![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
74 Cards in this Set
- Front
- Back
|
Categorise oxygen delivery devices |
1. invasive - ETT 2. Non-invasive - fixed performance - variable performance --> performance vary with FGF and inspiratory flow rate |
|
|
Fixed performance device |
FGF > peak inspiratory flow --> constant FiO2 Require high gas flow --> dry mucous membrane e.g. venturi mask |
|
|
Bernoulli principle |
gas forced thru stricture increases gas flow velocity (fall in potential energy (pressure) --> increased kinetic energy (velocity) ) |
|
|
variable performance devices |
e.g. NP, HM, non-rebreather mask |
|
|
Nasal prongs |
oxygen reservoir = nasopharynx max FiO2 44% at 6L/min degree of O2 enrichment depend on: - oxygen flow rate - peak inspiratory flow rate - minute ventilation - nasal vs oral breathing - expiration more important (nasal expiration --> clear reservoir) |
|
|
Non-rebreather mask |
- 2L reservoir bag - One way valve - force inspiration from reservoir, prevent air entrapment - FiO2 60-90% |
|
|
what does the size of an ETT measure |
internal diameter |
|
|
ideal ETT cuff pressure |
25-30cmH2O |
|
|
at what position is the tip of the ETT located - Portex - Parker Flexi-tip |
Portex - 3 o'clock Parker - 12o-clock (make easier to insert) |
|
|
Tracheal tube connector |
set dimensions, set by ASTM/ ISO standards patient end - size set as per ETT size machine end - 15-mm male fitting |
|
|
Tapered connector |
- connector b/w ETT (15mm) and circuit or facemark (22mm) - tapered end - ID 15mm ( fit ETT) - ED 22mm (fit facemask) Filter - same tapered end (15mm ID, 22mm OD) |
|
|
aintree catheter |
"turtoise" catheter 56cm long, 4.7 mm ID - help convert LMA to ETT - max size bronch = 4.5cm - smallest ETT #7 railroaded over aintree - 15mm attachment to allow oxygenation through aintree - dont inserted more than 26cm at teeth |
|
|
Cook exchange catheter |
= long blue catheter 83cm length attachment allow oxygen to be delivered (connect directly to green O2 circuit) |
|
|
optimal cuff pressure in LMA |
60mmHg |
|
|
max eat size fit down lma - 3 - 4 - 5 |
3-4 = 6ETT 5 = 7 ETT |
|
|
iLMA |
size 3, 4, 5 LMA all same internal diameter accept up to size 8 ETT iLMA ETT come in 6 to 8mm iLMA longer than normal ETT |
|
|
Proseal LMA c/w classic - advantage - disadvantage |
Advantage 1. higher airway seal pressure (30-35cmh2O c/w 20cmH2O for classic) --> better ventilation (even better than supreme LMA) - ventral cuff pushed by dorsal cuff into periglottic structures to improve seal 2. gastric port 3. successful use in difficult and rescue airway 4. incorporated bite block Disadvantage 1. higher cuff pressures 60cmH2O (but no increase in mucosal pressure) |
|
|
Allen test - rating delay |
Normal : 7 sec Borderline 7-15sec Abnormal >15sec low sensitivity and specificity |
|
|
How does pressure transducer in arterial line work? |
change in pressure proportional to change in length of diaphragm which is proportional of change in resistance change in resistance detected via wheatstone bridge and converted to electrical change |
|
|
Definition of dampening |
reduction in amplitude of oscillation in an oscillating system, caused by energy loss. described as dampening coefficient --> underestimate SBP + overestimate DBP, MAP same |
|
|
Factors affecting dampening |
1. inertance = viscous friction within the fluid column 2. impedance = changes in caliber of fluid path 3. compliance = elastic catheter material or air bubbles |
|
|
What is resonance? |
tendency of system to oscillate with greater amplitude at the natural frequency than at other frequencies. diaphragm will have natural frequency (tendency to vibrate). If natural frequency = HR then increased lengthening for any change in pressure. aim to have frequency well above same frequency as HR --> overestimate SBP, underestimate DBP, MAP same |
|
|
Dampening |
optimal dampending: 0.64 best glance b/w speed of response and accuracy ensures: 1. minimise amplitude distortion 2. maximal frequency response 3. Phase distortion minimised |
|
|
system with high natural frequency |
e.g. high resonance will cope with a wide range of dampening damping coefficient incr as damping incr |
|
|
Causes of too much damping |
1. long rigid tube 2. blocked sample line (kinks or bubbles) 3. arterial vasospasm |
|
|
problem with bubbles in arterial line |
damping increase, resonance decrease because it does both, inaccurate reading and SBP can be high or low |
|
|
2 steps in calibrating an arterial line |
1. zeroing - remove atmospheric pressure 2. Leveling - specific position on patient's body (level of right atrium) |
|
|
slurring systolic upstroke in arterial line trace |
suggest AS |
|
|
Differences in arterial pulse pressure trace as you move further away from heart |
1. high systolic pressure 2. further dicrotic notch 3. lower diastolic pressure (wider pulse pressure) 4. later arrival of pulse NB - MAP doesn't change much |
|
|
how do you determine the size of the reservoir bag in a circuit |
patient's peak inspiratory flow rate |
|
|
Compare having a vaporiser inside or outside the circle circuit |
Inside not as good as outside Problem with inside: 1. need low resistance inside vaporise to allow air to go thru 2. risk of high volatile concentration (gas "to-and-fro" thru vaporiser) 3. slow onset in spont breathing pt as concentration of violate dependent on pt's inspiratory flow rate Good about outside vaporiser: 1. required concentration achieved by adjusting vaporiser 2. never deliver more than max volatile concentration |
|
|
Disadvantages of circle system |
1. small tidal volumes may not generate enough pressure to open valves effectively 2. Dead space in y-absorber (cause re-breathing) 3. Expensive and bulky 4. unstable is used closed 5. slow change in inspired VA conc with low flows or out-of-circuit vaporiser 6. resistance to breathing - soda lime and valves 7. inhalation of soda-lime dust |
|
|
Advantages of circle system |
1. economy of gas consumption 2. warm + humidify 3. reduced atmospheric pollution 4. efficient use of soda lime |
|
|
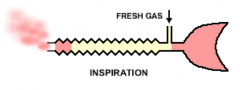
Mapleson E system - draw |
|
|
|
FGF requirement in mapleson E systemm |
1.5 - 2 x MV in spontaneously breathing patient |
|
|
advantages of t-piece |
1. compact 2. inexpensive 3. No valves 4. Low dead-space 5. low resistance to breathing 6. Economical for controlled ventilation |
|
|
Disadvantages of T-peice |
1. heavy, difficult to keep connected to ETT in small kids 2. twisted bag may impede breathing 3. high FGF requirements |
|
|
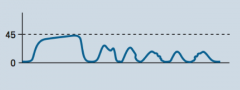
Air leak - loose connection b/w sampling tube and capnograph/ broken connection or filter |
|
|
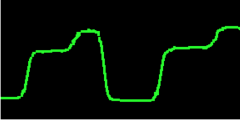
Bronchospasm, COPD, emphysema, obstructed ETT |
|
|
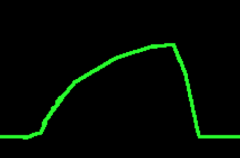
ETT cuff leak/ deflated cuff ETT in hypo pharynx partial obstruction |
|
|
Describe process for cell salvage |
1. collection - mixed with anti-coagulant 2. filtered - remove debris/ clot 3. centrifuge - remove plasma - inc platelet and clotting factors + addition of N/S 4. stored in re-infusion bag for infusion |
|
|
Hct of RBC produced by cell salvage |
60-70% |
|
|
Advantages of cell salvage |
1. reduce autologous blood transfusion - finite resource - less cross matching - risk of early or delayed reaction to autologous blood - risk infection - immunosuppression from autologous blood 2. Acceptable to Jehovas witness 3. minimise risk DIC with rein fusion |
|
|
Disadvantage of cell salvage |
1. machinery, personnel, training 2. NO platelets, some clotting factors 3. inefficient - 60% salvaged blood saved 4. C/I : betadine, malignant cells, infection, amniotic fluid, sickle cells disease 5. incorrect washing --> cell lysis and prob on rein fusion 6. air embolism on reinfusion 7. can't be pumped back --> haemolysis |
|
|
What is CLABSI? |
laboratory-confirmed blood stream infection related to presence of central line or umbilical catheter that is in place either at the time of or within 48hr before the onset on an infection Not related to infection at another site |
|
|
Modifiable and non-modifiable risk factors for CLABSI |
Modifiable: 1. type - polyurethane < silicone 2. lumens - more lumen > less lumen 3. frequency of hub manipulation 4. location - peripheral < central; subclavian < IJ < femoral 5. type: tunnelled < non-tunnelled 6. duration 7. emergency > elective 8. skilled < un-skilled operator 9. TPN Non-modifiable 1. child > adults 2. disease - immunocompromised, CVS, GI disease 3. male |
|
|
Sources of catheter infection |
1. extra-lumen (skin --> migrate down CVC) 2. Intra-lumen (more common) |
|
|
What are the contents of soda lime |
80% - calcium hydroxide 15% - water 4% - Na hydroxide 1% - K hydroxide |
|
|
Max absorbed CO2 |
26L of CO2 / 100gram absorbent |
|
|
Disadvantages of soda lime |
1. increase time to anaesthetic onset 2. CO - from CHF2 terminal groups - desflurane most CO - production promotional to time VA in contact with CO2 absorbent - more common in anaemic pt, long surgery 3. compound A - nephrotoxic in rats, not proven in humans - need 1.25 MAC over 4-8 hr at 2L/min FGF - sevoflurane 4. Trichloroethylene - react with soda-lime to produce toxic compounds (dichloroacetylene - cranial neurotoxin) |
|
|
Factors incr CO production |
1. Agent DEs > en > iso 2. Dryness of absorbent 3. Baralyme 4. incr temp 5. low gas flow rates |
|
|
Factors that incr compound A formation |
1. baralyme 2. dehydration of baralyme 3. hypercapnia 4. low flow rates 5. incr temp 6. fresh absorbent NB - soda lime dehydration decreases production of compound A from sevoflurane |
|
|
what are the waves of the CVP trace and what do they mean? |
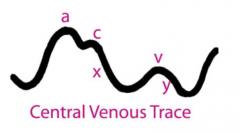
A - atrial contraction. none in AF. incr in TS, PS, pul HTN C - tricuspid valve budge into right atrium - isovolumentric contraction x descent - atrial relaxation V - incr atrial pressure before tricuspid valve open (end of RV systole). prominent in TR y-descent - atrial empty blood enter ventricle cannon wave - large wave not correspond to a,v, or c --> complete heart block or junctional arrhythmia |
|
|
Cause of cannon a wave |
AV dissociation + VT |
|
|
Monophasic waveform in defibrillator |
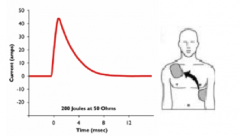
-shock delivered from one vector -no ability to adjust for patient impedance -graphically shown as current vs time |
|
|
Biphasic waveform in defibrillator |

- shock delivered to heart via two vectors - lower current required c/w monophasic - two types of waveforms |
|
|
TOE 4 chamber view - angle used - diagnostic uses |
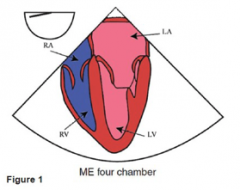
Angle: 0-10degree
Primary diagnostic uses - chamber enlargement/ dysfunction - LV regional wall - MV and TV - intracardiac mass |
|
|
TOE 2 chamber view - angle - diagnostic uses |
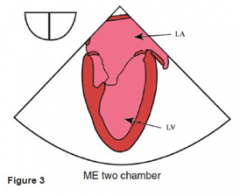
Angle: -80-100 degree Diagnostic uses: - LA appendage - mass/ thrombus - LV apex - LV systolic dysfunction - LV regional wall - anterior and inferior wall |
|
|
TOE ME AV Short-axis (SAX) view - angle - diagnostic uses |
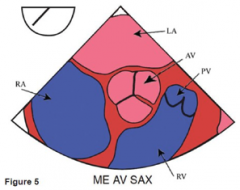
Angle: 25-45 degree Diagnostic uses 1. AV morphology 2. AS/ regurg 3. coronary arteries 4. air in roof of LA |
|
|
Microshock definition |
- induction of VF by small electrical currents (below the threshold of skin sensation) - requires small area of contact with heart muscle so current density high despite low current - = <10 uAmps - e.g. central line with a faulty transducer attached |
|
|
RCD (residual current device) |
- detect difference b/w active and neutral wire. - leak >5-10mA --> trip RCD --> stop current flow |
|
|
Disadvantages of RCD |
1. Not protect against microshock
2. trip electricity to whole theatre complex until faulty device removed 3. will not detect faults in electricity pass thru body and back thru neutral wire (rare) |
|
|
Line isolation monitor - how does it work |
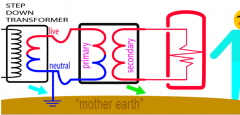
- floating circuit with no earth - isolation transformer with 2 coils - can't form circuit by connecting to earth |
|
|
Advantages of line isolation monitor |
1. protect against MACROshock 2. does NOT cut off electricity supply to machines |
|
|
Disadvantages of line isolation monitor |
1. require two breaks in circuit to cause macroshock 2. only detect problem with wire A, B and earth; NOT wire A, B and other metal covering 3. does not protect against MICROshock |
|
|
what do you need for cardiac protected area |
- equipotential earthing+ either RCD or LIM |
|
|
Types of electrical damage |
1. burns 2. ignition of a flammable substance 2. electrocution |
|
|
Injuries possible in electrical damage |
1. depolarisation of muscle cells - VF, systole 2. vascular: thrombosis, compartment synd, rhabdomyolysis 3. neuro: peripheral nerve inju 4. renal: myoglobinuria 5. other: trauma, fire |
|
|
3 elements of "fire triangle" |
1. ignition source - laser (10%), diathermy (70%) 2. oxidiser - O2, N2O 3. Fuel - ETT, drapes |
|
|
How to prevent fire during tracheostomy: |
1. lowest possible FiO2, avoid N2O 2. don't use diathermy to incise trachea 3. single lumen ETT with cuff is distal trachea (therefore O2 conc 21% on tracheal incision) 4. Saline in ETT cuff instead of air |
|
|
Management of fire in tracheostomy: |
1. Disconnect from circuit 2. remove burning material 3. extinguish fire - water or CO2 extinguisher 4. complete tracheostomy 5. ventilate pt with room air and self-inflating bag 6. other: flush saline thru ETT to extinguish fire, assess extent of burn |
|
|
how does Ultrasound work |
frequency 2-15mHz Generation: - crystal in transmitter probe stimulated to vibrate by electrical current - piezoelectric effect - electrical energy transduced to sound energy detection - reflected waves detected by probe - sound wave --> crystal vibrate --> transduce electrical signal (piezoelectric effect) Transmission - absorbed, transmitted through or reflected off - change in density - amplitude = brightness - water = hyper echoic = black - bone = hypoechonic = white |
|
|
conversion french to diameter |
Fr = D (mm) x 3 D (mm) = Fr/3 |
|
|
tool for detecting awareness under GA |
Brice questionarrie 1. last thing remember before sleep? 2. first thing remember when awake? 3. Dream? 4. worst thing about operation 5. next worst thing? |