![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
49 Cards in this Set
- Front
- Back
|
Labial fusion 1. causes 2. treatment
|
1. This most commonly arises from excess exogenous androgen exposure, but it can also occur from increased androgen production from an enzymatic error, such as 21-hydroxylase deficiency, which leads to congenital adrenal hyperplasia. 2. reconstructive surgery |
|
|
21 hydroxylase deficiency |
Enzymatic deficiency which leads to congenital adrenal hyperplasia.
|
|
|
Imperforate hymen - cause |
The hymen is located at the junction between the urogenital sinus and sinovaginal bulbs. Before birth, the epithelial cells in the central portion of the hymenal membrane degenerate, leaving a thin rim of mucous membrane at the vaginal introitus, known at the hymenal ring. If this degeneration fails to occur then there is an imperorate hymen (1 in 1000 women) |
|
|
Imperforate hymen- presentation and problems |

- obstruction of the outflow tract of the reproductive system, which can lead to buildup of secretions in the vagina behind the hymen - if not diagnosed at birth, this condition is usually diagnosed at puberty when there is amenorrhea and cyclic pelvic pain. This is due to accumulation of blood in the vagina (hematocolpos) and in the uterus (hematometra) * treatment is surgical |
|
|
Transverse vaginal septum |
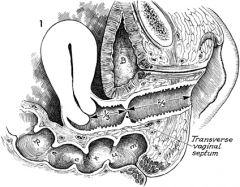
- failure for the upper and lower portions of the vagina to fuse during congenital development, resulting in a septum that divides the two portions. - this usually occurs between the lower 2/3 and the upper 1/3 - It often presents as primary amenorrhea with cyclic pelvic pain and menstrual symptoms during puberty- like imperforate hymen, however on exam there is normal external female genitalia with a short vagina that appears to end in a blind pouch. |
|
|
Vaginal atresia |
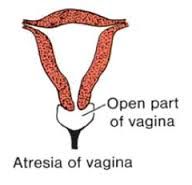
- when the lower vagina fails to develop and is replaced by fibrous tissue - the ovaries, uterus, cervix and upper vagina all develop normally - presents during puberty as primary amenorrhea and cyclic pelvic pain - physical exam reveals the absence of an introitus and the presence of a vaginal dimple - tx: vaginal pull-through surgical procedure |
|
|
Vaginal agenesis |
- congenital absence of the vagina and the absence or hypoplasia of all or part of the cervix, uterus, and fallopian tubes - these patients generally have normal external genitalia and normal secondary sexual characteristics (breast development, axillary and pubic hair) - patients are phenotypically and genotypically female with normal 46, XX karyotype - Tx- non-surgical approach uses vaginal dilators pressed into the perineal body, while the surgical approach involves using a skin graft to create a neo-vagina. With the surgical approach vaginal dilators still need to be used in order to keep it patent |
|
|
What are the non-neoplastic epithelial disorders of the vulva |
* These lesions often require histological examination of the tissue in order to differentiate between them , neoplasia and cancer |
|
|
Lichen sclerosis |

- inflammatory dermatosis that can be found on the vulva of women of all age groups, but has major significance in postmenopausal women, where it is associated with a 3-4% risk of vulvar skin cancer - the atrophy that results from this condition can lead to resorption of the labia minora, labial fusion, occlusion of the clitoris, contracture of the vaginal introitus, thinning of the vulvar skin and skin fragility - There are ivory white plaques, "cigarette paper" appearance of the skin in a butterfly/figure 8 pattern |
|
|
Lichen planus |

- uncommon inflammatory condition that affects the nails, scalp, and skin mucosa - when it affects the vulva, there are papular or erosive lesions of the vulva that may also involve the vagina - the inflammatory process results in the chronic eruption of shiny purple papules with white striae on the vulva, and often the flexor surfaces, mucous membranes of the oral cavity - may be associated with vaginal adhesions and erosive vaginitis - normally occurs in women in their 50s and 60s and is associated with a 3-4% risk of vulvar cancer |
|
|
Vulvar psoriasis |
- this may occur in combination with generalized psoriasis (which affects 2% of the population), or may occur in isolation. - it appears as silvery-red patches of skin that often occurs on the elbows and knees, but may also affect the scalp and nails |
|
|
Lichen simplex chronicus |

- thickened skin with accentuated skin markings and excoriations due to chronic itching and scratching - the intense pruritus that leads to this may be from atopic dermatitis, psoriasism, neuropathic pain, or psychological disorders - there is a scratch-itch cycle. The scratching leads to thickened skin, which then scratches more. |
|
|
Indications for definite vulvar skin biopsy |
|
|
|
Differential diagnosis for vulvar skin lesions |
|
|
|
Treatment for benign epithelial disorders of the vulva or vagina |
|
|
|
What is the most common tumor of the vulva? |
Epidermal inclusion cyst- usually result from the occlusion of pilosebaceous duct or a blocked hair follicle - they are lines with squamous epithelium and contain tissue that would normally be exfoliated - these are solitary and usually asymptomatic, however if they become superinfected and develop into abscesses - I&D or complete excision in required |
|
|
Sebaceous cysts |
- these occur when the duct of subaceous gland becomes blocked trapping the sebum - these can become superinfected with local flora and require I&D |
|
|
Apocrine sweat gland cysts |
If a sweat gland becomes blocked this can form a cyst |
|
|
Fox-Fordyce disease |
- uncommon chronic pruritic papular eruption that localizes to areas where apocrine glands are found |
|
|
Hidradentis suppurativa |
- skin disease that most commonly affects areas bearing apocrine sweat glands or sebacous glands, such as the underms, breasts, inner thighs, groin and buttocks - these cysts can become infected and form multiple abcesses - treatment is with I&D or excision. Antibiotics are needed if there is an overlying cellulitis |
|
|
Skene's/ paraurethral glands |
These are located next to the urethral meatus and can become blocked, leading to cystic dilation |
|
|
Bartholin's duct cysts and abscesses |
- the batholin's glands are found bilaterally at the 4 and 8 o'clock positions on the posterior lateral aspect of the vaginal orifice. These are mucus-secreting glands with ducts that open just external to the hymenal ring. - obstruction of these ducts forms cysts that can be left alone if small (1-2 cm)-- sitz baths may resolve them - if the bartholin duct cyst occurs for the first time in a woman over 40 then a biopsy should be done to rule out cancer - if these cysts enlarge they can become quite painful, resulting in dyspareunia and difficulty walking - if they do not resolve they can become infected and form abscesses which are usually polymicrobial in nature, but can at times be associated with STDs - these should be treated with I&D, however simple I&D usually leads to recurrence, so word catheter placement or marsupialization should be done |
|
|
Word catheter placement |
- this is commonly preferred method for treating abscesses of the Bartholin's gland in the emergency setting or office - a small incision is made to drain and irrigate the abscess, the a catheter with a balloon tip is inserted. The balloon is expanded to fill the space and left in place for 4-6 weeks, being serially reduced in size, while epithelialization of the cyst and tract occurs - adjunct antibiotic treatment is only required when the drainage is culture positive for n. gonorrhea or there is concomittant cellulitis |
|
|
Marsupialization |
- treatment for recurrent Bartholin's cysts or abscesses. - the entire lesion is incised and the cyst wall is sutured to the vaginal mucosa to prevent reformation - adjunct antibiotic treatment is only required when the drainage is culture positive for n. gonorrhea or there is concomittant cellulitis |
|
|
Gartner's duct cysts |
- gartner's ducts are remnants of the mesonephric ducts of the wolffian system and are most commonly found in the anterior lateral aspects of the upper part of the vagina. - these cysts are usually asymptomatic, however patients may present during adolscence with dyspareunia or pain with inserting a tampon - treatment is usually with excision (IVY and cystoscopy should be done pre-op to locate the bladder and ureters relative to the cyst and rule out other possible causes of the symptoms such as urethral diverticula, cancer etc) |
|
|
Lipomas |
- soft pedunculated or sessile tumors composed of mature fat cells and fibrous strands - these usually do not require removal unless they become large and symptomatic |
|
|
cherry hemangiomas |
- elevated soft red papules that contain an abnormal proliferation of blood vessels |
|
|
urethral caruncles and urethral prolapse |
- the present as small, red, fleshy tumors found in the distal urethral meatus - they occur almost exclusively in postmenopausal women as a result of vulvovaginal atrophy - when there is bloody spotting then a short course of vaginal estrogen is needed - rarely, surgical excision may be required |
|
|
DES exposure in utero |
- 25% of these females will have cervical abnormalities including cervical hypoplasia, cervical collars, cervical hoods, cock's comb cervix, and pseudopolyps - these women are at increased risk for cervical insufficiency during pregnancy - these women are also at risk for a very rare clear cell adenocarcinoma or the cervix and vagina, which is seen in young women under 20 and only 0.1% of women with DES exposure |
|
|
Nabothian cysts |
- cervical cyst that are dilated retention cysts caused by intermittent blockage of an endocervical gland - they usually expand to no more than 1 cm - most commonly found in menstruating women and are usually asymptomatic |
|
|
Mesonephric cysts |
- cervical cysts that are remnants of the wolffian ducts - they tend to lie deeper than nabothian cysts and on the external surface of the cervix |
|
|
Cervical endometriosis |
- endometriosis can implant on the cervix - these cysts tent to be red or purple - the patient usually has associated cyclic pelvic pain and dyspareunia |
|
|
Cervical polyps |
- benign growths that may be pedunculated or broad-based - often asymptomatic, but if there are symptoms, it is usually intermenstrual spotting, NOT pain - they are not considered pre-cancerous but are usually removed to prevent masking of irregular bleeding from other causes |
|
|
Cervical fibroids |
- Leiomyomas (myomas or fibroids) are common within the uterine body, however they can also occur in the cervix or prolapse into the cervical canal - usually cause intermenstrual bleeding, but can also cause dyspareunia and bladder or rectal pressure and may lead to hemorrhage, poor dilation of the cervix, malpresentation, or obstruction of the birth canal - rule out cancer, if symptomatic surgical excision (myomectomy or hysterectomy can be performed) |
|
|
Cervical stenosis |
- this may be congenital, a product of infection, atrophy, or scarring - it can also occur from obstruction with a neoplasm, polyp, or fibroid - typically asymptomatic and does not affect menstruation or fertility- and in these settings no treatment is needed - if there are symptoms or there needs to be access to the endocervical canal or glands then gentle dilation can be performed-- a catheter can be left in place to prolong patency |
|
|
What is the most common non-drug related congenital mullerian anomaly? |

|
|
|
bicornuate uterus |
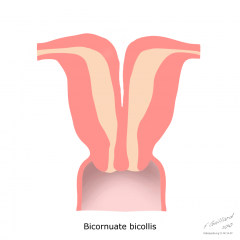
uterine anomaly involving a "heart-shaped" uterus with two horns. Pregnancy/implantation can occur in either horn. If IUDs are used for contraception that an IUD is needed in both horns. There is increased risk for second trimester pregnancy loss, preterm labor, malpresentation, and deformity. |
|
|
What is the most common indication for surgery in women in the US? |
Uterine fibroids (approximately 1/3 of all hysterectomies are performed for fibroids) |
|
|
Describe the hormone responsivity of fibroids |
|
|
|
Classification of uterine fibroids |
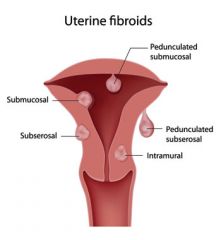
Uterine fibroids are classified by their location within the uterus. This includes: 1. submucosal (beneath the endometrium) 2. intramurual (in the muscular wall of the uterus)- most common type 3. subserousal (beneath the uterine serosa) 4. pedunculated (on a stalk with it's own blood supply) |
|
|
What is the most common type of uterine fibroid? |
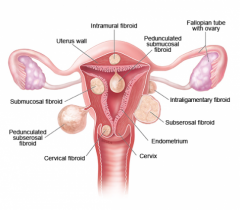
intramural (in the muscular wall of the uterus) |
|
|
What are the symptoms associated with uterine fibroids? What is most common? |
F- Frequency and retention of urine, hydronephrosis I- Iron deficiency anemia B- bleeding abnormalities (menorrhagia, metrorhagia, menometrorrhagia, postcoital spotting) Bloating - most common if symptoms exist however 50-65% of woman are asx R- Reproductive difficulties (dysfunctional labor, premature labor/delivery, fetal malpresentation, increased need for c-section) O- obstipation, constipation, rectal pressure I- Infertility D- Dysmenorrha, dyspareunia S- Symptomless - most common |
|
|
What is the relationship between uterine fibroids and uterine cancer? |
|
|
|
Epidemiology and risk factors of uterine fibroids |
|
|
|
Pelvic pain and uterine fibroids |
|
|
|
Uterine fibroids and pregnancy |
|
|
|
Diagnostic evaluation of uterine fibroids |
1. pelvic ultrasound is the most common means of diagnosis 2. sonohysterogram, HSG, and hysteroscopy may also be used 3. MRI is especially helpful in distinguishing between fibroids and adenomyosis and planning for surgery 4. on physical exam, there may be a non-tender, irregularly enlarged uterus with a lumpy-bumpy or cobblestone feel on palpation |
|
|
Treatment of uterine fibroids |
|
|
|
Follow-up care for uterine fibroids |
|