Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
How many cases of IBD are there in the US? UC vs CD?
|
> 1 million
50% UC and 50% CD |
|
|
How many new cases of IBD are there per year? How many total cases of IBD are there / 100,000?
|
- New cases: 10 / 100,000 / year
- Total cases: >200 / 100,000 in the West |
|
|
What is the long-term outlook of IBD?
|
- Chronic, lifelong disease without medical cure
- Surgery often necessary |
|
|
Where are the highest incidences of IBD in the world?
|
- US
- Canada - Europe |
|
|
What part of the GI tract is affected by Ulcerative Colitis? Pattern?
|
- Continuous inflammation
- Colon only, superficially affects mucosa, lamina propria, and submucosa - Starts at rectum and works its way proximally |
|
|
What is the clinical presentation of Ulcerative Colitis?
|
- Diarrhea (bloody w/ mucus)
- Abdominal pain and tenderness - Loss of appetite and weight - Fever - Fatigue - Urgency for BM - Children: growth and developmental failure |
|
|
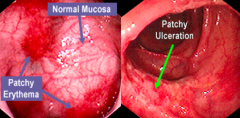
What findings are there of Ulcerative Colitis on endoscopy?
|
- Erythema
- Loss of usual fine vascular pattern - Granularity of mucosa - Friability - Edema - Pseudopolyps - Erosions and ulcers - Spontaneous bleeding - Cecal patch - Backwash ileitis |
|
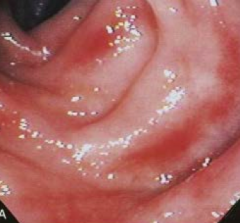
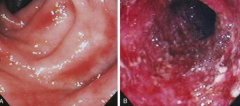
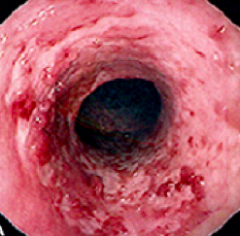
What does this endoscopy show?
|
- Mild ulcerative colitis with loss of vascular pattern
- Hard to see the blood vessels - Some whitening = accumulation of immune cells |
|
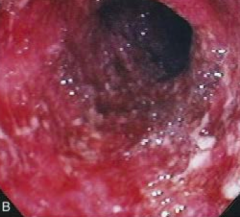
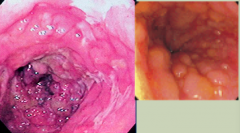
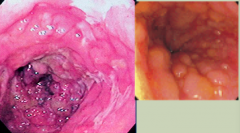
What does this endoscopy show?
|
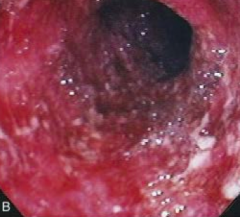
Severe ulcerative colitis
- Spontaneous bleeding and friability - Occult blood leaking in from bowel - White blobs are mucus, neutrophils, macrophages, and lymphocytes leaking into lumen |
|
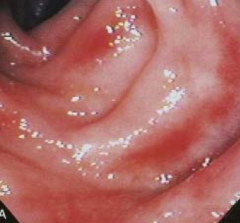
What does this endoscopy show?
|

Ulcerative Colitis
- Erythematous - Friable - Loss of vascular pattern - Also notice continuous and circumferential pattern |
|

What does this endoscopy show?
|

Ulcerative Colitis
- Inflammatory pseudopolyp - outpouching of inflammatory cells predominantly seen in UC - Large population of goblet cells covers the pseudopolyps with mucous |
|

What does this endoscopy show?
|
Ulcerative Colitis
- Lots of Pseudopolyps decreasing the size of the lumen |
|
|
What is the remission rate of Ulcerative Colitis?
|
Around 40% no matter how many years after diagnosis
|
|
|
What are the potential outcomes of Ulcerative Colitis over time?
|
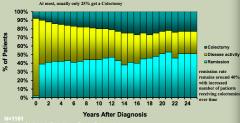
- Colectomy (up to 20%)
- Disease activity persists (30-50%) - Remission (~40%) |
|
|
What are the possible disease severities in Ulcerative Colitis? How common?
|
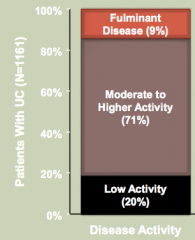
- Low activity (20%)
- Moderate to Higher activity (71%) - Fulminant disease (9%) Activity = patients presenting with symptoms of their disease (diarrhea, pain, etc) |
|
|
What is meant by Fulminant Colitis?
|
Severe UC, with:
- Fever, elevated WBC count, and unstable vitals - High risk of perforation |
|
|
How do you diagnose Fulminant Colitis?
|
- Usually full colonoscopy not necessary
- Flex sig only to rule out other causes such as C. difficile and take biopsies - Otherwise based on presence of fever, elevated WBC count, and unstable vitals |
|
|
What part of the GI tract is affected by Crohn's Disease? Pattern?
|
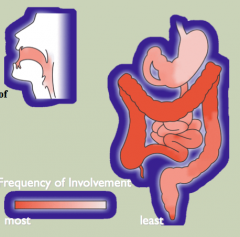
- Patchy inflammation
- Mouth to anus involvement - Full-thickness inflammation (all layers of the bowel wall) |
|
|
What are the characteristics that indicate Crohn's Disease?
|
- Variable involvement
- "Cobblestone" appearance - Fistulae - Strictures |
|
|
What is the most common location to be affected by Crohn's Disease?
|
Ileocecal area
|
|
|
How common is Crohn's Disease that only affects the small intestine? Only the large intestine? Both small and large intestine?
|
- Small intestine: 30%
- Large intestine: 20-25% - Small AND Large intestine: ~50% (remember UC always only affects the large intestine) |
|
|
What is the typical clinical presentation of Crohn's Disease?
|
Usually in pediatric population (<18 years):
- Abdominal pain - Diarrhea and occasionally rectal bleeding (bleeding less common in CD) - Weight loss - Anorexia (failure to thrive) - Vomiting - Stunted growth - Fevers |
|
|
How does Crohn's Disease that presents in an adult differ from that which presents in a pediatric patient?
|
- Similar symptoms
- Growth and development issues less apparent - Often had silent disease as a child / teen |
|
|
What are the three major endoscopic findings that are specific for Crohn's Disease?
|
- Aphthous ulcers (looks like a canker sore)
- Cobble-stone appearance - Discontinuous lesions |
|
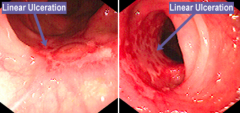
What does this endoscopy show?
|
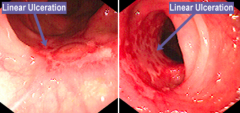
Crohn's Disease with linear ulcerations
|
|
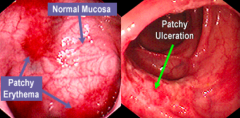
What does this endoscopy show?
|
Crohn's Disease: skip lesions (areas of inflammation are adjacent to normal mucosa)
|
|
What does this endoscopy show?
|
Crohn's Disease: Cobble-stone appearance
|
|
|
What findings favor a diagnosis of Crohn's Disease?
|
- Rectal sparing (UC always affects the rectum)
- Normal vasculature next to affected tissue (skip lesions) - Isolated involvement of the terminal ileum (pancolitis/UC can have backwash ileitis where the lesion extends up to the ileum) - Fistulas or Strictures - Granulomas on biopsy |
|
|
What are the extra-intestinal manifestations of IBD?
|
- Acute Arthropathy (knees, spine, proximal joints of hands): 15-20%
- Erythema Nodosum (red rash on shins): 15% - Choledocholithiasis: 15-30% - Ocular complications: 5-15% - Sacroiliitis: 9-11% - Nephrolithiasis: 5-10% - Ankylosing Spondylitis: 3-5% - Pyoderma Gangrenosum: 1-2% - Primary Sclerosing Cholangitis: 1-2% - Amyloidosis: rare |
|
|
Which extra-intestinal manifestations are more common in Crohn's Disease?
|
- Ankylosing Spondylitis (3-5%)
- Nephrolithiasis (later on in CD in patients who have had surgery): 5-10% |
|
|
Which extra-intestinal manifestations are more common in Ulcerative Colitis?
|
- Pyoderma Gangrenosum: 1-2%
- Primary Sclerosing Cholangitis: 1-2% |
|

What is this? What is it associated with?
|

Erythema Nodosum: painful and tender extra-intestinal manifestation of IBD (15%)
|
|

What is this? What is it associated with?
|

Pyoderma Gangrenosum: violet tinge at endges of rash, extra-intestinal manifestation of IBD (more common in UC) (1-2%)
|
|
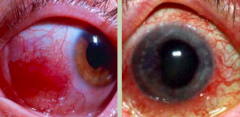
What is this? What is it associated with?
|
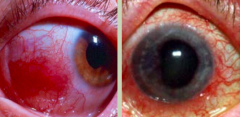
Ocular complications (5-15%), extra-intestinal manifestation of IBD:
- Left: Episcleritis - white part of eye is very inflamed, usually not painful, more of a cosmetic issue - Right: Uveitis - painful inflammation of the iris that hurts between light and dark rooms as the iris contracts |
|
|
What are the goals of management of IBD?
|
- Confirm accurate diagnosis
- Induce remission (absence of inflammatory symptoms and feeling "well") - Maintain remission - Avoid surgery when possible - Enhance quality of life - Avoid complications of disease and therapy |
|
|
How common is maintenance therapy in patients in remission from IBD?
|
- 95% of patients require maintenance therapies
- Transition to maintenance occurs AFTER a successful induction |
|
|
What genetic abnormalities are associated with CD and UC? How common?
|
Crohn's Disease:
- NOD2 mutations: 35-40% of patients with this mutation get the disease (incomplete penetrance) and not all patients w/ CD have this mutation - Only associated with CD (not UC) - Concordance rate for monozygotic twins is approximately 50% Ulcerative Colitis: - Concordance rate for monozygotic twins is only 16%, suggesting that genetic factors are less dominant |
|
|
What is the function of the NOD2 gene?
|
- Encodes a protein that binds to intracellular bacterial peptidoglycans and subsequently activates NF-κB
- Disease-associated NOD2 variants are less effective at recognizing and combating luminal microbes, which are then able to enter the lamina propria and trigger inflammatory reactions - Other data suggest that NOD2 may regulate immune responses to prevent excessive activation by luminal microbes |
|
|
What is the mucosal immune response to bacteria in IBD?
|

- Dendritic cells sample bacteria in lumen and present them to T cells on MHC
* Some T cells become TH1 cells, which release TNF * TNF can lead to epithelial barrier defects which can cause an influx of bacterial components * Some T cells can become TH17 cells (via IL-23) - Additionally, some T cells can become TH2 cells, which release IL-13 |
|
|
What epithelial defects have been described in Crohn's Disease and/or Ulcerative Colitis?
|
- Defects in intestinal EPITHELIAL TIGHT JUNCTION barriers seen in CD and some of their healthy 1st-degree relatives
- Barrier dysfunction can activate innate and adaptive mucosal immunity and sensitize subjects to disease |
|
|
How does the microbiota relate to IBD pathogenesis?
|
- Some antibiotics, such as metronidazole, can be helpful in maintenance of remission in Crohn disease by controlling the microbiota
- Ill-defined mixtures containing probiotic bacteria may combat disease in experimental models, as well as in some patients with IBD - The mechanisms responsible are not well understood |
|
|
What is the most predominant, non-genetic factor in IBD?
|

Colonizing bacteria:
- IBD is characterized by an amplified response to the intestinal microbiota - Differences in microbiota composition and diversity may also contribute to IBD |
|
|
What are the types of disease behavior in Crohn's Disease? How common are they at DIAGNOSIS of CD?
|
* Inflammatory: 85% (eg, erythema, ulcerations)
- Stricturing: ~0% (eg, blockage) - Penetrating: 15% (eg, fistulas) |
|
|
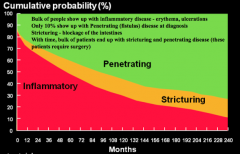
What are the types of disease behavior in Crohn's Disease? How common are they 20 years after diagnosis of CD? Implications?
|
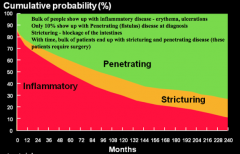
* Penetrating: 70%
* Stricturing: ~20% - Inflammatory: ~10% Most patients end up requiring surgery d/t penetrating disease (fistulas) or stricturing disease |
|
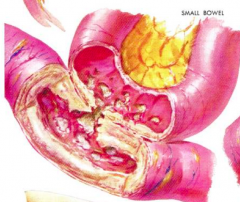
What does this image represent? Which type of IBD is it associated with?
|
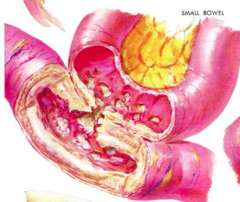
- Fistula (can be between two loops of small intestine, or with the vagina, skin, peritoneum, etc)
- Sign of Crohn's Disease |
|
|
What are the new classes of drugs for treating IBD?
|

Biologics: antibodies against TNF
|
|
|
What are the Biologics used to treat IBD? Mechanism?
|

Anti-TNF monoclonal antibodies:
- Infliximab - Certolizumab pegol - Adalimumab |
|
|
What are the benefits of anti-TNF therapy for IBD?
|
- Induces and maintains remission of IBD
- Steroid sparing - Heals perianal fistulizing disease |
|
|
What is the efficacy of anti-TNF therapy based on how long a patient has been diagnosed with IBD?
|
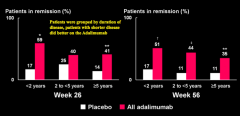
The patients who have had a shorter disease time course were more likely to induce remission than those who had the disease for a longer period of time
|
|
|
What are the side effects of anti-TNF therapy?
|
Slight increase in incidence of lymphoma (however, the risk of lymphoma is very low compared to the risk that you will need surgery if you remain untreated)
|
|
|
Why is there decreased rates of infection in patients with IBD?
|
- Fewer patients on steroids now d/t anti-TNF therapy, therefore fewer opportunistic infections
- Improved mucosal healing - Fewer fistulas, strictures, and abscesses |
|
|
What are the types of Microscopic Colitis?
|
- Collagenous Colitis
- Lymphocytic Colitis |
|
|
What are the symptoms of Collagenous Colitis and Lymphocytic Colitis (types of microscopic colitis)?
|
- Chronic, non-bloody, watery diarrhea without weight loss
- Findings on radiologic and endoscopic studies are normal |
|
|
What are the characteristics of Collagenous Colitis?
|
- Type of microscopic colitis
- Presence of dense sub-epithelial collagen layer - Increased numbers of intra-epithelial lymphocytes - Mixed inflammatory infiltrate within lamina propria |
|
|
What are the characteristics of Lymphocytic Colitis?
|
- Type of microscopic colitis
- Histologically similar to collagenous colitis - Sub-epithelial collagen layer is of normal thickness and the increase in intra-epithelial lymphocytes may be greater - Associated with celiac and auto-immune diseases |
|
|
Which type of microscopic colitis is associated with celiac and auto-immune diseases?
|
Lymphocytic Colitis
|
|
|
How do you treat Microscopic Colitis (both collagenous and lymphocytic)?
|
Budesonide
|
|
|
Why is the small intestine relatively sterile compared to the colon?
|
- Protected by gastric acid
- Protected from bacteria in colon by ileocecal valve - Relatively fast transit time |
|
|
What can cause increased bacterial contact with unabsorbed carbohydrates? Implications?
|
- Surgery (eg, gastric bypass disrupts pH)
- Antacid - Slow motility - Can lead to small intestinal bacterial overgrowth |
|
|
How do you diagnose Small Intestinal Bacterial Overgrowth?
|
- Duodenal aspirate
- Hydrogen breath test |