Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
143 Cards in this Set
- Front
- Back
|
Kinematics
|
Type of motion without regard for forces producing the motion
|
|
|
Osteokinematics
|
movements of bony partners/segments that make up a joint
|
|
|
Arthrokinematics
|
minute movements occurring within a joint and b/w joint surfaces
|
|
|
Frontal Plane
|
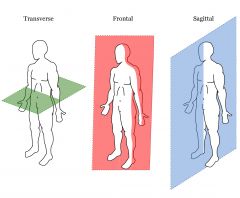
Also know as Coronal Plane
*Divides body into ANTERIOR:POSTERIOR |
|
|
Motions within the frontal plane
|
Abduction/Adduction (Hip, shoulder, digits)
Ulnar/Radial Deviation Lateral Flexion (Neck, Trunk) |
|
|
Sagittal Plane
|
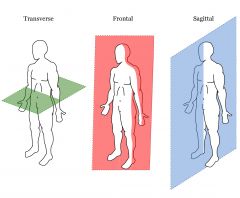
Divides body into LEFT:RIGHT
|
|
|
Motions in the sagittal Plane
|
Flexion/Extension
Dorsiflexion/Plantar Flexion |
|
|
Transverse Plane
|
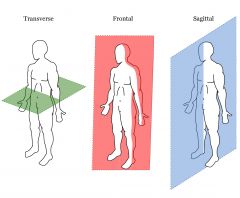
Also known as Horizontal Plane (parallel to horizon/floor)
Divides body into: UPPER:LOWER |
|
|
Motions occurring in the transverse plane
|
Medial/Lateral rotation (hip/shoulder)
Pronation/Supination (Forearm) Eversion/Inversion (Foot) |
|
|
Degrees Of Freedom
|
# of planes a joint moves within
|
|
|
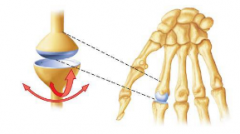
Uniaxial Joint
|
Hinge, Pivot
Ex) Humerounlar, Radioulnar **1 DEGREE OF FREEDOM |
|
|
Condyloid Joint
|
Biaxial (Frontal + Sagittal)
Spherical Convex on concave (metacarpophalangeals) |
|
|
Ellipsoidal Joint
|
Biaxial (Frontal + Sagittal)
somewhat flattened convex on deep concave Wrist |
|
|
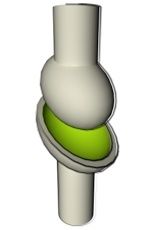
Saddle Joint
|
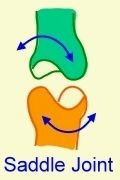
Biaxial (Frontal + Sagittal, sometimes transverse)
concave+convex perpendicular Thumb |
|
|
Triaxial Joint
|

3 Degrees of freedom (all 3 planes)
Ball & Socket Joint Glenohumeral, Hip |
|
|
Concave ON Convex
|
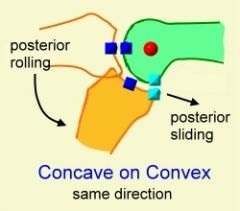
conCAVE moving on conVEX surface
move in SAME direction EX) Tibia on Femur |
|
|
Convex on Concave
|
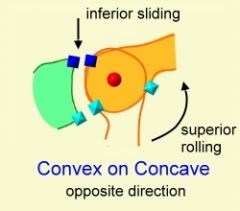
VEX moving on CAVE
move in OPPOSITE direction EX) Humerus on scapula, shoulder abduction |
|
|
Closed-Pack Position
|
Maximum surface area contact occurs
Capsuloligamentous tissues are taut Minimal amount of accessory motion |
|
|
Open-Pack Position
|
Any position but “close-packed”
Joint surfaces do not fit congruently Also referred to as loose-packed position “Resting” position |
|
|
Newtons 1st Law
|
Inertia:
A body at rest will stay at rest, and a body in motion will stay in motion, until acted on by an outside force Clinical EX) ath cant lift leg, clinician helps by lifting/starting the motion and then they can raise it (overcome inetia @ begining of motion) |
|
|
Newtons 2nd Law
|
Acceleration is proportionate to the magnitude of the net forces acting on it and inversely proportionate to the mass of the body.
Greater force needed to move/stop BIG rather than small |
|
|
Newtons 3rd Law
|
Action-Reaction:
For every action force there is an equal and opposite reaction force. Ex:) 2 football players push against each other, no motion if A then pushes more than B, B will fall back |
|
|
1st class lever
|

MECHANICAL ADVANTAGE depends on which lever arm is longer, the resistance, or force. Equilibrium can be produced by balancing
EX) See Saw Force item closer to axis, resistance longer arm, resistance arm giving MECHANICAL ADVANTAGE EX) Strong athlete, I push at wrist for MMT |
|
|
2nd Class Lever
|

Point of resistance b/w axis and force, Lever arm of resistance is shorter than of force.
*FORCE advantage |
|
|
3rd Class Lever
|

Axis of rotation at end; force arm smaller than resistance arm.
Most common in human body. Designed to produce speed of distal segment. OPEN CHAIN KINEMATICS |
|
|
Mechanical Advantage
|
Ratio between the length of the force arm and the length of the resistance arm
MA only with arm length; longer arm length=task easier regardless of the amount of force that is working. |
|
|
Isometric contraction
|
Generates force without changing length
|
|
|
Isotonic Contraction
|
Tension remains the same, length changes.
CONCENTRIC, ECCENTRIC |
|
|
Concentric contraction
|
muscle shortens while generation force
EX)quads in getting up from a chair produces acceleration of body segments |
|
|
Eccentric contraction
|
Muscle lengthens/elongates while under tension.
EX) Biceps in deceleration phase of a pitch, slows down elbow often against gravity as muscles control speed of gravity moving joint ( |
|
|
Isokinetic
|
contraction occurs when rate of movement is constant
EX) BIODEX |
|
|
Agonist
|
Prime Movers
Principle muscle producing a motion/maintaining static posture |
|
|
Antagonist
|
-Muscle that acts in opposition to movement of agonist
-Inactive during activity, then passively elongates or shortens (opp of agonist) -responsible to returning to original position EX) fork to mouth, bicep is agonist, triceps elongate to allow motion, then triceps contract and bicep becomes antagonist to allow return to position |
|
|
Synergist
|
muscle contracts at same time as agonist
*Identical movement* (Brachioradialis w/ brachialis in elbow flexion) *Obstruct unwanted agonist action* (Wrist extensors preventing wrist flexion when grasping something) *Stabalize proximal to allow distal movement* |
|
|
Muscle Size: LENGTH
|
end-to-end, series
provide "Speed of motion" Longer muscles provide mobility |
|
|
Muscle Size: WIDTH
|
side-to-side, parallel
Associated with a greater ability to produce force. Shorter muscles provide stability. |
|
|
primary function of shoulder complex
|
position hand for function
|
|
|
SITS
|
Supraspinatus
Infraspinatus Teres Minor Subscapularis |
|
|
Supraspinatus
|
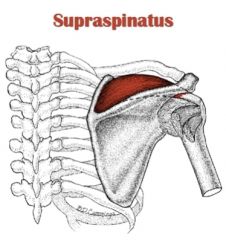
Origin: Supraspinous fossa of scapula
Insertion: Lesser tubercle of humerus Action: ABduction of GH joint |
|
|
Infraspinatus
|
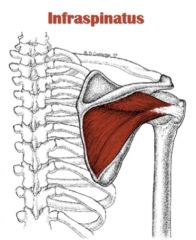
Origin: Infraspinous fossa of scapula
Insertion: Greater Tubercle of humerus Action: LAT rotation, ADDuction of GH |
|
|
Teres Minor
|
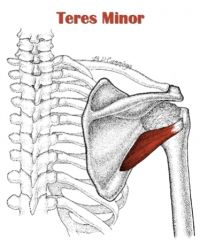
Origin: lower Lateral border of scapula
Insertion: Greater Tubercle of humerus Action: LAT rotation, ADDuction of GH |
|
|
Subscapularis
|
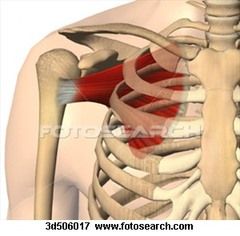
Origin: median 2/3 of subscapular fossa
Insertion: Lesser tuberosity of humerus, capsule of shoulder joint Action: medial rotation of GH |
|
|
Glenohumeral Capsular Reinforcers
|
Superior/middle/inferior GH ligaments
Coracohumeral ligament Long head of biceps/triceps Rotator cuff tendons blend with capsule |
|
|
Scapular Stabalizers
|
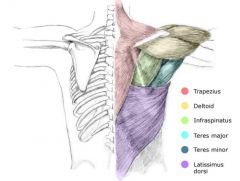
Serratus anterior
Trapezius Rhomboid major/minor Pectoralis minor Levator scapulae |
|
|
Glenohumeral Stabalizers
|
(Rotator cuff + biceps+triceps)
Supraspinatus Infraspinatus teres minor Subscapularis Biceps Triceps brachii |
|
|
Shoulder Complex Large Movers
|
Deltoid
Latissimus dorsi Teres major Pectoralis major Coracobrachialis |
|
|
Shoulder Complex:Passive Stabilizers
|
Sternoclavicular & acromioclavicular support= LIGAMENT
GH & scapulothoracic support= MUSCLES @ rest, humeral head suspended by: 1.Ligaments—superior GH; coracohumeral 2.Negative Intra-articular pressure |
|
|
Shoulder Complex: Dynamic Stablizers
|
Upper trapezius—low-level activity at rest
Rotator cuff Biceps |
|
|
Long Thoracic Nerve Palsy
|
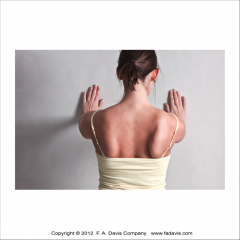
Paralysis of SERRATUS ANTERIOR= Winging Scapula
Trauma to superficial long nerve. |
|
|
Glenohumeral Joint Arthrokinematics
|
Flexion/extension—spin
Abduction—superior roll; inferior glide Lateral rotation—posterior roll; anterior glide Medial rotation—anterior roll; posterior glide |
|
|
Elbow:
Type of Joint Degree(s) of freedom Motions/planes ROM |
Hinge Joint
1 degree of freedom (Sagittal Plane) Extension/Flexion 0-145 |
|
|
Elbow Capsule is taught when?
|
Anterior aspect taut in extension
Posterior aspect taut in flexion |
|
|
Elbow Flexors
|
Brachialis—largest of all elbow flexors
Biceps brachii Brachioradialis |
|
|
Brachioradialis
|

Origin: Lat.Supracondylar ridge
Insertion: styloid process Action: Elbow flexion, supination/pronation radioulnar |
|
|
Biceps Brachii
|
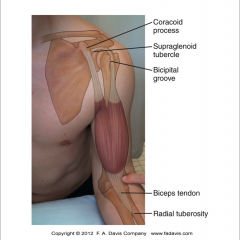
Origin: Long head- Bicipital glenoid groove
Short Head- coracoid process Insertion: Radial Tuberosity Action: GH flexion, elbow flexion, supination |
|
|
Elbow Extensors
|
Triceps
Anconeus |
|
|
Tricep Brachii
|

Origin: infraglenoid process of scapula
Insertion:olecranon process Action:extension |
|
|
Anconeus
|

Origin: Lateral Epicondyle
Insertion: Proximal Ulna, distal to olecranon process Action: Extension |
|
|
Forearm Supinators
|
Biceps brachii
Supinator |
|
|
Forearm Pronators
|
Pronator teres
Pronator quadratus |
|
|
Forearm Synergists
-muscle -action |
-Biceps/triceps
-flexion/extension |
|
|
Lister's tubercle
|
Radial Dorsal Tubercle (palatable in medial 2/3 of wrist)
Acts as a pulley for the extensor pollicis longus (EPL) |
|
|
Styloid Process
|
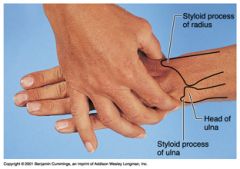
Radial process
Bigger bump |
|
|
Common carpals to remember
|
Capitate—occupies central position
Scaphoid—most commonly fractured carpal Lunate—most frequently dislocated carpal Pisiform—serves as attachment for flexor carpi ulnaris (FCU) |
|
|
Carpals in rows proximal->distal
(pronated view) |
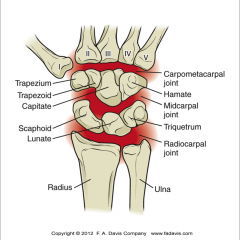
Scaphoid Trapezium
Lunate Trapezoid Triquetrium Capitate Pisiform Hamate |
|
|
Phalanges
|
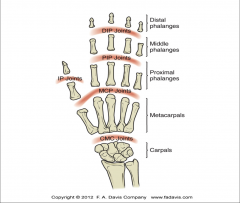
Thumb—two: proximal and distal
Digits 2–5—three: proximal, middle, and distal Base—biconcave Distal heads—bicondylar |
|
|
Hand Bones act in Con? on Con?
|
Convex on Concave
|
|
|
Wrist extensors
|
Extensor carpi radialis brevis (ECRB)
extensor carpi radialis longus (ECRL) extensor carpi ulnaris (ECU) Origin: Lat. Epicondyle |
|
|
Wrist Flexors
|
Flexor carpi radialis (FCR) (FCU)
flexor digitorum superficialis (FDS) flexor digitorum profundus (FDP) Palmaris Longus (PL)—Flexor Palmaris Longus Origin: Medial Epicondyle |
|
|
Power Grip
|
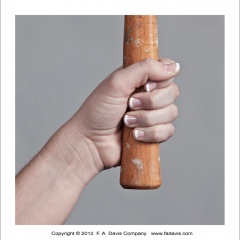
Incorporates entire hand
Is used for gross grasping activities Is involved in holding an object between partially flexed fingers and palm while thumb provides counterpressure -hook, cylindrical, spherical, fist |
|
|
Precision Grip
|

Is used for accuracy and refinement; object manipulation
Thumb abducted—ready to oppose |
|
|
Swan Neck Deformity
|
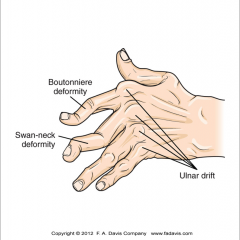
PIP hyperextension
DIP flexion |
|
|
Boutonnieres Deformity
|
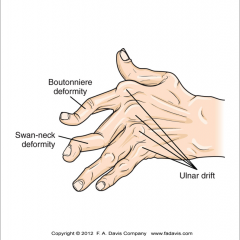
PIP flexion
DIP hyperextension |
|
|
Pitching Phases
|
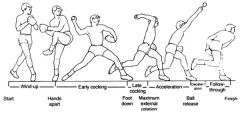
Windup
Cocking: Early, Late Acceleration/Deceleration Follow Through |
|
|
Head Palpatable Structures
|
Hyoid bone C3
Thyroid cartilage C4–5 Cricoid cartilage C6 Manubrium T4 |
|
|
Neck Palpatable Structures
|
Inferior angle of scapula T7 (spinous process)
Xiphoid process T10 (body) Iliac crest L4 Posterior superior iliac spine (PSIS) |
|
|
Atlanto-occipital (AO) joints
|
Two degrees of freedom
Flexion/extension; small amount of side bending |
|
|
Atlanto-axial (AA) joints
|
Facet joints nearly horizontal
50% of cervical spine rotation occurs at AA joints |
|
|
Lumbar Joint movement
|
L1–5 facet joint orientation—sagittal plane
Facilitates flexion/extension ROM Little or no rotation L5–S1 facet joint orientation—frontal plane Provides bony stabilization of L5 on S1 |
|
|
Slippage of L5 on S1
|
spondylolisthesis
|
|
|
Sacroiliac Joint
|
Very small amounts of motion (1–3 mm)
Diarthrodial joint Motions Anterior—posterior rotation (M-L axis) Abduction—adduction (A-P axis) Medial—lateral rotation (vertical axis) |
|
|
SI Nutation
|
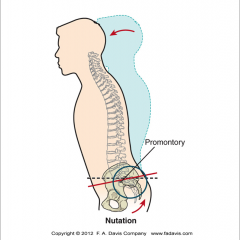
sacrum moves anteriorly and inferiorly while the coccyx moves posteriorly relative to the ilium
|
|
|
SI Counternutation
|
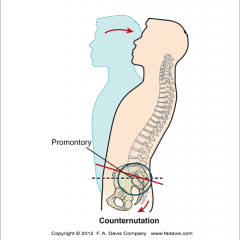
sacrum moves posteriorly and superiorly while the coccyx moves anteriorly relative to the iliu
|
|
|
Primary Hip/Pelvis function
|
Primary function is power production during closed chain activities.
locomotion |
|
|
Angle of Inclination
-typical adult |
Anatomic and mechanical axes of the femur
typical adult=125 degrees |
|
|
Coxa Valga
|
Greater angle of inclination than 130 degrees
Predisposes to hip instability, dislocations/sublux's, leg may appear longer |
|
|
Coxa Vara
|
Angle of inclination less than 125 degrees
predesposes to femoral FX |
|
|
Angle of Torsion
|
Transverse plane neck-shaft angle of the femur
Anteversion: angles greater than normal (10-20 degrees) can result in joint instability. "pigeon toe" Retroversion: Not as common; decrease in this angle presents with “out-toeing,” |
|
|
Pelvic Motions on femur
-planes |
Anterior/posterior tilt—sagittal plane
Lateral tilt—frontal plane Protraction/retraction—transverse plane |
|
|
Femur on Pelvis motions
|
Flexion/extension—sagittal plane
Abduction/adduction—frontal plane Medial/lateral rotation—transverse plane |
|
|
Hip Flexors
|
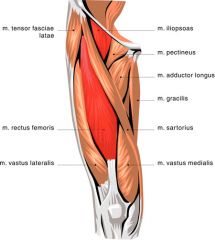
Iliopsoas
Rectus femoris Sartorius Pectineus Tensor fascia latae |
|
|
Hip Adductors
|
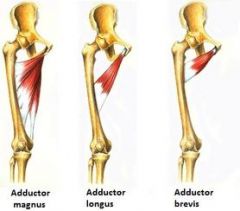
Adductor magnus
Adductor longus Adductor brevis Gracilis |
|
|
Hip Extensors
|

Gluteus maximus
Biceps femoris Semitendinosus Semimembranosus |
|
|
Hip Abductors
|
Gluteus medius
Gluteus minimus Tensor fascia latae |
|
|
Hip LATERAL rotators
|
Piriformis
Gemellus superior and inferior Obturator internus and externus Quadratus femoris |
|
|
Hip Medial Rotators
|
Trick question
no primary medial rotators |
|
|
Most powerful hip flexor
|
Iliopsoas
|
|
|
Most powerful Hip Extensor
|
Gluteus maximus
|
|
|
Strongest Hip ABductor
|
Gluteus medius strongest hip abductor
|
|
|
Line of pull: Piriformis
|
Lateral rotator = hip is extended
medial rotator= hip is flexed. |
|
|
Why is the knee, the largest joints in our body, so often injured?
|
because it is positioned between two long bony levers
|
|
|
Patella functions
|
Increase internal moment arm of quadriceps
Centralize force of quadriceps pull Reduce tendon and friction forces Contribute to overall knee stability Provide bony protection |
|
|
Menisci serve to:
|
Deepen socket and improve congruency
Absorb and distribute forces/increase surface area Promote lubrication of joint Prevent joint capsule from intruding into joint space Partially protect against excessive motion Move anteriorly w/ knee extension posteriorly w/ knee flexion |
|
|
Knee Flexion
|
Flexion
On average, to 135° Limited by soft tissue approximation |
|
|
Knee Extension
|
Extension
To 0°; often hyperextends but not past 15° Limited by capsular tightening |
|
|
Screw Home Mechanism
|
lateral tibial rotation in terminal extension (open kinematic chain)
|
|
|
Patellar movement in open/closed kinematic chains
|
Open kinematic chain—patella moves on femur
Maximum contact occurs at 90° of flexion. Closed kinematic chain—femur moves on patella |
|
|
Patella Baja
|
patella above joint line
|
|
|
Patella Alta
|
patella below joint line
|
|
|
Q Angle
|
Line drawn from the ASIS -->central patella and
second line drawn from central patella--> tibial tubercle |
|
|
Increased Q angle is caused by:
|
genu valgum
increased femoral anteversion external tibial torsion Laterally positioned tibial tuberosity Tight lateral retinaculum |
|
|
Normal Q Angles: Female/Male
|
17-18, 13-14
|
|
|
Knee Extensors
|
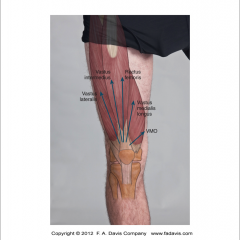
Quadriceps femoris:
Vastus lateralis Vastus medialis oblique and vastus medialis longus Vastus intermedius Rectus femoris |
|
|
Knee Flexors
|
Hamstrings
Gastrocnemius—plantaris—popliteus Gracilis Sartorius |
|
|
Tibial Rotators
|
Medial:
Semitendinosus/semimembranosus Gracilis/sartorius Popliteus Lateral: Biceps femoris |
|
|
Knee extensors function to:
|
Stabilize—isometric
Decelerate—eccentric Accelerate—concentric |
|
|
Normal Hamstring:Quadriceps ratio
|
2:3, or 66%
|
|
|
How many bones and joints are in the foot/ankle
|
26 bones and 34 joints
|
|
|
% Of weight bearing during ambulation
|
Tibia= 90% of weight
Fibula=10% |
|
|
Malleolus' (Fibula/tibia)
|
Prominent lateral malleolus (Fibula)
Projects further distal than medial malleolus Sits more posterior than medial malleolus (tibia) |
|
|
What forms the transverse arch?
|
Cuneiforms
(Medial, Intermediate, Lateral, ) |
|
|
Motions of the foot in the transverse plane:
|
Abduction and adduction
|
|
|
What motions occur at the subtalar joint
|
Pronation/supination
Primary motion is that of inversion (30°)/eversion (20°). |
|
|
Define Locomotion
|
Moving from one place to another
|
|
|
Define Gait
|
Achieving upright locomotion on foot
Walking, running, or jogging |
|
|
Define Ambulation
|
Type of locomotion
Used clinically—with or without assistive device |
|
|
Functional stance at ankle
|
Line of gravity falls anterior to talocrural joint.
Motion is resisted by calf group—soleus. |
|
|
Functional stance @ Knee
|
Line of gravity falls anterior to knee joint.
Motion is resisted by passive posterior knee tissues. |
|
|
Functional stance @ hip
|
Line of gravity falls posterior to hip axis
Slight iliacus activity is required to counteract gravity |
|
|
Functional stance @ Head/Trunk
|
Line of gravity falls on concavity of spinal curves.
Thoracic erector spinae are active to maintain posture Cervical extensors balance occiput on atlas. |
|
|
Gait Cycle: Stride
|
Heel contact to heel contact of same lower extremity
Divided into “stance” and “swing” phases **Stance = 60%; swing = 40% **Two periods of double limb support |
|
|
Stance Subdivisions
|
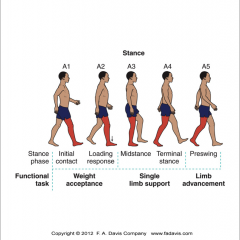
Initial contact (IC)
Loading response Midstance Terminal stance Preswing |
|
|
Swing subdivisions
|
Initial swing
Midswing Terminal swing |
|
|
Step vs. Stride
|
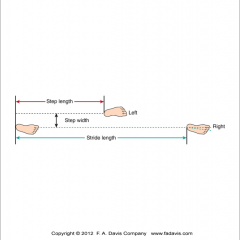
one complete stride (gait cycle) is 2 steps
|
|
|
Hip ROM: gait cycle
|
10° extension
25–30° flexion 15° adduction 5° abduction 8–14° medial/lateral rotation |
|
|
Knee ROM:gait cycle
|
Full extension
60° of flexion 3–8° in frontal plane—abduction 10–20° in transverse plane |
|
|
Ankle/Foot ROM:gait cycle
|
10° dorsiflexion
20° plantarflexion 5° of eversion/pronation 11° of inversion/supination |
|
|
Initial Contact muscles
|
Tibialis anterior and gastrocnemius-soleus cocontract to maintain stability.
Hamstrings decelerate knee as limb prepares to land. Quadriceps cocontract with hamstrings. Hip is in slight flexion and is stabilized by gluteus maximus/medius. |
|
|
Midstance muscles
|
single-limb support
Stability is primary requirement. Gastrocnemius and soleus maintain ankle stability. Knee muscles are fairly quiet; they rely on gastrocnemius. Gluteus medius works hard to stabilize pelvis in frontal plane. |
|
|
Terminal and Preswing muscles
|
Is associated with primarily concentric activity for propulsion.
Gastrocnemius is primary contributor. Knee flexion occurs almost passively from hip flexion and ankle plantarflexion. |
|
|
Immature Walking
|
baby starts b/w 11 and 15 months
Wide-based gait/poor pelvic mobility Stepping initiated at hips with stiff knees IC made with entire foot **Short steps; increased cadence **Exaggerated periods of double limb support Upper extremities used for balance |
|
|
Gait changes in cerebral palsy
|
Increased hip flexion/adduction/medial rotation
Weak hip extensors/abductors/quadriceps and leg muscles Increased energy cost of ambulation |
|
|
Gait change in running vs walking
|
Swing is longer than stance.
Two periods of no limb support occur—double float. Walking is modeled as an inverted pendulum. Running is modeled as a pogo stick. Velocity, cadence, and step length increase. Ground reaction forces increase. Running pace is 2–5x > walking speeds. |