Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
79 Cards in this Set
- Front
- Back
|
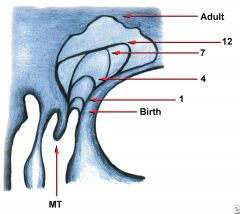
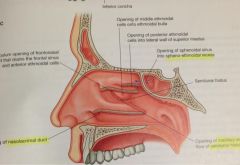
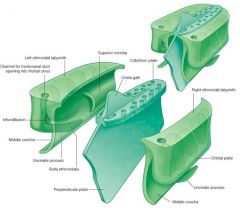
Embryology of the Paranasal Sinuses
Classic anatomic studies attribute paranasal sinus development to lateral wall ridges called _______________ |
ethmoidturbinals - these are medial extensions
from the lateral wall of the nasal capsule at approximately the 8th week 6-7 folds initially emerge but only 3-4 persist |
|
|
Embryology of the Paranasal Sinuses
What does the first ethmoturbinal form? |
Regresses during development
- ascending portion forms the agger nasi - descending portion forms the uncinate process |
|
|
Embryology of the Paranasal Sinuses
What does the second ethmoturbinal form? |
middle turbinate
|
|
|
Embryology of the Paranasal Sinuses
What does the third ethmoturbinal form? |
superior turbinate
|
|
|
Embryology of the Paranasal Sinuses
What do the fourth and fifth ethmoturbinal form? |
supreme turbinate (when present)
|
|
|
Embryology of the Paranasal Sinuses
All of the structures derive from the ethmoturbinals are considered to be _____________ in origin. |
ethmoid
|
|
|
Embryology of the Paranasal Sinuses
An additional ridge, the _______________, arises inferior to the other structures and ultimately forms the inferior turbinate. |
maxilloturbinal
|
|
|
Embryology of the Paranasal Sinuses
What does the first furrow develop into? |
Located between the first and second ethmoturbinals
Descending aspect forms the ethmoidal infundibulum, hiatus semilunaris, and middle meatus (the primordial maxillary sinus develops from the inferior aspect of the ethmoid infundibulum) Ascending aspect can contribute to the frontal recess |
|
|
Embryology of the Paranasal Sinuses
What does the second furrow develop into? |
Located between the 2nd and 3rd ethmoturbinals
Forms the superior meatus |
|
|
Embryology of the Paranasal Sinuses
What does the third furrow develop into? |
Located between the 3rd and 4th ethmoturbinals
Forms the supreme meatus (when present) |
|
|
Embryology of the Paranasal Sinuses
How does the frontal sinus develop? |
From anterior pneumatization of the frontal recess into the frontal bone.
A series of one to four folds & furrows arise within the ventral and caudal aspect of the middle meatus. 1) the first frontal furrow forms the agger nasi cell 2) the second frontal furrow forms frontal sinus (usually) 3) the third and fourth furrows form other anterior ethmoid cells |
|
|
Embryology of the Paranasal Sinuses
Sphenoid Sinus development During the 3rd month the nasal mucosa invaginates into the posterior portion of the cartilaginous nasal capsule to form a pouch-like cavity referred to as the ________________________________ recess of the nasal cavity. The wall surrounding this cartilage is ossified in the later months of fetal development and the complex is referred to as the _________________________. |
cartilaginous cupolar recess
ossiculum Bertini |
|
|
Embryology of the Paranasal Sinuses
Sphenoid sinus pneumatization is typically completed between the ___ and ___ year of life. |
9th and 12th
|
|
|
Anatomy
Ethmoid Lamella What is the first lamella? Second? Third? Fourth? |
First lamella - uncinate process
Second lamella - ethmoid bulla Third lamella - basal or ground lamella of the middle turbinate Fourth lamella - superior turbinate "UEMS" |
|
|
Anatomy
Ethmoid Lamella What structure divides the anterior and posterior ethmoids? |
the basal lamella of the middle turbinate
|
|
|
Anatomy
The frontal, maxillary, and anterior ethmoids drain into the _____________________ |
middle meatus (they all arise from the region of the anterior ethmoid
|
|
|
Anatomy
The posterior ethmoid cells drain into _____________ |
the superior and supreme meati
(they lie posterior to the basal lamella) |
|
|
Anatomy
The sphenoid sinus drains into the _____________________ |
sphenoethmoid recess
|
|
|
Anatomy
Describe the location of the Agger Nasi cells |
‘Little Mound’
Most anterior ethmoid air cell Part of 1st ethmoturbinal Defines ant. boarder of frontal recess |
|
|
Anatomy
What are the following borders of the Agger Nasi cells? Anteriorly: Superiorly: Anterolaterally: Inferolaterally: Inferomedially: |
Anteriorly: frontal process of the maxilla
Superiorly: frontal recess or sinus Anterolaterally: nasal bones Inferolaterally: lacrimal bone Inferomedially: uncinate process of the ethmoid bone |
|
|
Anatomy
What are the typical dimensions of the uncinate process? |
~ 3-4mm wide and 1.5-2cm long; nearly sagittally oriented
|
|
|
Anatomy
The uncinate process forms the medial wall of the _________________________ |
ethmoidal infundibulum
|
|
|
Anatomy
What are the anterior attachments of the uncinate process? |
Anteriorly and superiorly attaches to the ethmoidal crest of the maxilla.
Immediately below this, it fuses with the posterior aspect of the lacrimal bone. The anterior inferior aspect does not have this bony attachment. |
|
|
Anatomy
What are the posterior attachments of the uncinate process? |
Posteriorly and inferiorly the uncinate attaches to the ethmoidal process of the inferior turbinate bone
At its posterior limit it gives off a small bony projection to atttach to the lamina perpendicularis of the palatine bone |
|
|
Anatomy
What are the three possible attachments of the superior aspect of the uncinate? |
1) On the lamina papyracea - most common ~ 88%
2) Skull base centrally /ethmoid roof ~ 6% 3) Skull base medially / middle turbinate ~ 6% |
|
|
Anatomy
Describe the anterior and posterior nasal fontanelles |
Nasal fontanelles lie anterior (Fa) and posterior (Fp) to the inferior aspect of the uncinate, where the lateral nasal wall consists only of mucosa
The posterior fontanelle is much larger and more distinct than its anterior counterpart. The fontanelles (especially posterior) may be perforated creating an accessory ostium into the maxillary sinus (20-25% of pts). These accessory ostia may be indicators of prior sinus dz |
|
|
Anatomy
Describe the ethmoid bulla |
Most consistent, largest and well pneumatized anterior ethmoid air cell
Located within the middle meatus directly posterior to the uncinate process and anterior to the basal lamella of the middle turbinate |
|
|
Anatomy
The anterior wall of the ethmoid bulla usually forms the posterior border of what? |
the frontal recess (only if the anterior wall of the ethmoid bulla extends to the skull)
A suprabullar recess will form if it does not extend to the skull |
|
|
Anatomy
Posteriorly, the bulla may blend with the basal lamella or have a space between it and the basal lamella of the middle turbinate, called ________________________ |
retrobullar recess
|
|
|
Anatomy
Describe the hiatus semilunaris? |
Is a crescent-shaped gap between the posterior free margin of the uncinate process and the anterior wall of the ethmoid bulla
Through this sagittaly oriented cleft or passageway the middle meatus communicates with the ethmoid infundibulum |
|
|
Anatomy
Describe the ethmoidal infundibulum |

Funnel-shaped passage through which secretions are transported or channeled into the middle meatus from various anterior ethmoid cells and the maxillary sinus
Depending upon the anatomy of the frontal recess, the frontal sinus can also drain through the infundibulum |
|
|
Anatomy
What are the following borders of the ethmoidal infundibulum? Medial: Lateral: Posterior: Anterior and superior: Superior and lateral: |

Medial: uncinate process
Lateral: lamina orbitalis Posterior: anterior wall of ethmoid bulla Anterior and superior: frontal process of the maxilla Superior and lateral: lacrimal bone |
|
|
Anatomy
The ethmoidal infundibulum communicates with the middle meatus through the ____________ |
hiatus semilunaris
|
|
|
Anatomy
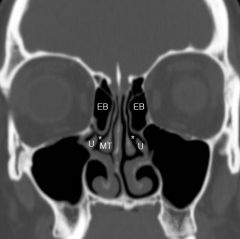
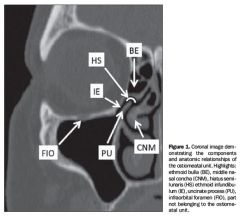
What are the structures in the ostiomeatal unit? |
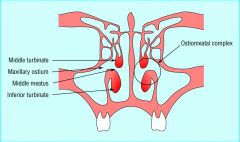
Functional concept, not anatomic structure
middle meatus uncinate process middle turbinate ethmoid infundibulum anterior ethmoid cells ostia of the anterior ethmoid, maxillary and frontal sinuses |
|
|
Anatomy
What are the following boundaries of the frontal recess? Lateral: Medial: Anterior: Posterior: |
Lateral: lamina papyracea
Medial: - middle turbinate Anterior: the posterior superior wall of the agger nasi cell (when present) Posterior: anterior wall of the ethmoid bulla |
|
|
Anatomy
Where is the anterior attachment of the middle turbinate? |
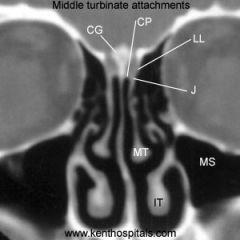
In its anterior aspct, the middle turb attaches laterally at the agger nasi region, specificallly at the crista ethmoidalis of the maxilla.
|
|
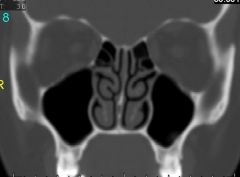
Anatomy
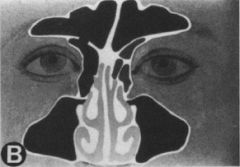
Which middle turb variant is seen here? |
paradoxically curved right turb
|
|
Anatomy
What is the name of a cell formed within the vertical portion of the middle turb? |
If the vertical portion, or lamella of the middle turb is pneumatized, the cell that is formed is referred to as the intralamellar cell
|
|
|
Anatomy
Typically, the ethmoid roof slopes __________ and __________, and is thinner _________ than __________ (by a factor of 10) |
Typically, the ethmoid roof slopes inferiorly and medially, and is thinner medially than laterally (by a factor of 10)
|
|
|
Anatomy
What are the following Keros classifications based on measurements? |
Keros classifications is a method of classifying the depth of the olfactory mucosa. Medially, the roof is formed by the lateral lamella of the cribriform.
Three types of formation of the ethmoid roof based upon the vertical height of the lateral lamella. Type 1 : has a depth of 1 - 3 mm Type 2 : has a depth of 4 - 7mm (most common type) Type 3 : has a depth of 8 - 16mm (rare) |
|
|
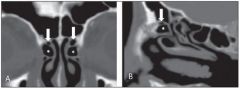
Anatomy
Describe Onodi cells |

Sphenoethmoidal Cells = Onodi cells
Increased pneumatization of the sphenoid sinus that can expose the optic nerve and the internal carotid artery at put them at risk during surgery |
|
|
Anatomy
Lateral to the sphenoid sinus lie which structures? |

carotid artery
optic nerve cavernous sinus 3rd, 4th, 5th and 6th CN |
|
|
Anatomy
Posterior and superior to the sphenoid sinus lie which structures? |
sella turcica
superior intercavernous sinus planum sphenoidale (forms the roof of the sphenoid sinus) |
|
|
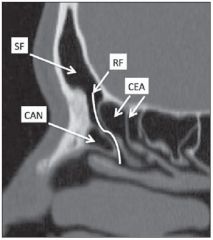
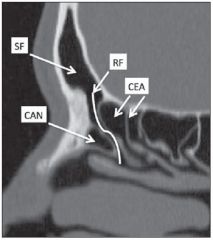
Anatomy
In a well-pneumatized sphenoid, the _______________ is often identified inferiorly and laterally within the sinus |

Vidian Canal (pterygoid canal) - transmits the vidian artery, vein, and nerve
|
|
|
Anatomy
What is the rate of dehiscence of the carotid and optic canals within the sphenoid sinus? |
Carotid canal - up to 22%
Optic canal - up to 6% |
|
|
Anatomy
In some cases, pneumatization of the posterosuperior lateral wall of the sphenoid extends between the optic nerve and carotid artery. What does this create? |
opticocarotid recess (OCR)
|
|
|
What is the histological difference between acute and chronic rhinosinusitis?
|
acute rhinosinusitis is an exudative process characterized by neutrophilic inflammation and necrosis; almost always infectious in etiology
chronic rhinosinusitis is a proliferative process that is more often characterized by thickened mucosa and lamina propria |
|
|
What is the predominant cell type found in chronic rhinosinusitis?
|
Most CRS has an inflammatory response where eosinophils are the predominant inflammatory cells in both atopic and nonatopic individuals with CRS
|
|
|
What are the environmental theories of chronic rhinosinusitis?
|
Progression of acute rhinosinusitis
Biofilms IgE independent fungal inflammation Bacterial superantigen |
|
|
Anatomy
What are Haller cells? |

AKA infraorbital ehtmoid air cells or maxilloethmoidal cells.
Present in ~20% (range 2-45%) |
|
|
Anatomy
Describe the different types of frontal cells |

Type I - Single cell above the agger nasi
Type II - Two or more cells above the agger cell Type III - Single cell extending from the agger cell into the frontal sinus Type IV - Isolated cell within the frontal sinus |
|
|
What are the various layers of the mucociliary blanket?
|

Gel layer is the top layer of the mucociliary blanket. It traps allergens, bacteria and pollutants.
Sol layer is the next layer of the mucociliary blanket, and enables rapid elimination of viscous secretions Both layers may be severely affected in pt's with cycstic fibrosis |
|
|
What is the most common type of fungal sinus dz?
|
Allergic fungal rhinosinusitis
|
|
|
What are the five classic criteria for allergic fungal rhinosinusitis?
|
1) Type I hypersensitivity
2) Nasal polyposis 3) Characteristic CT appearance (hyperdense material in the sinus cavity) 4) Positive fungal stain or culture 5) Presence of thick, eosinophilic mucin |
|
|
What is the typical appearance of eosinophilic mucin?
|

Typically thick, tenacious, "peanut butter"-like, brown-green mucus that contains sheets of eosinophils, Charcot-Leyden crystals, and fungal hyphae
|
|
|
What is Samter's triad?
|
Triad of:
1) Nasal polyps 2) Asthma 3) Aspirin sensitivity |
|
|
What is the pathogenesis of aspirin sensitivity in the development of CRS?
|
oversynthesis of leukotrienes
ASA & other NSAID's inhibit cyclooxygenase and decrease prostaglandin E2, resulting in a net increase in leukotrienes due to uninhibited production. Leukotrienes are also known as the slow reacting substances of anaphylaxis, and are a class of inflammatory mediators that increase vascular permeability, inflammatory cell chemotaxis and smooth muscle constriction. |
|
|
On histology, most CRS stimulates the Th1 or Th2-type inflammatory response?
|
Th2-type inflammatory response seen in asthmatics where eosinophils are the predominant inflammatory cells in both atopic and nonatopic individuals
Thus, asthma and CRS are intimately related in many individuals even in the absence of aspirin sensitivity |
|
|
Summarize the 'immune barrier hypothesis' of chronic sinusitis
|
The interface between the nasal mucosa and the external environment contains both a mechanical and innate immune protective barrier that helps maintain the integrity and function of the respiratory epithelium.
Defects in these protective mechanisms can allow antigen passage and processing which can lead to the chronic inflammation seen in chronic sinusitis. This theory places chronic sinusitis in the same framework seen in other chronic mucosal inflammatory dz's (IBD, reactive airway dz, etc). |
|
|
What are the patient selection general guidelines for sinus surgery?
|
a) pt should have had a trial of maximal medical therapy
b) CT should be performed at least 4 weeks following the onset of medical therapy for the most recent episode of rhinosinusitis and at least 2 weeks following the most recent URI c) there should be persistent evidence of mucosal dz (radiographic or endoscopic) d) nasal congestion or obstruction, discolored nasal discharge, decreased olfaction, and nasal or sinus fullness are generally good signs of CRS e) Headache correlates poorly with sinus dz and severe pain is unusual in CRS f) performing elective sinus surgery on patients who continue to smoke may result in increased scarring and worsening of sx |
|
|
What are the 3 general passes, in order, performed during a diagnostic nasal endoscopy?
|
1) First pass - along the floor of the nose
2) Second pass - between the middle and inferior turbinates 3) Third pass - done while the telescope is being withdrawn. The middle meatus, including the bulla ethmoidalis, hiatus semilunaris and infundibular enterance are inspected. |
|
|
What can you give pt's to reduce polyp size prior to surgery?
|
As long as there are no contraindications, may give prednisone 20-40mg/d for 2-6 days
|
|
|
Regardless of the reason for sinus surgery, all pt's should have at least a coronal CT with __-mm cuts.
|
3 mm
|
|
|
What are the key points in reviewing the CT scan prior to sinus surgery?
|
1) Shape slope and thickness of skull base
2) Shape and dehiscence of medial orbital wall 3) Vertical height of the posterior ethmoid (in relation to the posteromedial roof of the maxillary sinus) 4) Location of the anterior ethmoid artery 5) Presence of sphenoethmoidal (Onodi) cell 6) Position of intrasinus sphenoid septae (in relation to carotid artery) 7) Presence of maxillary sinus hypoplasia or infundibular atelectasis 8) Conceptualization of the frontal sinus drainage pathway from the use of multiplanar CT |
|
|
In sinus surgery what are the 4 areas injected with xylocaine & epi?
|
Anterior to the attachment of the middle turb
Anterior to the inferior portion of the uncinate process Inferior aspect of middle turb Mid point of the root of the inferior turbinate |
|
|
What will be removed in a Draf type I procedure?
|
Removal of frontal recess obstruction by:
- anterior ethmoidectomy without touching the frontal sinus outflow tract (complete removal of the anterior ethmoid cells and the uncinate process up to the frontal sinus ostium, including the removal of any frontal cells or other obstructing structures to assure the patency of the frontal sinus ostium) |
|
|
What will be removed in a Draf type II procedure?
|

This is performed if Draf type I was unsuccessful and further resection is necessary.
Draf type I + Removal of frontal sinus floor lateral to the middle turbinate. Removal of ethmoidal cells protruding into the frontal sinus ("uncapping the egg") creating an opening between the middle turbinate medially and the lamina papyrecea laterally. |
|
|
What is the difference between Draf type IIA & IIB?
|
Draf IIA - frontal sinus is opened between the lamina papyracea and the insertion of the middle turb
Draf IIB - frontal sinus is opened medial to the middle turb by removal of the most anterior attachment of the middle turb to the skull base. Best reserved for revision procedures. |
|
|
What will be removed in a Draf type III procedure?
|

AKA trans-septal frontal sinusotomy or modified endoscopic Lothrop procedure.
Removal of the floor of both frontal sinuses, the upper part of the nasal septum, and the lower part of the intersinus septum. Has a failure rate of almost 14%, so must be performed only by experienced surgeons. |
|
|
What are the three main types of balloon catheter devices used in balloon catheter sinus surgery?
|
1) Transnasal guide wire
2) Transnasal malleable suction-based device 3) Transantral |
|
|
Transantral balloon devices only treat which sinus?
|
maxillary sinus, using the canine fossa puncture technique
|
|
|
During endoscopic sinus surgery if an
orbital hematoma is suspected and a sudden dramatic onset of progressive proptosis occurs, a"compartment syndrome" quickly results. To decrease the pressure within the orbit, initially perform what? |
canthotomy and cantholysis and then follow with orbital decompression and ophtho consult
|
|
|
What is the recommendation for postop CSF rhinorrhea?
|
early repair is recommended.
|
|
|
What is the risk of meningitis in pt's with CSF leaks who are managed conservatively?
|
29% incidence of meningitis with long-term follow-up of CSF leaks managed conservatively
|
|
|
Which nasal site is the most common site for persistent disease following surgery?
|
frontal recess
|
|
|
Which various positions increase the dosage of steroid that is delivered to the frontal recess?
|
Moffat's head-down kneeling position
Mygind's position (supine and head extened) Lying on the side head-down (LSHD) position |
|
|
Adding which medicine to nasal saline irrigations reduces edema and may eliminate the necessity for oral steroids?
|
budesonide (0.5mg)
|
|
|
In the case of CSF leak repair, when is the packing typically removed?
|
5-7 days
|
|
|
Which symptom appears to be the most sensitive indicator of persistent or recurrent disease following endoscopic sinus surgery?
|
olfaction
|