Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
169 Cards in this Set
- Front
- Back
|
What are the symptoms of a lacunar stroke?
|
Pure motor hemiparesis
Pure sensory Ataxic hemiparesis Sensory motor Dysarthria clumsy hand syndrome |
|
|
What medications and interventions are used in the tx of cerebral palsy to alleviate contractures and improve function?
|
Dantrolene – muscle relaxer
Baclofen – muscle relaxer Benzodiazepines Botox |
|
|
What is the ACLS tx for ventricular fibrillation?
|
CPR
Defibrillate at 360 joules, Epinephrine or vasopressin |
|
|
Which vasopressor matches the following statement?
High doses optimize the α-1 vasoconstriction |
Epinephrine
|
|
|
Which vasopressor matches the following statement?
Best choice for septic shock |
Norepinephrine
|
|
|
Which vasopressor matches the following statement?
Causes vasoconstriction but with bradycardia |
Phenylephrine
|
|
|
What is the next step in the evaluation of penetrating injuries to the different zones of the neck?
|
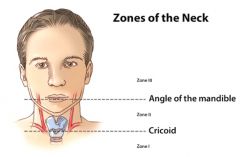
Zone 1 → CT angiogram (4-vessel arteriogram)
Zone 2 → Surgical exploration Zone 3 → CT angiogram, triple endoscopy |
|
|
What EKG finding is seen in pts with Wolff-Parkinson-White syndrome? What causes WPW?
|
EKG: delta wave prior to QRS complex
Cause: reentry thru accessory conduction pathway |
|
|
What is the next step in the management of an AGUS pap smear?
|
Colposcopy & Endocervical curettage
|
|
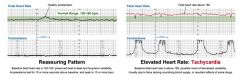
What is the differential diagnosis for fetal tachycardia?
|
Maternal fever/ infection/ dehydration
Fetal anemia Fetal tachyarrhythmias (HR > 200) Fetal immaturity Chorioamnionitis Maternal thyrotoxicosis Drugs or medications (Terbutaline, atropine) Fetal hypoxia |
|
|
What type of fetal surveillance strategy is typical for high-risk pregnancies?
|
Biophysical profile or NST
|
|
|
What are the first steps in the management of non-reassuring fetal heart tones during labor?
|
Place maternal O2 + turn off Pitocin (remove cervidil) + turn mom to left side
Correct hyperstimulation if needed with terbutaline 0.25mg SubQ Correct any maternal hypotension (often a/w epidural). IVF bolus if needed SVE and place FSE (check for cord prolapse) Consider need for intervention such as amnioinfusion or C-section |
|
|
One hour into the active stage of labor, a fetus’s heart tones become nonreassuring. What actions are taken immediately?
|
Maternal O2
Turn off oxytocin Turn mother in LLD position |
|
|
What would be some contraindications to fetal scalp electrode placement?
|
Breech presentation
< 36wks gestation Worry of maternal viral infection |
|
|
HYQ: What defines prolonged latent phase and prolonged active phase of labor dystocia?
|
Prolonged latent phase: does not progress from latent ot active phase for >20hours in nulliparous pts or >14 hrs in multiparous pts
Prolonged active phase: Active phase > 12 hrs or Nulliparous < 1.2 cm/hr dilation Multiparous < 1.5 cm/hr dilation |
|
|
What is the definition of arrest of descent? In general, how is it managed?
|
Arrest of descent occurs when the cervix does not continue to dilate during the active phase of >2 hrs in multips and >3hrs in primips
Management: Reassess the 3 Ps Placement of IUPC to better assess “power” (>200 MVU/10min) Augmentation with oxytocin to augment “power” C-section if power, passenger and passage are unable to be further augmented |
|
|
What is the definition of uterine hyperstimulation? What adrenergic antagonist is particularly helpful in reversing uterine hyperstimulation?
|
Uterine hyperstimulation is defined by one of the following:
>5 contractions over 10min with duration > 60secs significant fetal heart rate decelerations Terbutaline 0.25mg Sub-Q if often used as a tocolytic to stop uterine contractions |
|
|
What defines prolonged latent phase of labor? Prolonged active phase?
|
>20 hrs nulliparous
14 hrs in multiparous 12 hrs or <1.2cm per hour nulliparous < 1.5 cm/hr multiparous |
|
|
By how much can an epidural lengthen stage 2 of labor?
|
About 1 hour
|
|
|
What are some of the methods that can be used for induction of labor?
|
Rupture of membrane
Oxytocin Other less common options |
|
|
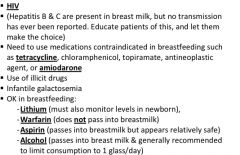
What are some of the contraindications to breastfeeding?
|
|
|
|
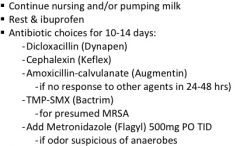
What is the treatment or mastitis in a postpartum female?
|
|
|
|
What are the treatment options for uterine atony/ postpartum hemorrhage?
|
Uterine massage
Oxytocin 10 units IM x1 Methergine (methylergonovine) 0.2 mg IM (ergot agent that is contraindicated if HTN) Hemabate (PGF2-α) 0.25mg IM of intra-uterine (contraindicated if asthma) Surgical options: uterine artery ligation, internal iliac artery ligation, selective arterial embolization, or hysterectomy |
|
|
What are the characteristic features of postpartum endometritis?
|

|
|
|
What is the treatment for postpartum endometritis?
|

|
|
|
What are the indications for a vertical incision vs low transverse incision for a caesarean section?
|
Transverse lie
Adhesions or fibroids Hysterectomy planned Cervical cancer Postmortem delivery |
|
|
What potential adverse events can occur during a VBAC?
|
Uterine rupture (1/100)
Catastrophic event (1/1000) |
|
|
A woman that is postpartum day 2, s/p C-section develops a temperature of 101°F, uterine tenderness, and foul lochia. Her urine urinalysis is normal & her incision is clean, dry and intact. What does this patient likely have and what is the treatment?
|
Dx: post-partum endometritis
Tx: Clindamycin + ampicillin + gentamicin Ceftriaxone + clindamycin Ampicillin/sulbactam (Unasyn) + doxycycline Cefoxitin + doxycycline |
|
|
What is the treatment for a woman that does not wish to breastfeed postpartum?
|
1st line: Icepacks, tight bras, avoid stimulation, analgesia
2nd line: Oral contraceptives 3rd line: Bromocriptine |
|
|
What medications can be used to control postpartum hemorrhage?
|
1st line: Uterine massage
Then: Oxytocin Other less common options |
|
|
What is the definition of arrest of descent?
|
(With epidural)
multiparous stage 2 for more than 2 hrs nulliparous stage 2 for more than 3 hrs if you don’t have an epidural, then subtract 1 hour |
|
|
What are the first steps in the management of uterine hyperstimulation (or non-reassuring fetal heart tones)?
|
Oxygen
Remove uterine stimulant Position in LLD Giver terbutaline Increase monitoring |
|
|
When is a normal child’s weight regained, doubled, tripled, and quadrupled in terms of their birth weight?
|
Regain weight in 2 weeks
Double weight in 4 months Triple weight in 12 months Quadruple weight in 24 months |
|
|
Define failure to thrive (FTT)
|
<5% on a growth chart
cross 2 or more lines in weight on the growth chart |
|
|
How do you distinguish between Type I and Type 2 diabetes in a child?
|
Type 1 – skinny, anti-islet antibodies
|
|
|
When does a normal child’s height increase by 50%, double, and triple?
|
Height ↑ by 50% by age 1
Height doubled by age 4 Height tripled by age 13 |
|
|
How many blocks can a child put in a tower at these ages: 12 months, 18months, 2 yrs, 3yrs?
|
12 months → 2 blocks
18 months → 4 blocks 2 years → 6 blocks 3 years → 9 blocks |
|
|
An infant that has any remaining primitive reflexes after what age needs a work-up for CNS pathology?
|
6 months of age
|
|
|
What is the first solid food parents should give their child?
|
Iron-fortified cereal
|
|
|
Why should cow’s milk not be given before 1 year of age?
|
Risk of allergy
Hemorrhaging in gut Iron deficiency anemia |
|
|
Car Seats:
|
< 1 year and <20 lbs → infant in back seat, facing backwards
1 – 4 years and > 20 lbs → in back seat but still in car seat, now have option of facing forward Once forward-facing car seat is outgrown (4 years and 40 lbs) → booster seat in back Keep in booster seat until the belt fits correctly (usually 4’9’’ and 8-12 years) → then belted with a lap/shoulder belt in the back seat until 13 years of age |
|
|
How many calories are present in an ounce of breast milk? How many calories are present in an ounce of formula?
|
20 kilocalories/ounce in both breast milk and formula
|
|
|
What are the caloric needs for an infant younger than 6 mos?
|
100-120 calories/kg/day
|
|
|
What work-up should be performed on a newborn with a single umbilical artery?
|
Occurs in ~0.5% of births and 20-30% of these infants have major structural anomalies
Obtain renal sonagram as 7% will have clinically significant renal symptomatic anomalies |
|
|
What are the most common problems that arise in premature infants?
|
Respiratory distress syndrome, hypoglycemia, persistent PDA, infection/sepsis, retinopathy of prematurity, intraventricular hemorrhage, necrotizing enterocolitis
|
|
|
What is the difference between caput succedaneum and cephalohematoma?
|
Caput → diffuse swelling or edema of the scalp, edema crosses suture lines, resolves within a few days
Cephalohematoma → subperiosteal hemorrhage, does NOT cross suture lines, resolves in weeks to months |
|
|
What is the next step in the management of a newborn female with bloody vaginal discharge in the first week of life?
|
Nothing (withdrawal from hormones)
|
|

is this benign?
|
Yes - Cutis marmorata: spider webbing/ marbling of the skin. Non-concerning
a normal reticulated mottling of the skin caused by vascular response to cold. |
|

Is this benign?
|

Erythema toxicum neonatorum: 2-3 mm, yellow pustule with red base (similar appearance to white-head) arising in the first 24-72 hours, microscopic examination of the pustular contents (not necessary for diagnosis) reveals numerous eosinophils, usually gone by 3 weeks, tell parents to leave alone
Erythema toxicum neonatorum can result in a “flea-bitten” appearance. |
|

what is this?
|

Transient neonatal pustular melanosis: superficial pustules overlying hyperpigmented macules. Tell parents to leave alone
Transient neonatal pustular melanosis is a vesiculopustular rash that occurs in 5 percent of black newborns, but in less than 1 percent of white newborns.6,9 In contrast with erythema toxicum neonatorum, the lesions of transient neonatal pustular melanosis lack surrounding erythema. In addition, these lesions rupture easily, leaving a collarette of scale and a pigmented macule that fades over three to four weeks. All areas of the body may be affected, including palms and soles. |
|
what is this?
|
Neonatal acne (acne neonatorum): seen in 20% of infants, due to maternal hormone stimulation of sebaceous glands, usual age of onset is 3 weeks old. There is no increased risk of acne in adolescence. Mild lesions should be left alone and will resolve in 4 months. Severe inflammation can be managed with benzoyl peroxide or topical retinoids
It typically consists of closed comedones on the forehead, nose, and cheeks, although other locations are possible. Open comedones, inflammatory papules, and pustules can also develop. |
|

What is this?
|
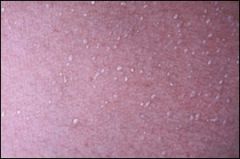
Milia (Miliaria): due to accumulation of sweat beneath eccrine sweat ducts that are obstructed by keratin at the stratum corneum usually develops in 1st week after birth, a/w excess warmth (incubator, excess clothes, fever). No treatment is needed except possibly to reduce sweating with loose clothing and cool baths
Miliaria crystallina is caused by superficial eccrine duct closure. It consists of 1- to 2-mm vesicles without surrounding erythema, most commonly on the head, neck, and trunk (Figure 5). Each vesicle evolves, with rupture followed by desquamation, and may persist for hours to days. |
|

What is this?
|

Harlequin color change: intense reddening of gravity dependent side and blanching of the nondependent side with a line of demarcation between the two, lasts a few sec-min, affects 10% of newborns (more common in newborns), most common in the first few days of life, may be due to immaturity of autonomic innervation to skin vessels. Completely benign and will resolve in days- 3 weeks.
|
|

What is this?
|
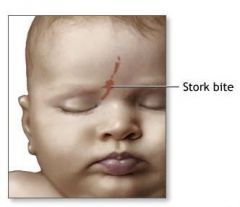
Macular stains (Stork bites): permanent vascular malformations most commonly occurring on the nape of the neck, but also upper eyelids and middle of forehead. Benign but persist throughout life
|
|

What is this?
|

Mongolian spot: bluish discoloration over buttocks and base of spine, probably present on at least one of the parents. Benign and will usually fade in 1-2 years. Document to avoid later confusion with bruises
|
|

What is this?
|

Infantile Acne: different than neonatal acne, onset usually at 3-4 months of age, yellow papules around nose & cheeks, usually clears by age one but may persist until age 3. Severe inflammation can be managed with benzoyl peroxide or topical retinoids
|
|
|
Who under the age of 11-12 should receive an MCV4 meningococcal vaccine?
|
Moving to endemic area
Children > age 2 with functional true asplenia |
|
|
When can a child switch to a front-facing car seat? A booster seat in the back seat?
|
Forward facing → > 2 years
Booster seat → until 4 ft 9 in & btw 8-12 years |
|
|
How many kilocalories are in an ounce of breast milk? Formula?
|
20 kcal/ounce
|
|
|
Cephalohematoma increases the likelihood of what?
|
Jaundice
Note: more common with vacuum-assisted deliveries |
|
|
A 2-day old baby boy presents with 2-3mm yellow pustules with red bases. What are these likely to be and what is the prognosis?
|
Erythema toxicum neonatorum
|
|
|
Why is it important to document Mongolian spots?
|
Prevent false accusations of abuse
|
|
|
What are some risk factors for SIDS?
|
2-3 months old
While infant is sleeping Low SES Maternal age < 20 Drugs/ cigarettes in pregnancy Prior sibling with SIDS Prone sleeping position Sleeping on soft surface Overheating |
|
|
What medications can be used to treat thrush in an infant?
|
Nystatin oral suspension
|
|
|
What are the risk factors for Sudden Infant Death Syndrome (SIDS)?
|

|
|
|
When would you expect the anterior fontanelle to close in a child? What would you suspect if it did not close in the expected time frame?
|
- Closed in 1% by age 3 months, 38% by 12 months, and 96% by 24 months
- If delayed consider: Down syndrome, achondroplasia, Rickets, congenital hypothyroidism, ↑ intracranial pressure - If closure < 3 months, carefully monitor head circumference for craniosynostosis (premature closure of cranial sutures) - Craniotabes (soft occipital bone, like ping-pong ball) from 3 – 12 months is highly suspicious for Rickets |
|
|
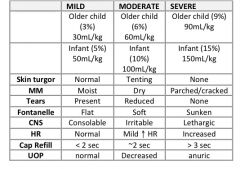
What are the signs of severe dehydration in a child?
|
|
|
|
What mnemonic can you use for the questions you should ask during an annual adolescent exam?
|
“HEADSSS”
Home environment Employment/ Education Activities Drugs Sex. Suicide, Safety |
|

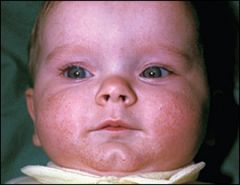
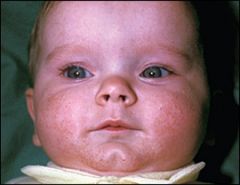
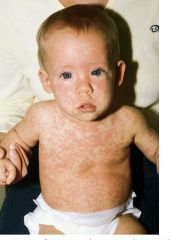
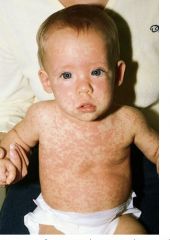
What are the clinical features of measles infection (rubeola)?
|

Prodrome for 2-3 days: fever, malaise, anorexia, and 3 “Cs” (Cough, Coryza, Conjunctivitis)
Koplik spots on buccal mucosa after 1-2 days (white-gray spots with a red base) → occur 48hrs prior to rash. Pathognomonic for measles Rash 5 days after prodrome onset: erythematous, maculopapular starting at the head then spreading to the feet → lasts 4 -5 days → resolves from head down |
|

What is the treatment for measles?
|

Supportive therapy (antipyretics, fluids)
Monitoring & treating bacterial superinfections such as pneumonia or otitis media Vit A 100,000 IU PO x1 in 6 – 12 mo olds, 200,000 IU PO x1 if older than 12 months WHO recommends vit A to all children with measles in areas where vitamin A def is prevalent and measles mortality exceeds 1% AAP recommends vit A given as above to children 6mos—12 years hospitalized for measles or its complications or if immunodeficient or high likelihood of vitamin A deficiency (ophthalmologic evidence, intestinal malabsorption, malnutrition, or recent immigration from an area with high measles mortality) Ribavirin is not yet well studied and not currently standard of care for measles despite that it harms measles virus in vitro |
|

What are the classic features of rubella virus (German measles)?
|

Low grade fever, lymphadenopathy, and rash
Prodromal malaise, fever, anorexia for 1-5 days prior to rash Lymphadenopathy – suboccipital & posterior cervical Erythematous, tender maculopapular rash that starts at the face then generalizes Rash persists 5 days and does not darken as does the rash of measles Polyarthritis may be seen up to a month in women and adolescents |
|

What are the characteristic features of Coxsackie hand, foot, and mouth disease?
|
Constitutional fever & anorexia
Oral vesicle on the buccal mucosa and tongue Small, tender, maculopapular/vesicular rash on the hands, feet and sometimes buttocks Duration is typically 3-5 days without complications |
|

What are the signs and symptoms or scarlet fever caused by Streptococcus pyogenes?
|
Rash that is coarse (“sandpaper-like”), erythematous and blanching (“sunburn-like”)
Rash starts on the trunk that generalizes, but spares palms & soles Rash is most prominent in skin creases of axilla and groin (Pastia’s lines/sign) Strawberry tongue, beefy-red pharynx, cervical LAD Fever/chills Later desquamation of hands & feet (addn ddx Kawasaki disease, Toxic Shock Sydrome, acrodynia or mercury poisoning) (+) throat culture or rapid strep test |
|
What are the characteristic symptoms of roseola infantum (HHV-6)?
|

Sudden, high fever (exceeding 102°F) for 3-4 days
Child has no other signs of infection and often acts/plays normally Rash that appears when fever dissipates and starts on the trunk then spreads over entire body & lasts 24 hours Other common findings: erythematous papules on soft palate & uvula, mild cervical LAD, edematous eyelids, bulging anterior fontanel in infants Commonly misdiagnosed as acute otitis media and subsequent antibiotic allergy! |
|
What is the treatment for roseola infantum?
|
Antipyretics as needed
|
|
|
What is the differential diagnosis for cervical lymphadenopathy in a child?
|

|
|
|
What is PFAPA syndrome?
|
Benign 4-5 day syndrome consisting of Periodic Fever, Aphthous ulcers, Pharyngitits, and Adenitis
Occurs monthly (q 28 days) Exclusion criteria include neutropenia, cough, coryza, diarrhea, severe abdominal pain, rash, arthritis, and neuro defects Usually affects preschool-aged children (2-5 yr olds) Benign, self-limiting disease Treatments Glucocorticoids relieve symptoms in a matter of hours Cimetidine may be used for prevention of episodes but is of questionable efficacy Average duration of recurring symptoms is 4.5 years |
|
|
What are the classic symptoms of pertussis?
|
Incubation 7 – 10 days
Catarrhal stage (1 – 6 weeks): paroxysms of cough with inspiratory whoop that is worse at night & often with post-tussive emesis and exhaustion Often confused with acute bronchitis Convalescent stage (2 – 3 weeks): waning of symptoms |
|
|
What is the treatment for pertussis?
|

|
|
|
What additional workup, if any, is needed in a child diagnosed with a UTI?
|
Voiding cystourethrogram (VCUG) and Renal U/S if:
Child 2 months – 2 years of age (AAP) Male of any age Girl < 3 years (or unable to verbalize urinary symptoms Febrile UTI or recurrent UTI Other red flags: abnormal voiding pattern, poor growth, FHx of renal disease, hypertension, abnormalities of the urinary tract |
|
|
What is the mnemonic for questions you should ask while examining adolescents?
|
“HEADSSS”
Home environment Employment/ Education Activities Drugs Sex. Suicide, Safety |
|
|
In addition to MCV4, what other vaccines should asplenic pediatric patients >2 years receive?
|
HIB & pneumococcal
|
|
|
What are the 3 C’s of the prodrome of rubeola?
|
Coryza, Cough, Conjunctivitis
|
|
|
What are some causes of desquamation of the hands & feet?
|
Scarlet fever
Kawasaki Disease Toxic Shock Syndrome Acrodynia Steven-Johnson Syndrome |
|
|
How long is the incubation period for pertussis? What is the treatment?
|
Incubation: 7-10 days
Treatment: macrolide |
|
|
Which viral infection is characterized by sudden high fevers for 3-4 days but is otherwise asymptomatic? A rash will often appear when the fever dissipates
|
Roseola Infection (HHV 6)
|
|

Intense reddening of gravity dependent side and blanching of the non-dependent side with a line of demarcation between the two, lasts a few sec-min
|
Harlequin Color Change
|
|

Due to accumulation of sweat beneath eccrine sweat ducts that are obstructed by keratin at the stratum corneum
|
Milia
|
|
|
HYQ: If a patient with measles required treatment with medication, what medication would you use?
|
Vitamin A
|
|
|
What is the treatment for roseola infantum?
|
Generally no treatment except antipyretics
|
|
|
What are some common causes of delayed closure of the anterior fontanelle?
|
Rickets
Down syndrome Achondroplasia Congenital hypothyroidism Elevated Intracranial pressure |
|
|
When do children first exhibit stranger anxiety?
|
6 – 9 months
|
|
|
When is gender identity typically formed?
|
2 – 3 years
|
|
|
When can children begin to eat solid foods?
|
4 – 6 months
|
|
|
When can children drink cow’s milk?
|
1 year
|
|
|
What interventions have been shown to ↓ incidence of SIDS?
|
Back to bed
Pacifier Fan on in room No smoking in house No pillows/ toys in bed |
|
|
How many total doses of the DTaP vaccine should a 6yo have received?
|
5 doses
|
|
|
At what age is the meningococcal vaccine indicated?
|
11 years
|
|
|
How would you expect weight to increase in the first 2yrs?
|
Double newborn weight – 4 mos
Triple newborn weight – 12 mos Quadruple newborn weight – 24 mos |
|
|
Bruton’s Agammaglobulinemia
|
X-linked (Boys)
B-cell deficiency → defective tyrosine kinase gene → low levels of ALL immunoglobulins Recurrent Bacterial infections after 6 months No B-cells on peripheral smear |
|
|
Thymic aplasia (DiGeorge Syndrome)
|
3rd & 4th brachial pouches fail to develop
↓ no thymus → no T cells no PTHs → low Ca2+ → tetany congenital defects in heart/ great vessels recurrent viral, fungal, protozoal infections 90% have a chr 22q11 deletion |
|
|
Severe Combined ImmunoDeficiency (SCID)
|
Defect in early stem cell differentiation
Can be caused by at least 7 different gene defects (ie adenosine deaminase deficiency) Presentation triad: Severe recurrent infections Chronic mucocutaneous candidiasis Fatal or recurrent RSV, VZV< HSV, Measles, Influenza, Parainfluenza PCP pneumonia Chronic Diarrhea Failure to Thrive (FTT) no thymic shadow on newborn CXR DO NOT GIVE LIVE VACCINES!! |
|
|
Chronic mucocutaneous candidiasis
|
T-cell dysfunction vs C. albicans
Tx: antifungals (ketoconazole, fluconazole) |
|
|
Wiskott-Aldrich syndrome: “WAITER”
|
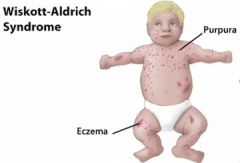
Wiskott-Aldrich
Immunodeficiency Thrombocytopenia Eczema (of the trunk) Recurrent pyogenic infections |
|
|
(A)taxia-Telangiectasia
|
Ig(A) deficiency
Cerebellar (A)taxia, and poor smooth pursuit of moving target with eyes Telangiectasias of face > 5 yo ↑ cancer risk: lymphoma & acute leukemias Radiation sensitivity (try to avoid x-rays) +/- ↑ AFP in children > 8 months average age of death ~ 25 years |
|
|
Selective Immunoglobulin Deficiencies
|
IgA deficiency is most common
Most appear healthy Sinus & lung infections 1/600 European descent a/w atopy, asthma possible anaphylaxis to blood transfusions and blood products |
|
|
What is the half-life of the IgG antibodies transferred from mother to infant?
|
28 days
|
|
|
What is the presentation triad for SCID?
|
Severe recurrent infections
Chronic diarrhea Failure to thrive (FTT) |
|
|
What are the clinical features of Wiskott-Aldrich syndrome?
|
“WAITER”
Wiskott-Aldrich Immunodeficiency Thrombocytopenia Eczema Recurrent pyogenic infections |
|
|
What is the management of chronic granulomatous disease?
|
Prophylactic TMP-SMX (Bactrim), Interferon-γ
|
|
|
If a female child is in the 80th percentile for height & the 25th percentile for head circumference, what chromosomal abnormality should you suspect?
|
Turner Syndrome (XO)
|
|
|
What is the most common malformation of the head & neck?
|
Unilateral cleft lip (multifactorial causes)
|
|

What features are characteristic of fetal alcohol syndrome?
|
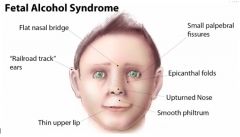
Facial features:
Short palpebral fissures Thin upper lip Smooth philtrum Flattened midface Deficient brain growth: Structural brian abnormalities < 10th percentile for head circumference Abnormal neuro exam Variable mental retardation Growth retardation: < 10th percentile for height and weight Failure to thrive (FTT) despite adequate intake Disproportional low weight to height |
|
|
What are the differences in presentation btw branchial cleft cyst and thyroglossal duct cyst?
|
Brachial cleft: lateral neck
Thyroglossal: (most common = tongue) midline neck, moves with swallowing, most common congenital neck cyst, commonly assoc with ectopic thyroid tissue |
|
|
What are the common possible presenting features of tuberous sclerosis?
|

Distinctive brown, fibrous plaque on the forehead seen in infancy
Ash leaf spots (hypopigmented macules) → most easily seen with Wood’s lamp Shagreen patch (leathery cutaneous thickening usually on the lower trunk) Facial angiofibromas (AKA adenoma sebaceum) Seizures Mental Retardation My notes: Seizures, shagreen path, sebaceous adenoma, “ash leaf” spots, mental retardation Hamartomas (mass of tissue in endogenous location) - in CNS, skin, organs Assoc cancers: “Angie, the astronaut, made a rap (rhabdo) about her heart and kidney” also think – when in space as an astronaut, your heart hurts b/c you miss your family & your kidney hurts cuz its hard to pee” Cardiac rhabdomyoma Renal angiomyolipoma Astrocytoma |
|
|
Lactic acidosis, hyperlipidemia, hyperuricemia (gout)
|

Type I
(Von Gierkes Disease) |
|
|
Diaphragm weakness → respiratory failure
|

Type II
(Pompe’s Disease) |
|
|
↑ glycogen in liver, severe fasting hypOglycemia
|
Type I
(Von Gierkes Disease) |
|
|
Hepatomegaly, hypOglycemia, hyperlipidemia (normal kidneys, lactate, uric acid)
|
Type III
Cori Disease |
|
|
Painful muscle cramps, myoglobinuria with strenuous exercise
|
Type V
(McArdle’s) |
|
|
Severe hepatosplenomegaly, enlarged kidneys
|
Type I
(Von Gierkes Disease) |
|
|
What malignancy is a/w Down syndome?
|
Acute lymphocytic leukemia (ALL) – “we ALL fall DOWN”
|
|
|
What GI complications are a/w Down syndrome?
|
Duodenal atresia
Hirschsprung’s disease Annular pancreas Celiac Disease |
|
|
What is WAGR syndrome?
|
Wilm’s tumor
Aniridia Genital abnormalities Retardation |
|
|
What is the most common cause of congenital mental retardation in men?
|
Fragile X Syndrome
|
|
|
A child presents with short palpebral fissures, a thin upper lip, smooth filtrum, and a flattened midface. He is below the 10th percentile for height & weight and his IQ is 65. What is the cause of his abnormalities? What could have been done to prevent them?
|
Dx: Fetal alcohol syndrome
Prevent – Don’t drink! |
|
|
Congenital heart defect + low calcium + recurrent infections
|
DiGeorge Syndrome
|
|
|
Chronic mucocutaneous candidiasis + chronic diarrhea + FTT
|
SCID
|
|
|
Thrombocytopenia + eczema + recurrent infections
|
Wiskott-Aldrich
|
|
|
Poor smooth pursuit of eyes + elevated AFP after 8 months
|
Ataxia Telangiectasia
|
|
|
Partial albinism + recurrent URIs + neurologic disorders
|
Chédiak- Higashi Disease
|
|
|
Cleft lip/palate, life expectancy < 1 yr, polydactyly
|
Trisomy 13
|
|
|
High-pitched cat-like cry
|
Cri du chat
|
|
|
Elfin facial features, cardiac defects
|
William Syndrome
|
|
|
Tall, thin male with gynecomastia and testicular atrophy
|
Klinefelter Syndrome
|
|
|
Obesity & overeating
|
Prader Willi
|
|
|
Micrognathia, life expectancy < 1 yr, rocker-bottom feet
|
Trisomy 18
|
|
|
Happy mood, inappropriate laughter, ataxic gait
|
Angelman syndrome
|
|
|
Large ears, MR, macroorchidism
|
Fragile X
|
|
|
MR, Simian crease, GI & Cardiac defects
|
Trisomy 21
|
|
|
Short stature, infertility, coarctation of aorta
|
Turner Syndrome (XO)
|
|
|
When do infections typically begin in children with immune disorders?
|
After first 3 months of life
|
|
|
What are the current screening recommendations for breast cancer in average risk women?
|
- Ages 40-49: Screening mammogram q 1-2 yrs +/- clinical breast exam
- Benefits of screening in this age group are uncertain, but most all expert groups recommend screening of this age group (ACS, AMA, ACOG, AAFP…) - Every group agrees that at least offering a mammogram and shared decision making for this age range is appropriate - Ages 50-69: Screening mammogram q1-2 years +/- clinical breast exam - Proven benefits and all expert groups agree here - Ages 70+ and life expectancy > 10 years → screening mammogram q 1-2 years +/- clinical breast exam |
|
|
What is the USPSTF recommendation for hypertension screening?
|
Every 2 years in normotensive pts, starting at age 18
|
|
|
What is the USPSTF recommendation for cholesterol screening in pts without CAD risk factors?
|
Start at age 35 in men
Start at age 45 in women |
|
|
What specific interventions are helpful in smoking cessation?
|

|
|
|
How often should a normotensive pt get their BP checked?
|
Every 2 years starting at age 18 years
|
|
|
When should you start screening for high cholesterol in otherwise healthy patients?
|
Men: after age 35
Women: after age 45 |
|
|
Which medication for smoking cessation carries a black box warning about its side effect of suicidality?
|
Varencicline (Chantix)
|
|
|
What smoking cessation method doubles the quit rate?
|
Nicotine replacement therapy
|
|
|
What symptoms of vitamin deficiency do you get if you haven’t have enough folate? Vit A? VIt D? E? B3?
|
Folate:
Neural tube defects Megaloblastic anemia Vit A: Bitot’s spots Keratomalacia Xerothalmia Vit D: osteomalacia, Rickets Vit E: ↑ RBC fragility Vit B3: Dermatitis, Diarrhea, Dementia |
|
|
What vitamin can be used to treat psoriasis?
|
Vit D analogs
|
|
|
Which vitamin deficiency:
↑ RBC fragility |
Vit E
|
|
|
Which vitamin deficiency:
Dermatitis, cheilosis, glossitis |
Iron Def & B2, B3
|
|
|
Which vitamin deficiency:
Peripheral neuropathy, angular cheilosis, glossitis |
B12
|
|
|
Which vitamin deficiency:
Hemorrhagic disease |
Vit K
|
|
|
Which vitamin deficiency:
Dermatitis, Diarrhea, Dementia |
B3 (niacin)
|
|
|
Which vitamin deficiency:
Megaloblastic anemia |
Folate/ B12
|
|
|
Which vitamin deficiency:
Pernicious anemia |
B12
|
|
|
Which vitamin deficiency:
Bitot’s spots, keratomalacia, xerophthalmia |
Vit A
|
|
|
Which vitamin deficiency:
Osteomalacia, Rickets |
Vit D
|
|
|
Which vitamin:
Can be used to treat acne & psoriasis |
Vit A
|
|
|
Which vitamin:
Involved in the hydroxylation of prolyl residues |
Vit C
|
|
|
Which vitamin:
Requires intrinsic factor for absorption |
B12 (Cobalamine)
|
|
|
Which vitamin:
Deficiency may result from kidney disease |
Vit D
|
|
|
Which vitamin:
Given prophylactically to newborns |
Vit K
|
|
|
Which vitamin:
Can be used to elevate HDL and lower LDL |
B3 (niacin)
|
|
|
Which vitamin:
Deficiency can be caused by isoniazid use |
B6 (pyridoxine)
|
|
|
Which vitamin:
Cobalt is found within this vitamin |
B12
|