![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
4th week |
-together with the liver, the GB and bile ducts are forced by a ventral diverticulum, or sac, which turns into the septum transversum |
|
|
Do we see the GB on fetal sonography? |
-yes but it is nonfunctional till birth |
|
|
What is the location of the gallbladder? |
-intraperitoneal in the RUQ -lateral to 2nd part of duodenum -anterior to right kidney -in main lobar fissure (GB fossa) btw rt & lt lobes -GB neck fixed to MLF and RPV but GB moves |
|
|
What is the shape of the gallbladder? |
-pear or tear drop, but can vary |
|
|
What is the length of the gallbladder and what is the length in transverse? |
7-10 cm length 3-4 cm in transverse |
|
|
How much bile is the gallbladder capable of holding? |
30-60 mL (cc) (fasting state) |
|
|
What is the thickness of the gallbladder wall? |
< 3mm thick |
|
|
What are the three sections of the gallbladder? |
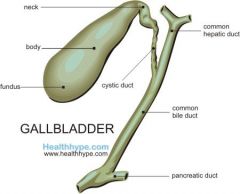
-neck -body -fundus |
|
|
Neck of the gallbladder |
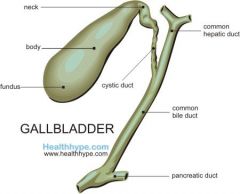
-narrowest portion of GB -continuous with cystic duct -oriented to the right of the portal hepatis |
|
|
Body of the gallbladder |
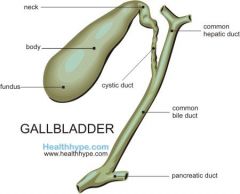
-large, central portion between the neck and fundus |
|
|
Fundus of the gallbladder |
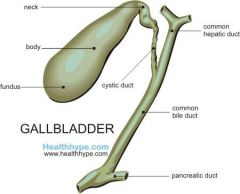
-widest, most inferior portion -position changes with patient position |
|
|
What are the wall layers of the gallbladder |
-serosal layer- outermost layer -subserosal layer -muscular layer -mucosal layer- innermost layer |
|
|
Muscular layer
|
-made of longitudinal and diagonal fibers which allow the GB to have expansion and contraction capabilities |
|
|
Mucosal layer |
-innermost layer consisting of folds -mucous glands are present only in the neck of GB |
|
|
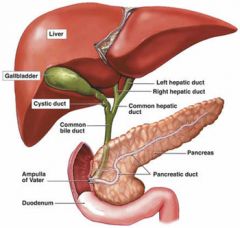
What are the branches of the biliary tree? |
-intrahepatic ducts form rt and lt hepatic ducts -RHD&LHD join & form common hepatic duct -CHD exits liver @ porta hepatis, courses inferiorly toward GB where it joins cystic duct -distal to CHD&CD, the common bile duct begins |
|
|
The cystic duct contains what? And what does it connect? |
-contains folds (spiral valves of heister), that prevent kinking of the cystic duct -connects the GB neck to the common hepatic duct |
|
|
Where does the common bile duct course and what does it join? |
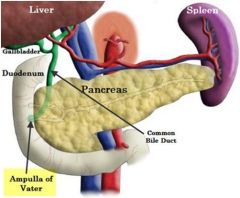
-courses inferiorly through head of pancreas where it joins the main pancreatic duct before emptying into duodenum through the opening (ampulla of vater) - controlled by muscle called sphincter of oddi |
|
|
What are the dimensions of the ducts? |
bile canaliculi: microscopic, unable to see RHD & LHD: < 2 mm CHD: < 6 mm (at porta hepatis) CD: < 2 mm, average length 1-2 cm CBD: < 7-8 mm, 8 cm in length |
|
|
Junctional fold |
-most common variant -incomplete wall appearing btw body and neck -fold in mucosal layer |
|
|
Multiseptated |

-internal septum dividing the GB into two or more chambers -septum can be partial fold or complete -complete septation can lead to bile stasis and stone formation |
|
|
Hourglass gallbladder |
-abnormal narrowing at the mid portion of the GB body |
|
|
Hartman's pouch |
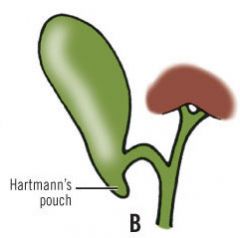
-small sac like diverticulum of GB neck -common area for stone formation due to bile stasis |
|
|
Phrygian cap |

-fold toward the fundus of the GB -results in 'cap like' appearance at fundus |
|
|
Agenesis |
-complete absence of the gallbladder -rare only occurring 0.04-0.07% of cases |
|
|
Ectopic location |
-Intrahepatic- embedded in liver parenchyma -located on the left side (situs inverse) or midline |
|
|
What are the functions of the gallbladder |
-concentrates bile produced by hepatic cells -stores concentrated bile in the gallbladder -transports bile to intestines to aid in digestion |
|
|
Bile Composition |
-bile salts -cholesterol -amino acids -various steroid hormones |
|
|
What is the bile functions |
-emulsifies ingested fat & aids in fat absorption* -stimulates the action of lipase |
|
|
Bile secretion |
-secreted by hepatocytes into bile canaliculi -in fasting, 1/2 bile is drained into CHD into GB, while other 1/2 drains into CBD |
|
|
What is secreted in a non-fasting state? |
-cholecystokinin is secreted by duodenal mucosa -tells GB to contract & sphincter of oddi to open -bile from GB drains in CBD and enters duodenum through ampulla of vater |
|
|
What happens with WBC and what is it associated with? |
Elevated with inflammatory processes -acute & chronic cholecystitis -empyema of the GB -cholangitis (inflammation of BD, not GB) |
|
|
Indirect (unconjugated) elevation suggests what? |
-hepatocellular disease |
|
|
Direct (conjugated ) elevation suggests what? |
Obstructive liver disease (affects biliary system) -subacute cholecystitis -choledocholithiasis (highest elevation) -injury to bile ducts -GB carcinoma -internal biliary fistula or retained bile duct stones |
|
|
What does an increase in Serum Alkaline Phosphatase indicate? |
ALP -biliary obstruction |
|
|
Indications for a GB exam |
-RUQ pain -positive (+) Murphy's sign -pain radiating to right shoulder (inflammation) -nausea, vomiting, loss of appetite -intolerance to fatty foods and diary -jaundice |
|
|
What does a Positive (+) Murphy's sign mean? |
-pain with transducer pressure over the gallbladder during inspiration |
|
|
Non-visulization of the gallbladder could be from what? |
-pt not NPO -cholecystectomy -GB is congenitally absent or ectopic -GB filled with stones |
|
|
What are some patient interview and physical exam questions for a gallbladder exam? |
-past medical and surgical history -chief complaints (frequency&duration) -check chart and include lab tests -check abd for surgical scars -check for (+) murphy's sign |
|
|
What is the sonographic appearance of the GB |
-anechoic and thin walled (< 3 mm) -acoustic enhancement posterior to GB -intrahepatic ducts typically not visualized -CD may or may not be seen -Follow CBD to head of pancreas -use color to differentiate bile ducts from vessels |