![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
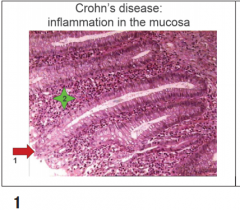
Crohn’s disease in mucosa
Gross< Thick wall:OedemaFibrosisMuscle hypertrophy Alternation of affected and normal areas Sharp border Microscopic picture Inflammation in the mucosa Crypt abscesses Chronic mucosal damage Ulcers and deep narrow fissures Transmural inflammation Non-necrotising granulomas Irregular muscle layer thickening due to fibrosisand reduplication Nerve hyperplasia Possible vasculitis |
|
|
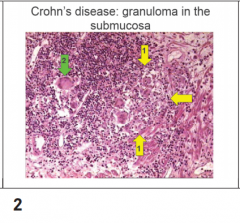
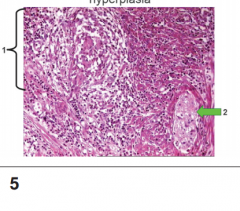
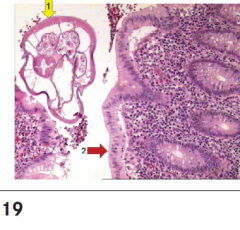
Crohn’s disease in submucosa 1.Granuloma 2.Gaint cells |
|
|
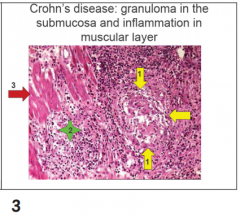
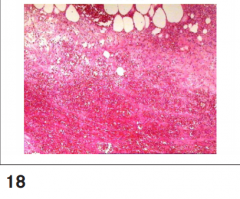
Crohn’s disease granuloma in submucosa 1.granuloma without necrosis 2.inflammation 3.muscle layer |
|
|
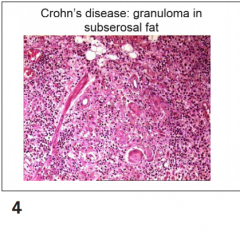
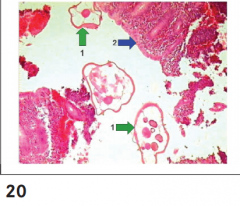
Crohn’s disease granuloma in subserosal fat; Inflammatory cells, granlomma central with fat cells |
|
|
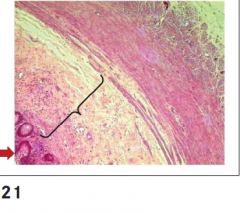
Crohn’s disease: granuloma and nerve hyperplasia. 1. Granuloma 2. Nerve hyperplasia |
|
|
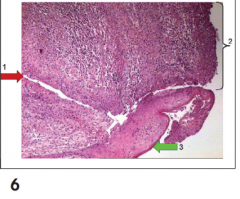
Crohn’s disease wide fissure 1.Fissure ulcer 2.Wide ulcer 3.Rectal epithelium |
|
|
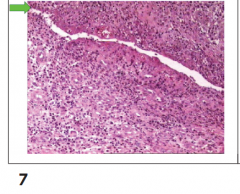
Crohn’s disease; fissure like ulcer |
|
|
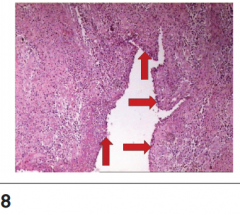
Crohn’s disease; deep ulcer |
|
|
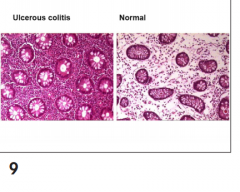
Mucosa of the large intestine - Difference severe inflamatory cells - Loss of goblet cells |
|
|
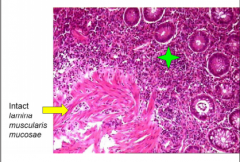
Ulcer colitis - Loss of goblet cells - Crypt abcess |
|
|
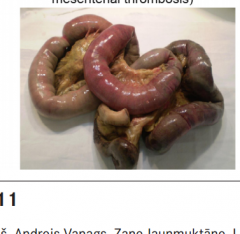
Necrosis of small intestine due mesenterial thrombosis; 1. Edema 2. Hemorrhage 3. Necrosis(dark) |
|
|
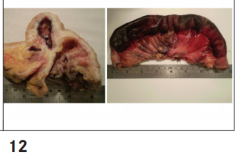
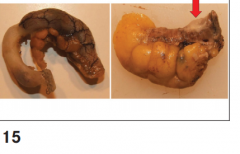
Hernia sac of large bowel showing hemorrhagic necrosis; Middle - complete necrosis |
|
|
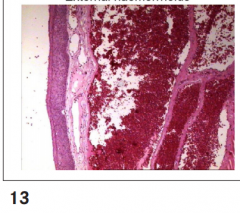
External haemorrhiodes - Dilated veins with blood clots inside of it. we pay attention to |
|
|
Internal hemorrhiodes, -Mucosa is dilated Haemorrhage overlaying |
|
|
Acute appendicitis; Initial acute appendicitis Flegmonous appendicitis Gangrenous appendicitis Perforation and purulent peritonitis * Diffuse appendicitis In early acute appendicitis, subserosal vessels are congested,and a modest perivascular neutrophilic infiltrate is presentwithin all layers of the wall. |
|

|
Phlegenomous appendicitis - purlent infiltation muscle layer: neutrophilic infiltrate is present within all layers of the wall. |
|
|
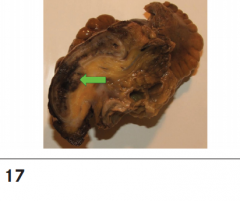
Gangrene appendicitis with perforation, to the left is there appendicitis with perforation into fat cells |
|
|
Ganagrenous appendicitis - complete necrosis |
|
|
Appendicular enteriobiosis - parasite(eosinophils) |
|
|
Appendicular enterbiosis - parasites - infiltereted e |
|
|
Chronic appendicitis, thickning of submucosa, increased level of lymphocytes. |
|
|
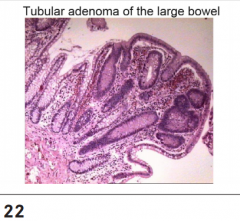
Tubular adenoma of large bowel; |
|

|
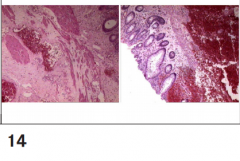
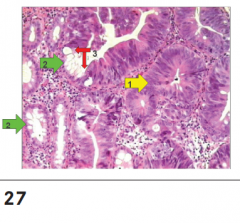
Epithelia dysplasia in adenoma, irregular shaped of cells, profliferation, greater lumen,loss of goblet cells. Green arow - normal Red arrow - Adenoma |
|

|
Familial adenematous polyposis, 60 years polyposis, |
|
|
Familial adenematous polyposis |
|
|
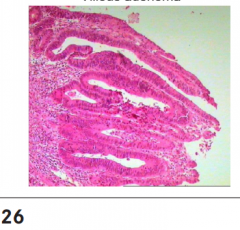
Vilious adenoma, is high risk to be malignant |
|
|
Intraepithelial carcinoma in large bowel, dysplasia, high number of cells. 1.Dysplasia 2. Normal gland cells with normal cells 3. Border between normal and abnormal |
|

|
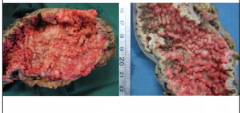
Gross view of colorectal cancer, the dark dots showes the cancer and the progression is intensive. |
|
|
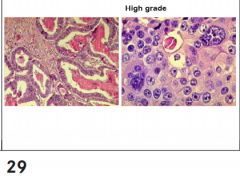
Colorectal adenocarcinoma, 99% Low grade - high differentiated High grade - low differented In the right picture - we see red structure is apoptic body. |
|
|
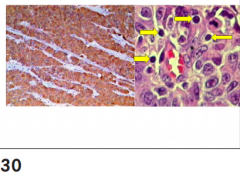
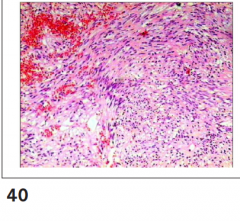
Medullary cancer, lots of inflammatory cells, the brown cells are tumor cells, and tumor assicated cells. |
|
|
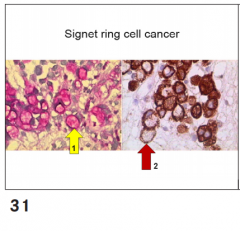
Signet ring cell cancer, typical for gastric cancer |
|
|
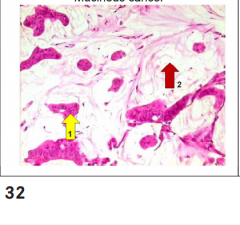
Mucinous cancer, another form of colorectal cancer. T0 No primary tumour Tis Carcinoma in situ: intraepithelial or possessing invasion into lamina propria. T1: invasion into submucosa T2: invasion into lamina muscularis propria |
|
|
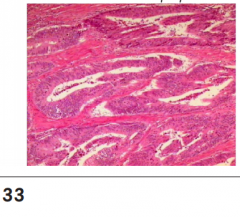
Colorectal adenocarcinoma - invasion in lamina musclaris propria, its T2, because its profliferation into muscle layer |
|
|
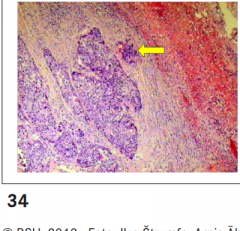
Serosal invasion, tumor cells into the right |
|
|
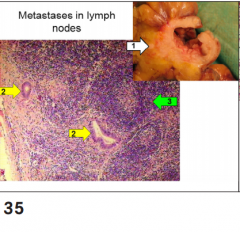
Metastasis in lymph nodes, cancerinoma 1. 2. 3. |
|
|
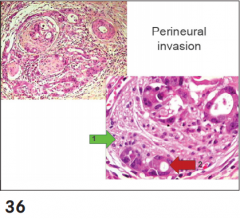
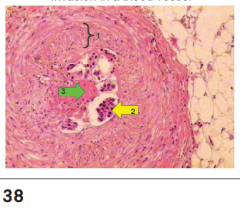
Perineural invasion |
|
|
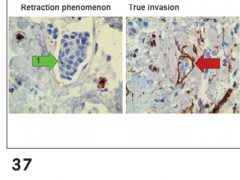
Invasion in lymphatic capillaries, specific stain to determine whether the tumor cells are inside the lymphatic cells. |
|
|
Invasion in blood vessels, thrombosis inside the blood vessel. |
|
|
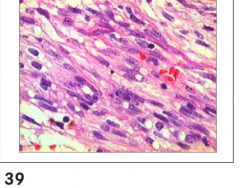
Gastrointestinal stromal tumor(GIST) mesenchymal tumour in the stomach and large bowel arising from Cajal cells and showing c-Kit s. CD117 positivity. Microscopic; Spindle cell (70%)Epitheloid (20%)Mixed |
|
|
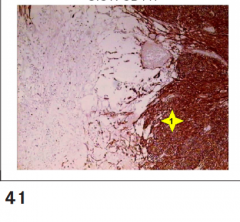
Gastrointestinal stromal tumor(GIST); Rounded mass lesion Cystic change possible Usually softer than leiomyoma White to tan |
|
|
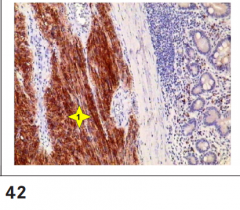
GIST(CD117) |
|
|
GIST(CD117) |
|
|
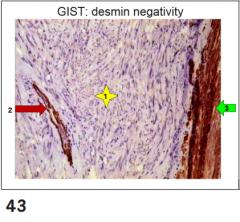
GIST, desmin negative 1. 2. 3. |
|
|
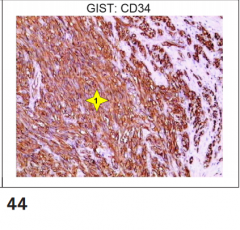
GIST(CD34) 1. |