Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
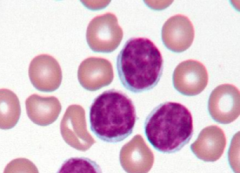
Case 1: 29 yo male presents complaining of SOB while jogging and progressive fatigue for 3 weeks. He usually runs several miles a day. He has felt well aside from this, has not had fever, weight change, loss of appetite, muscle aches, sweats, bruising, or bleeding.
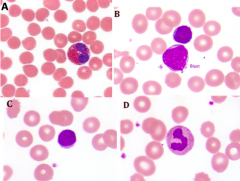
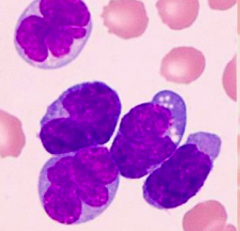
WBC: 11.3 / µL w/ abnormal WBCs on peripheral blood smear. Which of the following pictures reveals cells that are abnormal in the blood? |
B - blasts
|
|
Case 1: 29 yo male presents complaining of SOB while jogging and progressive fatigue for 3 weeks. He usually runs several miles a day. He has felt well aside from this, has not had fever, weight change, loss of appetite, muscle aches, sweats, bruising, or bleeding.
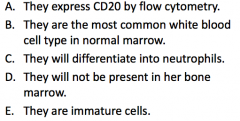
WBC: 11.3 / µL w/ abnormal WBCs on peripheral blood smear. Differential shows 60% blasts. What is the correct statement above? |
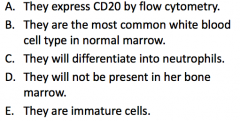
They are immature cells
|
|
|
Case 1: 29 yo male presents complaining of SOB while jogging and progressive fatigue for 3 weeks. He usually runs several miles a day. He has felt well aside from this, has not had fever, weight change, loss of appetite, muscle aches, sweats, bruising, or bleeding.
WBC: 11.3 / µL w/ abnormal WBCs on peripheral blood smear. Differential shows 60% blasts. What test can you do to further characterize these cells? |
Flow Cytometry - figure out definitively what kind of cells these are
|
|
|
Case 1: 29 yo male presents complaining of SOB while jogging and progressive fatigue for 3 weeks. He usually runs several miles a day. He has felt well aside from this, has not had fever, weight change, loss of appetite, muscle aches, sweats, bruising, or bleeding.
WBC: 11.3 / µL w/ abnormal WBCs on peripheral blood smear. Differential shows 60% blasts. Flow Cytometry shows they are positive for CD10, CD19, CD34 and negative for CD3 and CD20. Similar cells (as those found in PB) may be observed in what other tissue sites? |
- Cerebrospinal Fluid
- Lymph nodes - Bone marrow - Splenic sinusoids |
|
|
Case 1: 29 yo male presents complaining of SOB while jogging and progressive fatigue for 3 weeks. He usually runs several miles a day. He has felt well aside from this, has not had fever, weight change, loss of appetite, muscle aches, sweats, bruising, or bleeding.
WBC: 11.3 / µL w/ abnormal WBCs on peripheral blood smear. Differential shows 60% blasts positive for CD10, CD19, and CD34, but negative for CD3 and CD20. What are the expected findings in the bone marrow? |
- Cells with cytogenetic abnormalities
- Hypercellularity |
|
Case 1: 29 yo male presents complaining of SOB while jogging and progressive fatigue for 3 weeks. He usually runs several miles a day. He has felt well aside from this, has not had fever, weight change, loss of appetite, muscle aches, sweats, bruising, or bleeding.
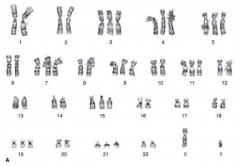
WBC: 11.3 / µL w/ abnormal WBCs on peripheral blood smear. Differential shows 60% blasts positive for CD10, CD19, and CD34, but negative for CD3 and CD20. Results of cytogenetic analysis of diagnostic BM shown above. No translocations identified. What do these cytogenetic results imply? |
This is a favorable cytogenetic finding for the diagnosis of B-ALL, the following are the favorable prognostic features:
- Hyperploidy (extra chromosomes) - Trisomy of chromosomes 4 and 7 (10 is also favorable if present) |
|
Case 1: If this patient were an adolescent male presenting with a large mediastinal mass, what would be an expected in the mediastinal biopsy?
|
CD3(+) tumor cells (because it is a T cell neoplasm)
|
|
What diagnosis and kind of symptoms would you predict for this patient?
|
CLL: soccer ball chromatin or ginger snap chromatin
- Often asymptomatic - Indolent, non-symptom presentation - Diagnose as incidental finding on routine CBC - May have extensive adenopathy and organomegaly |
|
What is the expected patient profile for this finding?
|
Older patient (more common in CLL)
|
|
Is this expected to be immunophenotypically normal or abnormal? Monoclonal or polyclonal?
|
- Immunophenotypically abnormal
- Monoclonal B cells (they all look the same so probably from the same precursor) |
|
What diagnosis would you predict for this patient?
|
Infectious Mononucleosis
|
|
What is the expected patient profile for this finding?
|
Young teenager (more common for Infectious Mononucleosis)
|
|
Is this expected to be immunophenotypically normal or abnormal? Monoclonal or polyclonal?
|
- Immunophenotypically normal
- Polyclonal B cells (they all look different so they are reactive lymphocytes) |
|
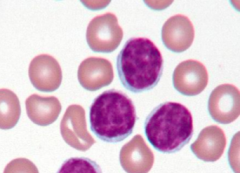
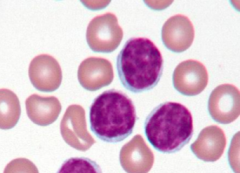
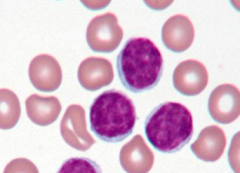
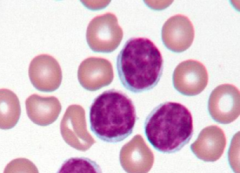
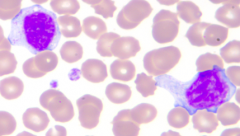
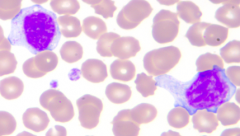
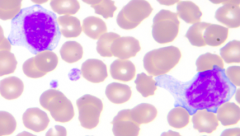
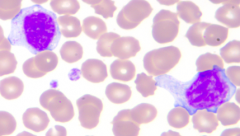
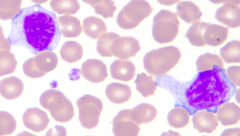
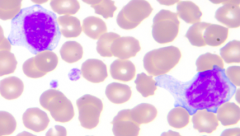
Case 3: 65 yo female presents with fatigue for 6 months. Discomfort in LUQ recently and decrease in appetite. Several, firm, mobile, lymph nodes 1-1.5 cm in posterior triangles on both sides of neck and tip of spleen is palpable.
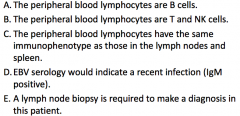
WBC count: 60,000/µL w/ 90% lymphocytes, 8% neutrophils, 2% eosinophils. Hemoglobin 9g/dL and platelets 50,000/µL. Which is true? |
C - peripheral blood lymphocytes have the same immunophenotype as those in the lymph nodes and spleen
Reactive processes don't get above 10,000/µL, so you know this is neoplastic, therefore whatever is in lymph nodes and spleen should be the same as in blood |
|
|
Case 3: 65 yo female presents with fatigue for 6 months. Discomfort in LUQ recently and decrease in appetite. Several, firm, mobile, lymph nodes 1-1.5 cm in posterior triangles on both sides of neck and tip of spleen is palpable.
WBC count: 60,000/µL w/ 90% lymphocytes, 8% neutrophils, 2% eosinophils. Hemoglobin 9g/dL and platelets 50,000/µL. What is the absolute lymphocyte count in this case? |
54,000 / µL
|
|
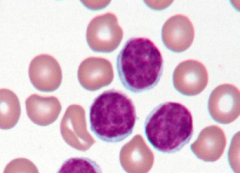
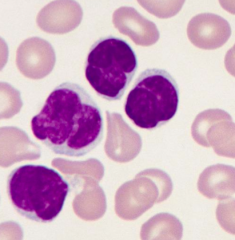
Case 3: 65 yo female presents with fatigue for 6 months. Discomfort in LUQ recently and decrease in appetite. Several, firm, mobile, lymph nodes 1-1.5 cm in posterior triangles on both sides of neck and tip of spleen is palpable.
WBC count: 60,000/µL w/ 90% lymphocytes, 8% neutrophils, 2% eosinophils. Hemoglobin 9g/dL and platelets 50,000/µL. Based on the peripheral smear provided, what is the most likely immunophenotype of the lymphocytes? |
CD5+, CD20+, CD23+ cells expressing kappa (or lambda, just can only be one) light chain only (immunophenotype for CLL)
|
|
|
Case 3: 65 yo female presents with fatigue for 6 months. Discomfort in LUQ recently and decrease in appetite. Several, firm, mobile, lymph nodes 1-1.5 cm in posterior triangles on both sides of neck and tip of spleen is palpable.
WBC count: 60,000/µL w/ 90% lymphocytes, 8% neutrophils, 2% eosinophils. Hemoglobin 9g/dL and platelets 50,000/µL. What is the most likely reason the patient is cytopenic (anemia and thrombocytopenia)? |
Bone marrow replaced w/ neoplastic cells
|
|
|
Case 3: 65 yo female presents with fatigue for 6 months. Discomfort in LUQ recently and decrease in appetite. Several, firm, mobile, lymph nodes 1-1.5 cm in posterior triangles on both sides of neck and tip of spleen is palpable.
WBC count: 60,000/µL w/ 90% lymphocytes, 8% neutrophils, 2% eosinophils. Hemoglobin 9g/dL and platelets 50,000/µL. When the diagnosis (CLL) is established, the patient opts for no treatment. What kind of clinical course does CLL have? |
Indolent clinical course
|
|
|
Case 3: 65 yo female presents with fatigue for 6 months. Discomfort in LUQ recently and decrease in appetite. Several, firm, mobile, lymph nodes 1-1.5 cm in posterior triangles on both sides of neck and tip of spleen is palpable.
WBC count: 60,000/µL w/ 90% lymphocytes, 8% neutrophils, 2% eosinophils. Hemoglobin 9g/dL and platelets 50,000/µL. Three months later she presents w/ night sweats, fever, and 20 lb weight loss and a lump in her neck. Biopsy reveals aggressive lymphoma. What poor prognostic indicators of CLL might have been present at diagnosis? |
- Presence of deletions of 11q and 17p
- Lack of somatic hypermutation - Expression of ZAP-70 (protein that augments signals produced by Ig receptor) |
|
|
What defines an absolute lymphocytosis?
|
≥ 4000 lymphocytes / µL
|
|
|
What are the benign causes of lymphocytosis?
|
* Infectious mononucleosis (common)
* IM-like syndromes, eg, CMV, adenovirus, acute HIV, toxoplasmosis (common) * Transient stress lymphocytosis (common) - Other viruses (hepatitis, chickenpox) - Drugs - Whooping cough - Persistent polyclonal B-cell lymphocytosis |
|
|
What are the neoplastic causes of lymphocytosis?
|
- Leukemic lymphoma
- Sézary syndrome - Hairy cell leukemia - T/NK cell large granular lymphocytic leukemia - Chronic Lymphocytic Leukemia - Adult T-cell Leukemia |
|
|
What are the immunophenotypical signs of AML?
|
- CD13
- CD14 - CD15 - CD33 - CD117 |
|
|
What are the immunophenotypical signs of ALL?
|
- CD3
- CD19 - CD20 |
|
|
How do AML and ALL compare in terms of common age of onset?
|
- AML: ADULTS > children
- ALL: CHILDREN > adults |
|
|
How do AML and ALL compare in terms of morphology?
|
- AML: myeloblasts ± Auer rods (may have granulocytic, erythroid, megakaryocytic, or monocytic differentiation)
- ALL: lymphoblasts |
|
|
What is the pre-leukemic state for AML vs ALL?
|
- AML: myelodysplasia syndrome
- ALL: no pre-leukemic state |
|
|
How do you classify AML types?
|
- AML w/ recurrent cytogenetic abnormalities
- AML w/ myelodysplasia associated changes - AML / MDS, therapy-related - AML, not otherwise specified |
|
|
How do you classify ALL types?
|
85% B-cell ALLs
- t(12;21) most common in kids - t(9;22) poor prognosis 15% T-cell ALLs - Adolescent males w/ mediastinal masses - Worse prognosis |
|
|
What are the good prognostic factors for B-ALL?
|
- 1-10 years
- Hyperdiploidy (>50 chromosomes) - t(12;21) |
|
|
What are the poor prognostic factors for B-ALL?
|
- < 1 yo, >10 yo
- t(9;22) - Hypodiploidy (<45 chromosomes) - Elevated WBC count (>100,000/µL) - CSF involvement - Marrow involvement at day 15 |
|
|
What is the classic presentation of T-ALL?
|
Mediastinal mass in adolescents - thymic lymphoma
|
|
|
How does T-ALL compare to B-ALL morphologically?
|
- May appear identical morphologically
- T-ALL flow cytometry: CD3+, CD1a+ |
|
|
What are the types of Small B cell Leukemia / Lymphomas?
|
- Mantle Cell Lymphoma
- CLL/SLL - Follicular Lymphoma - MALT Lymphoma |
|
|
How do you distinguish Mantle Cell Lymphoma from the other small B cell leukemia / lymphomas?
|
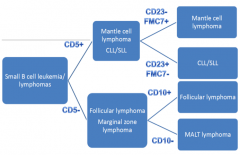
CD5+
CD23- / FMC7+ |
|
|
How do you distinguish CLL/SLL from the other small B cell leukemia / lymphomas?
|
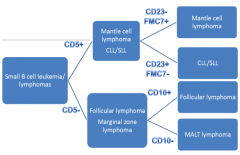
CD5+
CD23+ / FMC7- |
|
|
How do you distinguish Follicular Lymphoma from the other small B cell leukemia / lymphomas?
|
CD5-
CD10+ |
|
|
How do you distinguish MALT Lymphoma / Marginal Zone Lymphoma from the other small B cell leukemia / lymphomas?
|
CD5-
CD10- |
|
|
Which of the small B cell leukemia / lymphomas are CD5+? How do you distinguish them?
|
- Mantle Cell Lymphoma: CD23- / FMC7+
- CLL/SLL: CD23+/FMC7- |
|
|
Which of the small B cell leukemia / lymphomas are CD5-? How do you distinguish them?
|
- Follicular Lymphoma: CD10+
- MALT Lymphoma / Marginal Zone Lymphoma: CD10- |
|
|
What are the good prognostic indicators in CLL/SLL?
|
- Low Rai stage
- Mutated IGHV gene - Deletion 13q |
|
|
What are the poor prognostic indicators in CLL/SLL?
|
- High Rai stage
- Unmutated IGHV gene - CD38 / ZAP-70 expression - Deletion 11q, 17p |
|
|
What is the staging system for CLL/SLL? Implications?
|
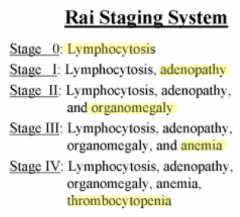
Rai Staging System
- 0: lymphocytosis - I: + adenopathy - II: + organomegaly - III: + anemia - IV: + thrombocytopenia The lower the stage the better the prognosis |
|
|
What neoplasms present with atypical lymphocytes ± lymphocytosis?
|
- CLL/SLL
- Leukemic lymphoma (follicular, mantle, etc) - Hairy cell leukemia - Adult T cell leukemia/lymphoma - Sézary syndrome |
|
|
What is the characteristic presentation of Hairy Cell Leukemia?
|
Middle aged (40-60yo) male
|
|
|
What are the exam findings of Hairy Cell Leukemia?
|
*Indolent
- Splenomegaly (d/t red pulp infiltration) - Pancytopenia - Lymphocytes w/ "hairy projections" ± lymphocytosis - TRAP+ cells - Fibrosis in marrow ("dry tap") |
|
|
What causes splenomegaly in Hairy Cell Leukemia?
|
Red Pulp infiltration
|
|
|
What are the morphological characteristics of Hairy Cell Leukemia?
|
Lymphocytes have 'hairy projections'
|
|
|
What are the features of Hairy Cell Leukemia on flow cytometry?
|
Bright CD11c and CD22 expression
|
|
|
What cells are proliferating in Sézary Syndrome?
|
CD4+ T cells
|
|
|
What is the triad of symptoms in Sézary Syndrome?
|
- Erythroderma
- Generalized lympadenopathy - Circulating Sézary cells |
|
|
What are "Sézary cells"?
|
CD4+ T cells that have "cerebriform" nuclei (look like brains)
|
|
|
What is Sézary Syndrome related to? Symptoms?
|

Mycosis Fungoides: patches, plaques
|
|
|
What can Sézary Syndrome / Mycosis Fungoides transform into?
|
Aggressive T cell tumor
|
|
|
What kind of cells are affected by Adult T-cell Leukemia / Lymphoma?
|
CD4+ T-cells
|
|
|
What infection is Adult T-cell Leukemia / Lymphoma associated with?
|
HTLV-1 infection (most w/ infection do NOT develop ATLL)
|
|
|
Where is Adult T-cell Leukemia / Lymphoma more common?
|
Japan, Caribbean, and Africa
|
|
|
What is the appearance and symptoms of Adult T-cell Leukemia / Lymphoma?
|
- "Flower cell" w/ lymphocytosis
- Hypercalcemia - Aggressive |