Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
78 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Liver Lobule
|
portal triad (bile duct, hepatic a., portal v.)
portal vein feeds central vein through limiting plate. Bile flows opposite to blood zone 1 (portal tract, highly oxygentated) zone 2 (intermediate) zone 3 (central vein, poorly oxygenated) |
|
|
|
hepatic endothelial cells
|
line hepatic sinusoids w/ fenestrae
sievelike communication btwen lumen and space of disse |
|
|
|
kupffer cells
|
phagocytes, 1st line of defense against infection and toxic molecules
|
|
|
|
stellate cells
|
beneath endothelial cells in space of disse, storage capacity
|
|
|
|
liver functions
|
Metabolic - glucose homeostasis (gluconeogenesis, glycogenolysis), free fatty acids converted to energy or converted to TG
Synthetic - albumin, clotting factors, complement, binding proteins Storage - glycogen, TG, Fe, Cu, lipid soluble vitamins Catabolic - endogenous and exogenous substances, released ammonia excreted Excretory - bile Regeneration |
|
|
|
Billirubin
|
Arises from the degradation of heme (85% erythrocytes)
Travels in blood bound to albumin (free form is toxic, leads to 'Kernicterus' - irreversible brain injury) Tranfer from blood to bile: 1) uptake - dissociated from Br taken up by hepatocyte 2) binding - bound to glutathione-S-transferase 3) conjugation - in ER, UGT system conjugates to glucuronic acid 4) excretion - diffuses through cytosol to canaliculus (rate-limiting step) Some conjugated Br hydrolyzed by normal flora to urobilinogen, absorbed, and excreted in urine |
|
|

|
Jaundice
|
Overproduction of Br - hemolytic dz (rise in unconjugated Br)
Decreased Br uptake - congenital (Crigler-Najjar, Gilbert, Dubin-Johnson, Rotor), Neonatal Jaundice (physiologic) Impaired Canalicular Bile Flow - Intrahepatic (intrinsic liver dz, intrahepatic cholestasis) extrahepatic (obstruction of large bile ducts) --> incr bile --> pruritus |
|
Liver
|
Dubin-Johnson
|
Benign, AR dz, chronic conjugated hyperBr w/ deposition of melanin-like pigment in liver. linked to MRP2 absence
|
|
|
Crigler-Najjar
|
rare, recessive, unconjugated hyperBr, absence of UGT
|
|
|
|
Gilbert Syndrome
|
mild, chronic unconjugated hyperBr, UGT promoter mutations, 3-7% of pop, more common in males, often symptomless or stress induced
|
|
|
|
Rotor Syndrome
|
familial conjugated hyperBr, similar to Dubin-Johnson w/o liver pigmentation
|
|
|
|
Crigler-Najjar
|
rare, recessive, unconjugated hyperBr, absence of UGT
|
|
|
|
Gilbert Syndrome
|
mild, chronic unconjugated hyperBr, UGT promoter mutations, 3-7% of pop, more common in males, often symptomless or stress induced
|
|
|
|
Rotor Syndrome
|
familial conjugated hyperBr, similar to Dubin-Johnson w/o liver pigmentation
|
|
|
|
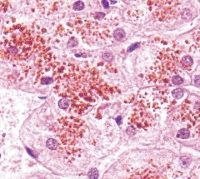
Bile stasis
|
prominent bile plus in dilated bile canalliculi
|
|
|
Cholestasis
|
hepatocytes are swollen and bile stained
necrotic hepatocytes secondary to toxic excess of bile early - contained in central zone chronic - bile plugs in periphery clinical presentation - pruritis, xanthomas, malabsorption |
|
|
|
Cholestasis
|
hepatocytes are swollen and bile stained
|
|
liver
|
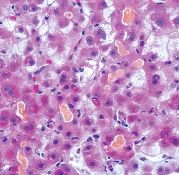
extrahepatic biliary obstruction
|
liver is swollen and bile stained (white bile if prolonged), swollen hepatocytes, diffuse bile pigment, reticulated "feathery" appearance
|
|
|
Bile Infarct (bile lake)
|
extrahepatic biliary obstruction, necrosis and accumulation of extravasated bile. caused by rupture of dilated bile duct
|
|
liver
|
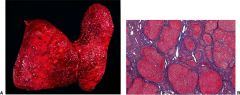
secondary biliary cirrhosis
|
|
|
|
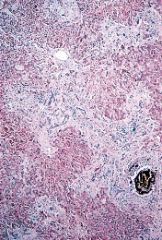
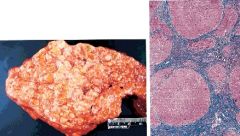
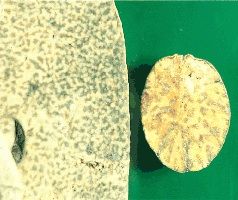
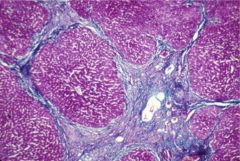
cirrhosis
|
end stage of chronic liver dz, destruction of normal liver architecture by fibrous septa encompassing regenerative nodules
|
|
|
|
micronodular cirrhosis
|
nodules slightly larger than a lobule (<3mm), thin CT, active stages contain mononuclear infiltrate and proliferated bile ducts, typical of alcoholic cirrhosis
|
|
|
liver
|
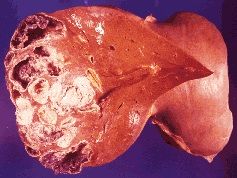
macronodular cirrhosis
|
associated w/ chronic hepatitis, and/or confluent necrosis, broad CT, alcoholic micronodular cirrhosis --> macronodular after EtOH cessation
|
|
|
Hepatic Failure
|
Liver cells unable to sustain vital activities of the liver
most common acute due to viral hepatitis or toxic liver injury viral hep or cirrhosis most common insidious leads to hyperBr (direct & indirect), hepatic encephalopathy, Coag defects |
|
|
|
Hepatic Encephalopathy
|
Stage 1 - sleep disturbances, irritability
Stage 2 - lethargy, disorientation Stage 3 - somnolence Stage 4 - coma Dx: asterixis, extensor toe responses, decerebrate posture pathogenesis: increased toxicity due to shunting around liver, increased Ammonia levels (help Dx, not necessary), GABA accentuation, false NTs, phenols, mercaptans Cerebral edema may be present in acute hepatic failure |
|
|
|
Coagulation defects
|
Thrombocytopenia, DIC, hypoalbuminemia, hepatorenal syndrome (hypoperfusion, reversible)
Secondary endocrine manifestations: gynecomastia, spider angiomas, palmar erythema (estrogen) |
|
|
|
Hepatic Failure
|
Liver cells unable to sustain vital activities of the liver
most common acute due to viral hepatitis or toxic liver injury viral hep or cirrhosis most common insidious leads to hyperBr (direct & indirect), hepatic encephalopathy, Coag defects |
|
|
|
Hepatic Encephalopathy
|
Stage 1 - sleep disturbances, irritability
Stage 2 - lethargy, disorientation Stage 3 - somnolence Stage 4 - coma Dx: asterixis, extensor toe responses, decerebrate posture pathogenesis: increased toxicity due to shunting around liver, increased Ammonia levels (help Dx, not necessary), GABA accentuation, false NTs, phenols, mercaptans Cerebral edema may be present in acute hepatic failure |
|
|
|
Coagulation defects
|
Thrombocytopenia, DIC, hypoalbuminemia, hepatorenal syndrome (hypoperfusion, reversible)
Secondary endocrine manifestations: gynecomastia, spider angiomas, palmar erythema (estrogen) |
|
|
|
Portal HTN
|
sustained increase in portal venous pressure results from obstruction of flow somewhere in portal circuit
Intrahepatic - cirrhosis, schistosomiasis Prehepatic - portal vein thrombosis Posthepatic - Budd-Chiari (thrombosis of hepatic vein), hepatic venoocclusive dz (BC variant, occlusion of central veins and hepatic vein branches) Complications: esophageal and anorectal varices, caput medusae, hypersplenism, Gamna-Gandy bodies (focal hemorrhages w/ fibrotic Fe laden nodules in spleen), ascites |
|
|

|
Budd-Chiari
|
thrombosis of hepatic vein
associated w/: polycythemia vera, hypercoag, malignancies, OC, bacterial infections, paroxysmal nocturnal hemoglobinuria, surgical trauma |
|
liver
|
acute viral hepatitis
|
swollen hepatocytes, lymphocytic infiltrate, apoptotic liver cells, councilman bodies (eosinophilic), lobular disarray
HAV - fecal/oral, daycares/travel/homosexual males, never chronic, lifelong immunity HBV - 10% infected -->carriers, vaccine, causes CD8s to attack hepatocytes, acute/fulminant/chronic, incr risk liver ca. HDV - coinfection or superinfection w/ HBV HCV - T-cell response to infected hepatocytes, chronic dz, incr risk hepatobiliary carcinoma, EtOH worsens course |
|
liver
|
Confluent Hepatic Necrosis
|
severe variant of acute viral hepatitis, death of almost all liver cells. most common in acute HBV
bridging necrosis, submassive necrosis, massive necrosis |
|
liver
|
massive hepatic necrosis s/p acute viral hepatitis
|
nearly all hepatocytes dead
|
|
liver
|
mild chronic hepatisis
|
|
|
liver
|
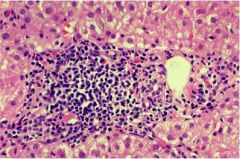
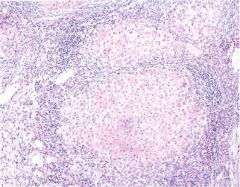
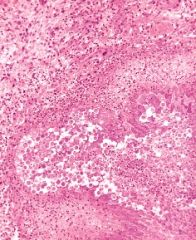
severe chronic hepatitis
|
mononuclear inflammatory infiltrate in expanded portal tract, inflammation penetrating limiting plate surrounding groups of hepatocytes at the border of the portal tract.
|
|
|
Chronic hepatitis w/ cirrhosis
|
|
|
|
|
Chronic hepatitis w/ cirrhosis
|
|
|
liver
|
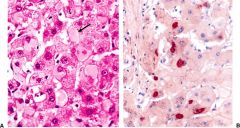
Ground glass hepatocytes
|
HBV, hepatocytes w/ HBsAg in cytoplasm (left), staining for HBsAg (right)
|
|
|
Autoimmune Hepatitis
|
severe chronic hepatitis of unknown cause, circulating Ab & high levels of serum Ig.
Type I - most common, antinuclear & anti-smooth muscle Ab, middle aged women, prolonged asymptomatic course (many present w/ cirrhosis) Type II - children 2-14 y/o, Ab to liver and kidney microsomes histologically resembles chronic viral hepatitis tx: corticosteroids & immunosuppressives, liver transplant |
|
|
liver
|
alcoholic fatty liver
|
EtOH --> fatty liver --> acute alcoholic hepatitis --> cirrhosis
steatosis is reversible (everything is going to be okay) |
|
liver
|
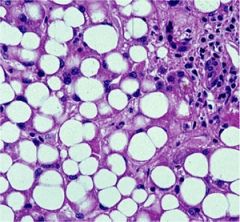
alcoholic hepatitis
|
acute necrotizing lesion, predominantly in central zone, hyaline inclusions within hepatocytes (Mallory bodies), neutrophilic inflammatory response, perivenular fibrosis, collagen around central vein (central hyaline sclerosis)
--> malaise, anorexia, fever, RUQ pain, jaundice, mild leukocytosis STOP DRINKING --> most recover don't --> 70% cirrhosis |
|
liver
|
central hyaline sclerosis
|
collagen deposition around central vein in alcoholic hepatitis
|
|
liver
|
alcoholic cirrhosis
|
15% of alcoholics
hepatocellular necrosis, signs of fatty liver and/or cirrhosis STOP DRINKING NOW!!! |
|
|
Nonalcoholic fatty liver dz
|
similar histology and progression as alcoholic liver dz
linked to obesity, DM2, hyperlipidemia |
|
|
|
Nonalcoholic fatty liver dz
|
similar histology and progression as alcoholic liver dz
linked to obesity, DM2, hyperlipidemia |
|
|
liver
|
Primary Biliary Cirrhosis (inflammatory infiltrate in portal tract w/ bile duct damage)
|
destruction of intrahepatic bile ducts--> cholestasis --> hepatic damage
typically affects middle aged women Dx: anti-mitochondrial Ab correlation w/ other autoimmune dzs Stage I - ductal lesion Stage II - scarring Stage III - cirrhosis |
|
|
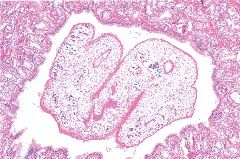
Primary Sclerosing Cholangitis (edematous, fibrotic, and inflamed portal tract. Inflammatory debris is present within the lumen of the bile duct.)
|
Chronic cholestatic liver dz of unknown cause, inflammation/fibrosis narrow and obstructs intra and extrahepatic bile ducts
2/3 of pts have UC Stage I - periductal inflammation/fibrosis Stage II - obliterated bile ducts, fibrous septa in parenchyma Stage III - secondary biliary cirrhosis |
|
liver
|
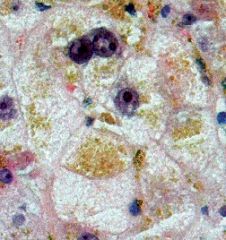
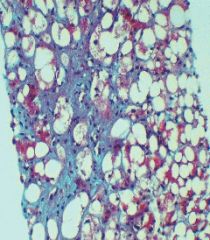
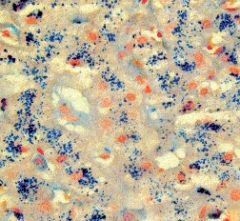
hemochromatosis
|
hereditary - altered gene expression in intestinal iron absorption (no negative feedback), AR
secondary - many causes Symptoms: Liver (micronodular cirrhosis --> macronodular cirrhosis), Pancreas (DM2, acinar degeneration), Heart (CHF), Endocrine (loss of libido, amenorrhea, impotence), Joints (arthropathy) |
|

|
Kayser-Fleischer ring
|
Wilson's Dz
autosomal recessive 1/100 carrier 1/30,000 live birthes failure to excrete ceruloplasmin (can't excrete Cu) Liver (mild to severe chronic hepatitis or cirrhosis) neuro/psych/optho symptoms transient acute hemolytic episodes |
|
|
liver
|
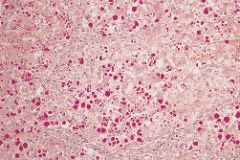
alpha 1 anti-trypsin deficiency (faintly eosinophilic PAS positive droplets)
|
autosomal recessive, retention of misfolded protein, micro-->macronodular cirrhosis, emphysema
30% of all cases neonatal hyperBr incr incidence hepatocellular carcinoma |
|
|
|
Kayser-Fleischer ring
|
Wilson's Dz
autosomal recessive 1/100 carrier 1/30,000 live birthes failure to excrete ceruloplasmin (can't excrete Cu) Liver (mild to severe chronic hepatitis or cirrhosis) neuro/psych/optho symptoms transient acute hemolytic episodes |
|
liver
|
alpha 1 anti-trypsin deficiency (faintly eosinophilic PAS positive droplets)
|
autosomal recessive, retention of misfolded protein, micro-->macronodular cirrhosis, emphysema
30% of all cases neonatal hyperBr incr incidence hepatocellular carcinoma |
|
|
hepatotoxin
|
-always produces liver cell necrosis w/ high enough dose
-extent of hepatic injury is dose dependent -same lesion(s) in different animal species -liver necrosis is zonal (typically centrilobular) -brief interval btwn administration and symptoms |
|
|

liver
|
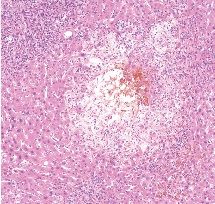
toxic centrilobular necrosis
|
i.e. acetaminophen, CCl4, mushrooms OD, greater activity of drug metabolizing enzymes in central zones --> more necrosis
pts either die of hepatic favor or recover w/o sequelae |
|
liver
|
microvesicular fatty liver
|
i.e. Reye's syndrome
accumulation of TG in hepatocytes. in Reye's also may see hepatic failure, encephalopathy |
|
|
liver
|
microvesicular fatty liver
|
i.e. Reye's syndrome
accumulation of TG in hepatocytes. in Reye's also may see hepatic failure, encephalopathy |
|

|
Budd-Chiari
|
thrombosis of hepatic vein
associated w/: polycythemia vera, hypercoag, malignancies, OC, bacterial infections, paroxysmal nocturnal hemoglobinuria, surgical trauma |
|
liver
|
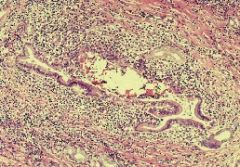
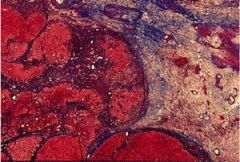
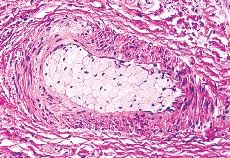
peliosis hepatis
|
peculiar hepatic lesion, characterized by cystic, blood-filled cavities that are not lined by endothelial cells. Anabolic sex steroids, contraceptive steroids, and the antiestrogen compound tamoxifen sometimes produce this lesion
|
|
liver and nut (not the anatomical one)
|
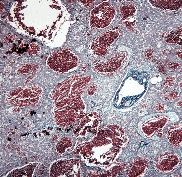
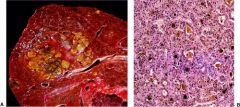
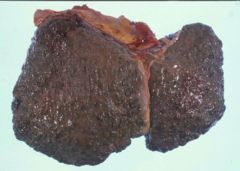
Nutmeg liver
|
chronic passive congestion
s/p R sided heart failure in severe cases may lead to hepatic fibrosis |
|
|
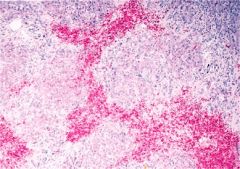
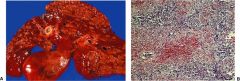
pyogenic liver abscesses
|
staph, strep, gram neg enterics
reach liver via portal blood or biliary tract, arterial blood in septic pt. |
|
|
|
pylephlebitic abscess
|
intraabdominal suppuration transmits organisms
|
|
|
cholangitic abscess
|
biliary obstruction --> ascending cholangitis --> abscess
typically e. coli pt presents w/ fever, rapid weight loss, RUQ pain, hepatomegaly, jaundice (25%), elevated AP tx: drainage if single, multiple difficult tx w/ high mortality |
|
|
liver
|
amebic abscess
(next slide: most common parasites) |
amebiasis, malaria, leishmania, ascariasis, liver flukes (clonorchis sinensis, fasciola hepatica), echinococcosis
|
|
liver
|
clonorchis sinesis
(next slide most common parasites) |
amebiasis, malaria, leishmania, ascariasis, liver flukes (clonorchis sinensis, fasciola hepatica), echinococcosis
|
|
liver
|
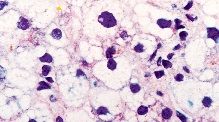
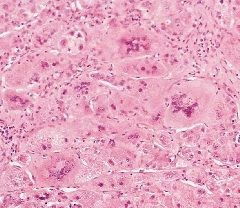
neonatal hepatitis
|
prolonged cholestasis --> liver cell injury and inflammation
causes: 50% unknown 30% alpha1AT deficiency, 20% TORCH, 1% etc (i know 101%, shutup) giant cell transformation |
|
|
biliary atresia
|
lack of a lumen in biliary tree
extrahepatic - causes persistent cholestasis, indication for 1/2 of pediatric liver transplants, hepatitis, chromosomal abnormalities, viral infection intrahepatic - paucity of bile ducts within the liver, neonatal hep, alagille syndrome (AD, congenital dz), idiopathic |
|
|
liver
|
hepatic adenoma
|
OC linkage, decreased w/ new Rx
encapsulated, pale w/ neoplastic hepatocytes w/o lobular architecture tumors may rupture and bleed into peritoneum (incr risk w/ preg) link in men w/ anabolic steroids |
|
liver
|
focal nodular hyperplasia
|
central scar w/ fibrous septa radiate
division by multiple fibrous septa resembles cirrhosis tortuous bile ducts, mononuclear inflammatory cells, absence of lobular architecture |
|
|
liver
|
focal nodular hyperplasia
|
central scar w/ fibrous septa radiate
division by multiple fibrous septa resembles cirrhosis tortuous bile ducts, mononuclear inflammatory cells, absence of lobular architecture |
|
liver
|
hepatocellular carcinoma
|
most common malignant tumor in world, uncommon in western industrialized countries
link w/ chronic HBV and HCV, alcoholic cirrhosis, hemochromatosis, alpha1ATD, Aflatoxin B (fungal contaminant in less developed countries) presents w/ painful enlarging mass in liver, dismal prognosis |
|
liver
|
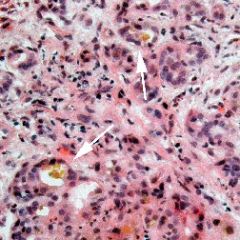
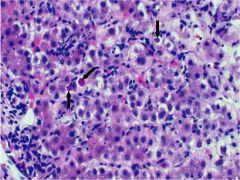
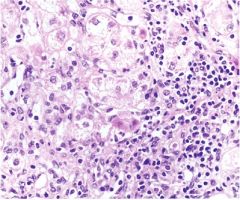
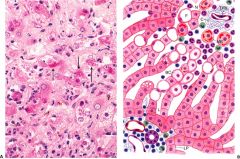
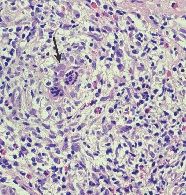
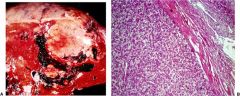
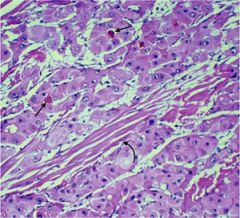
Fibrolamellar HCC
|
uncommon variant of HCC w/ distinctive histology that appears in normal livers of adolescents/young adults
Eosinophilic tumor cells show a lamellar pattern. A fibrous band (curved arrow) traverses the tumor. Bile casts (straight arrows) are seen within neoplastic acini. |
|
liver
|
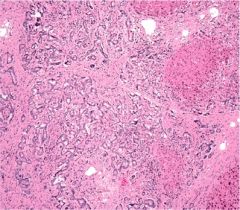
cholangiocarcinoma
|
originates from biliary tree, predominantly in older pts
high incidence in Asia (C. sinensis), link w/ primary sclerosing cholangitis |
|
|
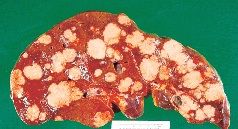
metastatic carcinoma
|
liver involved in 1/3 of matastatic cancers
pt presents w/ weight loss, splenomegaly, ascites, portal HTN, jaundice, hepatic failure tx: surgical resection |
|
liver
|
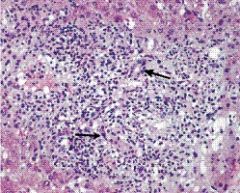
acute rejection
|
distortion of bile ducts by portal inflammatory infiltrate, atypism of bile duct epithelial cells, inflammation of the ductal epithelium
|
|
liver
|
chronic rejection
|
more than 2 months, damage to interlobular ducts, progresses to small bile ducts and persistent cholestasis "vanishing bile duct syndrome"
|
|
liver
|
cirrhosis
|
|
|
|
cirrhosis
|
|