area
Psoriasis 5% of BSA Impact on patient’s life Psoriasis does impact quality of life Expectation is that therapies will improve quality of life Treatment Phototherapy, topicals, and systemic oral medications Therapies have toxicities associated with long term use that limit effectiveness and may be inconvenient, expensive, and time-consuming |
Clinical Definition of Psoriasis: Moderate to Severe
|
|
|
Body surface area
Psoriasis on generally >10% of BSA Impact on patient’s life Disease may alter the patient’s quality of life Patients may be willing to accept medications with potentially significant side effects Treatment A satisfactory response is usually not achieved by treatments that have minimal risks |
Severe Psoraisis
|