Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
236 Cards in this Set
- Front
- Back
|
What are the classic findings of Henoch-Schönlein purpura?
|
Palpable purpura
GI symptoms (Abd pain, vomiting, guaiac (+) stool, intussesception) Renal disease Arthritis/ arthralgia |
|
|
What are Ranson’s criteria in determining the prognosis in pts with acute pancreatitis?
|
criteria at admission: Glucose, AST, LDH, Age, WBC ct
criteria (after 48 hrs): Ca2+ Hematocrit, O2, BUN, Base deficit, sequestration of fluid |
|
|
What is the tx for diarrhea from Entameoba histolytica?
|
Metronidazole
|
|
|
What is the tx for diarrhea from
Giardia lamblia? |
Metronidazole
|
|
|
What is the tx for diarrhea from Salmonella ?
|
Fluroquinolones
TMP-SMX (Bactrim) |
|
|
What is the tx for diarrhea from Shigella?
|
Fluroquinolones
TMP-SMX (Bactrim) |
|
|
What is the tx for diarrhea from Campylobacter?
|
Erythromycin
|
|
|
Which type of lung cancer is assoc with the following paraneoplastic syndrome
Elevated ACTH → glucocorticoid excess → Cushing’s Syndrome |

Small cell
|
|
|
Which type of lung cancer is assoc with the following paraneoplastic syndrome
Elevated PTH related peptide → hypercalcemia |

Squamous cell
|
|
|
Which type of lung cancer is assoc with the following paraneoplastic syndrome
Elevated ADH → SIADH → hyponatremia |

Small Cell
|
|
|
Which type of lung cancer is assoc with the following paraneoplastic syndrome
Antibodies to presynaptic Ca2+ Channels → Lambert-Eaton Syndrome |

Small cell
|
|
|
Which type of vasculitis would you suspect with:
Weak pulses in upper extremity |
Takayasu’s Arteritis
|
|
|
Which type of vasculitis would you suspect with:
Necrotizing granulomas of lung & necrotizing glomerulonephritis |
Wegener’s Granulomatosis
|
|
|
Which type of vasculitis would you suspect with:
Necrotizing immune complex inflammation of visceral/renal vessels |
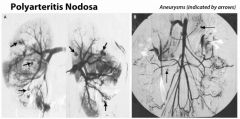
Polyarteritis nodosa
|
|
|
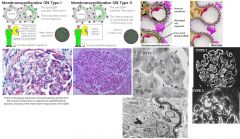
Which type of vasculitis would you suspect in young male smokers?
|
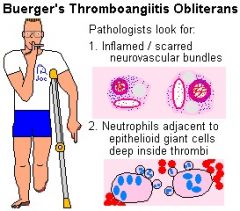
Buerger’s Thromboangiitis Obliterans
(Note: do not confuse with Berger's IgA nephropathy, a glomerular disease) Buerger disease is a segmental, inflammatory, and thrombotic process of the distal most arteries and occasionally veins of the extremities. Pathologic examination reveals arteritis in the affected vessels. The cause is not known but it is rarely seen in nonsmokers. Arteries most commonly affected are the plantar and digital vessels of the foot and lower leg. In advanced stages, the fingers and hands may become involved. Fortunately, the incidence of Buerger disease seems to have decreased in the past decade. |
|
|
Which type of vasculitis would you suspect in young asian women?
|
Takayasu’s Arteritis
|
|
|
Which type of vasculitis would you suspect in young asthmatics?
|
Churg-Strauss
|
|
|
Which type of vasculitis would you suspect in infants & young children with involved coronary arteries
|
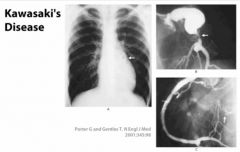
Kawasaki Disease
|
|
|
what is the most common vasculitis?
|
Temporal (Giant cell) arteritis
|
|
|
Which type of vasculitis is assoc with hep B infection?
|
Polyarteritis nodosa
|
|
|
Which type of vasculitis would you suspect with:
Occlusion of the ophthalmic artery, (that can lead to blindness) |
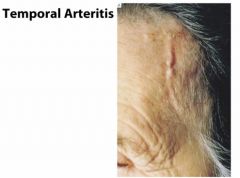
Temporal (giant cell) arteritis
|
|
|
Which type of vasculitis would you suspect with: perforation of nasal septum
|
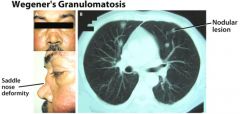
Wegener’s Granulomatosis
|
|
|
Which type of vasculitis would you suspect with:
Unilateral headache, jaw claudication |
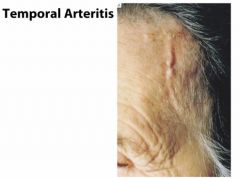
Temporal (giant cell) arteritis
|
|
|
Which lipid-lowering drug is assoc with:
SE: facial flushing |
Niacin (vit B3)
Can tx with aspirin |
|
|
Which lipid-lowering drug is assoc with:
SE: ↑ LFTs, myositis |
Statins (lovastatin) &
Fibrates (gemfibrozil) |
|
|
Which lipid-lowering drug is assoc with:
SE: GI discomfort, bad taste |
Bile acid resins (cholestyramine, colestipol, colesevelam)
|
|
|
Which lipid-lowering drug has the Best effect on HDL
|
Niacin (vit B3)
|
|
|
Which lipid-lowering drug has the Best effect on triglycerides/ VLDL
|
Fibrates (gemfibrozil, clofibrate, bezafibrate, fenofibrate)
|
|
|
Which lipid-lowering drug has the Best effect on ↓ LDL/ cholesterol
|
Statins (lovastatin)
|
|
|
Which lipid-lowering drug binds C. diff. toxin?
|
Cholestyramine
|
|
|
What drugs are known for causing ↑ prolactin levels?
|
Phenothiazines
Risperidone Haloperidol Methyldopa Verapamil |
|
|
What are the side effects of HCTZ?
|
AE: “HyperGLUC”
hyperGlycemia hyperLipidemia hyperUricemia hyperCalcemia also sulfa allergies |
|
|
What diuretic or class of diuretic would be most helpful in pt with Acute pulmonary edema
|
Loop Diuretic – Furosemide
|
|
|
What diuretic or class of diuretic would be most helpful in pt with Idiopathic hypercalcinuria
(→ calcium stones) |
Thiazide Diuretics
|
|
|
What diuretic or class of diuretic would be most helpful in pt with Glaucoma
|
Acetazolamide, Mannitol
|
|
|
What diuretic or class of diuretic would be most helpful in pt with Mild – mod CHF with expanded ECV
|
Thiazide or Loop Diuretics
|
|
|
What diuretic or class of diuretic would be most helpful in conjunction with loop or thiazide diuretic to retain K+
|
K+ sparing diuretic – Spironolactone, Amiloride
|
|
|
What diuretic or class of diuretic would be most helpful in pt with Edema due to nephrotic syndrome
|
Loop
|
|
|
What diuretic or class of diuretic would be most helpful in pt with ↑ intracranial pressure
|
Mannitol
|
|
|
What diuretic or class of diuretic would be most helpful in pt with Mild – mod HTN
|
Thiazide (HCTZ)
|
|
|
What diuretic or class of diuretic would be most helpful in pt with hypercalcemia
|
Loop Diuretic
|
|
|
What diuretic or class of diuretic would be most helpful in pt with Altitude sickness
|
Acetazolamide
|
|
|
What diuretic or class of diuretic would be most helpful in pt with hyperaldosteronism
|
Spironolactone or Eplerenone
|
|
|
What are the 2 common disorders that carbonic anhydrase inhibitors (acetozolamide) treat?
|
Glaucoma
Altitude sickness |
|
|
What diuretic is used in the initial stage of ↑ ICP?
|
Mannitol
|
|
|
What are the adverse effects of Mannitol?
|
Mannitol draws free water into the vasculature:
Initial dilutional hypOnatremia which may result in pulmonary edema Ultimately hypernatremia, hyperosmolality |
|
|
Which diuretics lose Ca2+ in the urine and are therefore contraindicated in nephrolithiasis pts? Which diuretics help to retain serum Ca2+?
|
“loops lose Ca2+, thiazides don’t”
|
|
|
Which side effect is commonly associated with the K+ -sparing duretic spironolactone?
|
Gynecomastia
|
|
|
What bacteria typically causes pyelonephritis?
|
#1 E. coli (ascending infxn most commonly)
others: Staph saprophyticus, Klebsiella, Proteus mirabilis |
|
|
What are the S/S of pyelonephritis?
|
Flank pain
Chills Nausea/vomiting Urinary frequency, dysuria, urgency Fever Costovertebral angle (CVA) tenderness |
|
|
How many bacteria have to be present in the urine sample to diagnosis pyelonephritis?
|
> 10^5
|
|
|
What is the treatment for pyelonephritis?
|
(usually admit pt & give IVF)
Fluoroquinolones 3rd Gen Ceph if preggers → ampicillin/gentamicin or Ceftriaxone |
|
|
What is the pattern of pain assoc with nephrolithiasis?
|
Colicky flank pain, can extend into groin or genitals
Usually unilateral |
|
|
What is the tx for radiolucent kidney stones? What are these stones made of?
|
Made of: uric acid
Tx: alkalinize urine Note: uric acid stones are the ONLY stones that be be dissolved with medical therapy |
|
|
What do Proteus & Klebsiella produce that causes the formation of the struvite stone (Mg-NH4-PO4)?
|
urease
|
|
|
What studies will you use to diagnose most kidney stones?
|
Xray or CT
Note: if pt has new onset hematuria, need to r/o stones! |
|
|
What should be done in a female smoker over age 50 with hematuria besides a UA?
|
Cystoscopy
|
|
|
What class of diuretic is commonly used in pts with renal stones due to hypercalciuria in pts with a normal serum Ca2+ level?
|
Thiazides
|
|
|
What is the most common location of renal stone impaction?
|
Ureterovesical junction
|
|
|
What intracranial abnormality is assoc with autosomal dominant polycystic kidney disease (ADPKD)?
|
Intracranial aneurysms
|
|
|
What should be done next in a pt who is a smoker with flank pain, weight loss, hematuria, and polycythemia?
|
Think cancer
Imaging to evaluated kidneys for tumor |
|
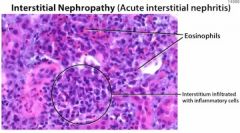
What is the most common cause of interstitial nephropathy/nephritis?
|
Medications → NSAIDs, aminoglycosides, β-lactams
|
|
|
A pt involved in a motor vehicle accident has a crushed thigh. Your attending advises you to make sure to give the pt enough IVF to maintain a high urine output of 100-200mL/hr. Why did he advise this?
|
Preventing interstitial nephropathy
|
|
|
Uncorrected severe benign prostatic hypertrophy (BPH) may cause what?
|
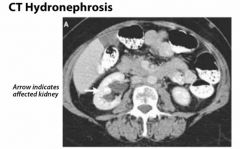
Bilateral hydronephrosis
|
|
|
What disease is the mnemonic “Can’t see, can’t pee, can’t hear” for? What does it stand for?
|
Dx: Alport’s Syndrome
Can’t see → cataracts Can’t pee → nephritis Can’t hear → high-frequency hearing loss |
|
|
what is the most common nephrotic syndrome in children?
|
minimal change disease
tx: steroids |
|
|
What is the most common nephrotic syndrome in adults?
|

membranous glomerulonephritis
|
|
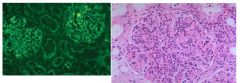
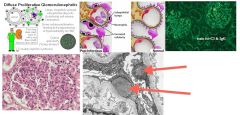
Which glomerular disease would you suspect with:
IF: granular pattern of immune complex deposition LM: hypercellular glomeruli |
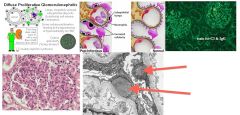
Post-strep glomerulonephritis
|
|
Which glomerular disease would you suspect with:
IF: linear pattern of immune complex deposition |

Goodpasture’s Syndrome
|
|
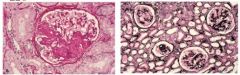
Which glomerular disease would you suspect with:
Kimmelstiel-Wilson lesions (nodular glomerulosclerosis) |

Diabetic Nephropathy
|
|
|
Which glomerular disease would you suspect with:
EM: loss of epithelial foot processes |
Minimal Change Disease
|
|
|
Which glomerular disease would you suspect with:
Nephrotic syndrome assoc with hepatitis B |
Membranoproliferative Glomerulonephritis (MPGN)
|
|

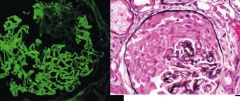
EM: mesangial cell proliferation
IF: IgA deposition |
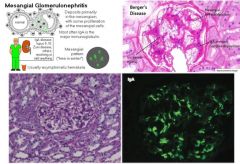
Berger’s Disease
(IgA Nephropathy) Dx: increased serum IgA Tx: occasionally self-limited; give ACEI and statins for persistent proteinuria give corticosteroids if nephrotic syndrome develops |
|
|
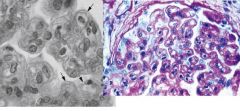
Which glomerular disease would you suspect with:
Nephrotic syndrome assoc with HIV |
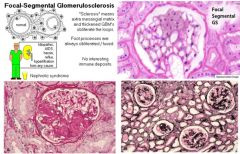
Focal Segmental Glomerulosclerosis (FSGS)
|
|
|
Which glomerular disease would you suspect with:
Anti-GBM antibodies, hematuria, hemoptysis |

Goodpasture’s Syndrome
|
|
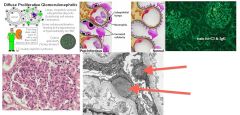
Which glomerular disease would you suspect with:
EM: subendothelial humps & tram-track appearance |
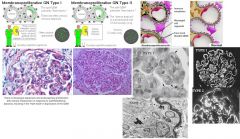
Membranoproliferative Glomerulonephritis (MPGN)
|
|
|
Which glomerular disease would you suspect in pt with Nephritis, deafness, cataracts
|
Alport’s Syndrome
|
|
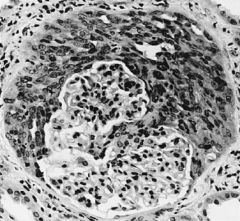
Which glomerular disease would you suspect with:
LM: crescent formation in the glomeruli |
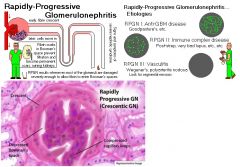
Rapidly Progressive (Crescentic) Glomerulonephritis (RPGN)
|
|
What glomerular disease would you suspect with:
LM: Segmental sclerosis and hyalinosis |
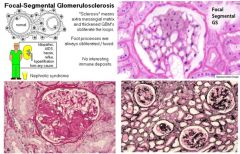
Focal Segmental Glomerulosclerosis (FSGS)
|
|

What glomerular disease would you suspect with:
Purpura on back of arms & legs, abd pain, IgA nephropathy |
Henoch Schlönlein Purpura
|
|
|
What glomerular disease would you suspect with:
Apple-green birefringence with Congo-red stain under polarized light |
Amyloidosis
|
|
|
What glomerular disease would you suspect with:
(+) ANCA |
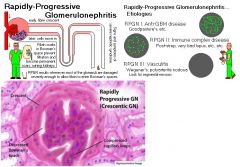
Rapidly Progressive (Crescentic) Glomerulonephritis (RPGN)
|
|
|
What glomerular disease would you suspect with:
Anti-dsDNA antibodies |
Lupus Nephritis
|
|
What glomerular disease would you suspect with:
EM: Spike & Dome pattern of the basement membrane |

Membranous GN
|
|
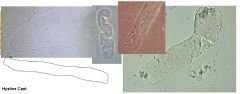
Which disease would you suspect with the finding of Hyaline casts
|
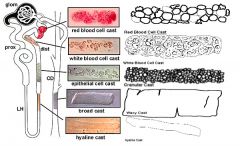
Not indicative of disease
|
|

Which disease would you suspect with the finding of Granular casts
|
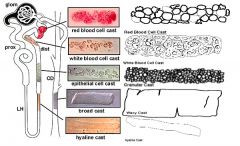
Chronic renal disease
|
|
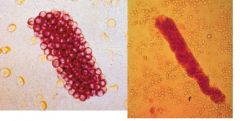
Which disease would you suspect with the finding of Red Cell casts
|
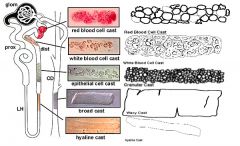
Glomerulonephritis or vasculitis
|
|
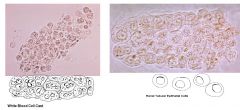
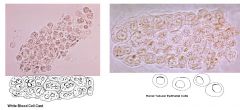
Which disease would you suspect with the finding of White Cell casts
|
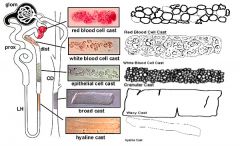
Tubulointerstitial disease or acute pyelonephritis
|
|
Which disease would you suspect with the finding of Epithelial cell casts
|
ATN & Acute GN
|
|
|
What are the defining characteristics of nephrotic syndrome?
|
>3g/day proteinuria
hypOalbuminemia hyperlipidemia |
|
|
What are the 3 drugs that can treat just about all the nephritic syndromes?
|
Corticosteroids
ACE inhibitors Statins |
|
|
What might you see on biopsy of a pt with hematuria & problems breathing (but no upper airway symptoms)?
|

Linear staining of IgG Ab on GBM
Dx: Goodpasture’s syndrome |
|
|
HYQ: glomerulonephritis + bilateral sensorineual deafness
|
Alport’s syndrome
|
|
|
What should be in the history of a pt with postinfectious glomerulonephritis?
|
Streptococcal infection w/in the last 3wks (check ASO)
|
|
|
What serum marker should tip you off that a pt has lupus nephritis?
|
Anti-DNA antibodies
|
|
|
What test might you order in conjunction with the renal biopsy in a pt with hematuria & dyspnea?
|
c-ANCA
dx: Wegener’s Granulomatosis |
|
|
What are the classic characteristics of a pt with minimal change disease?
|
Young child
Edema HTN ↑ freq of infections |
|
|
A HIV+ patient with nephrotic syndrome most likely has what disease?
|
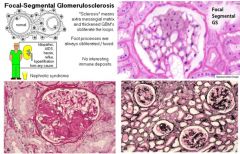
Focal Segmental Glomerulosclerosis (FSGS)
|
|
|
Membranous glomerulonephritis is the most common nephrotic syndrome and has what characteristic on biopsy?
|

Spike & Dome basement membrane thickening
|
|
|
What is the biopsy appearance of membranoprolierative glomerulonephritis?
|
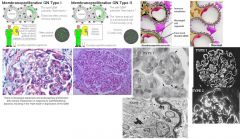
Double layer “train track” appearance
|
|
|
HYQ: 60yo M smoker is found to have a varicocele that does not empty when the pt is recumbent. What should you be suspicious of in this pt?
|
Renal Cell Carcinoma (RCC) → get CT of the abdomen
|
|
|
HYQ: what are the dietary recommendations in the treatment of nephrolithiasis?
|
Adequate dietary Ca2+
↑ fluid intake ↓ Na+ intake ↓ protein & oxalate intake |
|
|
HYQ: a young black male presents with painless hematuria – what should you suspect?
|
Sickle cell trait
|
|
|
HYQ: What is the treatment for uric acid renal stones?
|
Alkalinize urine
|
|
|
HYQ: what is the most common cause of nephrotic syndrome in African American males?
|
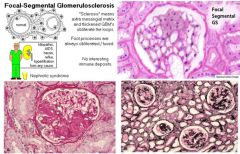
Focal Segmental Glomerulosclerosis (FSGS)
|
|
|
What medications are used in the treatment of Wegener’s granulomatosis?
|
Steroids
Cyclophosphamide |
|
|
What is the classic presentation of poststreptococcal glomerulonephritis?
|
Child with brown urine
HTN Strep infection 1-3wks ago High serum ASO titer |
|
|
What is the most common cause of morbidity & mortality in pts with SLE?
|
Lupus nephritis
|
|
|
Fever + rash + elevated creatinine + eosinophlia → what is the diagnosis?
|
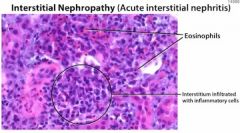
Acute interstitial nephritis (AIN)
|
|
|
What is the biggest risk factor for renal cell carcinoma?
|
smoking
|
|
|
What are 5 etiologies of temporary hematuria?
|
UTI
Nephrolithiasis Trauma Exercise Endometriosis |
|
|
What are 4 potassium sparing diuretics?
|
Spironolactone
Eplerenone Amiloride Triamterene |
|
|
What size calcium renal stone has a 50% likelihood of passing w/o surgical intervention?
|
8-9mm
|
|
|
What are the Treatment options for Chronic Kidney Disease?
|
● Stop smoking!
● aggressive BP control to goal <130/80 (JNC-7). Most need >3 medications (ACE-I or ARB, Β-blockers to reduce CAD risk, Diuretic (usually loop), Dihydropyridine CCB, Clonidine patch, Minoxidil in refractory cases) ● aggressive DM control to HgA1c goal of <6.5% with insulin and oral agents (usually not metformin) (rosiglitazone OK) ●agggressive Lipid control with statins to goal LDL <100 (but <70 is better) Statins have been shown to ↓ sepsis risk by 63% in pts on hemodialysis (JAMA 2007) ● Anemia aggressive control to goal Hg 11-12 For every ↓ in Hg of 0.5g/dL, increase risk of LVH by 32% (→ increase CAD and CVD risk) Usually requires iron and erythropoietin ●Vitamin D replacement ●Phosphate binders (Phos-Lo) ●Daily Aspirin 81mg to ↓ endothelial injury CAD risk |
|
|
In pre-renal acute renal failure (ARF) what is the value for the fractional excretion of sodium (FENa)? For the BUN:Cr ratio?
|
Pre-renal = hypotension (not perfusing kidneys)
FENa < 1% BUN:Cr >20 |
|
|
Which test is used for screening diabetic pts for kidney damage?
|
Urine microalbumin
|
|
|
What BP medications are renal protective and preferred in the treatment of HTN in chronic kidney disease (CKD) pts?
|
ACE-I and ARBs
|
|
|
What drug is used for chronic kidney disease (CKD) to lower their potassium levels on a chronic basis?
|
Sodium polystyrene sulfonate (Kayexalate)
|
|
|
What are the indications for dialysis?
|
Severe hypokalemia
Severe metabolic acidosis Severe fluid overload Uremic syndrome Cr >12 BUN >100 |
|
|
What is the difference btw hemodialysis and peritoneal dialysis?
|
Hemodialysis: blood is filtered thru a machine – arterio-venous fistulas placed in forearm
Peritoneal dialysis: fluid pumped into peritoneal space, filtered thru peritoneum & then pumped out (osmotic exchange) |
|
|
What are the normal lab values to assess in acid-base disorders?
|
pH 7.35-7.45
pCO2 35-45 mmHg pO2 75-105 mmHg HCO3- 22-28 mEq/L |
|
|
Determine acid-base disorder:
pH 7.4 HCO3 23 pCO2 40 |
Normal
|
|
|
Determine acid-base disorder:
pH 7.50 HCO3 35 pCO2 42 |
Metabolic acidosis
|
|
|
Determine acid-base disorder:
pH 7.33 HCO3 13 pCO2 28 |
Metabolic acidosis, Respiratory compensation
|
|
|
Determine acid-base disorder:
pH 7.42 HCO3 32 pCO2 64 |
Combined metabolic alkalosis, Respiratory acidosis
|
|
|
Determine acid-base disorder:
pH 7.24 HCO3 18 pCO2 40 |
Metabolic acidosis
|
|
|
Determine acid-base disorder:
pH 7.24 HCO3 24 pCO2 54 |
Respiratory Acidosis
|
|
|
Determine acid-base disorder:
pH 7.50 HCO3 22 pCO2 22 |
Respiratory Alkalosis
|
|
|
Determine acid-base disorder:
pH 7.58 HCO3 36 pCO2 30 |
combined metabolic & respiratory alkalosis
|
|
|
Determine acid-base disorder:
pH 7.47 HCO3 14 pCO2 22 |
Respiratory alkalosis, metabolic compensation
|
|
|
Determine acid-base disorder:
pH 7.46 HCO3 35 pCO2 53 |
Metabolic alkalosis, respiratory compensation
|
|
|
Determine acid-base disorder:
pH 7.39 HCO3 12 pCO2 22 |
Mixed metabolic acidosis, respiratory alkalosis
|
|
|
Determine acid-base disorder:
pH 7.34 HCO3 31 pCO2 62 |
Respiratory acidosis, Metabolic compensation
|
|
|
Determine acid-base disorder:
pH 7.10 HCO3 15 pCO2 50 |
Combined metabolic & respiratory acidosis
|
|
|
What is the differential diagnosis for metabolic acidosis with a normal anion gap? How can serum potassium be useful in narrowing the differential diagnosis?
|
Low serum K+ :
Diuretics Renal tubular acidosis types I & II Diarrhea Fanconi’s Syndrome High serum K+ : Addison’s Disease Renal tubular acidosis (RTA) type IV K+ sparing diuretics Hyperalimentation |
|
|
What is the differential diagnosis for elevated anion gap metabolic acidosis with high serum osmolality?
|
“MUDPILERS”
Methanol Uremia DKA/ Alcoholic KA Paraldehyde Isoniazid Lactic acidosis ETOH/ Ethylene Glycol Rhabdo/ Renal failure Salicylates |
|
|
What are the common causes of metabolic alkalosis?
|
Dehydration, Vomiting, Diuretics
|
|
|
What are the common causes of respiratory alkalosis?
|
Hyperventilation: High altitude, ASA toxicity, Pulmonary Embolism, Asthma
|
|
|
What are the common causes of respiratory acidosis?
|
COPD, Respiratory Depression (narcotic OD, neuromuscular dysfunction)
|
|
|
What are the common causes of Anion Gap Metabolic Acidosis?
|
“MUDPILERS”
Methanol, Uremia, DKA/ Alcoholic KA Paraldehyde, Isoniazid, Lactic acidosis ETOH/ Ethylene Glycol, Rhabdo/ Renal failure, Salicylates |
|
|
What are the common causes of Non-Gap Metabolic Acidosis?
|
Diarrhea, Renal tubular acidosis (RTA), TPN
|
|
|
A previously healthy 25yo M came to the hospital with a head injury and is now hypernatremic and has polyuria. What is the diagnosis?
|
Central Diabetes Insipidus (↓ ADH)
|
|
|
What complications are avoided with gradual, rather than rapid, correction of rehydration of a hypernatremia pt?
|
Cerebral edema – seizures, CNS damage
|
|
|
Determine the Acid-base disorder:
pH 7.30 HCO3 12 pCO2 26 |
Metabolic acidosis, respiratory compensation
|
|
|
Determine the Acid-base disorder
pH 7.25 HCO3 17 pCO2 40 |
Metabolic acidosis
|
|
|
Determine the Acid-base disorder
pH 7.23 HCO3 24 pCO2 55 |
Respiratory acidosis
|
|
|
What is pseudohyponatremia? How is this different from hyponatremia from hyperosmolality?
|
When the serum volume is expanded by a substance such as lipid or protein (ie multiple myeloma) the amt of sodium per volume of serum may decrease even though the amt of sodium per unity of water in serum is appropriate. This is referred to as pseudohyponatremia
This is different than hyponatremia due to hyperosmolality from elevated glucose or mannitol administration. In the case of hyperosmolality, the increase in serum osmols pulls water out of cells thereby diluting serum sodium. Here the plasma sodium level is expected to fall by 1.6 mEq/L for every increase of 100mg/dL of plasma glucose (which increases to 2.4 mEq/L per 100 after glucose levels exceed 400mg/dL). Use this calculation to determine how much you can expect the sodium to rise as the plasma glucose begins to fall with treatment and water is consequently shifted back into cells |
|
|
What volume status would you expect to find in a pt with hyponatremia due to thiazide diuretics
|
hypOvolemic or euvolemic
|
|
|
What volume status would you expect to find in a pt with hyponatremia due to SIADH?
|
Euvolemic
|
|
|
What volume status would you expect to find in a pt with hyponatremia due to Hepatic cirrhosis?
|
Hypervolemic
|
|
|
What volume status would you expect to find in a pt with hyponatremia due to Addison's disease?
|
Hypervolemic + hypertension
|
|
|
What volume status would you expect to find in a pt with hyponatremia due to hypothyroidism?
|
Euvolemic
|
|
|
What volume status would you expect to find in a pt with hyponatremia due to renal failure?
|
Hypervolemic
|
|
|
What volume status would you expect to find in a pt with hyponatremia due to psychogenic polydipsia?
|
euvolemic
|
|
|
What is the differential diagnosis for hypOvolemic hyponatremia based on urine Na+ levels?
|
Urine Na+ <10 mEq/L = Extrarenal losses
GI losses (vomiting, diarrhea, NG tube) Fluid sequestration (peritonitis, pancreatitis) Insensible loss (sweating, extensive burns) Urine Na+ > 20 mEq/L = Renal losses Diuretics (thiazides) Salt-losing renal disease Partial urinary tract obstruction Adrenal insufficiency (inadequate mineralcorticoid, Addison’s) |
|
|
What is the differential diagnosis for hypervolemic hyponatremia based on urine Na+ levels?
|
Low urine Na+ : CHF, cirrhosis, nephrotic syndrome
High urine Na+ : renal failure |
|
|
What condition may result from the rapid correction of hyponatremia? What are the manifestations?
|
Central pontine myelinosis (osmotic demyelination)
Occurs when sodium is corrected by more than 12-20 mEq/L over 24 hrs or is corrected to above 140 Symptoms are irreversible and typically delayed 2-6 days after the correction of hyponatremia Dysarthria, dysphagia Paraparesis or quadriparesis Behavioral disturbances Lethargy and coma Head CT or MRI 4wks after the event reveals areas of demyelination |
|
|
What are the different etiologies of the syndrome of inappropriate antidiuretic hormone (SIADH)?
|
CNS disease: head trauma, brain tumor, stroke, CS infection, pituitary surgery
Pulmonary disease: pneumonia, tumor (small cell) Drugs: NSAIDs, antidepressants, antipsychotics, antineoplastic agents, carbamazepine, ecstasy, vasopressin, DDAVP Other: HIV/AIDs, major abdominal or thoracic surgery |
|
|
What are the serum Na+ and urine osmolality expected to be in diabetes insipidus (DI)?
|
Serum Na+ = high
Urine osmolality = low |
|
|
What should happen to a pt’s urine osmolality with nephrogenic DI after ADH administation?
|
Urine osmolality will remain decreased
|
|
|
How do you correct central DI?
|
Desmopressin (DDAVP)
|
|
|
What is the treatment for nephrogenic DI?
|
Salt restriction, ↑ water intake
Thiazide diuretic +/- Indomethacin In cases of Lithium toxicity → thiazide + amiloride Tx underlying condition |
|
|
Though hyponatremia is defined as a serum Na+ of <135, at what serum Na+ does a pt get into trouble and risk seizure?
|
Serum Na+ <120
|
|
|
What is the consequence of correcting hyponatremia too rapidly? How rapidly can it safely be corrected?
|
Central pontine myelinolysis
Keep below 12-20 mEq/day |
|
|
How will a large infusion of IV mannitol likely affect the serum Na+ ?
|
Decrease serum Na+
|
|
|
Explain how hyponatremia develops despite serum hyperosmolality (>295 Osm/kg)?
|
Another solute pulls H2O out of cells & dilutes the serum sodium
|
|
|
How are sodium levels corrected for high glucose?
|
Add 1.6 mEq to the Na+ value for ever 100mg/dL of glucose above normal
Add 2.4 mEq for every 100mg/dL glucose above 400mg/dL |
|
|
What are some causes of Hyperkalemia? (K+ shift OUT of cells)?
|
Low insulin
β-blockers acidosis Digoxin Cell lysis (ie leukemia) |
|
|
What are some causes of HypOkalemia? (K+ shifts into cells)
|
Insulin
β-agonists alkalosis cell creation/ proliferation |
|
|
What is the emergency treatment for hyperkalemia?
|
STAT EKG to identify any EKG changes such as peaked T waves
Repeat K+ level to insure no lab errors/ lysis D50 1 amp IV followed immediately by 10 units regular insulin IV (drives K+ into cells → 4-6 hr effect) Calcium-gluconate 1-2 amps (or CaCl 1 amp) to protect myocardium NaHCO3 50mEq IV over 5 min (drive K+ into cells in exchange for H+ ) Albuterol nebulizer (page RT stat if needed) (drives K+ into cells) Kayexalate 30g PO4-/PR (exchanges Na+ for K+ in the gut → excretion of K+ → 24 hr effect) Repeat K+ in 30 min Consider Lasix 40-80 mg IV to increase K+ wasting in urine. May also use dialysis Replace magnesium if it is less than 2.0 Determine the cause of hyperkalemia and treat |
|
|
Which lung cancer is highly associated with SIADH as a paraneoplastic syndrome?
|
Small cell lung cancer
|
|
|
What is the first agent you should give a pt with hyperkalemia and EKG changes?
|
Calcium gluconate or calcium chloride
|
|
|
After having given the calcium gluconate (or calcium chloride) what are the other treatments needed in the hyperkalemic pt?
|
Amp of D50
Bolus of 10 units regular insulin NaHCO3 infusion Albuterol nebulizer Kayexalate Loop Diuretics Magnesium Dialysis |
|
|
What are the two eponym signs of hypOCalcemia?
|
Chvostek’s sign: tap the cheek, facial nerve spasm “Chvostek Cheek”
Trousseau’s sign: carpal spasm when BP cuff is inflated “Trousseau’s, Tighten” |
|
|
Which diuretics lose calcium? Which spare it?
|
“Loops lose Ca2+ Thiazides don’t”
|
|
|
What electrolyte abnormality is associated with peaked T waves on EKG
|
hyperkalemia
|
|
|
What electrolyte abnormality is associated with flattened T waves on EKG
|
hypokalemia
|
|
|
What electrolyte abnormality is associated with U waves on EKG
|
hypokalemia
|
|
|
What electrolyte abnormality is associated with QT prolongation
|
hypocalcemia
|
|
|
What electrolyte abnormality is associated with QT shortening
|
hypercalcemia
|
|
|
How are total Ca2+ levels corrected for low albumin?
|
Add 0.8mg/dL Ca2+ for each 1g/dL Albumin <4
|
|
|
HYQ: hyponatremia + low serum osmolality + high urine osmolality:
|
SIADH
|
|
|
HYQ: what is the next step in the management of a pt with peaked T waves on EKG due to hyperkalemia?
|
Calcium Gluconate
|
|
|
HYQ: What is the most common cause of death in dialysis pts?
|
Cardiovascular Disease
|
|
|
What are the distinguishing characteristics of each type of renal tubular acidosis (RTA)?
|
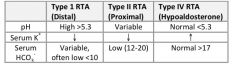
see above
|
|
|
What is the consequence of correcting HYPERnatremia too rapidly? How rapidly can it safely be corrected?
|
Cerebral edema
No more than 12-20 mEq/day |
|
|
What is the consequence of correcting hypOnatremia too rapidly? How rapidly can it safely be corrected?
|
Central pontine myelinosis
No more than 12-20 mEq/day |
|
|
What medications can be used to rapidly correct hyperkalemia by shifting potassium into cells?
|
NaHCO3, Albuterol nebs, Insulin (with glucose)
|
|
|
What are the causes of euvolemic hypOnatremia?
|
SIADH, hypothyroidism, polydipsia
|
|
|
What medications are known for causing hyperkaemia? Hypokalemia?
|
Hyperkalemia: ACEI/ARBs, K+ sparing diuretics, β-blockers, Digoxin
Hypokalemia: Albuterol, Insulin, Loops, thiazides, carbonic anhydrase inhibitors |
|
|
What are the causes of a normal anion gap metabolic acidosis?
|
Diarrhea, RTA, hyperalimentation
|
|
|
What medications are necessary in pts with end stage renal dz?
|
Statin
Vit D Iron EPO Phosphate binder Aspirin ACEI/ARB Loop Diuretic |
|
|
What is the treatment for nephrogenic diabetes insipidus?
|
HCTZ +/- Indomethacin
If Lithium toxicity → Thiazide + amiloride |
|
|
How is benign prostatic hyperplasia (BPH) diagnosed?
|
Clinical diagnosis based on symptomatic scoring system
R/O other pathologies that may cause similar symptoms using history and the following tests: ● Digital rectal exam – to detect malignancy ● Urinalysis – to detect hematuria indicating infection, calculi, or prostatitis ● Serum Creatinine – to detect possible renal or prerenal disease Other useful but optional tests: serum PSA, postvoid residual, maximum urinary flow rate |
|
|
What is the treatment for benign prostatic hyperplasia (BPH)?
(long DIT answer) |
Alternative Medicine
- Isoflavones as found in soy decrease the growth of hyperplastic prostate tissue in histoculture. Trinovin at 40-80mg/d may help relieve symptoms - Saw palmetto is as effective as finasteride (Proscar) (Urology 2001;58;71-6), has fewer SE and decreases prostate size without changing PSA values (JAMA 1998;280:1604-9) Medical intervention - Nonselective α-blockers: Doxacin (Cardura), Prazosin (minipress), Terazosin (Hytrin) MOA: ↓ prostate smooth muscle tone → immediate improvement in urine flow SE: dizziness, postural hypOtenstion, fatigue, asthenia. To reduce SE, dose qHS and titrate dose upward slowly over time (weekly) -5α-reductase inhibitors: FInasteride (Proscar), Dutasteride (Avodart) MOA: slowly reduces dihydrotesterone levels → 20% decrease in prostate volume over 3-6mos Surgical Intervention - Indications for surgery: failure of medical therapy, refractory urinary retention, inability to express urine without a catheter, recurrent infection, persistent hematuria, bladder stones, or renal insufficiency - TURP: transurethral resection of the prostate. Most common surgery for BPH. Symptomatic improvement in 88%. SE include excessive bleeding (1%) retrograde ejaculation (70%), impotence (14%), partial incontinence (6%), total incontinence (1%) - Open prostatectomy: symptomatic improvement in 98% but is invasive and assow with more morbidity than TURP. Usually reserved for those with extremely large prostate or structural problems (protrusion into bladder, large bladder stone, urethral diverticulum) - Other interventions: transurethral incision of the prostate (TUIP), transurethral microwave thermotherapy (TUMT), transurethral vaporization of the prostate (TUVP), transurethral electrovaporization of the prostate (TVP), transurethral needle ablation of prostate (TUNA) |
|
|
What is the next step in management of a 65yo M that presents to the ER with inability to urinate and painful bladder distention?
|
Decompression of bladder with 14-18 French Foley catheter (may downsize to 10-12 French if necessary)
If h/o BPH, may require a cath with a firm Coude tip to “power-through” the narrowed urethra Is unable to pass urethral cath, then suprapubic cystostomy (usually under US guidance) If unable to pass urethral cath and no one trained in suprapubic cath placement will be available for hours, then aspirate the bladder with a spinal needle |
|
|
What are the common antibiotics use to treat uncomplicated cystitis?
|
(1) TMP-SMX (Bactrim)
(2) Fluoroquinolones: Ciprofloxacin (Cipro), Levofloxacin (Levaquin), Moxifloxacin (Avelox) (3) Amoxicillin (4) Cephalexin (Keflex, 1st Gen Ceph) |
|
|
What are the risk factors for developing bladder cancer?
|
Tobacco smoking
Shistosomiasis Alanine dye Cyclophosphamide (Cytoxan) Recurrent UTI Petroleum byproducts Male sex |
|
|
What is the primary lab screen for bladder cancer?
|
Hematuria on urinalysis
|
|
|
What is the primary study done to confirm the diagnosis of bladder cancer?
|
Cystoscopy with biopsy
|
|
|
What are the treatment options for urethritis?
|
Ceftriaxone (Rocephin, 3rd Gen) + doxycycline or azithromycin
Be sure to also treat partners |
|
|
What are classic s/s of benign prostatic hyperplasia (BPH)?
|
Urinary hesitancy
Frequency Nocturia Urgency Weak stream |
|
|
Name the 2 classes of medications used to treat BPH:
|
Nonselective α-1 receptor blockers: Doxacin (Cardura), Prazosin (minipress), Terazosin (Hytrin)
↓ prostate smooth muscle tone → immediate improvement in urine flow SE: dizziness, postural hypOtenstion, fatigue, asthenia 5-α reductase inhibitors: FInasteride (Proscar), Dutasteride (Avodart) saw palmetto |
|
|
A 60yo M presents to the clinic for a Well-Male Exam and on digital examination a hard nodule is palpated on the prostate. Lab workup shows an ↑ PSA. What is the next step in the management of this patient?
|
Transrectal US-guided prostate biopsies
(think: Prostate Cancer) |
|
|
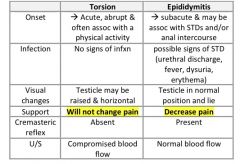
How can testicular torsion be differentiated from epididymitis?
|
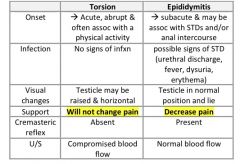
see above
|
|
|
Treatment of Testicular Torsion vs Epididymitis?
|
Tx of Torsion: surgical detorsion with bilateral orchiopexy within 6hrs
Tx of Epididymitis: depends on age: Age <35 yrs : most likely GC/Chlamydia ➔ Ceftriaxone IM (Rocephin, 3rd Gen) then doxycycline x10days Age >35 yrs or h/o anal intercourse = Enterobacteriaceae ➔ Fluoroquinolone x10-14 days [Ciprofloxacin (Cipro), Levofloxacin (Levaquin), Moxifloxacin (Avelox) ] |
|
|
What drugs are commonly used to treat testicular cancer?
|
“Eradicate Ball Cancer”
Etoposide Bleomycin Cisplatin |
|
|
In a pt suspected of having prostate cancer, what might an elevated alkaline phosphatase indicated?
|
Prostatic metastasis to bone
|
|
|
What are 2 common side effects of radical prostatectomy?
|
incontinence
impotence |
|
|
A sexually-active homosexual man arrives at the ER because of sudden severe testicular pain that occurred while he was playing soccer 30min ago. Before that time, he had no dysuria or increased frequency of urination or testicular pain. What is the likely diagnosis?
|
Testicular torsion
|
|
|
What is the next step in the management of testicular torsion confirmed with U/S?
|
Manual detorsion then surgery
|
|
|
What is the most common germ cell tumor (GCT) of the testis?
|
Seminoma
|
|
|
What are the characteristic features of a varicocele?
|
What it is: Dilation of pampiniform plexus in scrotum (“testicular mass”)
S/S: Dull aching scrotal pain usually on the left (left-sided varicoceles are 10 times more common than right-sided) Note: Right-sided varicocele may point to a renal cell carcinoma (the tumor is compressing the IVC or gonadal vein causing the variocele) Testicular atrophy on the affected side Infertility is common – varicoceles are present in 25% of infertile men vs only 11% of fertile men Dx: Color Doppler U/S shows retrograde flow to the scrotum |
|
|
Undescended testes put a pt at higher risk for what?
|
Testicular cancer
|
|
|
WTQ: 18yo M comes to the office c/o dull aching & fullness of the scrotum. Exam shows soft left-sided srotal swelling; transillumination testing is negative. The scrotal swelling increases when the patient performs the Valsalva maneuver. The PE is otherwise unremarkable. What is the most likely cause of his condition?
|
cause: dilation of the pampiniform plexus
Dx: Varicocele notes: pts with varicocele classically present c/o dull, aching pain in the testis. Varicocele is most common on the left side. If results from a swelling of the pampiniform plexus of veins and feels like a "bag of worms" on exam |
|
|
What medications are known for causing erectile dysfunction?
|
Most antidepressants esp SSRIs
Spironolactone Sympathetic blockers: clonidine, guanethidine, methyldopa Thiazide diuretics, β-blockers Ketoconazole Cimetidine (but NOT ranitidine or famotidine) Antipsychotics |
|
|
What are the treatments for a pt with erectile dysfunction (ED)?
|
First line = Phosphodiesterase inhibitors:
Sildenafil (Viagra) Vardenafil (Levitra) Tadalafil (Cialis) Second line= Penile self-injectable drugs: Papaverine, phentolamine, alprostadil, Vacuum & constriction devices Third line: penile prothesis implantation Other: Androgen replacement if hypogonadism |
|
|
What is the classic presentation of the most common renal tumor in children?
|
Mc renal tumor in kids → Wilm’s Tumor
Presentation: Most common age: 2-4 yrs Palpable flank mass (most common presenting symptom) Abdominal pain (30%) Hematuria (12-25%) Hypertension (25%) Possible multiple other assoc congenital anomalies including WAGR syndrome Wilm’s tumor Aniridia GU abnormalities Retardation (mental) |
|
|
At what age should nocturnal enuresis be treated? What are the treatment options?
|
Enuresis cannot be diagnosed until 5yrs of age (chronological and developmental)
Treatment is usually delayed until the child is at least 7yrs First line → behavioral interventions Start toilet training if not yet attempted Motivational therapy (ie star charts) Restrict fluids before bed (with a compensatory increase in daytime fluids) Nighttime chaperone to the toilet or scheduled wakening to void using alarm clock Enuresis alarm (pad with alarm device) in bed for classic conditioning. This is most effective long-term therapy Second-line → Pharmacologic interventions High likelihood of recurrence upon discontinuation Imipramine (tofranil) for short-term (up to 6wks) Desmopressin (DDAVP) orally (FDA 2007: intranasal desmopressin is no longer indicated for enuresis due to risk of hyponatremic seizures) Indomethacin suppository Posterior Urethral Valves Most common obstructive urethral lesion in infants and newborns Abnormal tissue folds in the distal prostatic urethra → thick-walled bladder and weak urinary stream and obstruction (bilateral hydronephrosis, megaureter, UTI) Diagnosed with a voiding cystourethrogram Definitive care → transurethral ablation of the abnormal tissue or urinary diversion (vesicostomy) |
|
|
In a pt with a varicocele, what is the scrotal mass made of?
|
Dilation of pampiniform plexus
|
|
|
What is the most common physical exam finding/ presenting symptom of a child with Wilm’s tumor?
|
Palpable flank mass
|
|
|
At what age would a normal child have to be before diagnosis of a nocturnal enuresis could be made?
|
5 years of age
|
|
|
A 4yo M is dx with a UTI. What study should be performed?
|
VCUG
|
|
|
What are the recommended therapies for nocturnal enuresis?
|
Enuresis alarm
Imipramine (Tofranil) < 6wks |
|
|
What is the classic presentation of a varicocele?
|
Scrotal mass that transilluminates
Infertility Scrotal pain Testicular atrophy |
|
|
3yo with am abdominal mass + hematura + HTN. What is the most likely diagnosis?
|
Wilm’s tumor
|
|
|
HYQ: A pt has signs of peritonitis and his clinical scenario favors rupture of the bladder (blunt trauma to fully distended bladder). What portion of the bladder must have been injured to allow for a chemical peritonitis to have developed?
|
Dome of the bladder (only part of bladder covered by peritoneum)
|
|
|
HYQ: What is the next step in the management of a woman with an uncomplicated cystitis?
|
Treat empirically
|
|
|
HYQ: Newborn males has a distended palpable bladder and oliguria. What is the most common cause of congenital urethral obstruction?
|
Posterior urethral valves
|
|
|
What is the treatment for epididymitis?
|
Age <35 yrs : most likely GC/Chlamydia
Ceftriaxone IM (Rocephin, 3rd Gen) then doxycycline x10days Age >35 yrs or h/o anal intercourse = Enterobacteriaceae Fluoroquinolone x10-14 days Ciprofloxacin (Cipro) Levofloxacin (Levaquin) Moxifloxacin (Avelox) |
|
|
What is the treatment for prostatitis?
|
Age <35 yrs : most likely GC/Chlamydia
Ceftriaxone IM (Rocephin, 3rd Gen) then doxycycline x10days Age >35 yrs or h/o anal intercourse = Enterobacteriaceae Fluoroquinolone x 4-6 weeks The key is to realize for prostatitis (not epididymitis), need to tx with fluoroquinolone for 2 months if >35yrs |
|
|
What labwork is included in the work-up for erectile dysfunction?
|
Total testosterone
Prolactin level TSH +/- PSA |
|
|
What is the treatment for urethritis in men?
|
Ceftriaxone IM (Rocephin, 3rd Gen) then doxycycline x10days
|
|
|
How doe the signs and symptoms of testicular torsion differ from epidiymitis?
|
see above
|
|
|
What is the defining characteristic of a hydrocele?
|
transillumination
|
|
|
WTQ: A newborn infant is found to have a scrotal mass. The mass is cystic & transilluminated with light. He is born without any other complications. The vital signs are wnl. Other physical examination is unremarkable. What is the most appropriate next step in management?
|
next step: reassurace & observation
dx: Hydrocele - a fluid collection within the processus or tunica vaginalis - the peritoneal projection that accompanies the testis during its descent into the scrotum when the processus vaginalis fails to obliterate, peritoneal fluid may accumulate within the processus vaginalis causing a communicating hydrocele - it will transilluminate most hydroceles will resolve spontaneously by age of 12mos if it doesn't resolve, then it should be removed surgically due to risk of inguinal hernia |