![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
287 Cards in this Set
- Front
- Back
|
AChEI relative contraindications
|
1. PUD
2. Hepatic disease 3. Renal disease 4. Bradycardia or AV block 5. Significant bronchospastic disease 6. Obstructive urinary disease 7. Epilepsy or history of seizure |
|
|
Side effects of donepezil, rivastigmine and galantamine.
|
Diarrhea
Nausea Vomiting Anorexia, weight loss Dizziness, syncope, vertigo Asthenia, fatigue, insomnia Muscle cramps Abnormal dreams Headache Peripheral oedema Tremor (Cochrane 2006 CI for AD) |
|
|
Adverse effects of memantine.
|
Dizziness 6.3%
Headache 5.2% Constipation 4.6% Hypertension 4.1% Somnolence 3.4% (van Marum. Neuropsych Dis and Treatment 2009) |
|
|
Dosing of memantine.
Renal clearance? Hepatic metabolism? Drug interactions? |
Memantine 5-10 mg bid
Renal excretion accounts for 65-90% of clearance. In patients with CrCl 10-30, maximum daily dose should be 5 mg bid. Not subject to major hepatic metabolism. No significant drug interactions, but alkaline urine can reduce renal excretion. Therefore, caution in patients taking sodium bicarbonate, carbonic anhydrase inhibitors, and severe UTI. (van Marum. Neuropsych Dis and Treatment 2009) |
|
|
How do you interpret a BMD T score?
|
Normal is +1 to -1 SD.
Below -1 is osteopenia. Below -2.5 is osteoporosis. |
|
|
DSM V diagnostic criteria for delirium.
|
A. Disturbance of attention (reduced ability to focus, sustain or shift attention), and awareness.
B. Disturbance develops over a short period of time (usually hours to days), represents a change from baseline attention/awareness, and tends to fluctuate in severity during the course of a day. C. An additional change in cognition (memory, disorientation, language, visuospatial ability, or perception). D. Not better explained by another NCD, and do not occur in the context of a severely reduced level of arousal, such as coma E. There is evidence that the disturbance is caused by a medical condition, substance intoxication, or withdrawal, or exposure to a toxin, or is due to multiple etiologies. |
|
|
What are causes of falls?
|
Medications
Accidental Neurological Cardiovascular Visual problems Precipitants (infection, infarction, social stress) |
|
|
Reach test - what is considered abnormal?
|
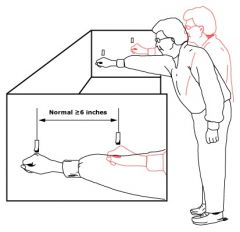
< 6 inches, or 15 cm.
|
|
|
What are the 6 target interventions in the Yale delirium prevention trial that were shown to be effective?
|
1. Cognition - orientation and therapeutic activities protocols
2. Sleep - non-pharmacological sleep enhancement protocols 3. Immobility - early mobilization protocol 4. Vision protocol 5. Hearing protocol 6. Dehydration protocol |
|
|
Major or mild FTD - what are the diagnostic criteria according to DSM V? |
A. Meets criteria for major or mild NCD. B. The disturbance has insidious onset and gradual progression. C. Either (1) or (2): 1. Behavioral variant: Three or more of the following: - Behavioral disinhibition - Apathy or inertia - Loss of sympathy or empathy - Perseverative, stereotyped or compulsive/ritualistic behavior - Hyperorality and dietary changes Relative sparing of memory and visuospatial functions Prominent decline in social cognition and/or executive abilities 2. Language variant: prominent decline in language ability, in the form of speech production, word finding, object naming, grammar, or word comprehension. D. Relative sparing of memory and perceptual-motor function. E. Not better explained by CVD, another neurodegenerative disease, the effects of a substance, or another mental, neurological, or systemic disorder. |
|
|
Features of semantic variant PPA. |
Core features: -Impaired confrontation naming -Impaired single-word comprehension Other features: -Impaired object knowledge, particularly for low-frequency or low-familiarity items -Surface dyslexia or dysgraphia -Spared repetition -Spared speech production (grammar and motor speech) Anterior temporal lobe atrophy |
|
|
Features of progressive nonfluent aphasia. |
Core features -Agrammatism in language production -Effortful, halting speech with inconsistent speech sound errors (apraxia of speech) Other features -Impaired comprehension of syntactically complex sentences -Spared single-word comprehension -Spared object knowledge Left posterior fronto-insular atrophy |
|
|
Features of logopenic variant PPA |
Core features -Impaired single-word retrieval in spontaneous speech and naming -Impaired repetition of sentences and phrases Other features -Speech (phonologic) errors in spontaneous speech and naming -Spared single-word comprehension and object knowledge -Spared motor speech -Absence of frank agrammatism Left posterior perisylvian or parietal atrophy |
|
|
What is the pathologic finding of FTLD? |
Phosphorylated tau Transactive response DNA-binding protein 43 (TDP-43) Fused in sarcoma (FUS) protein |
|
|
Give two theories for aging. |
Programmed cell death, or "adaptive" aging. In this theory, aging is considered a beneficial aspect of evolution, to prevent overcrowding. Genes evolved that actively cause aging. Non-adaptive theories (stochastic theories) -Pleiotropic gene theory. There is a declining force of natural selection with age. Therefore, some genes that confer an advantage early in life will be favoured even if the same gene has deleterious effects later on (called pleiotropic genes). -Disposable soma theory. Goal of an organism is to balance keeping itself going on a day-to-day basis, versus maintaining itself in the long-term. Optimum course of life is to invest fewer resources in the maintenance of somatic tissues, and deleterious effects of this are not seen until long after the organism would have died in the wild environment. |
|
|
Two human progeroid syndromes |
Werner's syndrome (DNA helicase) Hutchinson-Gilford progeria (lamin A gene) |
|
|
What is the Hayflick limit? |
Human cells grown in culture have a limited life span. Telomeres are the structures at the ends of chromosomes, synthesized by telomerase. As cells divide, the length of telomeric DNA shortens until a lower limit is reached (called the Hayflick limit) at which point proliferation ceases. |
|
|
Theories of cellular senescence. |
1. Programmed cell death: reduction in telomere length and telomerase activity. 2. Stochastic theory of genomic instability (DNA mutations, gene repression, gene overexpression, genomic DNA damage, mitochondrial DNA damage). |
|
|
MCI - DSM V criteria |
A. Evidence of modest decline from previous level of performance in one or more cognitive domains based on: (i) concern of the individual, a knowledgeable informant, or the clinician; and (ii) a modest impairment on neuropsychological testing or other quantified clinical assessment B. The cognitive deficits do not interfere with everyday activities. C. Does not occur in the context of delirium D. Not explained by another mental disorder (e.g. depression, schizophrenia) |
|
|
Major neurocognitive disorder - DSM V criteria |
A. Evidence of significant cognitive decline in one or more cognitive domains based on: (i) concern of individual, knowledgeable informant, or clinician; and (ii) substantial impairment in cognitive performance on standardized neuropsychological testing or other quantified clinical assessment B. The cognitive deficits interfere with independence in everyday activities C. Not in context of a delirium D. Not better explained by another mental disorder |
|
|
Major or minor NCD due to vascular disease - DSM V criteria Probable versus possible |
A. Criteria met for dementia B. Clinical features are consistent with a vascular etiology, as suggested by either: (i) Onset of cognitive deficits is temporally related to one or more cerebrovascular events (ii) Evidence for decline is prominent in complex attention (including processing speed) and frontal-executive function C. There is evidence of cerebrovascular disease from history, physical exam, and/or neuroimaging considered sufficient to account for the neurocognitive deficits. D. The symptoms are not better explained by another brain disease or systemic disorder. Probable vascular neurocognitive disorder is diagnosed if one of the following is present; otherwise possible vascular neurocognitive disorder should be diagnosed: 1. Clinical criteria are supported by neuroimaging evidence. 2. Neurocognitive syndrome is temporally related to one or more documented cerebrovascular events. 3. Both clinical and genetic (e.g. CADASIL) evidence of cerebrovascular disease is present. |
|
|
Major or minor NCD due to Alzheimer disease - DSM V criteria Probable versus possible |
A. Criteria met for major or mild NCD B. Insidious onset, and gradual progression in one or more cognitive domains (for major NCD, at least 2 domains must be impaired) C. Criteria are met for either probable or possible AD as follows: For major NCD, probable AD is diagnosed if either of the present is following is present; otherwise possible AD should be diagnosed: 1. Evidence of a causative AD genetic mutation from family history or genetic testing. 2. All three of the following are present: a. Clear evidence of decline in memory and learning and at least one other cognitive domain b. Steadily progressive, gradual decline in cognition, without extended plateaus c. No evidence of mixed etiology For mild NCD: Probable AD is diagnosed if there is evidence of a causative AD genetic mutation from either genetic testing or family history Possible AD is diagnosed if there is no evidence of a causative AD genetic mutation from either genetic testing or family history, and all three of the following are present: 1. Clear evidence of decline in memory and learning 2. Steadily progressive, gradual decline in cognition, without extended plateaus. 3. No evidence of mixed etiology D. The disturbance is not better explained by cerebrovascular disease, another neurodegenerative disease, the effects of a substance, or another mental, neurological, or systemic disorder. |
|
|
Probable vs probable AD dementia - NIA-AA criteria |
Probable AD dementia, use when meets criteria for dementia, and in addition, has the following characteristics: -Insidious onset, over months to years, not sudden over hours or days; -Clear-cut history of worsening cognition by report or observation; and -The initial and most prominent cognitive deficits are evident on history and examination in one of the following categories Amnestic presentation Nonamnestic presentation (language, visuospatial, executive dysfunction) Possible AD dementia, should be used in either of these circumstance: -Atypical course: sudden onset of cognitive impairment or demonstrates insufficient historical detail, or objective documentation of progressive decline. -Etiologically mixed presentations Stroke temporally related; or presence of extensive infarcts or severe white matter disease Features of DLB Evidence of another neurological disease, non-neurological medical comorbidity, or medication use that could have a substantial effect on cognition |
|
|
What are risk factors for MCI progressing to dementia? |
JAMA 2014: older age, fewer years of education, stroke, diabetes, amnestic type MCI |
|
|
Dementia - who needs neuroimaging? |
From CCCDTD4 1. Age less than 60 years 2. Rapid (e.g., 1 or 2 months) unexplained decline in cognition or function 3. “Short” duration of dementia (less than 2 years) 4. Recent and significant head trauma 5. Unexplained neurological symptoms (e.g. new onset of severe headache or seizures) 6. History of cancer (especially in sites and types that metastasize to the brain) 7. Use of anticoagulants or history of bleeding disorder 8. History of urinary incontinence and gait disorder early in the course of dementia (as may be found in normal pressure hydrocephalus) 9. Any new localizing sign (e.g., hemiparesis or a Babinski reflex) 10. Unusual or atypical cognitive symptoms or presentation (e.g. progressive aphasia) 11. Gait disturbance |
|
|
Diagnosis of dementia with Lewy Bodies |
Central feature: progressive cognitive decline, dementia Core features: fluctuations, visual hallucinations, parkinsonism - 1 feature for possible DLB, 2 features for probable Suggestive features: REMSBD, neuroleptic sensitivity, dopamine transporter imaging - 1 feature for possible, or 1 suggestive + 1 core for probable Supportive features (undetermined diagnostic specificity) -repeated falls -syncope or transient loss of consciousness -autonomic failure -hallucinations in other modalities -systematized delusions -depression -relative preservation of medial temporal lobe on MRI or CT -generalized low uptake on SPECT or PET with reduced occipital activity -abnormal uptake on MIBG cardiac scintigraphy -prominent slow wave activity and temporal lobe transient sharp waves on EEG |
|
|
List characteristics of the fluctuations of cognition in DLB, and list assessment tools that can be used. |
1. Daytime drowsiness and lethargy 2. Daytime sleep >2 hours 3. Disorganized speech 4. Duration of episodes last seconds to days 5. Staring into space for long periods (see original DLB consensus) Tools include: Clinician Assessment of Fluctuation scale One Day Fluctuation Assessment scale Mayo Fluctuations Composite scale |
|
|
List the characteristics of parkinsonism in DLB that may be different from idiopathic PD. |
Axial tendency, with greater postural instability, gait difficulty, facial immobility. Resting tremor less common Less levodopa responsive |
|
|
For mild or major vascular NCD, what is considered sufficient evidence of vascular disease on neuroimaging?
|
For mild vascular NCD, single stroke or extensive white matter disease is generally sufficient. For major vascular NCD, two or more strokes, a strategically placed stroke (angular gyrus, thalamus, basal forebrain), or a combination of white matter disease and one or more lacunes is generally necessary. DSM V, page 622 |
|
|
What are clinical features supportive of vascular dementia? |
1. Abrupt deterioration within 3 months after stroke, and fluctuating or stepwise course 2. History of gait disorder, or frequent falls 3. Urinary frequency and incontinence early in the course of the dementing illness 4. Neurological findings (focal deficit, sensory loss, pseudobulbar syndrome, extrapyramidal signs, psychiatric symptoms) From the NINDS-AIREN vascular dementia diagnostic criteria 1993 paper |
|
|
Biomarkers of the AD pathophysiological process |
NIA-AA 2011 workgroup: Evidence of brain amyloid-beta (Aβ) protein deposition: -Low CSF Aβ42 -Positive PET amyloid imaging Evidence of downstream neuronal degeneration or injury: -Elevated CSF tau, both total tau and phosphorylated tau (p-tau) -Decreased FDG uptake on PET in temporoparietal cortex -Disproportionate atrophy on structural MRI in medial, basal and lateral temporal lobe, and medial parietal cortex |
|
|
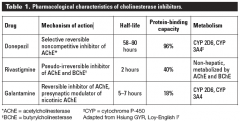
List the MOAs, half-lives, and metabolism pathways of the ChEIs. |
|
|
|
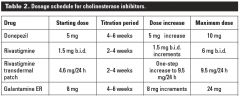
Dosing of cholinesterase inhibitors. |
|
|
|
Pathophysiological mechanisms linking late-life anxiety and cognitive impairment. |
Structural alterations in brain are seen in anxiety disorders (limbic system, hippocampal and prefrontal regions) Reduced neurotransmitter function (serotonin, acetylcholine) HPA-axis dysregulation (chronic high cortisol may damage the hippocampus) Genetic vulnerability (serotonin transmitter, Apo e4 allele) |
|
|
Differences of how late-life anxiety presents, compared to anxiety in younger counterparts. |
DSM-V: Content of worry - older adults report greater concern about well-being of family or their own physical health. Frail elderly may also worry about safety, such as falling, and limit their abilities. Chronic physical disease may be a potent issue for excessive worry in elderly. Linked with cognitive impairment, and what may appear to be excessive worry, such as the whereabouts of things, may be due to cognition. |
|
|
Oculomotor findings in PSP. |
1. Ophthalmoplegia (vertical > horizontal) 2. Saccadic intrusions into fixed gaze (square wave jerks) 3. Loss of optokinetic nystagmus 4. Loss of convergence 5. Blepharospasm 6. Eyelid-opening apraxia |
|
|
Rome III diagnostic criteria for chronic constipation |
Criteria must be fulfilled for last 3 months, with symptom onset at least 6 months before diagnosis. 1. 2 or more of the following: -straining during at least 25% of defecations -lumpy or hard stools in at least 25% of defecations -sensation of incomplete evacuation for at least 25% of defecations -sensation of anorectal obstruction/blockage for at least 25% of defecations -manual manoeuvres to facilitate at least 25% of defecations -fewer than 3 defecations/week 2. Loose stools are rarely present without the use of laxatives 3. Insufficient criteria for IBS |
|
|
Why does lactulose cause more side effects than PEG? |
Adverse effects include bloating, flatulence, abdominal pain, diarrhea. These effects are most often with lactulose, because of its metabolism by colonic bacteria to carboxylic acids. Patients can also develop an aversion to sweet taste of lactulose. (Gandell 2013) |
|
|
List drugs commonly associated with constipation |
Antacids containing calcium or aluminum Calcium supplements NSAIDs Oral iron Antihistamine Opioids CCB Antiparkinsonian agents Anticholinergic Diuretics Antipsychotics TCA |
|
|
Diseases states commonly associated with constipation |
Metabolic -Diabetes -Hypothyroidism -Hypercalcemia -Hypokalemia GI -CRC -Stricture Neurologic -Stroke -Parkinson disease -Dementia -MS -Autonomic neuropathy Psychiatric -Depression -Anxiety -Somatization Connective tissue -Systemic sclerosis -Amyloidosis |
|
|
Alarm symptoms and signs in patients with chronic constipation |
Family history of colorectal cancer Hematochezia Anemia Weight loss ≥ 5 kg in previous 6 months Positive result of fecal occult blood test Persistent constipation unresponsive to treatment Acute onset of constipation |
|
|
Agents used for constipation |
Osmotic agents (lactulose, PEG, Mg, sodium phosphate) Bulk agents (psyllium, methylcellulose) Stimulants (sennosides, bisacodyl) Stool softeners (docusate) Prokinetic agents (prucalopride) Enemas or suppositories Guanylate cyclase C agonist (linaclotide) |
|
|
Definition of constipation |
Any complaint of difficulty passing stool, incomplete passage of stool, or diminished frequency. Straining is the most commonly identified symptom. |
|
|
Non-pharmacologic management strategies for constipation. |
-Ensuring adequate time to toilet -Positioning knees at or above level of the hips for mechanical advantage -Taking advantage of the gastrocolic reflex by guiding cognitively impaired patients to toilet following meal -Biofeedback (electromyographic), for dyssynergistic defecation No great evidence for physical activity or fluid intake, but still encouraged. |
|
|
List changes in the GU system with aging |
Decreased renal plasma flow Decreased bladder contractility Increased bladder overactivity Decreased bladder capacity (lower voiding volumes) Higher pressure threshold for voiding Decreased detrusor muscle to collagen ratio Impaired sphincteric function |
|
|
Innervation of the bladder (sympathetic, parasympathetic, somatic) |
Sympathetic (T10 - L2), via the hypogastric nerve (mostly storage function) Parasympathetic (S2 - S4) via the pelvic splanchnic nerve (mostly voiding function) Somatic (S2 - S4) via the pudendal nerve (controls the external urethral sphincter) |
|
|
6 steps in management of constipation |
1. Identify the main symptom (frequency, straining, incomplete evacuation) 2. Look for secondary causes 3. Exclude fecal impaction 4. Optimize behavioural factors 5. Trial of dietary modifications 6. Trial of previously preferred laxatives, followed by other laxatives |
|
|
8 steps for a QI project initiative |
1. Identify the issue 2. Identify appropriate measures that will allow use to test our hypothesis 3. Determine ideas to improve those measures 4. Test the idea using four steps - Plan - Do - Study - Act 5. Sustain - ensure the process is sustainable |
|
|
Complications of transvaginal sling mesh. |
Infection, erosion, UTIs, retention, incomplete resolution of symptoms. |
|
|
List drugs used for urge incontinence. |
Oxybutynin Fesoterodine Solifenacin Tolterodine Darifenacin Mirabegron |
|
|
Non-pharmacologic interventions/strategies for urge incontinence. |
Weight loss Adequate fluid intake Appropriately timed fluids Dietary changes (avoid excess caffeine, alcohol, artificial sweeteners, concentrated sugars) Behavioural strategies such as urge suppression, bladder retraining, appropriate containment products, manage constipation, strengthening pelvic floor muscles) Prompted or timed voiding |
|
|
Non-pharmacologic treatments of stress incontinence |
Pelvic floor exercises Pessary Surgical procedures (e.g. mid-urethral sling) |
|
|
Evidence-based interventions that have been shown to reduce falls risks in the community.
|
Multi-component group/home-based exercises Tai Chi Multifactorial interventions, including individual risk assessment Vitamin D (in trials that only enrolled patients with low vitamin D) Home safety assessment/modification Pacemakers in people with CSS First eye cataract in women Gradual withdrawal of psychotropic meds Prescribing modification program for primary care physicians Anti-slip shoe device in icy conditions Multifaceted podiatry (Cochrane 2012) |
|
|
List an approach to management of falls/fracture prevention.
|
1. Address medical issues 2. Medication review 3. Assess fracture risk 4. Review home environment 5. Provide appropriate walking aid 6. Gait and balance exercise training
(Dr. Dian's slides)
|
|
|
Key steps to developing a falls prevention program. |
1. Assess your community's needs 2. Establish your program's purpose, goals, and objectives. Goals should be quantitative with objectives that can be easily measured 3. Determine what risk factors your program will address (single intervention programs vs multifaceted intervention programs) 4. Collaborate with partners to address additional risk factors 5. Decide who will implement the various program components (physician, optometrist, NP, pharmacist, RN, PT, OT, SW, certified exercise instructor, Tai Chi instructor) 6. Find a location to conduct the program (home, physician's office, hospital/clinic, PT facility, pharmacy, seniors center, gym/fitness centre, senior housing facility) 7. Evaluate your program 8. Promote your program 9. Sustain your program |
|
|
Consequences of urinary incontinence |
Falls Pressure ulcers, perineal infections Depression Sexual dysfunction Increased caregiver burden (Up-to-date) |
|
|
Consequences of falls |
Hip fracture Fear of future falls Social isolation Economic cost Nursing home admission Mortality (Up-to-date) |
|
|
Positive evidence-based outcomes of deprescribing. |
Reduced falls, improved cognition (withdrawal of psychotropic drugs and benzos) Fewer cardiovascular events and death (inappropriate antihypertensives) Reduced emergency visits Reduced annual mortality and referrals to acute care hospital in LTC (Garfinkel 2007) Patient-reported global improvement in health (Garfinkel 2010) Reduced days in hospital |
|
|
Describe a protocol for deprescribing. |
1. Ascertain all drugs and the reasons for taking them 2. Consider overall risk of drug-induced harm in determining the required intensity of deprescribing intervention 3. Assess each drug for its eligibility to be discontinued 4. Prioritize drugs for discontinuation 5. Implement and monitor drug discontinuation regiment (Scott IA. JAMA Int Med 2015) |
|
|
Barriers to deprescribing. |
Clinical complexity Limited consultation time Fragmented care among multiple prescribers, incomplete information (on past rationales for, and patient tolerance of drugs) Ambiguous or changing care goals Uncertainty about benefits and harms of continuing or discontinuing specific drugs Community/professional attitudes toward more rather than less use of drugs Fear of withdrawal effects Recommendations within disease-specific clinical guidelines. Less applicable to older, multimorbid patients with polypharmacy. (Scott IA. JAMA Int Med 2015) |
|
|
Pharmacokinetic changes with ageing. |
Absorption -not much change -absorption of B12, calcium, and iron may be reduced, whereas absorption of levodopa may be increased -reduction of salivary amylase may decrease buccal absorption Distribution -fat increases, water decreases -water soluble drugs (digoxin) have smaller Vd, therefore higher concentration -lipid soluble drugs (diazepam) have larger Vd, therefore longer half-life -decreased albumin, which may increase serum levels of acidic drugs (furosemide, phenytoin, warfarin, salicylic acid) Metabolism -decreased liver mass -decreased liver blood flow -toxicity due to decreased metabolism -decreased first-pass metabolism may increase bioavailability of drugs such as propanolol and labetalol. Some ACE inhibitors are prodrugs (enalapril and perindopril), and require activation in the liver. Their first-pass activation may be reduced. Excretion -decreased renal function -increases half-life of many drugs (diuretics, digoxin) |
|
|
Comorbidities of chronic HIV infection. |
Cardiovascular disease Kidney disease Liver disease CNS disease Bone disease Non-AIDS-associated malignancies (cervical/anal carcinoma, HCC, EBV-related lymphoma, NHL, lung cancer) May be 1) direct effect of HIV, 2) effect of traditional risk-factors in HIV-positive individuals, 3) effect of antiretroviral therapy. (JAMA 2013) |
|
|
List 6 drug-interactions with HIV ART. |
1. Statins and protease inhibitors (increased statin exposure) 2. Benzodiazepines (midazolam, alprazolam, diazepam) and protease inhibitors and efavirenz (increased benzodiazepine exposure) 3. PPI and atazanavir (decreased atazanavir absorption) 4. Opiates (methadone) and ritonavir-boosted protease inhibitors (decreased methadone exposure) 5. Corticosteroids (systemic, inhaled, or intranasal) and ritonavir (increased fluticasone and budesonide exposure; decreased protease inhibitor exposure with dexamethasone) 6. Rivaroxaban and protease inhibitors (increased rivaroxaban) 7. Warfarin and protease inhibitors (increased or decreased warfarin effect) (JAMA 2013) |
|
|
Drug interaction mechanism and consequence of glyburide and Septra. |
Septra inhibits CYP 2C9, which increases risk of hypoglycemia with glyburide. |
|
|
Drug interaction mechanism and consequence of dabigatran and clarithromycin. |
Clarithromycin is a P-glycoprotein inhibitor. Dabigatran is a substrate that has moderate affinity for the P-glycoprotein transport system. Leads to increased serum concentration of dabigatran. |
|
|
Drug interaction mechanism and consequence of warfarin and amiodarone. |
Amiodarone enhances anticoagulant effect of warfarin. The primary mechanism of this interaction is likely related to the ability of amiodarone to inhibit one or more of the enzymes responsible for warfarin metabolism. |
|
|
MoA by which NSAIDs cause hypertension. |
Inhibition of COX-2 in the kidneys, which reduces sodium excretion and increases intravascular volume (Up-to-date: NSAIDs and acetaminophen: Effects on blood pressure and hypertension) |
|
|
Drug interaction mechanism and consequence of carbamazepine and warfarin. |
Carbemazepine reduces serum concentration of warfarin. Carbamazepine induces enzymes responsible for warfarin metabolism (CYP 1A2, CYP 3A4, CYP 2C9). |
|
|
Differentiating features of serotonin syndrome versus NMS. |
They both have FARM: fever, autonomic instability, rigidity, mental status changes. Typical features in serotonin syndrome that are not often seen in NMS are shivering, hyperreflexia, myoclonus, and ataxia. Nausea, vomiting, and diarrhea are also a common part of the prodrome in serotonin syndrome, and are rarely described in NMS. |
|
|
Complications of serotonin syndrome. |
DIC, rhabdomyolysis, myoglobinuria, metabolic acidosis, renal failure, ARDS. (Up-to-date) |
|
|
Clinical manifestations of chronic lithium toxicity. |
Sluggishness, ataxia, confusion, tremor, agitation, seizure, encephalopathy, nephrogenic DI. (Up-to-date) |
|
|
What are 6 components of a falls prevention exercise program (British guidelines)? |
1. Balance and strength (resistance) exercise 2. Individualized 3. Progressive 4. 2-3 times per week 5. Continued over 50 hours 6. Delivered by specially trained instructors |
|
|
Predictors of 6-month mortality in advanced dementia. |
Functional Assessment Staging tool (FAST): 1. Stage 7c (unable to ambulate independently) or beyond on FAST. 2. Patient must have had at least one of the following in the last year (mnemonic: PAUSER) i. Pressure ulcer, multiple, stage 3 or 4 ii. Aspiration pneumonia iii. UTI (pyelonephritis or other upper UTI) iv. Septicemia vi. Eating problems, defined as food or fluid intake insufficient to sustain life v. Recurrent fever after treatment with antibiotics NEJM 2015 "Advanced Dementia" |
|
|
What were the outcomes found to be significantly improved in the Yale delirium prevention trial? |
Reduced number and duration of episodes of delirium in hospitalized older patients. |
|
|
Clinical prediction rule for noncardiac postoperative delirium. |
1. Functional status
2. Aortic aneurysm surgery 3. Thoracic surgery 4. Age > 70 5. Metabolic abnormalities (markedly abnormal sodium, potassium, glucose) 6. Alcohol abuse 7. Cognitive status Mnemonic: FATAMAC (JAMA 1994) |
|
|
Tinetti's POMA balance assessment tasks. |
1. Sitting balance 2. Arises 3. Attempts to arise 4. Immediate standing balance 5. Standing balance 6. Nudged 7. Eyes closed 8. Turning 360 degrees 9. Sitting down |
|
|
Tinetti's POMA gait assessment tasks.
|
1. Initiation of gait 2. Step length and height 3. Step symmetry 4. Step continuity 5. Path 6. Trunk (amount of sway) 7. Walking stance (?wide-based) |
|
|
Changes in PFT with aging. Consequences of these changes. |
Reduced FEV1 Reduced FVC Reduced FEV1/FVC Reduced DLco Increased RV Increased FRC Reduced VO2max Decreased MIP, MEP, SNIP Consequences: 1. Increased frequency of pneumonia 2. Increased risk of hypoxia 3. Decreased max O2 uptake |
|
|
5 features seen in normal aging gait. |
1. Flexed posture 2. Reduced toe-floor clearance 3. Reduced length of stride 4. Slightly broad base 5. Excessive flexion at hips and knees Brocklehurst chapter 16. |
|
|
Normal changes in sleep architecture with aging. |
More fragmented sleep (periods of wakefulness) Decreased sleep duration Decreased slow wave sleep (stage 3/4) Decreased REM sleep Decreased sleep efficiency Lower auditory awakening thresholds Sleep desynchronized from circadian rhythm |
|
|
Normal hearing changes with aging. |
Decreased hearing of higher frequencies Decreased speech discrimination Increased pure tone threshold averages |
|
|
List 5 adverse outcomes of delirium. |
1. Prolonged hospital stay 2. Persistent cognitive impairment 3. Functional decline 4. Mortality 5. Admission to institution |
|
|
Inouye's risk factors for predicting delirium on admission, and during hospitalization.
|
On admission (Arch Int Med 1993): 1. Vision impairment 2. Severe illness 3. Cognitive impairment 4. BUN/Cr ratio high
During hospitalization (JAMA 1996): 1. Physical restraints 2. Malnutrition 3. Meds > 3 4. Bladder catheter 5. Iatrogenic event
|
|
|
5 performance measures of balance
|
Performance oriented mobility assessment (POMA) Berg balance scale TUG Hierarchical assessment of balance and mobility (HABAM) Functional reach
|
|
|
Factors that predispose to developing persistent delirium (Inouye study 2007) |
Dementia (OR 2.3, 95% CI1.4-3.7) Vision impairment (OR 2.1, 95% CI 1.3-3.2) Functional impairment (OR 1.7, 95% CI 1.2-3.0) High comorbidity (OR 1.7, 95% CI 1.1-2.6) Use of physical restraints during delirium (OR 3.2, 95% CI 1.9-5.2) VPD-CF |
|
|
4 risk factors for cataracts. |
Sun exposure Diabetes Alcohol Steroids Smoking Metabolic syndrome (Up-to-date) |
|
|
Age-related differences in response to water deprivation on labs. |
Hypernatremia Increased serum osmolality Increased serum vasopressin Decreased urine osmolality NEJM 1984 Reduced Thirst after Water Deprivation in Healthy Elderly Men. Paddy P et al |
|
|
4 age-related reasons that elderly are predisposed toward hyperkalemia. |
1. Decreased renal tubular secretion of potassium 2. Obstructive uropathy can lead to renal tubular acidosis 3. Hyporeninemic hypoaldosteronism may occur in elderly, in association with diabetes and renal insufficiency 4. Drug-induced hyperkalemia |
|
|
Clinical features of AMD. |
Blurred vision Scotoma Visual distortions (on Amsler grid) Decreased contrast sensitivity Abnormal dark adaptation Need for brighter light or additional magnification to read small print (NEJM 2008 review) |
|
|
Clinical differences between dry versus wet AMD. |
Dry AMD: gradual, insidious vision loss with central or pericentral scotomas, over months to years. Wet AMD: may have sudden, profound visual loss within days to weeks as a result of subretinal hemorrhage or fluid accumulation secondary to choroidal neovascularization. Responsible for 80% of cases of severe visual loss or legal blindness from AMD. (NEJM 2008 review) |
|
|
Risk factors for AMD. |
Advanced age White race Heredity History of smoking in the past 20 years Obesity High dietary intake of vegetable fat Low dietary intake of antioxidants and zinc |
|
|
Pathophysiology of dry versus wet AMD.
|
Dry, or atrophic age-related MD - retinal pigment epithelium and choriocapillaris underlying the macula appears to degenerate, resulting in dysfunction of overlying photoreceptors.
Wet, or exudative age-related MD - neovascular net emanates under the macular region of the central retinal from choroidal circulation, proliferating between the retina and the underlying retinal pigment epithelium. Leakage of plasma components and frank subretinal hemorrhage or scarring cause loss of vision.
(NEJM review 2008)
|
|
|
7 factors associated with longevity past 100 years of age. |
1. Female gender 2. Not smoking 3. Moderation of alcohol 4. Dietary factors 5. Exercise 6. Genetics 7. Compressed morbidity 8. Compressed disability 9. Social factors (emphasis of time spent with friends and family) |
|
|
Biomarkers for delirium. |
High IL-6, IL-8, S-100 ß High cortisol, CRP Low IGF-1 (Khan, JAGS 2011) |
|
|
3 factors that contribute to pruritus of aging. |
Dry skin Immunosenescence Peripheral neuropathy |
|
|
Sensitivity and specificity of the CAM. |
86% sensitivity, 93% specificity (JAMA 2010) |
|
|
Define likelihood ratio. |
The Likelihood Ratio (LR) is the likelihood that a given test result would be expected in a patient with the target disorder compared to the likelihood that that same result would be expected in a patient without the target disorder |
|
|
Formula for positive LR and negative LR. |
Positive LR = sensitivity / (1-specificity)
Negative LR = (1-sensitivity) / specificity |
|
|
What is the difference between relative risk and attributable risk? |
Relative risk is the ratio of the probability of developing an outcome with vs without a given risk factor or intervention. Attributable risk is the absolute difference in incidence between an exposed and unexposed group. |
|
|
Complications of ECT. |
Aspiration pneumonia Fracture Dental and tongue injuries Headache ← most common complication Nausea Memory loss (anterograde and retrograde amnesia) (Up-to-date) |
|
|
Conditions that increase the risk of ECT. |
Unstable or severe cardiovascular disease
Space-occupying intracranial lesion with evidence of elevated intracranial pressure Recent cerebral hemorrhage or stroke Bleeding or otherwise unstable vascular aneurysm Severe pulmonary condition American Society of Anesthesiologists (ASA) Class 4 or 5 (Up-to-date: medical consultation for ECT) |
|
|
Conditions that predispose patients to herpes zoster. |
Physical trauma Malignancy Chronic lung or kidney disease HIV Lymphoma (HL, NHL) Patients on immunosuppressive therapy |
|
|
Formula for PPV (from sensitivity, specificity, prevalence) |

|
|
|
ADAM questionnaire for androgen deficiency. |
1. Do you have decrease in libido 2. Do you have a lack of energy? 3. Do you have a decrease in strength or endurance? 4. Have you lost height? 5. Have you noticed a decreased “enjoyment in life”? 6. Are you sad and/or grumpy? 7. Have you noticed a recent deterioration in your ability to play sports? 8. Are you falling asleep after dinner? 9. Has there been a recent deterioration in your work performance? If you answer yes to number 1 or 7 or if you answer yes to more than 3 questions, you may have low testosterone |
|
|
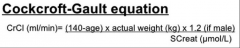
Cockcroft-gault formula. |
|
|
|
Predisposing and precipitating risk factors for depression in elderly. |
Predisposing risk factors 1. Female gender 2. Widowed or divorced 3. Previous history of depression 4. Brain changes due to vascular problems 5. Personality type, such as avoidant or dependent personality and lifelong problems developing close relationships 6. Major physical and chronic disabling illnesses 7. Taking medications, such as centrally acting antihypertensive drugs (e.g. BB, CCB, digoxin), analgesics, steroids, antiparkinsonians, benzodiazepines, and antipsychotics 8. Excessive alcohol 9. Social factors (e.g. social disadvantage and low social support) 10. Providing care to a significant other person affected by a major disease (e.g. dementia) Precipitating risk factors 1. Recent bereavement 2. Moving to an institution, such as nursing home, particularly in the first year of placement 3. Adverse life events (e.g. separation, losses, financial crisis) 4. Chronic stress associated with declining health, family, or marital problems and social isolation 5. Persistent sleep difficulties (CCSMH 2006 2.1.1) |
|
|
Screening tools for depression in cognitively intact and cognitively impaired elderly patients. |
Cognitively intact: GDS, SELFCARE self-rating scale, and the Brief Assessment Schedule for the Elderly (BASDEC). Cornell Scale for Depression in Dementia |
|
|
Which antidepressants does CCSMH recommend for treatment of MDD in the elderly? |
Citalopram Sertraline Venlafaxine Bupropion Mirtazapine |
|
|
Non-pharmacological management of weight loss assuming intake is inadequate. |
Minimize dietary restrictions Optimize energy intake (high energy foods at best meal of the day, eating smaller meals more often, eating favourite foods and snacks, providing finger foods) Optimize and vary dietary texture Avoid gas-producing foods Ensure adequate oral health Nutritional supplements Take supplements between meals Eat in company or with assistance Use flavour enhancers Participate in regular exercise Take a multivitamin Use community nutritional support services (CMAJ 2005, unintentional weight loss in elderly patients) |
|
|
What are non-modifiable risk factors of suicide in the elderly? How about modifiable risk factors? |
Non-modifiable riskfactors 1. Old age 2. Male gender 3. Being widowed or divorced 4. Previous attempt at self harm 5. Losses (e.g. health, status, role, independence,significant relations) Potentially modifiable 1. Social isolation 2. Presence of chronic painful condition 3. Abuse/misuses of alcohol or other medications 4. Presence and severity of depression 5. Presence of hopelessness and suicidal ideation 6. Access to means, especially firearms (CCSMH 2006) |
|
|
What behaviours should alert clinicians to potential suicide risk? |
1. Agitation 2. Giving personal possessions away 3. Reviewing one's will 4. Increase in alcohol consumption 5. Non-compliance with medical treatment 6. Taking unnecessary risk 7. Preoccupation with death (CCSMH 2006) |
|
|
Symptoms of bereavement complicated by coexisting MDD.
|
1. Excessive feelings of guilt not related to the deceased and self-devaluation 2. Psychomotor retardation 3. Active suicidal ideation (more than a passive wish to have died first or with the deceased) 4. Presence of mood-congruent delusions 5. Significant functional limitations impairing one’s routine daily activities beyond the first 2 months of the loss 6. Reaction out of proportion with the degree of loss (CCSMH 2006, page 20)
|
|
|
Indications for electroconvulsive therapy (ECT). |
1. Psychotic depression 2. MDD with need for rapid response 3. MDD with medical comorbidities that prevent the use of antidepressant medication 4. Previous response to ECT 5. Refractory or resistant to antidepressant therapy 6. Catatonia 7. Persistent suicidal intent 8. Bipolar depression or mania (Up-to-date: overview of ECT for adults) |
|
|
List 4 behavioural interventions that have evidence in improving sleep disorders in the elderly. |
1. Sleep hygiene 2. Stimulus control 3. Relaxation strategies 4. Sleep restriction |
|
|
List 6 features of atypical depression in the elderly. |
1. Less likely to endorse feelings of sadness and/or guilt 2. Prominent somatic complaints 3. Loss of interest, apathy common 4. Anxiety, worry 5. Cognition impairment more likely 6. Unexplained functional impairment FACADS: function, apathy, cognition, anxiety, depression (less), somatic |
|
|
Five question GDS. |
5 question GDS (2 out of 5 is considered a positive screen) 1. Are you basically satisfied with your life? 2. Do you often get bored? 3. Do you often feel hopeless? 4. Do you prefer to stay at home rather than going out and doing new things? 5. Do you feel pretty worthless the way you are now? SHHWB - satisfied, hopeless, home, worthless, bored |
|
|
What is the relative risk increase in mortality and absolute risk increase with use of antipsychotics in the elderly? |
OR 1.54, AR 1.2 (JAMA 2005) Most deaths due to cardiovascular and infectious diseases. |
|
|
Risk factors for late-life anxiety. |
Female
Recent adverse life events Chronic physical and mental health disorders Poverty Parental loss or separation Low affective support during childhood Mental health problems in parent |
|
|
6 reasons for getting neuropsychological testing. |
1. Differentiates MCI from normal aging 2. Differentiates different types of dementia 3. Differentiates dementia from mood disorder 4. Following patient with MCI or subjective cognitive concerns over time 5. Assessing changes in cognition following TBI 6. Supporting patients or their families with behavioural strategies and education about their disease (BCMJ 2011) |
|
|
Psychotherapy for depression. |
Behavioural therapy CBT Interpersonal therapy Problem solving therapy Reminiscence therapy Brief psychodynamic therapy (BCMJ 2017, and CCSMH 2006) |
|
|
Criteria for probable and possible MSA. |
Probable MSA Sporadic, progressive, adult (>30 y)- onset disease with: 1. Autonomic failure (urinary incontinence, erectile dysfunction, or orthostatic decrease of 30/15 AND 2. Poorly levodopa-responsive parkinsonism OR 3. Cerebellar syndrome Possible MSA Sporadic, progressive, adult (>30 y)- onset disease with: 1. Parkinsonism OR 2. Cerebellar syndrome AND 3. At least one feature suggesting autonomic dysfunction AND 4. At least one of the additional features of possible MSA-P or MSA-C Possible MSA-P or MSA-C 1. Babinski sign with hyperreflexia 2. Stridor Possible MSA-P 1. Rapidly progressive parkinsonism 2. Poor response to levodopa 3. Postural instability within 3 y of motor onset 4. Gait ataxia, cerebellar dysarthria, limb ataxia, or cerebellar oculomotor dysfunction 5. Dysphagia within 5 y of motor onset 6. Atrophy on MRI of putamen, middle cerebellar peduncle, pons, or cerebellum 7. Hypometabolism on FDG-PET in putamen, brainstem, or cerebellum Possible MSA-C 1. Parkinsonism (bradykinesia and rigidity) 2. Atrophy on MRI of putamen, middle cerebellar peduncle, or pons 3. Hypometabolism on FDG-PET in putamen 4. Presynaptic nigrostriatal dopaminergic denervation on SPECT or PET Second consensus statement on diagnosis of MSA. Neurology 2008. |
|
|
What proportion of Canadians will have dementia by 2038? |
2.8% (Rising tide, 2010) |
|
|
4 reasons why prevalence of dementia may be decreasing. |
Higher education Better vascular risk factor control Changes in diet Physical activity (NEJM2016: Incidence of dementia over three decades) |
|
|
Rascovsky criteria for bvFTD. |
1. Disinhibition 2. Apathy or inertia 3. Lack of empathy or sympathy 4. Perseverative, stereotyped, or compulsive/ritualistic behavior 5. Hyperorality and dietary changes 6. Neuropsychological profile: executive deficits, with relative sparing of memory and visuospatial deficits |
|
|
3 things the CCCDTD4 suggests when patient presents with RPD (time from onset of symptoms to dementia of < 1 year, or worsening of 3 points on MMSE in < 6 months) |
1. Refer to a specialist and diagnostic centre with the expertise and access to diagnostic facilities to mount an organized and comprehensive diagnostic procedure. 2. Exclude delirium and other evident underlying causes. 3. Focus diagnostic strategy on reversible causes such as infections, immune-mediated, and toxic-metabolic causes. |
|
|
According to CCCDTD4, what are reasons why you would discontinue CI in an AD patient? |
1. Patient or proxy decides to stop 2. Non-adherent, and no way of rectifying the problem 3. Rate of cognitive, functional or behavioural decline is greater on the medication than prior to starting it 4. Side effects that are definitely or probably related to the CI 5. Comorbidities of the patient make continuation of the CI too risky or futile (e.g. terminally ill) 6. Dementia is at a stage where there would be no clinically meaningful benefit (e.g. GDS stage 7) |
|
|
Components of the Frontal Assessment Battery |
1. Similarities (conceptualization) 2. Verbal fluency 3. Luria test 4. Conflicting instructions 5. Go, no-go 6. Prehension behavior (do not take my hands) |
|
|
Components of the Dementia Severity Rating Scale. |
1. Memory 2. Speech & language 3.Recognition of family members 4. Orientation to time 5. Orientation to place 6. Decision making ability 7. Social and community activity 8. Home activities and responsibilities (IADLs) 9.Personal care/cleanliness 10. Eating 11. Continence 12. Mobility |
|
|
MCI - 5 strategies to delay progression |
Cognitive training Vascular risk factor modification (BP control) Exercise Diet (Mediterranean diet) Treat comorbidities (hypothyroidism, depression) |
|
|
Five reasons we don't use CSF biomarkers. |
1. Core clinical criteria provides good diagnostic accuracy and utility in most settings 2. More research needed to ensure properly designed criteria 3. No standardized values from one locale to another 4. Not readily accessible 5. Cost effectiveness (invasive, expensive, risk of false positives) |
|
|
List the global deterioration scale. |
Stage1: No cognitive decline · Experiences no problems in daily living. Stage 2: Very mild cognitive decline · Forgets names and locations of objects. · May have trouble finding words. Stage 3: Mild cognitive decline · Has difficulty traveling to new locations. · Has difficulty handling problems at work. Stage 4: Moderate cognitive decline · Has difficulty with complex tasks (finances, shopping, planning dinner for guests). Stage 5: Moderately severe cognitive decline · Needs help to choose clothing. · Needs prompting to bathe. Stage 6: Severe cognitive decline · Loss of awareness of recent events and experiences. · Requires assistance bathing; may have a fear of bathing. · Has decreased ability to use the toilet or is incontinent. Stage 7: Very severe cognitive decline · Vocabulary becomes limited, eventually declining to single words. · Loses ability to walk and sit. · Requires help with eating. |
|
|
Contraindications to memantine. |
Severe renal impairment Severe hepatic impairment Previous allergic reaction |
|
|
What were the vascular risk factors in the CAIDE study (Arch Neurol 2005). |
Midlife obesity High total cholesterol High systolic blood pressure Were all significant risk factors for dementia, with OR of 2 for each, and they increased the risk additively (OR 6.2 for the combination) |
|
|
List two trial that show that treating HTN prevents dementia and what drug class they used |
Syst-Eur. Lancet 1998. Prevention of dementia in randomised double-blind placebo-controlled Systolic Hypertension in Europe (Syst-Eur) trial · Randomized to placebo, versus nitrendipine 10-40 mg daily, with possible addition of enalapril 5-20 mg and HCTZ 12.5 – 25 mg daily · Target was to reduce SBP by at least 20 mm Hg to reach a value below 150 mmHg. · 21 vs 11 patients (7.7 to 3.8 cases per 1000 patient-years) PROGRESS. Arch Intern Med 2003. Effects of BP lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease |
|
|
What are points to emphasize when disclosing a new diagnosis of dementia (as per CCCDTD3)? |
1. Disclosure should begin as soon as possibility of cognitive impairment is suspected 2. Consider the disclosure as opportunity for education/discussion 3. Potential for adverse psychological consequences must be assessed and addressed through education 4. Disclose the diagnosis in a manner consistent with the expressed wishes of the patient 5. Follow-up plans must be made and discussed |
|
|
What are donepezil cytochrome P450 enzymes; what are their inducers? |
CYP 3A4, 2D6. 3A4 inducers: carbamazepine, phenytoin, glucocorticoids, rifampin 2D6 inducers: dexamethasone, rifampin |
|
|
Potential FLUID biomarkers being researched for diagnosis of AD |
CSF Aβ 42 CSF tau/p-tau CSF Aβ oligomers CSF dendritic protein neurogranin (a synaptic biomarker) CSF presynaptic protein SNAP25 (Alzheimer's disease. Lancet 2016) |
|
|
Features of the cognitive impairment seen with DLB. |
1. Attentional deficits 2. Executive dysfunction 3. Visuospatial dysfunction 4. Preserved confrontation naming, and short and medium term recall as well as recognition 5. Greater impairment on verbal fluency, visual perception and performance tasks |
|
|
What neurotransmitters are affected in FTD? What meds are effective? |
Serotonin and dopamine neurotransmitter deficiencies. Antidepressants may improve behavioral symptoms in FTD, but not cognitive symptoms. Antipsychotics have also been shown to decrease NPI score. |
|
|
Differences between explicit and implicit memory. Semantic and episodic memory. |
Explicit (or declarative) memory -"knowing what". Facts and events. Refers to memories that can be consciously recalled. Further divided into semantic and episodic memory. Semantic memory - facts, meanings, concepts, and knowledge about the external world. Examples: types of food, capital cities, social customs, functions of objects, vocabulary. Episodic memory - events and experiences. Implicit (procedural) memory - "knowing how". The unconscious memory of skills and how to do things, like riding a bike, tying shoelace. |
|
|
Behaviours of dementia that are unlikely to respond to medications |
Wandering Exit-seeking behaviours Excessive noisiness Inappropriate voiding Hiding/hoarding Inappropriate undressing Eating inedible objects (BC Best Practices for accommodating and managing BPSD in residential care, 2012) |
|
|
Pressure ulcers: 4 intrinsic and 4 extrinsic risk factors. |
Intrinsic risk factors: 1. Advanced age 2. Poor nutrition 3. Vascular disease 4. Immobility 5. Incontinence Extrinsic risk factors 1. Pressure 2. Moisture 3. Shear force 4. Friction |
|
|
Preventative strategies for pressure ulcers |
1. Regular skin inspection 2. Supportive surfaces 3. Repositioning schedule 4. Nutrition 5. Staff education 6. Treat incontinence, wound drainage |
|
|
Features of failure to thrive syndrome. |
US NIA description: 1. Weight loss 2. Decreased appetite and poor nutrition 3. Inactivity 4. Dehydration 5. Depressive symptoms 6. Impaired immune function 7. Low cholesterol |
|
|
What are predictors of better outcome in patients going to rehab? |
1. Lower frailty index 2. Fewer steps to do 180 degree turn 3. Higher Functional Independence Measure (FIM) 4. Higher score on MMSE; better ability to pass clock test 5. Higher serum albumin Mnemonic: SCAFF (steps, cognition, albumin, FIM, frailty index) (Age Ageing 2012; 41:242-246) |
|
|
Protein-calorie malnutrition. 3 physical findings, 4 biochemical markers, and 5 adverse outcomes. |
3 physical findings 1. Muscle wasting 2. Edema, ascites 3. BMI 4 biochemical markers 1. Low albumin 2. Low transthyretin (prealbumin) 3. Low transferrin 4. Lymphopenia 5 adverse outcomes 1. Death 2. Infections 3. Pressure sores 4. Falls 5. Fracture (Royal College example questions) |
|
|
Reasons why a severe dementia patient may be calling out (other than pain). |
Toileting needs Delirium Agitated depression Social isolation Hunger/thirst |
|
|
Non-pharmacological management strategies for BPSD |
1. Sensory enhancement/relaxation 2. Social contact 3. Structured activities (recreational, physical) 4. Environmental modifications (reduced stimulation) 5. Training of staff, family/caregivers (BC Best Practices for accommodating and managing BPSD in residential care, 2012) |
|
|
BPSD in LTC, pharmacological options as per CCSMH. |
Psychotic features - use atypical antipsychotics Without psychotic features - can use atypical antipsychotics, trazodone, citalopram, or sertraline Sexual disinhibition - hormone therapy in men, SSRI, atypical antipsychotics FTD - trazodone, SSRI PDD or DLB - cholinesterase inhibitors as first line, and quetiapine if needed (CCSMH 2006 LTC guidelines) |
|
|
3 characteristics of cognitive impairment in NPH. |
1. Executive dysfunction 2. Psychomotor slowing 3. Apathy |
|
|
In NPH CSF tap test, how much CSF should be removed and how soon after should you reassess for improvement? What are objective measurements of improvement? |
30-50 ml
Reassess 30-60 minutes after procedure Objective measurements: -Gait speed -Stride length -Number of steps to turn 180 or 360 degrees (Up-to-date) |
|
|
Choices of dressings, based on ability to absorb exudates. |
In order of increasing absorbance Films Gauze Hydrogel Hydrocolloid Foam Alginate If infected, use silver |
|
|
Six characteristics of gait in NPH
|
1. Wide based 2. Decreased step height and stride length 3. Feet turned outwards 4. Diminished cadence 5. Slow turn with several steps 6. No response to visual or verbal cues
(Up-to-date)
|
|
|
Predictors of good response to shunt in NPH. |
1. Improvement with CSF tap test 2. Known secondary cause (SAH, meningitis, aqueductal stenosis) 3. Mild amount of cognitive impairment 4. Gait disturbance preceded mental impairment 5. Short history of mental impairment 6. Absence of substantial white matter lesions 7. B-waves during > 50% of recording time on continuous ICP monitoring |
|
|
NPH shunt complications. |
1. Overdrainage causing headache 2. Shunt failure (blockage) 3. Bleed 4. Seizure 5. Shunt infection, meningitis 6. Arrhythmia from incorrect placement or systemic emboli (particularly for ventriculoatrial shunt) |
|
|
Stages of pressure ulcer |
Stage 1: Skin intact. Non-blanchable erythema Stage 2: Partial thickness loss of dermis. Shallow open ulcer with a red/pink wound bed. May blister. No slough. Stage 3: Full thickness skin loss. No bone, tendon or muscle visible or directly palpable. May have undermining/tunneling. Stage 4: Full thickness tissue loss. Exposed bone, tendon or muscle. + slough or eschar. Often undermining/tunnelling. Unstageable: Full thickness tissue loss in which the base of the ulcer is covered by slough and/or eschar in the wound bed. Suspected deep tissue injury: purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying tissue from pressure and/or shear. |
|
|
Cochrane review of stroke unit care: what were the outcomes? |
1. Odds of death at final follow-up (OR 0.81) 2. Odds of death or institutionalized care (OR 0.78) 3. Odds of death or dependency (OR 0.79) Cochrane 2013: Organised inpatient (stroke unit) care for stroke |
|
|
CT/MRI findings that support NPH (other than ventriculomegaly). |
1. CSF flow void sign, especially in the aqueduct 2. White matter lesions, due to transependymal egress of fluid 3. Corpus callosum impingement |
|
|
6 things you would like to find out on clinical exam, when assessing someone for suitability of rehabilitation. |
1. Cognition 2. Demonstration of carry-over 3. Ability to sit 4. Ability to transfer 5. Ability to perform ADLs 6. Medical stability 7. Urinary and bowel continence (HFH admission guidelines) |
|
|
Sporadic CJD diagnostic criteria. |
University of California, San Francisco Criteria (UCSF, 2007) 1. Rapid cognitive decline 2. Two of the following six signs/symptoms a. Myoclonus b. Pyramidal/extrapyramidal dysfunction c. Visual dysfunction d. Cerebellar dysfunction e. Akinetic mutism f. Focal cortical signs (e.g. neglect, aphasia, acalculia, apraxia) 3. Typical EEG and/or MRI 4. Other investigations should not suggest an alternate diagnosis Geshwind 2015. Continuum. Prion Diseases. |
|
|
What are the neuropathological changes of chronic traumatic encephalopathy (CTE)? |
1. Tau-immunoreactive degenerative changes, distinct from other tauopathies such as AD, with preferential involvement of superficial cortical layers 2. Astrocytic tangles 3. Spindle-shaped and thread-like neurites 4. In 40% of causes, diffuse senile plaques (β-amyloid) (McKee A. J Neuropathol Exp Neurol 2009;68(7):709-735) |
|
|
Activities related to prehabilitation. |
1. Exercise 2. Nutrition interventions 3. Anxiety reduction |
|
|
What is considered a rapidly progressive dementia? |
RPD defined as a dementia that develops within 12 months after first cognitive symptoms. For individuals with AD, a decline of 3 or more points on MMSE in 6 months identifies a group with worse prognosis, and is a signal to explore co-morbid conditions and review pharmacological management. (CCCDTD4, 2012) |
|
|
Diagnostic tests for sporadic CJD. |
EEG: 1-2 Hz period sharp-wave (often biphasic or triphasic) complexes in about two-thirds of cases MRI DWI and ADC showing restricted diffusion in the cortical or deep nuclei gray matter. -Cortical ribboning: abnormal hyperintensity on FLAIR and especially DWI in the cortical gyri -Abnormal hyperintensity also in the caudate, putamen or thalamus. When striatum is involved, there is an anterior to posterior gradient of decreasing hyperintensity |
|
|
Alcohol screening tools, other than CAGE. |
1. Alcohol-Related Problems Survey (ARPS), specifically for geriatric population. 2. Alcohol Use Disorders Identification Test (AUDIT) 3. Self-Administed Michigan Alcoholism Screening Test (SMAST) |
|
|
What is considered safe amount of drinking on the Brief Alcohol Use Intervention? |
Men: < 2 drinks/day, < 7 drinks/week, < 4 drinks/occasion. Women: < 1 drink/day, < 5 drinks/week, < 3 drinks/occasion. (BCMJ 2011 Geriatric drinkers - evaluation and treatment foralcohol overuse) |
|
|
What should be assessed during driving assessments? |
1. Cognition 2. Acute or fluctuating illness 3. Neuromuscular disease or neurological affects 4. Drugs 5. Record (of accidents/violations) 6. In-car experiences (near accidents, unexplained car damage, change in driving skills, self-restriction, becoming lost, needing a copilot, etc) 7. Vision 8. Ethanol use |
|
|
What is capacity? |
In general, a capable adult must be able to understand information and appreciate the consequences of decisions. (Elder abuse practical guide 2011) In other words, the 4Cs: need to understand the context, choices, consequences, and express their wishes with consistency. |
|
|
What to assess for testamentary capacity? |
1. The nature and effect of making a will. 2. The extent of the testator’s property that may be disposed by a will. 3. The persons who are to receive the property under the will, and the moral claims of persons (such as family members and others who are close to the testator) who should receive a share of that property. 4. The way in which the assets are to be distributed under the will. (BCLI Consultation Paper on Common Law Tests of Capacity, Feb 2013, Page 25) |
|
|
What to assess for capacity of health care decision making? |
1. Condition for which health care needs to be provided to the adult 2. Nature of the health care that needs to be provided 3. Risks and benefits of receiving or not receiving the health care 4. That the information about the health care and the need for such health care applies to the situation of the adult (Martha Donnelly's slides on Incapability assessments) |
|
|
What is on the 10 minute office based dementia and driving checklist, recommended through the driving and dementia toolkit 2009? |
1. Dementia type (DLB or FTD are red flags) 2. Functional impact of the dementia/MCI 3. Family concerns (granddaughter question) 4. Visuospatial function (intersecting pentagons, clock drawing numbers) 5.Physical inability (neck turn, use of steering wheel/pedals, cardiac/neurologic issues) 6. Vision/visual fields 7. Drugs 8. Trailmaking A&B tests (>3 minutes or ≥ 3 errors on the Trails B test is unsafe) 9. Ruler drop reaction time test (12” ruler, normal is catch at 6-9”) 10. Judgment/insight |
|
|
What is the likelihood of survival after CPR in elderly? |
Pooled survival to discharge after in-hospital CPR was 70-79 yo: 18.7% 80-89 yo: 15.4% 90+: 11.6% Of those who survive and are older than 80, only 20% were able to return to independent functioning outside institutionalized care. At 1 year follow-up, the survival rate is somewhere between 7 - 21% (Myke S. Age Ageing 2014;43:456-463) |
|
|
Tri-council policy statement. What are the 3 conditions that must be met for a patient with dementia lacking capacity for consent to be included in a clinical trial? |
1. The research question can be addressed only with participants within the identified group; and 2. The research does not expose the participants to more than minimal risk without the prospect of direct benefits for them; or 3. Where the research entails only minimal risk, it should at least have the prospect of providing benefits to participants or to a group that is the focus of the research and to which the participants belong. Source: http://www.pre.ethics.gc.ca/eng/policy-politique/initiatives/tcps2-eptc2/chapter4-chapitre4/, article 4.6 |
|
|
Indicators of physical abuse in elderly. |
Bruises, black eyes Welts, rope marks Swelling Broken assistive devices Lacerations Punctures Untreated injuries in various stages of healing Fractures, sprains, dislocations |
|
|
Indicators of financial abuse in the elderly. |
Unpaid bills Sudden change in lifestyle and living conditions No money for basic necessities Absence of aids, medications, services Refusing to spend money without permission of caregiver Sudden appearance of previously uninvolved relatives Abrupt changes in wills/accounts Forged signature Sudden sale or change in property title |
|
|
Diagnostic criteria for restless legs syndrome. |
1. Urge to move legs with/without uncomfortable and unpleasant sensation in the legs 2. Worse with inactivity 3. Better with activity 4. Worse towards the evening/night 5. Not accounted for by symptoms of another medical or behavioural condition |
|
|
Order in which Parkinson's treatment drugs should be discontinued if patient experiencing psychosis. |
Anticholinergics, amantadine, DA, MAO-B and COMT inhibitors, and lastly, reduce levodopa.
(Canadian consensus guidelines 2012) |
|
|
What is the clinical presentation of Paget's disease of the bone? disease markers? indications for treatment? treatment? |
Presentation: bone pain, bone deformity, warmth over bone. Rarer presentations include deafness, hydrocephalus, high output HF, osteosarcoma. Disease markers: ALP, P1NP Indications for treatment: symptomatic. In asymptomatic patients, if skull, spine or long bone affected, or disease close to a major joint. Treatment: alendronate 40 mg daily x 6 months, risedronate 30 mg daily x 2 months, or zoledronate 5 mg IV x 1 |
|
|
Three most common types of tremor. |
Resting tremor (PD)
Kinetic tremor (cerebellar) Postural tremor (ET) |
|
|
What are medication options for treatment of essential tremor? |
Propanolol Primidone Botox injection Benzodiazepines |
|
|
Non-pharmacological methods of managing freezing gait in Parkinson's patient. |
Shifting weight
Wider turns Concentrating on taking a bigger step forward Laser or L-shaped cane Auditory cue (e.g. singing to a beat) |
|
|
Reasons for disturbed sleep in Parkinson's patient. |
Motor symptoms (tremor, difficulty turning over) Nocturia Pain Depression Daytime somnolence RLS PLMS Hallucinations Nightmares |
|
|
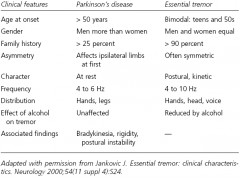
6 differentiating features between essential tremor and Parkinson's disease |
|
|
|
10 non-motor findings in PD. |
Constipation OH Urinary incontinence Pain Dementia Depression Psychosis REMSBD RLS Fatigue Olfactory dysfunction |
|
|
3 principles of non-surgical management of proximal humerus fractures. |
Immobilization in sling Ice Analgesics |
|
|
Other conditions associated with RLS |
Iron-deficiency
Pregnancy CKD Alpha-synucleinopathies (MSA, PD, DLB) MDD, GAD, panic disorder, ADHD |
|
|
In which 3 situations would you want to check the vitamin D level according to Canadian osteoporosis guidelines? |
Recurrent fractures despite pharmacologic therapy. Bone loss despite osteoporosis treatment. Comorbid conditions that affect vitamin D absorption or action. |
|
|
4 factors that increase the risk for osteonecrosis of the jaw. |
Periodontitis Smoking Glucocorticoid use Diabetes Bisphosphonates (used in oncology settings) |
|
|
5 things to check when someone fractures on osteoporosis treatment. |
1. Compliance 2. Taking properly? 3. 25-OH-D levels 4. Calcium untake 5. Secondary causes - SPEP, pathological fracture? |
|
|
Contraindications to teriparatide other than allergy. |
Hypercalcemia Primary or secondary hyperparathyroidism Increased risk of osteosarcoma (Paget's disease of bone, history of prior RT) Severe renal insufficiency |
|
|
Osteomalacia, what would show on histology of bone biopsy? |
Prolonged mineralization lag time Widened osteoid seams Increased osteoid volume |
|
|
Ocular findings of Parkinson's disease (4). |
Hypometric saccades Impaired vestibuloocular reflex Impaired upward gaze and convergence Eyelid opening apraxia |
|
|
Osteoporosis. 8 major and 8 minor risk factors. |
Major RF: i. Age ≥ 65 ii. Vertebral compression fracture iii. Fragility fracture after age 40 iv. Family history of osteoporotic fracture v. Systemic steroids > 3 months vi. Malabsorption syndrome vii. Primary hyperparathyroidism viii. Propensity to fall ix. Osteopenia on x-ray x. Hypogonadism xi. Early menopause (before age 45) Minor RF: i. RA ii. Past history of clinical hyperthyroidism iii. Chronic anticonvulsant use iv. Low dietary calcium intake v. Smoker vi. Excess alcohol intake vii. Excess caffeine viii. Weight < 57 kg ix. Weight loss 10% of weight at age 25 x. Chronic heparin use |
|
|
Name 4 major sleep disorders in PD patients. |
Insomnia Excessive daytime somnolence REMSBD RLS |
|
|
Features to differentiate vascular parkinsonism from idiopathic PD. |
Vascular parkinsonism: 1. Presents with postural instability and falls 2. Wider base of stance 3. Absence of festination 4. Pyramidal signs 5. Early subcortical dementia 6. Poor or non-sustained response to levodopa 7. Greater involvement of legs |
|
|
Osteoporosis - additional factors that warrant pharmacological treatment in moderate risk patients |
1. Additional vertebral fracture(s) (>25% height loss with end-plate disruption). 2. Previous wrist fracture in individuals older than age 65 or those with T-score ≤ -2.5. 3. Lumbar spine T-score much lower than femoral neck T-score. 4. Rapid bone loss. 5. Men on androgen deprivation therapy for prostate cancer. 6. Women on aromatase inhibitor therapy for breast cancer. 7. Long-term or repeated systemic glucocorticoid use (oral or parenteral) that does not meet the conventional criteria for recent prolonged systemic glucocorticoid use. 8. Recurrent falls defined as falling 2 or more times in the past 12 months. 9. Other disorders strongly associated with osteoporosis, rapid bone loss or fractures. |
|
|
Benefits of exercise in elderly, and contraindications to exercise. |
Benefits: 1. Blood pressure improvements 2. Reduced pain from OA 3. COPD symptoms and functional capacity 4. Cognition 5. Decreases falls 6. Decreases cardiovascular disease 7. Decreases depressive symptoms Contraindications: 1. UA 2. Severe VHD 3. End stage CHF 4. Severe AS 5. BP > 200/110 6. Large or expanding aortic aneurysm 7. Known cerebral aneurysm or recent intracranial bleed 8. Uncontrolled or end-stage systemic disease 9. Acute retinal hemorrhage or recent ophthalmologic surgery 10. Acute or unstable MSK injury 11. Severe dementia or behavioural disturbance |
|
|
3 adverse outcomes of low gait speed. |
Falls Institutionalization Mortality Poor post-operative function |
|
|
Describe the Fried frailty model.
|
1. Weight loss (≥ 5% of body weight in last year) 2. Exhaustion (positive response to questions) 3. Weakness (decreased grip strength) 4. Slow walking speed (> 6-7 seconds to walk 15 feet) 5. Decreased physical activity (Kcals spent per week: males expending <383 Kcals and females < 270 Kcals) |
|
|
5 ACE principles, and 5 positive outcomes from ACE units. |
ACE principles: 1. Early rehabilitation 2. Enhanced discharge planning 3. Frequent medical review 4. Patient-centred care 5. Prepared environment Outcomes: 1. Decreased hospital cost 2. Decreased LOS 3. Increased discharge home 4. Decreased functional decline 5. Decreased delirium 6. Decreased falls |
|
|
In "NORFOLK" study, what four lifestyle behaviours lead to longer life? |
Healthy living with these behaviours can add 14 years of life: 1. Not smoking 2. Exercising 3. Eating fruits and vegetables 4. Drinking alcohol moderately |
|
|
Name a screening tool that is used in the ER for predicting outcomes in the elderly. |
Triage Risk Screening Tool (TRST) |
|
|
Things to observe for during swallowing test in oral and pharyngeal phases. |
Oral phase 1. Chewing 2. Food retained in cheek pouches 3. Tongue movement 4. Saliva 5. Bolus formation 6. Drooling Pharyngeal phase 1. Soft palate elevation 2. Vocal folds close 3. Hyoid bone and larynx pull upward and forward 4. Epiglottis tilts backward 5. Coughing 6. Change in voice quality 7. Pharyngeal clearance |
|
|
Complications of dysphagia. |
1. Malnutrition 2. Dehydration 3. Aspiration 4. Social interaction 5. Airway obstruction |
|
|
Indications for home visit from geriatrician. |
1. Patient has severe mobility disability 2. High risk of falls where environment assessment required 3. Severe and disruptive behaviour problem making clinic visit problematic 4. End-stage terminal illness 5. No access to transportation 6. Refuse to come into clinic but willing to be seen in home |
|
|
Ideal criteria for admission to geriatric day hospital |
1. At risk of losing independence 2. Few supports at home (social frailty) 3. Caregivers with caregiver burnout 4. Need for multidisciplinary support 5. Motivated to participate |
|
|
What are positive outcomes for CGA in hospital setting? |
1. Less likely to live in LTC 3. Cognition (BMJ 2011) |
|
|
10 features of an elder friendly hospital.
|
1. Favourable physical environment 2. Zero tolerance for ageism throughout the organization 3. ACE unit for patients above a certain age 4. Informed and shared decision-making 5. Fostering links between the hospital and the community 6. Focus on delirium management 7. Comanagement for patients in ortho, oncology, cardiac surgery 8. Comprehensive nutrition support program 9. Elder-assist program to navigate hospital services and appointments 10. Specialized unit for management of patients with BPSD
(CGJ “Moving Towards the Age-friendly Hosptial” by Huang 2011) |
|
|
Three other settings where ACE principles have been adopted. |
1. Orthopedics 2. Oncology 3. Stroke |
|
|
Two quick physical performance measures that are independently predictive of mortality. |
Gait speed Grip speed |
|
|
Three limitations of the timed up and go test |
1. Only looks at recorded time, not the patient's movements 2. Can't be performed in small areas 3. Footwear and assistive devices may alter test results unpredictably 4. Chair may alter test results unpredictably 5. Three meters may not be long enough |
|
|
Three types of elder abuse |
Financial
Physical Psychological |
|
|
Eight risk factors for elder abuse |
1. Advanced age 2. Female 3. African American / Hispanic 4. Social isolation 5. Cognitive impairment 6. Physical impairment 7. Poor mental health of caregiver 8. Substance abuse |
|
|
Seven reasons why feeding tubes are not recommended in advanced dementia. |
1. Does not prevent aspiration 2. Does not prevent complications of malnutrition 3. Does not prolong survival 4. Does not reduce risk of pressure sores or infx 5. Does not improve function 6. Does not improve comfort 7. Adverse effects of tube feeding including aspiration pneumonia, leaking, tube occlusion, and infection |
|
|
Negative outcomes of frailty. |
Falls, institutionalization, death, disability. |
|
|
On the Clinical Frailty Scale, each 1 category increment increases the ... |
Risk of death by 21.2% within 70 months, and entry into institution by 23.9% |
|
|
Indicators of psychological abuse. |
Agitation Fearfulness (especially in presence of caregiver) Low self-esteem Sleep disturbance Withdrawal Deference to caregiver |
|
|
Three reasons for increase of resistant microorganisms in LTC. |
1. Transfer of patients from acute care to LTC 2. Excess use of antibiotics 3. Inadequate infection control precautions, facilitating spread 4. Risk factors for colonization/infection (percutaneous gastrostomy tubes, pressure ulcers, malnutrition, immunosuppression) |
|
|
Findings of acute ischemic limb, versus chronic PVD. |
Acute: paresthesia, poikilothermia, paralysis, pulselessness, pallor, pain. Chronic: lack of hair, thickened nails, shiny atrophic skin, ulcers, bruits/pulseless. |
|
|
Complications of ORIF and hemiarthroplasty. |
Infection Bleeding VTE Delirium Dislocation Non-union Chronic pain |
|
|
Four characteristics of gout in older adults that are different than the classic presentation in younger patients. |
1. Women are equally represented 2. Polyarticular 3. Upper extremities more often 4. Increased tophi |
|
|
3 relative contraindications for colchicine in the elderly. |
1. Severe hepatic impairment 2. Severe renal impairment 3. Concurrent use of CYP 3A4 inhibitor, in setting of hepatic or renal impairment |
|
|
Five age-associated changes leading to diastolic dysfunction. |
1. Increased collagen and structural changes in elastin 2. Prolonged availability of intracellular calcium causes persistent activation of contractile filaments 3. Increased vascular stiffness causes prolonged contraction time 4. Increased afterload leads to LVH 5. CAD |
|
|
Risk factors for peripheral arterial disease. |
Age Smoking Diabetes HTN Dyslipidemia |
|
|
Contraindications to kyphoplasty. |
1. Fractures secondary to tumour or infection 2. Loss of integrity of posterior vertebral cortex 3. Coagulopathy 4. Complete vertebral collapse |
|
|
As medical director of a LTC, actions for flu prevention. |
1. Handwashing protocol 2. Patient, family and staff education 3. Immunization program for staff and residents 4. Rapid confirmation of suspected cases 5. Isolation of suspected and confirmed cases |
|
|
Six reasons for persistent pain after TKA. |
1. Patellofemoral instability 2. Patellar component loosening 3. Patella fracture 4. Extensor mechanism rupture (quadriceps or patellar tendon) 5. Periprosthetic fracture 6. Polyethylene wear |
|
|
Three steps to establish that an Influenza outbreak has occurred at a LTC facility. Six steps to contain and manage the outbreak. |
Determining an outbreak has occurred
1. Assess suspected cases, including obtaining specimens. 2. Establish a case description. 3. Begin a line-list. Managing outbreak: 1. General infection control measures 2. Declare outbreak and notify local Medical Officer of Health 3. Notify other appropriate individuals 4. Identify new cases by surveillance of symptoms, obtaining specimens 5. Treatment and prophylaxis (antiviral) 6. Communications to residents, family, staff, volunteers |
|
|
What is arterial compliance? |
Index of elasticity of the arterial wall. |
|
|
Three surgical options for OA.
|
1. Debridement 2. Total joint arthroplasty 3. Joint resurfacing |
|
|
Five most cost-effective tests for evaluating syncope in the older adult. |
1. Postural BP 2. Telemetry 3. ECG 4. Echocardiogram 5. Cardiac stress test |
|
|
Three physiological causes of anemia |
1. Decreased erythropoietin level (from decline in renal function) 2. Proinflammatory cytokines with age (IL-6) 3. Decrease in androgens |
|
|
Five clinical features that increase likelihood of lumbar spinal stenosis. |
1. Absence of pain while seated 2. Improvement of pain when bending forward 3. Presence of bilateral buttock or leg pain 4. Wide-based gait 5. Abnormal Romberg (JAMA 2010 RCE on lumbar spinal stenosis) |
|
|
How to give pneumococcal vaccine in the elderly. |
If patient never received pneumovax before, then give prevnar 13 followed by pnuemovax 23 8 weeks later. If patient has already received pneumovax, then prevnar 13 should be given 1 year later. |
|
|
Treatment of serotonin syndrome |
Remove offending agents Sedation with benzodiazepines Supportive care (fluids, O2, monitoring) Anti-serotonergic agent (cyproheptadine) |
|
|
Adverse drug reaction vs adverse drug event. |
Adversedrug reaction (ADR) = noxious response to drugs used in usual doses for treatment/prevention. Adverse drug event (ADE) = any injury that occurs from a drug, including noxious responses but also drug administration error. |
|
|
Treatment of herpes zoster. |
Valacyclovir 1 g TID x 7 days |
|
|
What is the definition of validity, and the three types of validity? |
Validity: The extent to which an observation reflects the “truth” of the phenomenon being measured. Three types of validity 1. Content validity: does a test measure all dimensions of a particular problem? 2. Construct validity: is the measure affirmed by an external established indicator? 3. Criterion validity: does the test predict an observable phenomenon. That is, does the test relate to the real world? (Uptodate: Glossary of common biostatistical and epidemiological terms) |
|
|
2 characteristics of the palmomental reflex that suggest it to be pathological. |
Strong, sustained and easily repeatable contraction. Can be elicited by stimulation of areas other than the palm. |
|
|
Two screening tests for hearing impairment. |
Whispered voice test.
Tone-emitting otoscope. |
|
|
Define health adjusted life expectancy. |
Average number of years that an individual is expected to live in a healthy state |
|
|
What are 5 changes in aging / disease processes that may cause nocturnal polyuria? |
1. Decreased diurnal variation in ADH 2. Redistribution of peripheral edema due to diastolic dysfunction 3. Autonomic neuropathy 4. Chronic kidney disease 5. Obstructive sleep apnea |
|
|
Two pathological features of wet AMD. |
Neovascularization Growth into subretinal space, as opposed to drusen in the RPE |
|
|
Define presbycusis and name three types. |
Age-related hearing loss. It is a true sensorineural hearing loss. Three main types: 1. Sensory, characterized by loss of hair cells and a high-frequency hearing deficit. 2. Metabolic, characterized by loss of stria vascularis, and a low-frequency hearing deficit. 3. Neural, characterized by loss of ganglion cells and a variable pattern of hearing loss. |
|
|
Three differences between QA and QI. |
1. In QA, a cut‐off point is set that demarcates the border between acceptable and unacceptable quality whereas in QI the aim is to improve quality overall by reducing unnecessary variation and focusing on what happens most often rather than what happens relatively rarely. 2. In QA, outliers, that fall below the cut‐off point (and thus are deemed undesirable) are removed but QI strives to improve the system and its processes rather than trying to eliminate an outlier event and therefore thrives in learning environments. 3. In QA, statistically the remaining points tend to automatically redistribute into a bell‐shaped curve over time and thus outlying points reappear below the cut‐off point. |
|
|
Process measures versus outcome measures. |
Process measures = what a provider does to maintain or improve health. E.g. the percentage of people with diabetes who had their blood sugar tested and controlled. Outcome measures = the impact of the intervention on the health status of the patients. E.g. rate of surgical complications or hospital-acquired infections. |
|
|
How does GERD present differently in the elderly? |
Likely to have complications, such as dysphagia due to strictures, Barrett's, hemorrhagic esophagitis, recurrent aspiration. May also mimic angina. |
|
|
Pathophysiology of HIV-associated neurocognitive disorders. |
1. Virus enters via monocytes that go across BBB. 2. Macrophages and microglial cells are key in pathogenesis. 3. HIV infects astrocytes. 4. Macrophage/microglial cells and altered cytokine/chemokine production lead to abnormal neuronal pruning. |
|
|
Three medication classes that lead to an increase in ER visits. |
1. NSAIDs including aspirin 2. Diuretics 3. Warfarin (STOPP and START) |
|
|
What are two good nutritional screening questionnaires/tools? |
1. Simplified Nutritional Assessment Questionnaire (SNAQ) 2. Mini-nutritional assessment (MNA) 3. Malnutrition universal screening tool (MUST) |
|
|
Three normal changes to skin with aging, and the clinical consequences. |
1. Dryness – pruritus 2. Reduced response of eccrine sweat glands – overheating 3. Loss of melanin – increased susceptibility to damage and cancer |
|
|
List the 5 Choosing Wisely Canada Geriatrics points.
|
1. Don’t use antimicrobials to treat bacteriuria unless specific symptoms are present 2. Don’t use benzodiazepines or other sedative-hypnotics as first choice for insomnia, agitation, or delirium 3. Don’t recommend percutaneous feeding tubes in advanced dementia 4. Don’t use antipsychotics as first choice for BPSD 5. Avoid medications known to cause hypoglycemia to achieve A1C < 7.5%. Moderate control is generally better. |
|
|
Four common adverse effects of trazodone. |
1. Sedation 2. Headache 3. Dizziness 4. Dry mouth (Lexicomp) |
|
|
Diagnostic maneuvers for BBPV. Therapeutic repositioning maneuvers. |
Diagnostic: 1. Dix-Hallpike 2. Side-lying test 3. Supine Head Roll test Repositioning maneuvers 1. Epley 2. Semont 3. Brandt-Daroff |
|
|
What is considered end-stage heart failure? |
1. Repeated ≥2 HF hospitalizations in the last year 2. Progressive deterioration in renal function 3. Weight loss (cardiac cachexia) 4. Intolerance of ACEi because of hypotension or renal function 5. Intolerance of BB because of HF, hypotension 6. Persistent dyspnea with activities such as dressing, or bathing 7. Inability to walk one block on level ground 8. Need to escalate diuretics to maintain volume status; often furosemide > 160 mg, and/or need metolazone 9. Progressive decline in sodium < 133 10. Frequent ICD shocks 1 year mortality of 75%, no survival at 2 years (J of Cardiac Failure 2015) |
|
|
How should physical activity be prescribed to patients? |
Multicomponent exercise program 1. Strength and balance training twice weekly 2. 150 mins or more of moderate intensity aerobic exercise weekly, in bouts of 10 minutes or more (CGS CME Journal 2016) |
|
|
What are some tools/questionnaires to find out how active patients are? |
1. International Physical Activity Questionnaire (IPAQ) 2. Rapid Assessment of Physical Activity (RAPA) (CGS CME Journal 2016) |
|
|
What is the 4D AID approach to orthostatic hypotension? |
4D (causes associated with compensatory tachycardia) 1. Drugs (6 anti's - hypertensives, anginals, parkinson, depressants, psychotics, BPH) 2. Dehydration 3. Deconditioning 4. Dysfunctional heart (low EF, aortic stenosis) AID (causes associated with lack of compensatory tachycardia) 1. Autonomic dysfunction (B12, thyroid, DM, amyloidosis, EtOH abuse, parkinsonism) 2. Idiopathic (Bradbury-Eggleston) 3. Drugs (beta-blockers) (CGS CME Journal 2016) |
|
|
How to prescribe sleep restriction therapy. |
Step 1: sleep log x 2-3 weeks Step 2: calculate total sleep time average (TST) Step 3: prescribe time in bed (TIB) = TST average Step 4: qweekly, increased TIB by 15-20 minutes when sleep efficiency > 85%. Wake-up time is fixed. Bedtime should be no later than 2 am. (CGS CME Journal 2016) |
|
|
Recommended approach to BPSD by the CME Journal |
4 "izes or ises" 1. Temporize. Don't rush. R/o delirium. Ask caregiver to keep a diary of behaviours. 2. Optimize. Try ChEI and memantine. 3. Improvise. Try non-pharmacological strategies. Try antidepressants. 4. Compromise. If all else fails, try low dose risperidone, olanzapine, or aripiprazole. (CGS CME Journal 2016) |
|
|
Clinical manifestations of B12 deficiency.
|
1. Cognitive impairment 2. Peripheral neuropathy 3. Glossitis 4. Macrocytic anemia 5. Subacute combined degeneration 6. Depression |
|
|
What were the relevant outcomes from the FRAME study (NEJM 2016) |
Romosozumab study.
Lower vertebral fractures at 12 months, RR 0.27, and after transition to denosumab, at 24 months. Lower clinical fractures (clinical vertebral and non-vertebral), HR 0.64 No significant difference in non-vertebral fractures, but this may have been due to inclusion of Latin American geographical region, that had lower than expected rates of non-vertebral fractures. |
|
|
What did the DOMINO trial show (NEJM 2012)? |
295 patients, moderate to severe dementia, with donepezil for at least 3 months were randomized to: Continue donepezil Discontinue donepezil Discontinue donepezil and start memantine Continue donepezil and add memantine Both donepezil and memantine were associated with cognitive and functional benefits at 1 year, but there was no additive benefit of combined therapy. |
|
|
Five physiological changes to explain sarcopenia.
|
1. Decreased fast-twitch (type II) fibres 2. Decrease in GH levels 3. Decrease in IGF-1 levels 4. Change in sex hormones 5. Increase in cytokine levels (IL-6, TNF-alpha) |
|
|
Three advantages and three disadvantages of lamotrigine |
Advantages 1. Well tolerated 2. Few drug interactions 3. No monitoring Disadvantages 1. Slow titration 2. Risk of SJS 3. Frequent rash |
|
|
The six cognitive domains on DSM 5, and two sub-domains of each. |
Complex attention -Sustained attention -Divided attention Executive function -Decision making -Planning Learning and memory -immediate memory span -recent memory Language -expressive language -receptive language Perceptual-motor -visual perception -praxis -gnosis Social cognition -recognition of emotions -theory of mind |
|
|
Describe the PIECES approach to management of BPSD. |
1. Physical - pain and physical conditions. 2. Intellectual - understand losses from dementia (amnesia, aphasia, apathy, agnosia, apraxia, anosognosia, altered perception). 3. Emotional - consider adjustment disorder, depression, personality disorder, delusions. 4. Capabilities - ADL/IADLs. 5. Environment - consider over/understimulation. 6. Social - consider social network, life story, culture. |
|
|
Define crystallized and fluid intelligence, and describe changes you may see in normal aging. |
Fluid intelligence is the ability to solve new problems without any previous training. -declines in normal aging -due to decreased processing speed, attention, executive function Crystallized intelligence is the amount of knowledge and information that one brings to the testing situation -stable, or increases through life -e.g. school-based knowledge, vocabulary, reading |
|
|
Three physiological changes in normal aging that predispose older adults to constipation |
1. Delayed colonic transit time. 2. Decreased number of high amplitude propagated contractions. 3. Higher sensory threshold to rectal distention. |
|
|
Canadian Diabetes Association recommendations for elderly. |
1. Healthy elderly should target same glycemic, BP and lipid targets as younger people. 2. In the frail elderly, target A1C < or = 8.5%, and FPG 5-12. 3. Elderly with T2DM should do exercise 4. Caution with sulphonylureas. Start at half the dose. 5. Caution with thiazolidinediones, due to fracture and HF. 6. Clock draw test may be done to predict who will have trouble with insulin management. |
|
|
Five predictors of poor rapid motor progression in Parkinson's disease.
|
1. Older age 2. Rigidity/hypokinesia as initial symptom 3. Comorbid stroke, auditory deficits, visual impairments 4. Postural instability/gait difficulty (PIGD) 5. Male CROMP |
|
|
Types of reliability (in research). |
1. Test-retest 2. Inter-rater 3. Parallel forms (administering different versions of an assessment tool to same group of individuals) |
|
|
Four mechanisms by which OA predisposes to falls. |
Pain Gait and balance disorder Reduced muscle strength Neurological entrapment |
|
|
What are essential elements of person-centered care, other than involving the patient/family? |
1. Individualized, goal-oriented care plan based on person's preferences 2. Ongoing review of the person's goals and care plan 3. Support by an interprofessional team 4. One primary or lead point of contact on the healthcare team 5. Continual information sharing and integrated communication JAGS 2016; 64(1) |
|
|
Define apraxia and agnosia. |
Apraxia: inability to carry out purposeful, voluntary movements in the absence of motor and sensory deficit. Agnosia: inability to process sensory information. |
|
|
What proportion of newly diagnosed HIV patients are over the age of 50? |
10% (Canada Public Health website) |
|
|
Ten strategies for caregivers to deal with wandering.
|
1. Look for triggers for wandering (pain, toileting needs) 2. Keep objects associated with outdoors (keys, jackets, shoes) out of view 3. Re-locate door locks above eye level 4. Door alarm 5. Door mats that set off alarm 6. Review medications 7. Physical activity 8. Tell neighbors, nearby businesses, local police about the situation 9. Identification bracelet 10. Disguise the doors
|
|
|
Barriers to interpretation of PFTs in older adults |
1. Poor effort 2. Cognitive impairment 3. Predicted values may be based on younger patients 4. Decline in height may affect predicted values 5. Can't hear instructions 6. Can't form tight seal with lips |
|
|
Probable corticobasal syndrome criteria. |
Asymmetric presentation of 2 of: 1. Limb rigidity or akinesia 2. Limb dystonia 3. Limb myoclonus Plus 2 of: 1. Orobuccal or limb apraxia 2. Cortical sensory deficit 3. Alien limb phenomenon |
|
|
What is the relative risk reduction for falls with vitamin D (JAMA 2004)? |
OR 0.78, 95% CI 0.64-0.92 |
|
|
How does vitamin D prevent falls? |
1,25-hydroxy-D binds to highly specific nuclear receptor in muscle, leading to improved muscle function. |
|
|
Age-related reasons of why elderly are prone to orthostatic hypotension. |
Reduction of renin, angiotensin, aldosterone Increased natriuretic peptides Decline in thirst reflex Decline in baroreceptor reflex Decreased cardiac compliance |
|
|
What percentage of Canadians will be > 65 yo by 2024? |
In 2015, 16.1% are > 65. By 2024, it is estimated that 20.1% will be > 65. (Stat Canada) |
|
|
PSP diagnostic probable, and supportive criteria (NINDS-SPSP) |
Mandatory inclusion criteria, Probable: 1. Gradually progressive disorder 2. Onset at age 40 or later 3. Vertical gaze palsy AND prominent postural instability with tendency to fall in the first year of disease onset 4. No evidence of other diseases that could explain the features Supportive criteria 1. Symmetric akinesia or rigidity, proximal > distal 2. Abnormal neck posture, especially retrocollis 3. Poor or absence response to levodopa 4. Early dysphagia and dysarthria 5. Early onset of cognitive impairment, including at least 2 of: apathy, impaired abstract though, decreased verbal fluency, utilization or imitation behaviour, or frontal release signs |
|
|
What is the recommended measures to improve dementia care in the National Dementia strategies? |
1. Accelerated investment in dementia research 2. Recognition of importance of informal caregivers 3. Increased recognition of importance of prevention and early intervention 4. Greater integration of care, and increased use of chronic disease prevention 5. Strengthen Canada's workforce |
|
|
What are features of Korsakoff syndrome? |
Anterograde amnesia
Retrograde amnesia Confabulation Apathy Lack of insight |
|
|
What is the classification of traumatic brain injuries? |
Mild TBI: GCS 13-15 Moderate TBI: GCS 9-12 Severe TBI: GCS <= 8 AD risk is increased in moderate TBI by 2.3x, and in severe TBI by 4.5x |