Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
278 Cards in this Set
- Front
- Back
|
Spondylolysis
|
i. Defect in pars interarticularis of vertebral arch
ii. Usually L5 |
|
|
Spondylosis
|
i. Degenerative osteoarthritis btw center of spinal certebrae and neural foraminae
ii. Compresses nerve roots |
|
|
Spondylolisthesis
|
i. A → P displacement of vertebra
|
|
|
i. What do you do for acute muscle spasm?
|
Muscle energy reciprocal inhibition and counterstrain
|
|
|
patient with pain radiating down leg
- what level is it |
L4 nerve root
|
|
|
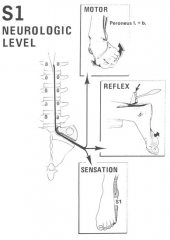
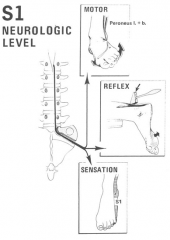
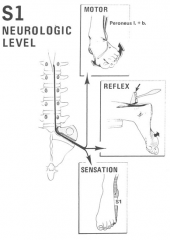
Weakness of plantar flexion of the foot
- what level is it |
S1 Nerve Root
|
|
|
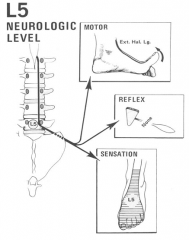
why is it very important to check the big toe (extensor hallicus longus) ?
- what level? - comse out btw |
L5 nerve root
L5 has no reflex comes out btwn L4 and L5 |
|
|
Sensory loss lateral & plantar plantar aspect of the foot/ankle
- what level? |
S1 Nerve Root
|
|
|
• Difficulty walking on toes
- what spinal level? |
S1 nerve root
|
|
|
diminished patellar reflex (asymmetric)
- what spinal level? |
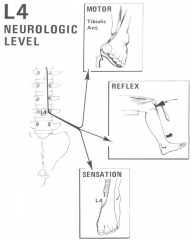
L4 nerve root
|
|
|
difficulty walking on heels
- what spinal level? |
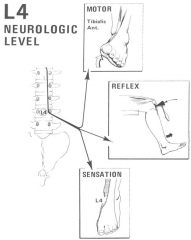
L4 nerve root
|
|
|
sensory loss medial aspect of the lower leg/foot/ankle
- what spinal level? |
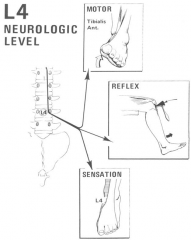
L4 nerve root
|
|
|
weakness of great tow dorsiflexion
- what spinal level? |
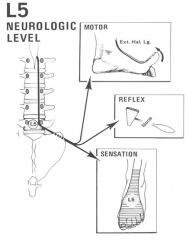
L5 nerve root
|
|
|
sensory loss to lateral leg and dorsum of foot
- what spinal level? |
dorsum = top
L5 nerve root |
|
|
difficult walking on toes
- what spinal level? |
S1 nerve root
|
|
|
diminished achilles reflex (asymmetric)
- what spinal level? |
S1 nerve root
|
|
|
sensory loss lateral & plantar aspect of foot/ankle
- what spinal level? |
S1 nerve root
|
|
|
• Lumbar Strain- Injury to the ?
|
strain = muscle / tendon / fascia
|
|
|
• Lumbar Sprain- Injury to the ?
|
sprain = ligaments / capsule
|
|
|
strain
sprain |
strain = muscle / tendon
sprain = ligament / capsule |
|
|
3 ways pain happens from nociceptor activation
|
broken fibers ->
K leaks into interstitial fluid blood leaves damaged vessels -> bradykinin leaves plasma proteins -> prostaglandins released neuropeptides leave nerve ending (substance P)-> pain |
|
|
kinetic chain
- what? |
combo several successively arranged joints making a complex motor unit
|
|
|
open and closed kinetic chain
|
open kinetic chain
- terminal joint is free (hand waiving) closed kinetic chain - terminal joint meets fixation (push ups / pull ups) |
|
|
what innervates latissimus dorsi? (nerve & root)
|
6, 7, 8 CN
thoracodorsal (long scapular) nerve |
|
|
Rhomboid of Michaelis
- what/why care - 5 muscles involved |
- diamond where 80% of back pain resides
- latissimus dorsi - quadratus lumborum - multifidus - gluteus maximus |
|
|
quadratus llumborum
- major function anatomically and in life function |
- pulls hip up
- balances postural distortion |
|
|
what muscle:
- pain in C6-8 - shoulder and back pain - innervated by thoracodorsal nerve |
latissimus dorsi
|
|
|
innervation of trapezius
|
cranial nerve XI (accessory)
|
|
|
diagnose:
- unremitting back pain - assoc w/ urinary tract, bowel symptoms - weakness requires urgent referral! |
cauda equina
surgical emergency |
|
|
aplasia
|
failure to form
|
|
|
hypoplasia
|
small
|
|
|
dysplasia
|
abnormal growth
|
|
|
hypertrophy
|
overgrowth
|
|
|
supernumerary parts
|
extra vertebra / fingers
|
|
|
arrested development
|
spina bifida
|
|
|
spina bifida most commonly occurs?
|
L5/S1
|
|
|
Spina Bifida
- what |
incomplete closure of embryonic neural tube
|
|
|
Spina Bifida Occulta
- what - % of population that has |
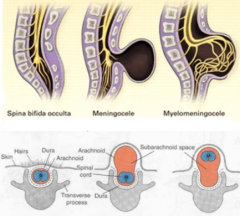
incomplete neural tube closure
- no meninges herniation - 8-10% pop has |
|
|
Spina Bifida Meningocele
|
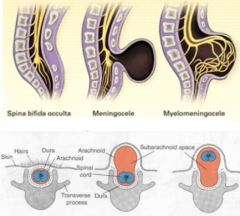
- herniation of meninges through the defect
|
|
|
Spina Bifida Meningomyelocele
|
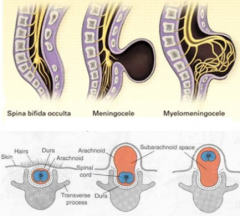
- herniation of meninges AND nerve roots through defect
|
|

what is this probably
|
spina bifida occulta
|
|
|
Stress defect or fracture, or anomalous development of the pars interarticularis (L4-5)
|
Spondylolysis
|
|
|
Spondylolysis
|
Stress defect or fracture, or anomalous development of the pars interarticularis (L4-5)
|
|
|
what type of spondylolisthesis:
- elongation of the pars interarticularis - pars remains intact - anterior displacement of L5 severe |
dysplastic (congenital) spondylolisthesis
|
|
what is this?
|
isthmic spondylolisthesis (spondylolytic spondylolisthesis)
a fracture then slip (usually 6-16yo |
|
|
degenerative spondylolisthesis
- from what generally? - what happens |
chronic instability from many things
- hypertrophy - degen of facet joints - discs and facets wear away and start to slip forward |
|
|
what is radicular pain
|
pain that radiates along dermatome of a nerve due to inflammation
|
|

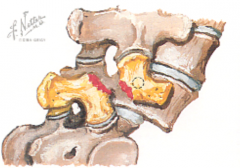
what is this called?
what is that |
- scottie dog
- lysis defect in the pars on the left of picture |
|
|
innominate is made of what 3 fused bones
|
ilium
ischium pubis |
|
|
2 joints of the innominate
|
sacroliliac joint
pubis symphysis |
|
|
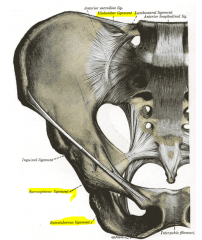
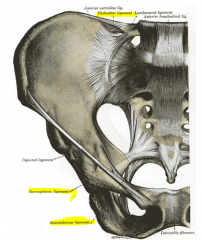
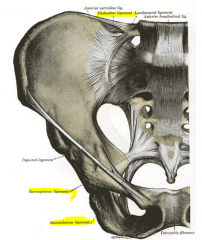
sacrotuberous ligament
- attachments |
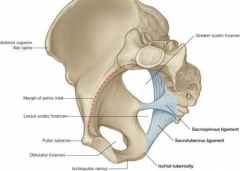
- sacrum - up to sciatic notch
- ischial tuberosity |
|
|
sacrospinous ligament
- where attach |
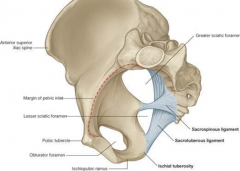
- ischial spine
- sacrum divides sciatic foramen to greater and lesser |
|
|
iliolumbar ligament
- where attach |
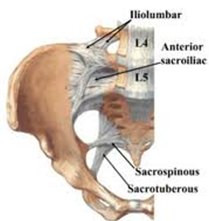
- ant iliac crest
- TPs of L4-5 |
|
|
3 primary pelvic diaphragm muscles = levator ani group
|
- pubococcygeus
- puborectalis - illiococcygeus |
|
|
cephalad
|
Superior
|
|
|
caudad
|
inferior
|
|
|
A positive seated FFT, after a positive standing FFT, suggests the _______ is the primary problem = _______dysfunction
|
A positive seated FFT, after a positive standing FFT, suggests the sacrum is the primary problem = sacroiliac dysfunction
|
|
|
A negative seated FFT, after a positive standing FFT, suggests an _________ problem = ____________dysfunction
|
A negative seated FFT, after a positive standing FFT, suggests an innominate problem = iliosacral dysfunction
|
|
|
what is radicular pain or a radiculopathy
|
pain down dermatome that is caused by inflammation / irritation at the root
|
|
|
what is a Chapman's point
|
Tissue change due to visceral (organ) change
|
|
|
what part of GI has bacteria? which doesnt
|
large has bacteria - sigmoid colon
small intestine is sterile |
|
|
how is breathing involved in GI
|
increases intrabdominal pressure - helps venous / lymphatic return
|
|
|
Stimulation of sympathetic fibers ________ (inhibit / stim) cholinergic activity of parasympathetics, slowing peristalsis and motility
|
Stimulation of sympathetic fibers inhibit cholinergic activity of parasympathetics, slowing peristalsis and motility
|
|
|
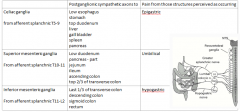
Celiac ganglia
- from afferent __________ (root nerve/segments) - postganglionc sympathetic axons to (7x) - pain from those structures perceived as occuring? |

|
|
|
superior ganglia
- from afferent __________ (root nerve/segments) - postganglionc sympathetic axons to (67x) - pain from those structures perceived as occuring? |

|
|
|
inferior ganglia
- from afferent __________ (root nerve/segments) - postganglionc sympathetic axons to (4x) - pain from those structures perceived as occuring? |
|
|
|
Stimulation of the parasympathetic fibers ___________ gut peristalsis and activities
|
Stimulation of the parasympathetic fibers increases gut peristalsis and activities
|
|
|
the main upper GI parasympathetic nerve is:
__________ nerve transmits fibers via celiac and superior mesenteric ganglia to foregut and midgut (entire upper GI tract) |
the main upper GI parasympathetic nerve is:
Vagus nerve transmits fibers via celiac and superior mesenteric ganglia to foregut and midgut (entire upper GI tract) |
|
|
Parasympathetic of GI – _________ nerve
|
Parasympathetic of GI – Vagus nerve
|
|
|
Sympathetic
Thoracic esophagus _____ Abdominal _______ |
Sympathetic
Thoracic esophagus T3-6 Abdominal T5-8 |
|
|
______ oil is a smooth muscle relaxant- great for IBS, get enteric coated to avoid acid reflux
|
Mint oil is a smooth muscle relaxant- great for IBS, get enteric coated to avoid acid reflux
|
|
|
OMM Tx for GERD
a. Viscerosomatic- Sympathetic _____ Especially _____ side b. Parasympathetic- _______ c. Mechanical- __________ |
OMM Tx for GERD
a. Viscerosomatic- Sympathetic T3-6, Especially right side b. Parasympathetic- Vagus - Occiput/C1/C2 c. Mechanical- Diaphragm/LES |
|
|
hicups
Phrenic nerve supplies the diaphragm - and phrenic is from what root levels |
C3,4,5
|
|
|
singultus technique
|
inhibitory pressure between sternal and clavicular heads of the sternocleidomastoid muscles
|
|
|
1. A 23 year old male medical student presents to your office complaining of new onset burning epigastric pain that has become progressively worse over the past four days. He notes temporary improvement with eating but overall is getting worse. He notes some nausea but not vomiting, hematochezia or melena. He drinks alcohol rarely and does not smoke. No significant past medical history. He takes ibuprofen OTC 400 mg tid for the past week for tension headaches associated with staying up late studying for an exam that he took yesterday.
2. Exam reveals epigastric tenderness but not rebound, rigidity or guarding. The rest of his exam is unremarkable except for findings of somatic dysfunction that include: a. T5F, Rr, Sr, T7N, Rl, Sr, Tenderness over the posterior angle of the left 7th rib, Restricted left hemidiaphragm 3. What is the most likely cause of this patient’s symptoms? what nerve structure is most likely involved? what other somatic dysfunction in this patient? a. C2- b. T2 c. T12 d. S2 e. S4 |
Duodenal ulcer- epigastric burning (upper GI), nonsteroidal use
- celiac ganglia - C2 - vagus nerve activity - other choices NOT INVOLVED IN STOMACH INNERVATION a. C2- vagus nerve activity b. T2- not specific for peptic ulcer disease, think T5-9 c. T12- too low for ulcers, think T5-9 d. S2- involved in large intestine, not stomach e. S4- involved in large intestine, not stomach |
|
|
1. A 23 year old male medical student presents to your office complaining of new onset burning epigastric pain that has become progressively worse over the past four days. He notes temporary improvement with eating but overall is getting worse. He notes some nausea but not vomiting, hematochezia or melena. He drinks alcohol rarely and does not smoke. No significant past medical history. He takes ibuprofen OTC 400 mg tid for the past week for tension headaches associated with staying up late studying for an exam that he took yesterday.
2. Exam reveals epigastric tenderness but not rebound, rigidity or guarding. The rest of his exam is unremarkable except for findings of somatic dysfunction that include: a. T5F, Rr, Sr, T7N, Rl, Sr, Tenderness over the posterior angle of the left 7th rib, Restricted left hemidiaphragm 3. What is the most likely cause of this patient’s symptoms? what nerve structure is most likely involved? what other somatic dysfunction in this patient? a. C2- b. T2 c. T12 d. S2 e. S4 |
Duodenal ulcer- epigastric burning (upper GI), nonsteroidal use
- celiac ganglia - C2 - vagus nerve activity - other choices NOT INVOLVED IN STOMACH INNERVATION a. C2- vagus nerve activity b. T2- not specific for peptic ulcer disease, think T5-9 c. T12- too low for ulcers, think T5-9 d. S2- involved in large intestine, not stomach e. S4- involved in large intestine, not stomach |
|
|
4 causes for PUD
|
- H pylori
- NSAIDS - smoking - drugs (bisphosphates) |
|
|
“___________” classically seen as:
C2 left, T3-6 right, T5-10 left, T6-8 right |
“UGI Pattern” classically seen as:
C2 left, T3-6 right, T5-10 left, T6-8 right |
|
|
Gastric Viscerosomatics
1. ________ (spine levels), especially left sided (sympathetic) 2. _______ (spine levels) (parasympathetic) |
Gastric Viscerosomatics
1. T5-10, especially left sided (sympathetic) 2. C1 and C2 (parasympathetic) |
|
|
1. 42 y/o female in good health, except for being 25 pounds overweight, presents with RUQ pain over the past week that is deep, aching with intermittent bouts of sever, sharp pain. The past two days her pain has worsened and now radiates to her right mid thoracic area. Today, she notes some right shoulder pain. Her pain is worsened by eating, especially after a meal of fried chicken last night. She notes nausea but denies diarrhea, melena or hematochezia.
2. Exam is unremarkable except for tenderness in the RUX with no rebound, rigidity or guarding, and also findings of somatic dysfunction that include T9RrSl with warm boggy changes over right transverse process as well as C2RrSr. 3. What is your presumptive diagnosis? a. Acute pancreatitis- b. Acute appendicitis- c. Acute diverticulitis- d. Acute cholecystitis e. Irritable bowel syndrome- typically spastic without clear presentation of radiation 4. What nerve structures are involved with her T9 viscerosomatic dysfunction? a. Superior mesenteric ganglia b. Inferior mesenteric ganglia c. Celiac ganglia d. Vagus nerve e. Pelvic splanchnic nerves 5. Which structure is involved in the spread of this patient’s pain to her right mid thoracic area? a. Vagus nerve b. Phrenic nerve c. Peripheral diaphragm d. Parietal pleura e. Central diaphragm 6. Which structure is involved in their shoulder pain? a. Vagus nerve b. Phrenic nerve c. Lateral diaphragm d. Parietal pleura e. Somatoemotional manifestation |
1. 42 y/o female in good health, except for being 25 pounds overweight, presents with RUQ pain over the past week that is deep, aching with intermittent bouts of sever, sharp pain. The past two days her pain has worsened and now radiates to her right mid thoracic area. Today, she notes some right shoulder pain. Her pain is worsened by eating, especially after a meal of fried chicken last night. She notes nausea but denies diarrhea, melena or hematochezia.
2. Exam is unremarkable except for tenderness in the RUX with no rebound, rigidity or guarding, and also findings of somatic dysfunction that include T9RrSl with warm boggy changes over right transverse process as well as C2RrSr. 3. What is your presumptive diagnosis? a. Acute pancreatitis- more epigastric, deep, boring, continuous, intolerance to eating, patient presented with RUQ pain b. Acute appendicitis- typically RLQ c. Acute diverticulitis- usually in LLQ around colon *D Acute cholecystitis e. Irritable bowel syndrome- typically spastic without clear presentation of radiation 4. What nerve structures are involved with her T9 viscerosomatic dysfunction? a. Superior mesenteric ganglia b. Inferior mesenteric ganglia *c. Celiac ganglia- innervates T5-9 d. Vagus nerve e. Pelvic splanchnic nerves 5. Which structure is involved in the spread of this patient’s pain to her right mid thoracic area? a. Vagus nerve b. Phrenic nerve *c. Peripheral diaphragm- as well as parietal peritoneum d. Parietal pleura e. Central diaphragm 6. Which structure is involved in their shoulder pain? a. Vagus nerve- doesn’t cause shoulder pain, does cause occiput pain *b. Phrenic nerve- C3-5 c. Lateral diaphragm d. Parietal pleura e. Somatoemotional manifestation |
|
|
1. Acute inflammation of the gall bladder
2. Often due to stones in cystic duct or common bile duct 3. Backup of bile into gallbladder causing inflammation of walls (thickening) and dilated duct 4. RUQ abdominal pain 5. Often radiating to back 6. Nausea, sometimes vomiting- usually don’t present with vomiting, progresses 7. Intolerance to fatty foods- fatty foods trigger ejection of bile what? |
Acute Cholecystitis
|
|
|
- severe RUQ pain - from inflammation in ant abdominal wall or peripheral diaphragm
- right shoulder pain - referred by common root w/phrenic nerve (C3,4,5) what disease causes this type of referred pain |
cholecystitis
(inflammation of the gallbladder) |
|
|
Viscerosomatic Reflexes for Gall Bladder Disease
1. Sympathetic viscerosomatic reflex findings at ________ (spinal level) on the right, transmitted via the _______ ganglia |
Viscerosomatic Reflexes for Gall Bladder Disease
1. Sympathetic viscerosomatic reflex findings at T5-T10 on the right, transmitted via the celiac ganglia |
|
|
2. Most common 10-30 y/o
3. Obstruction leads to distension, ischemia and bacterial overgrowth and eventually perforation and peritonitis (can cause infertility, adhesions, chronic pain, can be life threatening) 4. Presentation a. Vague periumbilical pain usually starts epigastrically, then migrates to RLQ in 4-8 hours i. Initially collateral ganglia, then more somatic involvement allowing localization b. Pain before vomiting i. Typically with infection vomit first and irritation from vomiting causes pain c. Nausea, anorexia, vomiting d. Retrocecal and pelvic appendix presentations will differ e. RLQ tenderness, fever, tachycardia |
Appendicitis
|
|
|
viscerosomatic findings of appendicitis
- vagus _______ sympathetic_____________ T9-12 right anterior Chapmans = tip of the right ______ rib |
a. Vagus – Occiput, C1, C2
b. Sympathetic T9-T12 right side c. Anterior Chapman’s = tip of right 12th rib |
|
|
Post-operative Ileus - somatic dysfunctions
a. Vagus associated upper __________ b. __________ stomach and small intestine viscerosomatic reflexes d. __________ /__________ dysfunctions |
Post-operative Ileus - somatic dysfunctions
a. Vagus associated upper cervical (C2) b. T5-11 stomach and small intestine viscerosomatic reflexes d. Lower rib/diaphragm dysfunctions |
|
|
a. Diarrhea, constipation or the alternation of both
b. Most common 20’s. Much less common by 50 y/o c. Cramping abdominal pain- Aggravated by eating, Relieved by defecation d. No hematochezia or melena |
Irritable Bowel Syndrome
1. IBS not IBD |
|
|
4. Viscerosomatic findings for what?
a. Large intestinal involvement- T11-L3 i. Different GI bacteria compositions have been associated with DM and CAD b. Small intestinal involvement (bacterial overgrowth?)- T8-10 c. Vagus – upper cervical d. Pelvic splanchnics – sacral findings |
Irritable Bowel Syndrome
1. IBS not IBD |
|
|
2 types of IBD (inflammatory bowel disease)
|
- Crohn's disease
- Ulcerative colitis |
|
|
Upper GI Reflexes
1. Esophagus- ______, often right sided 2. Stomach- ______, often left sided 3. Duodenum- ______, often right sided 4. Pancreas- ______, b/l, especially extended 5. Liver- ______, right sided 6. Gall bladder-______, right sided. Some sources state T7-9 right. |
Upper GI Reflexes
1. Esophagus- T3-6, often right sided 2. Stomach- T5-10, often left sided 3. Duodenum- T6-8, often right sided 4. Pancreas- T5-9, b/l, especially extended 5. Liver- T5-10, right sided 6. Gall bladder- T5-10, right sided. Some sources state T7-9 right. |
|
|
Upper GI Reflexes
1. ______- T3-6, often right sided 2. ______- T5-10, often left sided 3. ______- T6-8, often right sided 4. ______- T5-9, b/l, especially extended 5. ______- T5-10, right sided 6. ______- T5-10, right sided. Some sources state T7-9 right. |
Upper GI Reflexes
1. Esophagus- T3-6, often right sided 2. Stomach- T5-10, often left sided 3. Duodenum- T6-8, often right sided 4. Pancreas- T5-9, b/l, especially extended 5. Liver- T5-10, right sided 6. Gall bladder- T5-10, right sided. Some sources state T7-9 right. |
|
|
Lower GI Reflexes
1. Small Intestine- ______, b/l (R>L) 2. Appendix - ______ Right side, Chapman’s point = tip of right ______ rib 3. Ascending and transverse colon- ______ (Right for ascending, b/l for transverse) 4. Descending colon- ______ Left side |
Lower GI Reflexes
1. Small Intestine- T8-10, b/l (R>L) 2. Appendix - T9-T12 Right side, Chapman’s point = tip of right 12th rib 3. Ascending and transverse colon- T11-L1 (Right for ascending, b/l for transverse) 4. Descending colon- L1-L3 Left side |
|
|
Anterior Chapman’s Points
1. ______ - B/w ribs 2 & 3 2. ______ - B/w ribs 5 & 6 and 6 & 7 3. ______and ______- B/w ribs 6 & 7 4. ______ - Iliotibial band |
Anterior Chapman’s Points
1. Esophagus- B/w ribs 2 & 3 2. Stomach- B/w ribs 5 & 6 and 6 & 7 3. Liver and gall bladder- B/w ribs 6 & 7 4. Colon- Iliotibial band |
|
|
Posterior Chapman’s Points
1. ______- Dorsal T2 b/w spinous and transverse processes 2. ______- Between T5-6 and /T6-7, b/w spinous and transverse processes 3. ______and ______ - T 5-6, T6-7 – same as stomach 4. ______- L2-4, Transverse processes to iliac crest |
Posterior Chapman’s Points
1. Esophagus- Dorsal T2 b/w spinous and transverse processes 2. Stomach- Between T5-6 and /T6-7, b/w spinous and transverse processes 3. Liver and gall bladder- T 5-6, T6-7 – same as stomach 4. Colon- L2-4, Transverse processes to iliac crest |
|
|
GI Viscerosomatic Reflexes
1. ______- T3-6, often right sided 2. ______- T5-10, often left sided 3. ______- T6-8, often right sided 4. ______- T5-9, b/l, especially extended 5. ______- T5-10, right sided 6. ______- T5-10, right sided. Some sources state T7-9 right. 7. ______ - T8-10, b/l (R>L) 8. ______- T9-T12 Right side, Anterior Chapman’s = tip of right______rib 9. ____________- T11-L1 (Right for ascending, b/l for transverse) 10. ______- L1-L3 Left side |
GI Viscerosomatic Reflexes
1. Esophagus- T3-6, often right sided 2. Stomach- T5-10, often left sided 3. Duodenum- T6-8, often right sided 4. Pancreas- T5-9, b/l, especially extended 5. Liver- T5-10, right sided 6. Gall bladder- T5-10, right sided. Some sources state T7-9 right. 7. Small Intestine- T8-10, b/l (R>L) 8. Appendix- T9-T12 Right side, Anterior Chapman’s = tip of right 12th rib 9. Ascending and transverse colon- T11-L1 (Right for ascending, b/l for transverse) 10. Descending colon- L1-L3 Left side |
|
|
OMT Tx for GER and PUD (3x)
|
- t-spine & rib eval
- rib raising - suboccipital release |
|
|
IBD OMT Tx (4x)
|
- t-spine & rib eval
- rib raising - suboccipital release - sacral |
|
|
5 general steps to OMM Dx
|
1 - Hx
2 - Structural exam - symmetry 3 - Regional range of motion 4 - layer by layer - static inspection (derm / therm) - dynamic palpation (skin / fascia / tissue) 5 - intersegmental motion testing |
|
|
what is the best innominate segmental motion test?
|
SI joint motion test
|
|
|
3x anterior static innominate landmarks
|
ASIS
umbilicus to ASIS distance medial malleolus |
|
|
3x posteriorstatic innominate landmarks
|
PSIS
ischial tuberosity sacrotuberous ligament |
|
|
SI joint key level (segment)
|
S2
|
|
|
2 attachment points of piriformis
and function |
- anterior sacrum
- femur externally rotate femur |
|
|
3 transverse sacral axis
|
- superior (respiratory & craniosacral motion)
- middle (postural motion) - inferior (innominate rotation) |
|
|
when placed in sphinx - the sacrum flexes or extends? how does this compare to lumbar?
|
sphinx
- sacrum flexes - lumbar extends |
|
|
+ standing flexion
+ seated flexion = ? |
sacral dysfunction
|
|
|
+ standing flexion
+ seated flexion + lumbosacral spring test = ? |
probably posterior torsion - which is non physiologic
|
|
|
+ standing flexion
+ seated flexion - lumbosacral spring test landmarks become more symmetric in sphinx = ? |
physiologic dysfunction - like anterior torsion
|
|
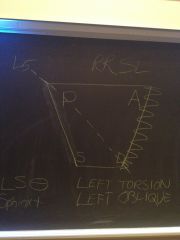
Dx?
|
left on left anterior torsion
|
|
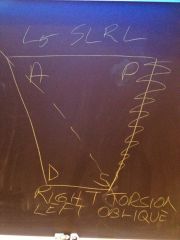
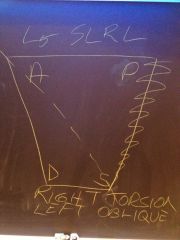
Dx?
|
right on right anterior torsion
|
|

Dx?
|
left on right posterior torsion
|
|
Dx?
|
right on left posterior torsion
|
|
|
right on left posterior torsion
- sacral suli - ILAs - standing and seated flexion tests - SI joint motion test - L5 |
right on left posterior torsion
- sacral suli (right is posterior) - ILAs (left is deep) - standing and seated flexion tests (both +) - SI joint motion test (right is restricted) - L5 SLRL |
|
|
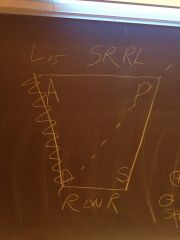
left on right posterior torsion
- sacral suli - ILAs - standing and seated flexion tests - SI joint motion test - L5 |

left on right posterior torsion
- sacral suli (left is posterior) - ILAs (right is deep) - standing and seated flexion tests (both +) - SI joint motion test (left side is restricted) - L5 SRRR |
|
|
oblique axis same/opposite side of SI jt restriction in sacral torsion?
|
opposite side
|
|
|
L5 rotation is same/opposite sacral direction in torsion
|
opposite
|
|
|
for torsions - L5 side bends toward or away from the oblique axis?
|
toward
|
|
|
sacral torsions - choose same or opposite side for each part of L5 dysfunction
- rotation - sidebending |
sacral torsions - choose same or opposite side for each part of L5 dysfunction
- rotation = OPPOSITE - sidebending = SAME SIDE as oblique axis |
|
|
describe unilateral flexion
- sacral suli - ILAs - standing and seated flexion tests - SI joint motion test - L5 |

- sacral suli (side of dysfunc deep)
- ILAs (side of dysfunc shallow) - standing and seated flexion tests (both +) - SI joint motion test (+ side of dysfunc) - L5 ? |
|
|
what is the difference and what is the same between
- left on left anterior - left on right posterior |
same = same landmark locations
diff = LoL (right sided dysfunc) = LoR (left sided dysfunc) but the location of the landmarks ON the axis is a bit ambiquous |
|
|
sphinx test
- sacral sulci right deep then becomes even side of dysfunc? |
right sided dysfunction
right stuck anteriorly |
|
|
sphinx test
- sacral sulci right deep then becomes WORSE side of dysfunc? |
left sided dysfunction
left stuck back |
|
|
Sacrospinous - from the _________ to the_________
|
Sacrospinous - from the sacrum to the ischial spine
|
|
|
Sacrotuberous - from the _________ to the_________
|
Sacrotuberous - from the sacrum to the ischial tuberosity
|
|
|
Illiolumbar - from the _________ to the_________
|
Illiolumbar - from the ileum to the lumbar spine
|
|
|
3x dysfunctions at pubic symphysis?
- each pysiologic or non physiologic? |
all are NON pysiologic
- sheared - gapped - compressed |
|
|
what is an amphiarthrodial joint?
|
moves slightly
|
|
|
acetabulum is fusion of what 3 bones
|
- ilium
- ischium - pubis |
|
|
iliolumbar ligaments attachments
|
between spinous processes of L4 and L5 and to the inner lip of the iliac crest
|
|
|
what is the false pelvis
|
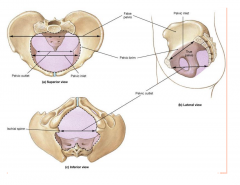
top part
|
|
|
which ligament is responsible for aiding in stabilizing the anterior motion of L5 on the pelvis?
|
iliolumbar ligament
|
|
|
female acetabula face which way? male?
|
female - anterior
male - lateral |
|
|
4 types of female pelvises (birthing) - describe each
- gynecoid - android - anthropoid - platyelloid |
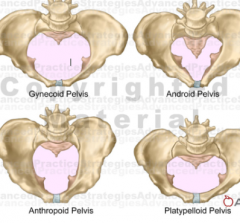
- gynecoid (classic - ideal for birthing)
- android (male - difficult) - anthropoid (ape - certain fetal positions problematic) - platyelloid (head engages later - fine after engages) |
|
|
4 types of female pelvises (birthing)
|
- gynecoid (classic - ideal for birthing)
- android (male - difficult) - anthropoid (ape - certain fetal positions problematic) - platyelloid (head engages later - fine after engages) |
|
|
The lesser pelvis is bounded primarily by bony structures ? (T/F)
|
true
|
|
|
Which of the Following is true about the differences in the male and female pelvis?
a. The female pelvis has a heart shaped inlet b. The male pelvis has a larger sacral base c. The female pelvis has larger ischial spines d. The male pelvis has lateral facing acetabula e. The female pelvis has higher iliac crests |
The male pelvis has lateral facing acetabula
|
|
|
4 types of posture and about each
|
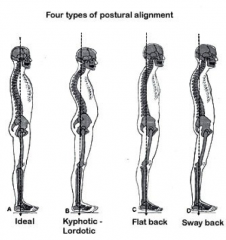
- ideal - pelvis level - ASIS + pubic symph in same vert plane
- kyphotic lordotic (ant head carrier / inc curves) - flat back / forward sway (tight hamstrings pull pelvis posterior) - sway back (gravity line posterior) |
|
|
what do these muscles do?
- iliospoas - rectus femoris - sartorius - TFL - pectineus - adductor longus and brevis - gracilis |
hip flexors
|
|
|
what do these muscles do?
- gluteus maximus - biceps femoris (long head) - semimembranosus - semitendinosus |
hip extensors
|
|
|
what do these muscles do?
- piriformis - gemellus superior and inferior - obturator int and ext - quadratus femoris - iliopsoas - sartorius |
external rotators
|
|
|
what do these muscles do?
- gluteus medius and minimus - semitendinosus - semimembranosus - TFL - gracilis |
internal rotators
|
|
|
what do these muscles do?
- adductor magnus - longus - brevis - minimus - pectineus - gracilis - obturator externus |
adductors
|
|
|
what do these muscles do?
- gluteus medius and minimus - TFL - portions of gluteus maximus |
abductors
|
|
|
Which of the following is not a hip flexor?
a. Sartorius b. Rectus femoris c. Illiacus d. Quadratus femoris e. Psoas |
Quadratus femoris
|
|
|
3 muscles of levator ani
|
- pubococcygeus
- puborectalis - iliococcygeus |
|
|
2 muscles of pelvic diaphragm
|
- levator ani (3 actual muscles - pubococcygeus / puborectalis / iliococcygeus)
- coccygeus |
|
|
Genu recurvatum
what? |
a deformity in the knee joint, so that the knee bends backwards. In this deformity, excessive extension occurs in the tibiofemoral joint. Genu recurvatum is also called knee hyperextension and back knee.
|
|
|
what muscle squeezes the vagina / urethra / rectum shut
|
levator ani
- iliococcygeus - pubococcygeus - puborectalis |
|
|
what is the urogenital hiatus?
what makes it up? |
the holes in the levator ani muscles (3 of them) through which vagina/urethra/rectum pass
- prolapse can happen too |
|
|
muscle strength deteriorates by ___% each decade after 30?
|
5%
|
|
|
what nerve innervates external genitalia / sphincters of bladder / rectum
|
pudendal nerve
|
|
|
what sex nerve can bike seats damage
|
pudendal nerve
|
|
|
Which of the following types of pelvis shapes has the most difficulty with labor and delivery
a. Gynecoid b. Android c. Anthropod d. Platypelloid e. Rhomboid |
android - male shaped
|
|
|
most common type of incontinence in women
- this is involuntary leakage with increased abdominal pressure |
stress urinary incontinence
|
|
|
Childbirth can result in pelvic floor dysfunction via damage to which of the following nerves?
a. Sciatic b. Pudendal c. Obturator d. Femoral e. Ilioinguinal |
pudendal
|
|
|
where is gluteus maximus main trigger point
|
over the ischial tuberosity
|
|
|
sympathetic root for (2 levels)
kidneys, gonads, upper ureter, adrenals |
T10-T11
|
|
|
sympathetic root for (3 levels)
- lower ureters, uterus, vagina, clitoris, vas deferens, bladder, urethra, fallopian tubes, seminal vesicles, sphincter, trigone |
T12-L2
|
|
|
which controls ejaculation (sym or parasym)
|
sym - shoot
|
|
|
pelvic parasympathetics
- root level and nerve? - ventral or dorsal rami? |
S2-4
- splanchnic nerves - ventral rami (sensory) |
|
|
what nerve controls parasympathetics for:
kidneys, upper ureters, ovaries, and testes |
vagus
|
|
|
Function is to control micturition, erection, and defecation (sym or parasympathetic?)
|
parasympathetic
|
|
|
Point, pee, poop (sym or parasympathetic?)
|
parasympathetic
|
|
|
c. Shoot, seal off (sym or parasympathetic?)
|
sympathetic
|
|
|
Which of the following muscles is not part of the levator ani?
a. Iliococcygeus b. Coccygeus c. Puborectalis d. Pubococcygeus |
Coccygeus
|
|
|
2 OMT techniques to help balance ANS
|
- OA release
- rib raising |
|
|
A 30 year old female with interstitial cystitis presents in follow up. On exam you find that she has a right anterior innominate, a left on left sacral torsion, L5 RRSL, a superior pubic shear, and a taut right iliolumbar ligament. Which of these somatic dysfunctions should be treated first?
a. Innominate b. Sacrum c. L5 d. Pubis e. Iliolumbar ligament |
Pubis
|
|
|
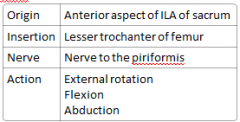
piriformis muscle
- origin - insertion - nerve - action |
|
|
|
L5 moves with/away from S1
|
away (opposite)
|
|
|
anterior torsion - what ME technique is utilized in piriformis in:
- top leg - bottom leg |
top = RI
bottom = PIR |
|
|
posterior torsion - what ME technique is utilized in piriformis in:
- top leg - bottom leg |
top = PIR
bottom - not used |
|
|
sacrum flex/extend on inhalation
|
extends
|
|
|
sacrum flex/extend on exhalation
|
flexes
|
|
|
unilateral flexion - you will resist inhalation or exhalation?
- this is resisting sacral flexion/extension? - hand on top/bottom of sacrum? |
for unilateral flexion
- resist exhalation (flexion) - hand on bottom |
|
|
unilateral extension - you will resist inhalation or exhalation?
- this is resisting sacral flexion/extension? - hand on top/bottom of sacrum? |
for unilateral extension
- resist inhalation (extension) - hand on top |
|
|
if the 2 sacral landmarks are the same on a given side (anterior/deep or posterior/shallow) then it is a torsion or unilateral whatever?
|
torsion
|
|
|
if the 2 sacral landmarks are different on a given side (anterior/shallow or posterior/deep) then it is a torsion or unilateral whatever?
|
unilateral flexion or extension
|
|
|
anterior torsions are generally type 1 or 2
|
anterior torsion = type 1
rotate opposite (always) SB toward axis (always) |
|
|
posterior torsions are generally type 1 or 2
|
posterior torsion = type 2
rotate opposite (always) SB toward axis (always) |
|
|
for sacral torsion Tx - pt lies on side of rotation or axis
|
axis
|
|
|
position for posterior torsion
|
reverse modified sims
- hips lat recum - chest opens up - ready for a hug from the world |
|
|
anterior torsion position
|
mod sims - hug the table - to de-rotate L5
|
|
|
sphinx flexs/extends the sacrum
|
flexes
|
|
|
If you have the patient prone and the left sacral sulcus was deep but this evens out in the sphinx position. What is L5?
|
L5 N RLSR
reasoning: L sacral sulcus is deep - this means it is either a LL anterior torsion, RonL posterior torsion, or unilateral flex or extended. it is however - ONLY anterior torsions that get better when going into sphinx ***?check - so do unilateral flexions??? |
|
|
Seated flexion test positive on the right. Right sacral sulcus is deep, left ILA is posterior. How man legs will hang off edge of table during treatment?
|
right sided R SS deep means either
- LonL ant torsion - unilateral flexion shallow left ILA - means MUST be LonL anterior torsion so L5 - RR (since opposite sacrum which is left) - SL (to side of axis) - making L5 SLRR or type 1 - neutral anterior torsions are treated with both legs off the table |
|
|
Seated flexion test positive on Left and left sacral sulcus is shallow and the left ILA is deeper than right ILA. What is the diagnosis?
|
left sided
L SS is posterior - posterior torsion - unilateral extension L ILA deep - must be left unilateral extension |
|
|
on unilateral flexion/extension - opposite sacral corners are same/opposite
|
SAME
|
|
|
Patient is lying with left leg off table ON their right side. What dysfunction is the doctor treating?
what is the top leg doing (PIR/RI)? |
1 leg off the table = posterior torsion
on right side = right sided axis - right sided axis means sacrum is facing left must be left on right posterior torsion top leg is doing PIR / muscle moves the bone - top leg piriformis is pulling into external rotation |
|
|
L5 is rotated left and flexed. How many legs are going to be off the table during treatment?
|
L5 RL and flexed
- means its type 2 - which means that SB is same direction as rotation = left - so L5 is F SLRL sacrum - opposite L5 rotation - so facing right - SB is same as axis - so left axis - so right on left axis - which is a posterior torsion Tx of a RonL posterior torsion - has 1 leg off the table using PIR |
|
|
in OMM - what Tx first
|
area of greatest restriction - start with non-pysiologic dysfunctions
|
|
|
Zink patterns - common compensatory patterns
OA? |
N SRRL
|
|
|
Zink patterns - common compensatory patterns
C2-6 |
F/E SRRR
|
|
|
Zink patterns - common compensatory patterns
T1-5 |
N SRRR
|
|
|
Zink patterns - common compensatory patterns
T1-12 |
N SRRL
|
|
|
Zink patterns - common compensatory patterns
L1-5 |
N SLRR
|
|
|
Zink patterns - common compensatory patterns
left innominate |
Lon R posterior torsion
|
|
|
golf low back - most likely what muscle
|
psoas
|
|
|
what is the "3rd principle of spine mechanics"
|
3 motions into spinal segment = physiological locking
as use thumb to flex, then sidebend, then rotate - grade end feel glide as 1,2,3 |
|
|
pain is where
greatest restriction / or where the body is trying to compensate |
where the body is trying to compensate NOT the area of greatest restriction
|
|
|
order of pelvic Tx
|
innominates - all non physiologic
- innominate shears - pubic shears - innominate rotations sacrum - non pyhsiologic 1st (posterior - LonR / RonL) |
|
|
red flag for a possible visceral etiology of low back pain for kids (<18yo)
|
pain > 6wks
|
|
|
red flag for a possible visceral etiology of low back pain for old ppl (> 50yo)
5x |
- trauma
- cancer - corticosteroids - drug abuse - HIV - difficulty urinating - fecal incontinence |
|
|
viscerosomatic reflex
peptic ulcer - where back pain |
interscapular radiation from T5-10
|
|
|
what sympathetic ganglia do the great / small splanchnic go through to innervate
esophagus stomach liver pancreas adrenal SI transverse colon |
celiac ganglia
|
|
|
epigastric pain could be sympathetic pain from what organs 5x
|
stomach
duodenum liver gallbladder spleen pancreas |
|
|
umbilical pain could be sympathetic related pain through the superior mesenteric ganglia from what organs 6x
|
duodenum
pancreas jejunum ileum ascending colon proximal 2/3 transeverse |
|
|
main nerve that is parasympathetic supply to gut
|
vagus nerve
|
|
|
GI viscerosomatic reflex
- T3-6 - right sided |
esophagus
|
|
|
GI viscerosomatic reflex
-T5-10, left sided |
stomach
|
|
|
GI viscerosomatic reflex
-T6-8, right |
duodenum
|
|
|
GI viscerosomatic reflex
-T5-9, b/l especially extended |
pancreas
|
|
|
GI viscerosomatic reflex
-T5-10 right |
liver
|
|
|
GI viscerosomatic reflex
- T9-10, right sided - or T7-9 |
gall bladder
|
|
|
GI viscerosomatic reflex
- T8-10 b/l R>L |
small intestine
|
|
|
GI viscerosomatic reflex
- T9-12 right - anterior chapmans = tip of right 12th rib |
appendix
|
|
|
GI viscerosomatic reflex
-T11-L1 |
right = ascending
b/l for transverse |
|
|
GI viscerosomatic reflex
- L1-3 left |
descending colon
|
|
|
how much does the kidney move w/respiration
|
4mm
|
|
|
A 41 year old female presents to your office with complaint of bilateral flank pain that has flared over the past 24 hours. She notes some dysuria and feeling warm. She denies abdominal pain, nausea or vomiting.
Vital signs: T 99.1, BP 110/70, HR 108, RR 14 Exam is significant for tenderness and warm boggy tissue texture changes over T9-11 bilaterally. She has no abdominal tenderness, rebound or guarding. What is the most likely diagnosis? a. Pancreatitis b. Gastritis c. Ureterolithiasis d. Pyelonephritis e. Endometriosis |
The correct answer is D. Pyelonephritis. One reason it is not gastritis is because she didn’t have any abdominal pain. Also, the tissue texture changes should give you a clue. (stomach is more T5-9)
|
|
|
A 34 year old male presents to the emergency room complaining of left flank pain over the past 8 hours that is severe, left sided and unrelenting. It has moved a little lower into the left lumbar area and slightly laterally. PMH is unremarkable. He denies fever, chills or dyuria. Physical exam, including vital signs, is normal except for som mild tenderness at thoracolumbar junction, left paraspinal musculature with acute tissue texture changes at left L1-L3. There is no abdominal rebound, rigidity or guarding.
What is th most likely diagnosis? A. Acute pyelonephritis B. Acute cholecystitis C. Acute cystitis (bladder infection) D. Acute appendicitis E. Acute uretoerolithiasis |
E. Acute ureterolithiasis
|
|
|
Over the next 2 hours the patient’s pain migrates inferiorly and wraps around to the laft inguinal area, radiating into the left testicle. Urinalysis shows significant microhematuria with few white cells, nitrite negative and leukocte esterase negative. Where is the most likely location of this patient’s lithiasis?
A. Kidney B. Proximal ureter C. Ureterovesicular junction D. Urethra E. Common bile duct |
C. Ureterovesicular junction. This is where the ureter enters the bladder.
|
|
|
the tollbooth for ureterolithiasis
|
UVJ - ureterovesicular junction
|
|
|
this is innervation for what?
Sympathetic reflex T10-L2 Parasympathetic reflex S2-S4 |
prostate
|
|
|
A 72 year old male with past medical history of hypertension and smoking presents to your emergency room complaining of severe pain at the thoracolumbar junction that started one hour ago and has since radiated down to the midline lumbar spinal area. He describes the pain as severe, agonizing, some of the worst pain of his life. What diagnosis must be considered immediately?
A. Meningitis B. Discitis C. Spinal stenosis D. Dissecting aortic aneurysm E. Cauda equina syndrome |
D. Dissecting aortic aneurysm. Cauda equina syndrome is possible but it typically invovles more bowel and bladder.
|
|
|
this is innervation for what?
Sympatheitc T1-T5 Sensort afferent Travel w/sympathetics - enabling viscerosomatic reflexes Parasympathetic - vagus |
aorta
|
|
|
Urogenital viscerosomatic reflexes
a. Urinary Tract - Sympathetically mediated i. __________ T9-L1 ipsilateral ii. __________ T11-L3 ipsilateral iii. __________ T11-L3 iv. __________ T11-L2 |
a. Urinary Tract - Sympathetically mediated
i. Kidney T9-L1 ipsilateral ii. Ureter T11-L3 ipsilateral iii. Bladder T11-L3 iv. Urethra T11-L2 |
|
|
Urogenital viscerosomatic reflexes
Urinary Tract -Parasympathetic i. __________ – occiput, C1, C2 ii. __________ – occ, C1, C2 iii. __________ – S2-S4 iv. __________ , __________ – S2-S4 |
b. Urinary Tract -Parasympathetic
i. Kidney – occiput, C1, C2 ii. Proximal ureter – occ, C1, C2 iii. Distal ureter – S2-S4 iv. Bladder, urethra – S2-S4 |
|
|
Urogenital viscerosomatic reflexes
__________ i. Sympathetic reflex T10/11 – L2 ii. Parasympathetic reflex S2-S4 |
c. __________
i. Sympathetic reflex T10/11 – L2 ii. Parasympathetic reflex S2-S4 |
|
|
Urogenital viscerosomatic reflexes
__________ i. T10-11 ipsilaterally |
d. Ovaries (and testes)
i. T10-11 ipsilaterally |
|
|
Urogenital viscerosomatic reflexes
__________ i. T9-L2 bilaterally ii. S2-S4 |
e. Uterus
i. T9-L2 bilaterally ii. S2-S4 |
|
|
GU chapmans point
adrenal |
periumbilical, T11
|
|
|
GU chapmans point
kidney |
periumbilical, T12
|
|
|
GU chapmans point
gonads |
pubic bone, T9-10
|
|
|
GU chapmans point
bladder |
periumibilical, L1
|
|
|
kidney sympathetic root
|
OA-C2
|
|
|
Lyod's punch test
test for |
kidney irritation
|
|
|
term described by this:
Spinal segment that is stimulated by afferents from a visceral or somatic source |
facilitated segment
|
|
|
define facilitated segment
|
Spinal segment that is stimulated by afferents from a visceral or somatic source
|
|
|
GU lymphatics drain into
|
left thoracic duct
|
|
|
uterus - symmpathetic
- do? - too much = ? |
- uterine contraction / vasocontriction
- too much -> inefective contractions |
|
|
uterus - parasympathetic
- do? - too much = ? |
- uterine relaxation / vasodilation
- too much tone -> congestion / poor sloughing |
|
|
KUB (kidney / ureter / bladder)
- parasympathetic - sympathetic |
para - T10-11 - vagus
sym - T12-L2 / S2-4 |
|
|
SLOWS DOWN AND STORES
|
Urinary sympathetic effects
|
|
|
MAKES URINE - SPEEDS UP AND EXPELS
|
Urinary parasympathetic effects
|
|
|
Common cause of mental status change in elderly
|
UTI
|
|
|
what OMT Dx/Tx can be done (2x) for nocturnal enuresis and urinary frequency?
|
pubic superior/inferior shear
- uses PIR |
|
|
#1 cause male recurrent UTI
|
Chronic prostatitis
|
|
|
3x OMM Tx for UTI
|
- thoracolumbar junction
- redome diaphragm - immune pump |
|
|
3x OMM Tx for ureterolithiasis
|
- thoacolumbar inhibition - sacral rock combo
- counterstrain psoas - OA-C2 indirect |
|
|
G2 P1001 means what
|
G - 2 pregnancies
P - outcome 1 - total deliveries 0 - premies 0 - abortions 1 - living children |
|
|
G1 2002
|
G - 1 pregnancy
P - outcome 2 - total deliveries 0 - premies 0 - abortions 2 - living children |
|
|
7x contraindications to OMT for pregnancy
|
- pre-eclampsia / eclampsia
- PROM (Premature rupture of membranes) - preterm labor - abruptio placenta - actopic pregnancy - undiagnosed vaginal bleeding - threatened orincomplete abortion - prolapsed cord |
|
|
pregnancy OMT protocol name, stand for, who made
|
PROMOTE
pregnancy research in osteopathic manipulation optimizing treatment effects Kendi Hensel, DO, PhD |
|
|
PROMOTE
- T-spine what do |
articulate
|
|
|
PROMOTE
- cervical |
MFR (myofascial release)
|
|
|
PROMOTE
- what do top half of body 7x - work your way down head to waist |
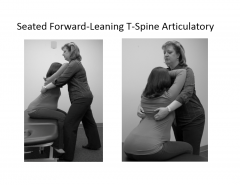
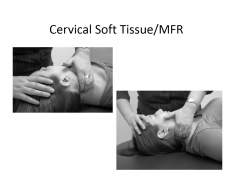
- articulate Tspine (seated)
- cervical soft tissue / MFR (supine) - OA release - thoracic inlet MFR - scapulothoracic MFR (lat recumbent) - lumbosacral soft tissue (lat recumbent) - diaphragm MFR (supine) |
|
|
PROMOTE
- what do top half of body 7x - work your way down head to waist |
- articulate Tspine (seated)
- cervical soft tissue / MFR (supine) - OA release - thoracic inlet MFR - scapulothoracic MFR (lat recumbent) - lumbosacral soft tissue (lat recumbent) - diaphragm MFR (supine) |
|
|
PROMOTE protocol for prego
- bottom half - 5x Tx |

-pelvic diaphragm MFR
- SI articulation - frogleg sacral articulation - innominate rotation - pubic decompression |
|
|
back pain in PM&R is chronic after how much time
|
12wks
|
|
|
2nd most common reason for PCP visits?
|
low back pain
|
|
|
5x Sx red flags that you should NOT start OMT or exercise to Tx low back pain?
|
- gait ataxia (uncoordinated)
- upper motor neuron signs (Babinski sign / Hoffman sign (flick distal phalanx of middle finger and see thumb adduct) / hyperreflexia) - night pain / wt loss - fever / chills - cool lower limbs (vasc insufficiency) |
|
|
Red flags for low back OMT - what is each/what Sx looking for?
- cervical stenosis - osteomyelitis - bone mets - vascular claudication - compression fracture - Cauda equina syndrome - lumbar spinal stenosis |
- cervical stenosis (gait ataxia-stumble)
- osteomyelitis (fever / chills) - bone mets (from prostate cancer - osteoblastic lesions) - vascular claudication (pain / diminished peripheral pulses) - compression fracture (spinal tenderness / pain on flexion) - Cauda equina syndrome (saddle paresthesias (groin numbness / incontinence /leg weakness) - lumbar spinal stenosis (pain relief w/flexion) |
|
|
motor testing - 0 - 5 score - what each is
|
0 - paralysis
1 - no motion/ not full ROM 2 - FULL ROM 3 - FULL ROM - gravity 4 - FULL ROM - gravity + some resistance - FULL ROM - gravity + FULL resistance |
|
|
muscles to test for each lumbar section
L1-3 L2-4 L4-5 L5 S1 |
L1-3 - hip flexors
L2-4 - quadriceps L4-5 - tibialis anterior L5 - extensor halluces longus S1 - gastrocnemius / soleus |
|
|
nerve root (level) for patellar tendon
|
L4
|
|
|
nerve root (level) for medial hamstring reflex
|
L5
|
|
|
nerve root (level) for Achilles tendon
|
S1
|
|
|
nerve root (level) for knee jerk
|
L3/4
|
|
|
bowstring test
- what? - + in 71% of pts with? |
i. After positive SLR, slightly flex the knee and apply pressure to the tibial nerve in the popliteal fossa.
1. Popliteal space compression was noted to be anatomically correlated with stretch of the sciatic nerve, and reproduced leg pain. lumbar disc herniation |
|
|
slump test - test for
|
disc herniation
- seated - bow back |
|
|
femoral nerve stretch test - tests for?
|
high lumbar disc herniation
|
|
|
Waddell signs - tests for?
|
physical findings without anatomic cause - psychological
|
|
|
what is Janda’s crossed syndrome?
|
some muscles are tight - some are weak
ex - levator scap / pectoralis tight - weak deep neck flexors/ rhomboids / trapezius |
|
|
Most effective Tx for improving pain and function in chronic LBP
|
stretching and strengthening
|
|
|
what is Sherrington’s law
|
Sherrington’s law of reciprocal inhibition states that a hypertonic antagonist muscle may be reflexively inhibiting their agonist
|
|
|
if you apply Sherringtons law to tight hamstrings what might you be concerned about
|
weak quads
if hams are tight - antagonistically inhibit quads |
|
|
what is the KEY to strengthening muscles?
|
stabilization - co-contraction
|
|
|
side plank strengthens this hard to strengthen core muscle?
|
transverus abdominis
|