Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
281 Cards in this Set
- Front
- Back
|
very, very basic, describe how blood flows
|
right atrium> right ventricle > lungs > left atrium > left ventricle > body > right atrium
|
|
|
What does cardiovascular system consist of
|
heart
blood vessels blood |
|
|
central wall
|
septum
|
|
|
artery where blood is pumped out of the left ventricle
|
aorta
|
|
|
why is blood lost in the cardiovascular system
|
because of resistance due to the walls of the blood vessels
|
|
|
Why does blood flow?
|
liquids and gases flow down pressure gradients
|
|
|
what is the pressure gradient like as one moves from the heart?
the cross sectional area? the velocity of blood flow? |
csarea: max at cappilaries...min at aorta and venea cava
velocity: max at aorta and vena cava |
|
|
hydrostatic pressure
|
the pressure a fluid (normally not moving) exerts on its container
|
|
|
name 2 things that are derivatives of coelomic cavities
|
-kidneys
-reproductive organs -pleural cavities -cardiac sack |
|
|
what is an alternate to diffusion
|
stirring
|
|
|
what does the cardio system have the highest priority in delivering blood too?
|
brain
heart kidney |
|
|
What part of the body has the most amount of blood?
|
veins
|
|
|
how is a fish's heart?
|
-2 chamber
-heart, gills, and systemic organs are in the same loop **second loop arose when fish came to land and had dual oxygen exchange between lungs and gills at the same time |
|
|
flow rate
|
volume of blood that passes a given point in the system per unit time
|
|
|
velocity of flow
|
distance fixed volume of blood travels in a given period of time
|
|
|
What acts as a pressure reservoir during the heart's relaxation phase?
|
arteries
|
|
|
MAP
|
mean arterial pressure
primary driving force of blood flow MAP=CO*PR CO=volume of blood the heart pumps per minute PR=resistance of the blood vessels to blood flow through them. |
|
|
velocity of flow equation
|
v=flow rate/AREA crosssec
|
|
|
connection in series vs, connection in parallel
|
series...
D(change in)P(total) = DP1 + DP2 + DP3 R(total) = R1 + R2 + R3 F1 = F2 = F3 DPn ~ Rn Parallel... 1/R(total) = 1/R1 + 1/R2 + 1/R3 DP(total) = DP1 = DP2 = DP3 F(total) = F1 + F2 + F3 Fn ~ 1/Rn |
|
|
how is a fish's heart?
|
-2 chamber
-heart, gills, and systemic organs are in the same loop **second loop arose when fish came to land and had dual oxygen exchange between lungs and gills at the same time |
|
|
flow rate
|
volume of blood that passes a given point in the system per unit time
|
|
|
velocity of flow
|
distance fixed volume of blood travels in a given period of time
|
|
|
What acts as a pressure reservoir during the heart's relaxation phase?
|
arteries
|
|
|
MAP
|
mean arterial pressure
primary driving force of blood flow MAP=CO*PR CO=volume of blood the heart pumps per minute PR=resistance of the blood vessels to blood flow through them. |
|
|
velocity of flow equation
|
v=flow rate/AREA crosssec
|
|
|
connection in series vs, connection in parallel
|
series...
DP(total) = DP1 + DP2 + DP3 R(total) = R1 + R2 + R3 F1 = F2 = F3 DPn ~ Rn Parallel... 1/R(total) = 1/R1 + 1/R2 + 1/R3 DP(total) = DP1 = DP2 = DP3 F(total) = F1 + F2 + F3 Fn ~ 1/Rn |
|
|
laminar flow
|

a
|
|
|
turbulent flow
|
a
|
|
|
what does pouiseuille's law work for?
|
only for laminar flow
flow=pressure/resistance R = 8Ln/pir4 R ~ Ln/r4 L=length n=viscosity r=radius |
|
|
tough membranous sac encasing heart
|
pericardium
|
|
|
pericardium
|
tough membranous sac encasing heart
|
|
|
peri
|
around
|
|
|
kardia
|
heart
|
|
|
myo
|
muscle
|
|
|
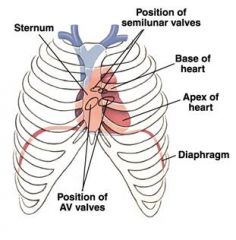
how does the apex of the heart point?
|
to the left side ofthe body, while the broaer base lies just behind the breastbone or sternum
|
|
|
what lubricates the heart?
|
a thin layer of clear pericardial fluid inside the pericardium
|
|
|
pulmonary trunk
|
directs blood to the lungs
|
|
|
where is the thyroid gland?
|
right below adams apple
rostral to trachea superior to heart |
|
|
coronary arteries
|
branch very early on aorta and supply blood to the heart
|
|
|
coronary veins
|
after blood is supplied to the heart, they return the deoxygenated blood to via the vena cava
|
|
|
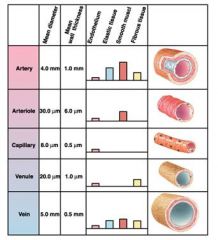
chart of different vessels with the following
diameter wall thickness endothelium elastic tissue smooth muscle fibrous tissue |
aa
|
|
|
draw the heart in the rib cage
|
aa
|
|
|
what does color of blood indicate?
|
red: well oxygenated blood
blue: not very good oxygenated blood |
|
|
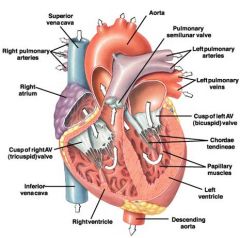
picture of heart open
|
aa
|
|
|
what prevents blood on one side of heart from mixing with blood on the other side of the heart?
|
interventricular septum
|
|
|
how must ventricles contract and why
|
they must contract bottom up because the aorta and pulmonary trunk are both at the top of the heart...this contracting makes sure blood is squeezed out of the heart
|
|
|
where does left atrium receive blood from?
|
pulmonary veins
|
|
|
what encases heart?
|
a membranous fluid-filled sac called the pericardium
|
|
|
what happens to valves during ventricular contraction?
|
right AV or tricuspid valve: closed
mitral, left AV, or bicuspid valve: closed aortic semilunar valve: open pulmonary semilunar valve: open |
|
|
what happens to valves during relaxation
|
left and right AV valve open
semilunar valves closed |
|
|
main purpose of valves?
|
prevent the backflow of blood
ensure that blood flows in only one direction |
|
|
talk about valves
|
-four fibrous connective tissue rings surround the four heart valves
-form the origin and insertion for cardiac muscle -acts as electrical insulator - |
|
|
right side of heart has what A-V valves?
|
tricuspid
mn...RST |
|
|
left side of the heart has what valves
|
bicuspid
or mitral valve |
|
|
how do valves work?
|
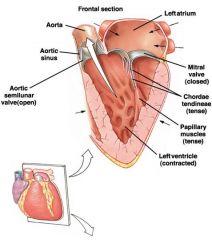
AV:
-have chordae tendineae on the inside of the ventrical that holds the valve to the papillary muscle that branches from the wall of the ventricle -valves move passively when flowing blood pushes on them -when ventricle contracts, blood pushes on ventricular side and causes valve to close...chordae holds the valve from going into the atrium semilunar valves: -seperate ventricles from major arteries -have 3 cuplike leaflets that snap sloces when blood attempting to flow back into the ventricles fills them -due not need connective tendons because of their shape |
|
|
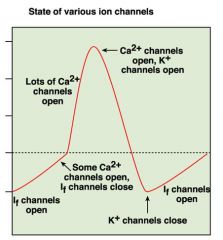
why are funny channels called funny channels?
|
because they allow both potassium and sodium in and researchers were unsure as to how they worked.
-sodium enters more rapidly because it has a higher driving force when the cell is at -60mv -these channels cause the pacemaker potential and when the Vm reaches -40mv an AP is fired - |
|
|
what is heart rate determined by?
|
the rate at which the pacemaker cells depolarize
-increased potassium P or decreased Ca P slows down heart pace |
|
|
How does NE speed up the heart rate?
|
it binds to B1 adrenergic receptors and causes cAMP to bind to If channels and make them remain open longer...thus they are open at the same time as Ca2+ channels are open
|
|
|
2 types of cardiac cells?
|
-autorhythmic
-contractile |
|
|
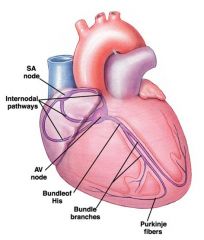
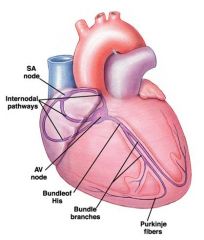
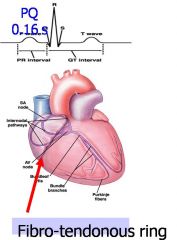
SA node
|
autorhythmic cells in the top of the right atrium that serve as the main pacemaker of the heart
|
|
|
AV node
|
autorhythmic cells near the floor of the right atrium
|
|
|
draw the picture of how the heart pacemaker works
|
autorhythmic cells fire slower as you move down the chain...pacemaker is set by the fastest firing cells:normally the SA node
|
|
|
what insulates atria from the ventricles?
|
Fibro-tendonous ring
|
|
|
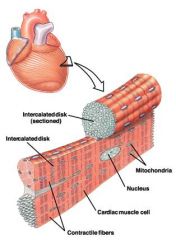
describe cardiac cells
|
-branched
-single nucleus -attached to each other by junctions called intercalated disks: have gap junctions |
|
|
what aids in ejection of blood from ventricle?
|
the spiral arrangement of muscles in the walls
|
|
|
mnemonic to remember nodes?
|
nodes SAAV the heart
|
|
|
second function of the AV node?
|
delays transmission of AP slightly allowing the atria to complete their contraction before ventricular contractino begins
-AP's move at only 1/20 the speed of AP's in the atrial internodal pathway. |
|
|
what cells set the pace of the heart
|
SA node
-other autorhythmic cells can act as pacemakers but their rhythm is slower than that of the SA node so they normally have no chance to set the heartbeat the fastest autorhythmic cells will set the pace if the SA node fails, the AV node will set the pace |
|
|
how are electrodes attached in an ECG
|
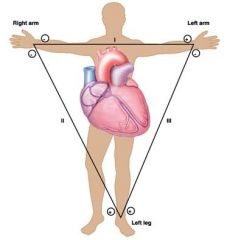
Einthoven's triangle
-right arm all negative -left leg all positive -left arm positive and negative - a normal ECG uses a 12-lead...3 limbs + 9 on the chest and trunk |
|
|
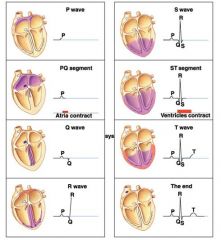
what is P wave?
|
depolarization of the atria
|
|
|
QRS complex
|
progressive wave of ventricular depolarization
|
|
|
T wave
|
represents the repolarization of the ventricles
|
|
|
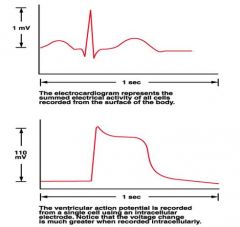
how do the mechanical events of the cardiac cycle relate to the electrical signals?
|
they lag slightly behind
|
|
|
can you tell if an ecg represents repolarization or depolarization?
|
no
|
|
|
what does the ecg represent
|
extracellular recording that represents the sum of multiple action potentials taking place in many heart muscle cells
|
|
|
faster than normal heart rate
|
tachycardia
|
|
|
slower than normal heart rate
|
bradycardia
|
|
|
how do you measure heart rate
|
go from one peak on ECG to next peak.....R to R
|
|
|
how do the lines occur during an ecg
|
when the electrical wave moving through the heart is directed toward the positive electrode, the wave points up
-negative electrode will point down |
|
|
where does atrial repolarization occur?
|
the qrs wave
|
|
|
name some things an ecg can tell u
|
heart rate
rhythm analyze the waves |
|
|
how can blood going through capillaries avoid some of them?
|
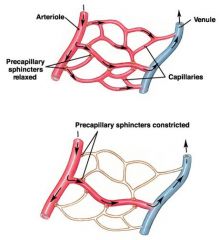
sphincters contracting and blood traveling through metarterioles
|
|
|
is blood an ideal fluid?
|
no
|
|
|
law of laplace
|
T=pr/2 for a sphere
T=pr for a cylinder T is tension p is pressure difference |
|
|
what assists passive filling of the heart
|
7-12 mmHg positive pressure that is always present in the circulation system irrespective of the pumping....systemic filling pressure
|
|
|
left ventricular pressure vs. left ventricular volume diagram
|

a
|
|
|
wigger's diagram
|
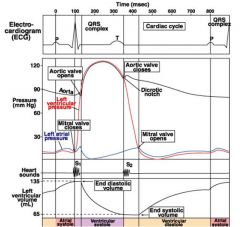
a
|
|
|
explain coronary circulation
|
Both, the left and the right coronary arteries branch from the aorta right above the semilunar valve
They provide blood to the epicardial (outer) layer of myocardium. The coronary arteries are interconnected with the inner network of smaller arteries named Subendocardial plexus. Endocardium receives part of its oxygen from the blood inside the heart Venous blood is discharged via cardiac veins into both left and right atria Blood flow in the coronary circulation is in counterphase relative to the systemic loop: it slows down during the systole |
|
|
angiogenesis
|
growth of new blood vessels from old ones
|
|
|
infarction
|
tissue that becomes necrotic because of inadequate blood supply
|
|
|
after a heart attack, what are the new passage ways that blood travels through?
|
collaterals
|
|
|
draw a diagram of the rapid homeostatic response to a sudden increase in arterial pressure
sudden decrease in bp? |
discussion questions set 5
|
|
|
draw the homeostatic loop that would provide long-term compensation for reduced blood pressure. Now give the loop for long-term compensation of increased blood pressure.
|
discussion 5
|
|
|
draw the o2/hb dissociation curve..label important things
what will make the curve shift to the right or left? |
discussion 5
|
|
|
draw the chloride shift mechanism, where does this occur....now draw the reverse of this...
|
discussion 5 and pg600
|
|
|
How do you know if HR will increase?
|
parameter sheet
|
|
|
how do you know if TPR will increase?
|
parameter sheet
|
|
|
how do you know if SV will increase?
|
parameter sheet
|
|
|
how do you know if will CO increase?
|
parameter sheet
|
|
|
how do you know if VR will increase?
|
parameter sheet
|
|
|
how do you know if DP will increase?
|
parameter sheet
|
|
|
How do you know if PP will increase?
|
parameter sheet
|
|
|
how do you know if MAP will increase?
|
parameter sheet
|
|
|
describe the heart cells....basic
|
-contain desmosomes that transfer force from one cell to adjacent cell
-also contain gap junctions to transfer impulses |
|
|
describe pacemaker
|
-fibro-tendonous ring electrically insulates atria from the ventricles
-AV node is the only pathway in which ventricles can be reached |
|
|
what are gap junctions formed by and what happens when different ones bind?
|
connexins
if different connexins bind, the gap will not be present and the electrical signal will not be conducted |
|
|
draw cardiac E-C coupling
|
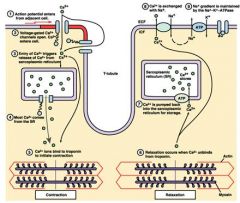
5% of Ca2+ required for contraction enters cardiomyocytes during the action potential from outside
other 95% comes from SR |
|
|
draw action potential of a contractile cell in the heart
|
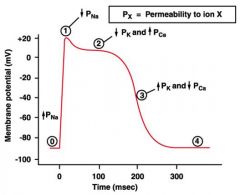
pg473
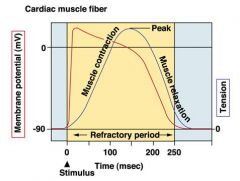
-calcium helps to prevent tetanus from occuring... -a normal muscle cell finishes its entire AP before the muscle cell is done contracting and relaxing...this is not the case with cardiac muscles |
|
|
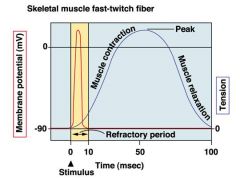
why does skeletal muscle twitch occur?
|
|
|
|
why doesn't cardiac twitch occur?
|
|
|
|
where does excitation begin
|
SA node
|
|
|
draw ap in autorhythmic cells
|
-first part is known as the funny channel
-second part is the Ap -...-60, -40, +20 are the big numbers -permeable to both sodium and potassium but sodium has a larger driving force |
|
|
another name for funny channels?
|
HCN channel
-hyperpolarization-activated cyclic-nucleotide gated channel |
|
|
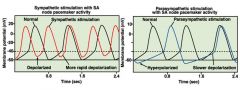
what would happen to the autorhytmic AP if stimulated by sympathetic response?
PS response? |
|
|
|
draw the pathway for epi and ACh interaction on heart autorhythmic cells
also contractile cells |
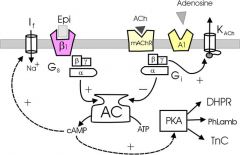
In the pacemaker (chronotropic effect):
a b1 stimulation increases [cAMP], which shifts the activation curve of the ‘funny’ channel, so it activates earlier and faster. It also increases the conduction velocity in the AV node a cholinergic stimulation through the right vagus (SA node) directly activates KACh channel (via mAChR and Gbg), hyperpolarizing the cell. At the same time, Ga inhibits Adenylyl Cyclase, reduces [cAMP], which downregulates the ‘funny’ channel. The left vagus slows down conduction in the AV node and the bundle of His ...right side through PKA affects contractile cells In the contractile myocradium (inotropic effect): a b1 stimulation increases [cAMP], activates PKA which phosphorylates several targets: -L-type Ca2+ channel (DHPR), letting more Ca2+ in -Phospholamban, which increases Ca2+ re-uptake into SR -TnC, which re-sets its Ca2+ binding curve to higher Ca2+ concentration As a result, a more forceful contraction is followed by a deeper relaxation, and the stroke volume increases. |
|
|
what does each part of a ecg mean?
|
|
|
|
draw an ecg with a ventricular action potential
|
|
|
|
CO=
|
CO= SVxHR
SV=EDV-ESV |
|
|
what does EDV depend on
ESV? |
rate of filling (degree of relaxation, ventricular filling pressure and time between strokes)
ESV depends on the contractility and the back pressure on the aorta |
|
|
what does HR depend on?
|
state of the pacemaker, balance of sympathetic and parasympathetic inputs, or alternatively it may rely on an artificial pacemaker
|
|
|
another name for effects on heart rate?
|
chronotropic
|
|
|
another name for effects on heart contraction
|
inotropic
|
|
|
abnormal electrical activity of the heart
|
arrhythmias
ex. tachycardia bradycardia |
|
|
ectopic focus
|
Any part of the heart that initiates an impulse without waiting for the sinoatrial node is called an ectopic focus
|
|
|
types of arrhythmias
|
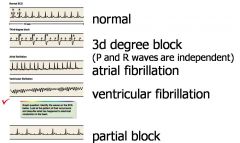
Tachycardia (elevated HR - high sympathetic tone, fever or intoxication)
Bradycardia (reduced HR - under vagal stimulation or abnormally high sensitivity of baroreceptors) Premature atrial or ventricular contractions due to the presence of an ectopic focus - additional pacemaker spot Accessory conduction pathways between atria and ventricles - premature ventricular systole Reentrant tachycardia (AVNRT) - early atrial systole due to re-entry back to atria Fibrillation-uncoordinated contraction of heart muscles |
|
|
how to normalize (usually reduce) the heart rate
|
use anti-arrhythmic effects
Cardiac glycosides, digoxin (Digitalis, Foxglove extract) – Na/K pump blocker (increases the force of contractions, slows the pacemaker down) Propranolol - b-blocker Adenosine – has parasympathomimetic effect - (both ACh and Adenosine reduce cAMP levels, see the messenger cascade) Lidocaine - Na+ channel blocker (prolongs refractory period) Verapamil, Diltiazem - cardiac L-type Ca2+ channel blockers (increase the excitation threshold) |
|
|
how to get rid of bad spots and fibrillation
|
use surgery to remove the following
-ectopic foci -some accessory pathways -some points of re-entry use electric defibrillator to deliver a strong discharge through the chest, re-polarizing (and thus stopping) the entire heart. A minute after the heart has a chance to resume paced contractions. |
|
|
how does digotoxin work?
|
blocks the sodium/k+ pump
increases the force of contraction while slowing the pacemaker down ..positve inotropic effect on myocardium ..negative chronotropic effect on pacemaker..reduces driving force for sodium in funny channels |
|
|
draw p-r and qt interval
|
|
|
|
long q-t syndrome
|
-recessively inherited disorder
-bilateral deafness and cardiac arrhythmias (prolonged q-t interval) -mutation in potassium channel that is expressed in both the ear and the heart -heart k+ is involved in repolarization (defects in timing repolarization is deadly) -the inner ear requires a special compartment filled with K+ rich endolymph...this fluid saves hair cells from sodium poisoning |
|
|
what is the refractory period?
|
the time that the action potential occurs in and no other action potentials can occur
|
|
|
early afterdepolarization that predisposes to a severe arrythmic condition called
|
exam 2 study sheet (1)
early afterdepolarization that predisposes to a severe arrythmic condition called called Torzade de Pointes |
|
|
what do mutations in potassium channels do to heart cells?
|
-prolonged cardiac action potentials beyond the refractory period
-via LQT 1 and 2 |
|
|
explain of blood coming from the left and right heart
|
must pump blood at the same rate
|
|
|
starling law of the heart
|
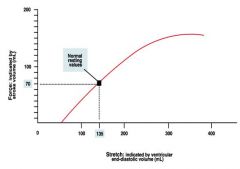
the more fibers are stretched, the more the fibers will contracts
|
|
|
compensation
|
increase of SV and CO following following the pressure buildup in front of the left or right heart
|
|
|
lack of compensation=
|
heart failure
causes congestive disease and edema |
|
|
besides starling law of the heart, what else did starling publish?
|
capillary filtration and absorption is set by osmotic difference between the interstitium and plasma
|
|
|
osmotic pressure=
|
RTC
|
|
|
relationship between capillaries and lymph vessels
|
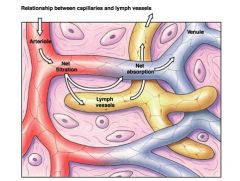
lymph vessels have openings that allow fluid to flow in via bulk flow
|
|
|
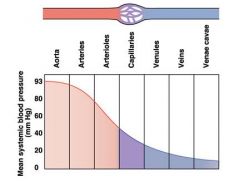
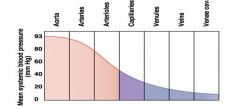
MAP through cardiovascular system
|
|
|
|
starling's capillary hypothesis
|
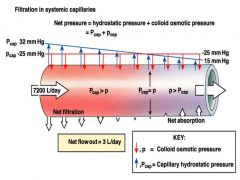
-red is the colloid osmotic pressure...occurs from there being more protein in the capillaries and water following its natural gradient
-capillary hydrostatic pressure decreases because of friction that takes away energy |
|
|
what can cause edema
|
valve regurgitation
cardiac tamponade weak heart infarction heart hypertropy low concentration of serum albumin (malnutrition or liver cirrhosis) dysfunction of lympatics |
|
|
left heart failure
|
pulmonary edema
|
|
|
right heart failure
|
systemic edema
|
|
|
filling is what?
|
passive...no venous pressure....no venous returnm
|
|
|
why is blood loss dangerous
|
hypovolumea reduces the systemic filling pressure which fills the heart
|
|
|
what to do when there is no spare blood to transfuse
|
inject physiological solutions supplemented with plasma expanders
-large molecules such as dextrans will provide onctotic pressure -salt solution will not stay in the blood, but will distribute into tissues and cause a massive systemic edema |
|
|
edema
|
fluid accumulating in the interstium
|
|
|
draw pressure profile throughout the systemic loop
|
|
|
|
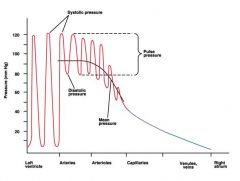
what does the SP and DP really measure?
|
the pressure in the aorta
|
|
|
arterial compliance
|
change in volume/ change in pressure
|
|
|
why is there still pressure during diastole
|
because of elastic recoil that sends blood forward
|
|
|
what happens if heart becomes too big?
|
laplacian disadvantage
T=pr/2 must generate larger tension to achieve sufficient pressure and eject the required amount of blood. After a certain size the heart fails. |
|
|
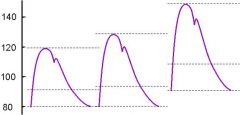
pulse pressure=
|
PP=SP-DP
|
|
|
Mean arterial pressure=
|
the average of the DP and SP....takes into account DP more because it lasts longer
MAP= DP + pp/3 |
|
|
CO=
|
CO=HR*SV
CO=MAP/TPR |
|
|
how is bp measured
|
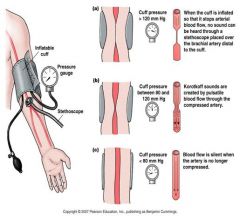
by a sphygmomanometer
-korotkoff sounds are created when pulsatile blood flows through compressed artery |
|
|
what happens to DP, SP and MAP w/ increased HR? at constant TPR
|
they will all increase because the aorta will fill up and the resistance will still be the same
|
|
|
what will Increased TPR do to DP, SP, MAP?
|
increase all of them because more hyrdrostatic will be allowed to act
-to determine, just view the picture of the aorta filling because of increased HR and then filling more because of more TPR |
|
|
what does increased SV do to Sp, DP, and MAP
|
larger increase in SP, smaller increase in DP and MAP
|
|
|
what causes increased sympathetic outflow?
|
worries, excitement, anxiety and a static load (weight with no muscles contracting)
|
|
|
respnonse to worries, excitement, anxiety or static load?
|
increase in pressure values
|
|
|
what does exercise do?
|
incresed SP
decreased DP decreased TPR only slightly raised MAP |
|
|
what does increase to SV and TPR do to BP values
|
increase all
|
|
|
what is complience and what does a decrease of this do to sp?
|
increased SP, decreased DP
complience is how contractile the arteries are....non-complient arteries stiff |
|
|
hyperemia
|
increased perfusion to tissues
|
|
|
vasodilators and vasoconstrictors...these will affect tpr and ap
|
Vasodilators:
CO2, H+, K+ (metabolic) NO, histamine, adenosine ANP (atrial natriuretic peptide) Epi (on b2 receptors) Vasoconstrictors: Serotonin Endothelins Angiotensin II Vasopressin NE, (on a1 receptors) |
|
|
autoregulation of perfusion in tissues
|
1. Myogenic autoregulation adjusts blood flow
2. Paracrines (H+, K+, CO2, NO, histamine, adenosine) relax vascular smooth muscle |
|
|
Relationships between major cardiovascular parameters
|
CO = VR (cardiac output = venous return)
CO = HRxSV, 70 beats/min x 70 ml = 4900 ml/min SV= EDV-ESV CO = mAP/TPR (blood flow=mean DPressure/Total Peripheral Resistance) PP = SP - DP (pulse pressure = Syst. P - Diast. P) mAP = DP+(1/3)PP, Arterial Compliance = DV/DP = SV/PP |
|
|
image of baroreceptor reflex
|

|
|
|
cardio big receptors
|
pacemaker
para: mACh symph: b1 mycoardium para: none symph: b1 vessels are either a1 or b2 depending on what is needed...there is no psympathetic innervation skeletal muscle also has mACh and a1 |
|
|
what neurotransmitters are involved with alpha
beta? |
NE
epi and NE |
|
|
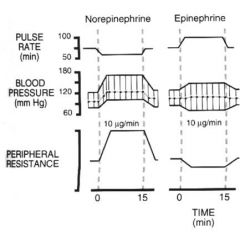
draw ne epi effect on pulse, bp, and TPr
|
|
|
|
how is blood volume regulated by kidneys
|
Blood Loss, BP decrease::::
hypovolumea + sympathetic stimulus Renin is released by kidney Stimulates activation of Angiotensin II Vasoconstriction, thirst, release of ADH (vasopressin) increased H2O reabsorption Release of Aldosterone (increases Na+ reabsorption) BV and BP increase ...too much volume, BPincrese Atrial pressure increases ANP is released by endocardium ANP reduces H2O and Na+ reabsorption (which stimulates excretion) More water is lost into urine together with Na+ BV decreases to normal |
|
|
Ach, epi, and Ne on...
Hr sv tpr vr dp sp pp co |
ACh......
Hr;d sv;i tpr;d vr;d dp;d sp;d pp;?/nc co;d epi... Hr i sv i tpr d vr i dp d sp i pp i co i NE... Hr d sv i tpr i vr i dp i sp i pp i co i alpha is Ne beta is epi and Ne NE increases Hr at first which will increase BP, baroreceptors detect this and then cause a decrease...thus, NE will decrease bp if asked on exam |
|
|
hypertension in experimental animals
|
Renal hypertension (by constriction of renal arteries)
Neurogenic hypetension (by denervation of baroreceptors) Spontaneous (in genetically-predisposed animals) Salt-induced hypertension (in salt-sensitive strains) |
|
|
statistics and treatability in humans of hypertension
|
90% -essential (the cause is not firmly established) -treatable, but not really curable
corrected by administering a1- and b-blockers, inhibitors of angiotensin-converting enzyme (ACE), Ca2+ channel blockers and diuretics 10% - secondary, usually caused by either an endocrine disorder and/or higher retention of fluid. This includes hypersecretion of aldosterone or other mineralocorticoids. Hypersecretion of catecholamines (tumors of adrenal medulla). Narrowing of renal arteries and other renal disorders, which reduce filtration/excretion |
|
|
how do atheroslerosis plaques form?
|
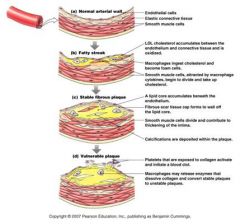
1)ldl cholesterol accumulates
2)macrophages ingest and become foam cells 3)release cytokines that causes smooth muscle to uptake cholesterol 3)lipid core accumulates below endothelium 4)fibrous scar tissue walls off endothelium 5) calcium deposits occur in fat deposit 6)if plaque ruptures, platelets will cause a blood clot |
|
|
arteriosclerosis
|
general hardening of arteries due to fat deposition usually followed by calcification
|
|
|
atherosclerosis
|
formation of atheromatous plaque due to inflammation, macrophage accumulation, and cholesterol (LDL) deposition followed by stenosis (narrowing) of arteries and arterioles. Increases the chance of thrombosis
|
|
|
thrombosis
|
aggregation
formation of a blood clot inside a vessel |
|
|
what are some complications of hypertension?
|
High pressure damage of vascular wall platelet
aggregation thrombosis arteriosclerosis = general hardening of arteries due to fat deposition usually followed by calcification atherosclerosis = formation of atheromatous plaque due to inflammation, macrophage accumulation, and cholesterol (LDL) deposition followed by stenosis (narrowing) of arteries and arterioles. Increases the chance of thrombosis Fat depositions may ‘eat up’ the elastic layer, resulting in weak bulged areas called aneurysms..bad because of laplace's law |
|
|
aneurysm
|
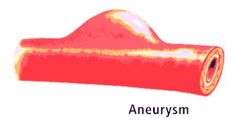
bad because of laplace law that says that
T=pr/2 |
|
|
angioplasty
|
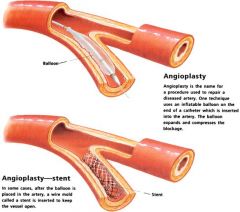
medical procedure to repair diseased artery
-inflatable ballon techneque to compress blockage -a stent can also be inserted to keep the vessel open |
|
|
vicious circle of hypertension
|
High TPR High BP, but tissues still require the same amount of perfusion, thus the heart generates stronger stokes the heart becomes stronger, the arterioles become stiffer, the heart becomes bigger which leads to hypertrophy, Laplacian disadvantage and failure
...caused by positive feedback |
|
|
perfussion
|
In physiology, perfusion is the process of nutritive delivery of arterial blood to a capillary bed in the biological tissue
|
|
|
anaphylaxis
|
Anaphylaxis is an acute systemic (multi-system) and severe Type I Hypersensitivity allergic reaction in humans and other mammals
Anaphylactic shock, the most severe type of anaphylaxis, occurs when an allergic response triggers a quick release from mast cells of large quantities of immunological mediators (histamines, prostaglandins, leukotrienes) leading to systemic vasodilation (associated with a sudden drop in blood pressure) and edema of bronchial mucosa (resulting in bronchoconstriction and difficulty breathing). Anaphylactic shock can lead to death in a matter of minutes if left untreated. |
|
|
septic shock
|
Septic shock is a serious medical condition caused by decreased tissue perfusion and oxygen delivery as a result of infection and sepsis, though the microbe may be systemic or localized to a particular site[1]. It can cause multiple organ dysfunction syndrome (formerly known as multiple organ failure) and death[1]. Its most common victims are children, immunocompromised individuals, and the elderly, as their immune systems cannot deal with the infection as effectively as those of healthy adults. The mortality rate from septic shock is approximately 50% [
|
|
|
tamponade
|
is a condition of blood flow stoppage into a blood vessel by a constriction of the vessel by an outside force.
Tamponade is a useful method of stopping a hemorrhage. This can be achieved by applying an absorbent dressing directly onto a wound, thereby absorbing excess blood and creating a blockage, or by applying direct pressure with a hand or a tourniquet. |
|
|
circulatory shock
and treatment |
- a condition of inadequate perfusion due to insufficient cardiac output
Hypovolumic shock: hemorrhage, trauma or surgery, fluid loss due to diarrhea or vomiting....dehydration or blood loss Distributive shock: anaphylaxis, septic shock Cardiogenic, obstructive or congested shocks: heart failure due to a loss of ventricular or valve function, tamponade, or fibrillation. Low O2 supply may lead to lactic acidosis, kidney failure and coma Refractory shock = condition beyond the “point of no return” With hypovolumic and distributive shocks the major problem is to increase BV and Venous Return - Immediate blood transfusion (when available) - Transfusion of physiological solution with plasma expanders - Injections of NE |
|
|
why is pressure lost as fluid moves through a container
|
friction between the fluid and the blood vessel walls
|
|
|
hydrostatic pressure
|
pressure that a fluid exerts on its container
|
|
|
what do arteries do during the hearts relaxation phase?
|
act as a pressure reservoir
|
|
|
pericytes
|
secrete factors that influenc
|
|
|
coronary heart disease
|
narrowing of the lumen of blood vessels...would like to promote angiogenesis
|
|
|
high bp considered?
|
140/90
|
|
|
how does stuff get out of the capillary
|
hydrostatic pressure forces stuff out through leaky junctions
|
|
|
colloid osmotic pressure?
|
more proteins in the cappilaries so water will want to move in from the interstitual fluid
|
|
|
why does capillary hydrostatic pressure decrease along the length of a cappilary?
|
energy is lost to friction
|
|
|
how does fluid enter lymph vessels from interstitual fluid?
how does flow occur |
there are large gaps that all fluid to flow in by bulk flow
flow occurs by contractile fibeers in endothelial ..one way valves .contraction of skeletal muscle:patients who havent moved in a while will have edema because of this |
|
|
what causes edema
|
1) inadequate drainage of lymph or
2) blood dapillary filtration that greatly exceeds capillary absorption ..increased hydrostatic pressure ..decrease in plasma protein concentration ..increase in interstitial proteins |
|
|
what does a heart attack do
|
-oxygen starved cells rely on glycolysis
-calcium can't be pumped out of cells so gap junctions close because of high ca and h to isolate damaged cells -action potentials must now find a different route |
|
|
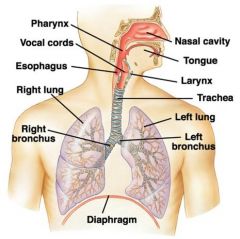
draw the respiration track
|
|
|
|
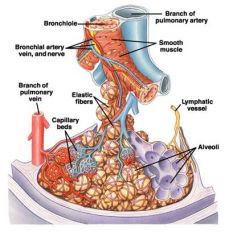
microanatomy of airway at bronchiole level
|
|
|
|
muscles used in ventilation
|
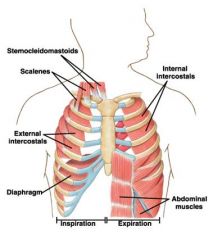
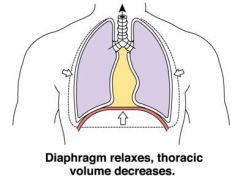
expiration muscles are only used during forced experation...otherwise experation is passive because of recoil
|
|
|
how do ribs increase with lateral motion
|
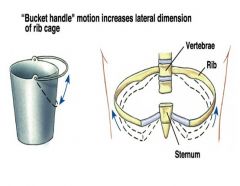
inhalation cause it to lift up and out
|
|
|
diaphragm
|
|
|
|
what is the pleural cavity
|
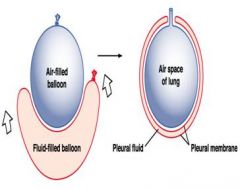
fluid filled with negative pressure
fluid acts to keep lungs attached to thoracic wall like 2 panes of glass |
|
|
air leakage into pleural cavity
and different lung values |
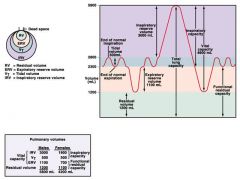
pneumothorax
causes air to rush into pleural cavity and causes lung to deflate |
|
|
tell about all of the lung values
|
|
|
|
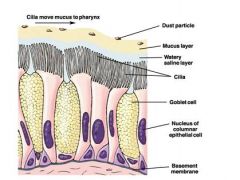
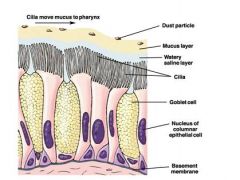
draw ciliated respiratory epithelium of airways
|
|
|
|
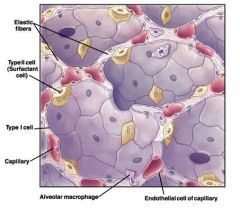
microscopic view of alveolar and endothelial cell of capillary interaction
|
|
|
|
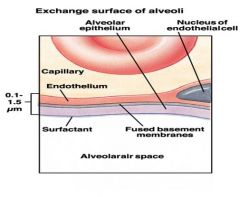
exchange surface of alveoli and capillary
|
|
|
|
2 components of tension in alveolar walls?
|
elastic and surface
|
|
|
surfactants
|
they do not disrupt cohesive forces between water molecules...they, compress the monolayer and because of this decrease surface tension
-DPPC or lecithin is the surfactant in lungs surface pressure of surfactant=surface tension of pure water-surface tension in the presence of surfactant Lung surfactant proteins facilitate fast equilibration between the micellar and surface fractions of surfactant |
|
|
what kinds of alveoles are at disadvantage?
|
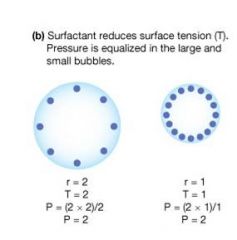
P=2T/r
has a greater inward pressure so they won't fill with air as easily t=surface tension r=radius p=pressure |
|
|
surfactant and infants
|
lack of it causes respiratory distress of infants (collapse of lungs
|
|
|
fibrosis
|
replacement of lung epithelium and elastic fibers with a fibroblast scar tissue (stiff lungs)
|
|
|
Emphysema
|
loss of elastic fibers (lungs are too compliant)
|
|
|
compliancy
|
the rate at which the alveoli will expand
...bag vs.balloon picture bag is very compliant, but not elastic balloon is somewhat compliant, but also elastic |
|
|
rank these in order of distensibilities
normal, no surfactant, water filled |
highest to lowest
water-filled, normal, no surfactant |
|
|
draw a graphic summary of mechanical pulmonary disorders
|
2
|
|
|
what is cystic fibrosis
|
-a disfunction of a chloride channel
-causes thick mucous -Cystic Fibrosis (CF) - is not only pulmonary, but a congenital systemic disorder that hits many epithelial functions in sweat and salivary glands, pancreas and kidney. -caused by mutations in the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR), which is a cAMP-regulated Cl- channel (1480 a.a. protein, 12 TM domains, two nucleotide binding sites, requires cAMP and ATP for proper activity) - one out of 2000 Caucasians carry the DF508 mutation which makes the channel insensitive to cAMP. There are other mutations that prevent intracellular targeting of the channel to the apical membrane. The main cause of death among CFTR patients is lung infection and pneumonia |
|
|
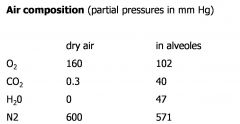
air composition
|
|
|
|
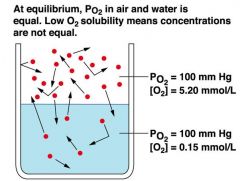
partial pressure and gas solubility of 02
|
|
|
|
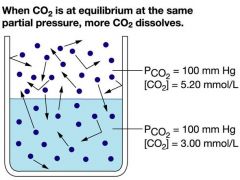
partial pressure and gas solubility of CO2
|
|
|
|
diagram showing basic alveoli, capillary and lung exchange
|

|
|
|
gas flow through the boundary and layer of fluid depends on what?
|
1) solubility
2) rate of diffusion |
|
|
diffusion coefficient=
|
D=S/sroot of MW
|
|
|
po2 changing from 100 to 40 mmhg does what to saturation
|
98% to 75%
|
|
|
50% o2 hb saturation?
|
28 mmHg
|
|
|
physiological range of o2 hb curve
|
40-100 mmhg
|
|
|
what percent of o2 is carried as oxyhemoglobin
|
97% hb02
3% dissolved in plasma |
|
|
how many oxygen bind to Hb and talk about equation
|
4
B=x/(kd+x) x is ligand concentration each x also has an n which is the hill coefficient... * n > 1 - Positively cooperative reaction: Once one ligand molecule is bound to the enzyme, its affinity for other ligand molecules increases. * n < 1 - Negatively cooperative reaction: Once one ligand molecule is bound to the enzyme, its affinity for other ligand molecules decreases. * n = 1 - Noncooperative reaction: The affinity of the enzyme for a ligand molecule is not dependent on whether or not other ligand molecules are already bound. oxygen bind in a cooperative manner |
|
|
carbon monoxide poisoning
|
Oxygen (O2) is coordinated between the Fe ion and the imidazole ring of Histidine E7. Carbon monoxide (CO) binds exactly the same way with a 300 times higher affinity. It displaces O2 and dissociates slowly.
|
|
|
talk about hb
|
4 globular chains with a heme ring that contains iron
|
|
|
when does an increase of 2,3-dpg take place?
|
-high altitude or under the action of growth hormones
-23dpg shifts curve to the right |
|
|
3 ways co2 is transported
|
~7% is carried as CO2 dissolved in plasma
~70% is in the form of bicarbonate. The conversion is catalyzed by carbonic anhydrase CO2+H2O = H2CO3 = H+ + HCO3- ~23% as carbamino compound at the N-terminus of Hb -C-NH2 + CO2 = -C-NH-COOH |
|
|
haldane effect
bohr effect |
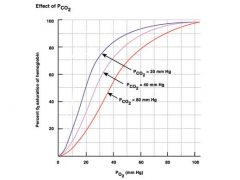
Deoxygenation of the blood increases its ability to carry carbon dioxide; this property is the Haldane effect. Conversely, oxygenated blood has a reduced capacity for carbon dioxide. This is a consequence of the fact that reduced (deoxygenated) hemoglobin is a better proton acceptor than the oxygenated form.
bohr:Bohr effect is a property of hemoglobin first described in 1904 by the Danish physiologist Christian Bohr (father of physicist Niels Bohr), which states that in the presence of carbon dioxide, the oxygen affinity for dissociation of respiratory pigments, such as hemoglobin, decreases; because of the Bohr effect, an increase in blood carbon dioxide level or a decrease in pH causes hemoglobin to bind to oxygen with less affinity. |
|
|
hematocrit
|
fraction of blood that is taken up by rbc's when centrifuged
|
|
|
chloride shift
|
an electrically neutral Cl-/HCO3- exchange occurs via the Band 3 anion exchanger.
|
|
|
what is special about blood in the lungs
|
blood is not fully oxygenated...20% remains venous...creates a physiologic shunt
|
|
|
hypoventilation vs. hyperventilation
|

|
|
|
ventilation vs perfusion rates
|
Ventilation (V) = 4.2 L/min
Perfusion (Q) = 5 L/min V/Q = 0.84 (normal) this indicates shunting because the perfused blood (blood reaching the lung) is not being properly ventillated shunting is when some blood remains venous and does not pick up oxygen |
|
|
effects of high altitude
|
Plasma CO2 decreases, pH increases and this leads to alkalosis. To correct for this condition acids need to be taken (citric acid).
At high altitude (low PO2) Erythropoietin is released, increasing hematocrit. Blood viscosity does up, making circulation less efficient |
|
|
when the blood flow is insufficient in a certain locus this is equivalent to ?
|
increase in dead space...space in airways with no gas exchange
|
|
|
when the ventilation is insufficient, this is equivalent to increased amount of?
|
shunted blood
|
|
|
a decrease in ventilation in a certain locus leads to
|
constriction of corresponding arterioles and diverting blood to better ventilated alveoli
|
|
|
table of gas compositin vs. bronchioles, pulmonary arterioles, systemic arterioles
|
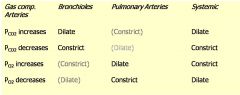
common sense if you think about it...just the gas component
|
|
|
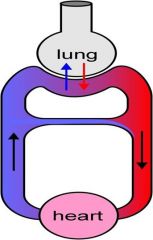
pulmonary loop of circulation is characterized by?
|
low pressure and high throughput
|
|
|
the boundary between the dry and blood compartments is
|
very thin and delicate
|
|
|
what keeps alveoli dry
|
low capillary pressure
-powerful lympatic system that keeps interstitial pressure negative (-4 to -8 mmHg) |
|
|
what follows alveolar edema
|
interstitial edema...lethal in 30 min
when left atrial pressure rises above 23 mmHg it becomes dangerous |
|
|
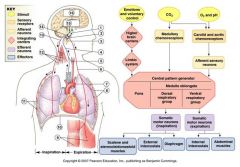
scheme for how respiratory muscles control respiration
|
|
|
|
comment on respiratory muscle innervation
|
third forth and fifth cervical segments throgh the thoracic cavity to the diaphragm
intercostal muscles are innervated by the spinal segmental nerves of the 1st through 11th spinal segments, they don't branch from the phrenic nerve |
|
|
respiratory chemoreceptors
|
Chemoreceptors
O2 Receptors in the aortic arch and carotid bodies, reside in glomus cells (K+ channels directly sensitive to [O2], non-adaptable, fire when PO2 gets below 60 mm Hg) Peripheral CO2 (pH) Receptors (in the aortic arch and carotid bodies) fire when plasma pH is low Central CO2 Receptors are located in the medulla, next to the inspiratory center. They are bathed in CSF and sensitive to the pH of CSF, which depends on plasma CO2 Central receptors are insensitive to plasma pH (H+ can not permeate through the blood brain barrier). All CO2 receptors are adaptable, i.e. during sustainrd stimulation their firing declines with time. In contrast, O2 receptors do not adapt. |
|
|
what type of channel is the oxygen receptor?
|

potassium channel
|
|
|
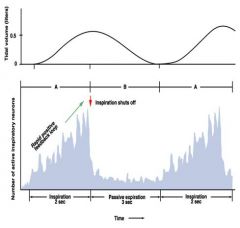
inspiratory ramp
|
|
|
|
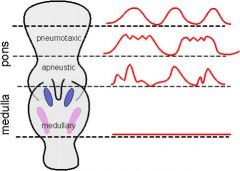
functional anatomy of the respiratory center
|
|
|
|
feedback loop that leads to intercostal muscles and diaphragm contracting
|
4
|
|
|
chemoreceptor reflex
|
Low arterial oxygen levels cause bardycardia and elevated TPR
Vasoconstriction in response to low O2 compensates the vasodilatory effect of accumulated CO2 |
|
|
respiratory sinus arrhythmia
|
During inspiration - sympathetic stimulation increases (tachycardia)
During expiration- parasympathetic activity increases (bradycardia) |
|
|
respiratory sinus arrhythmia
|
During inspiration - sympathetic stimulation increases (tachycardia)
During expiration- parasympathetic activity increases (bradycardia) |
|
|
physiolgy of diving
diving animals and scuba divers |
Diving reflex: temporary brdycardia on exposure to cold water, usually combined with peripheral vasoconstriction
The skeletal muscles are forced to draw on its store of O2 in myoglobin and then shift to anaerobic glycolysis - O2 is therefore spared for the heart and brain Lactic acid is accumulated in muscles and washed out at the end of the dive Diving animals exhale before they dive. Deep in the seas their lungs collapse and the residual gas is stored in the ‘dead’ space. No N2 dissolved in the blood at high pressure. Scuba divers breathe air which is exactly at the same pressure as is in the surrounding water. At depths greater than 30 m, a considerable amount of N2 gets dissolved in the plasma, so on decompression (assent) it may form bubbles. The bubbles cause ‘divers bends’. Therefore, decompression must be slow. There are tables stipulating safety stops during assent to allow time to clear N2 from the blood. |
|
|
4 types of immune hypersensitivity
|
There are four types of immune hypersensitivity reactions:
1. IgE - mediated mast cell degranulation (histamine and leukotriene release) 2. Cytotoxic action of killer cells and complement mediated by IgG directed against ‘self’ antigen (autoimmune IgG) 3. Immune complex deposition in tissues (antigen-antibody clot), attracting complement and polymorphonuclear cells that cause local damage of tissue 4. Sensitization of T-cells on the first exposure to antigen and massive release of cytokines followed by inflammatory reaction on the second contact Asthma is type 1 |
|
|
asthma
|
-type 1
-strongly hereditary in the young (70%) - allergic reaction to pollen and other inhaled allergens (dust mite feces, cat dander particles, fungal spores, rat urine) - in older individuals (30%) - reaction to persisting irritants in the polluted air Allergic reaction= development of sensitivity to the irritant and generation IgE against it. Mast cells and basophils reside in the mucus layer close to the airway lining. They carry IgE receptors (Fc) on their surface which bind IgE’s from the plasma. On arrival of the stimulus (irritant) crosslinking of Fc receptors occurs, the mast cells degranulate and release histamine and a mix of leukotrienes and prostaglandins (substance of anaphylaxis), then also release IL-4 and TNF-a. -edema and brochospasm occur. airway resistance increases which makes it difficult to inhale and especially exhale -asthma is an allergan induced bronchial edema and bronospasm |
|
|
corticosteroids
|
Corticosteroids (Cortisol, Hydrocortisone) generally suppress inflammation and immune response
- in macrophages and monocytes they induce the protein called lipocortin, which blocks PLA2 and the production of arachidonic acid, prostaglandins and leucotriens - block IgE-dependent degranulation of basophils and mast cells - in endothelial cells they prevent release of molecules that mediate leukocyte adhesion and tissue penetration - suppress adhesion and proliferation of fibroblasts that form scar tissue (fibrosis, sclerosis). - inhibit release of cytokines (IL’s) from lymphocytes |
|
|
obstructive lung disease
|
narrowing of the bronchioles
|
|
|
pneumothorax
|
air in the pleural sac
|
|
|
boyles law
|
pv=pv
|
|
|
solubilities of O2 and co2 in water
|
co2 is 20x more soluble
at 100 mmhg co2= 3 mmol/L o2=.15 mmol/l both have a conc of 5.2mmol o2/L air |
|
|
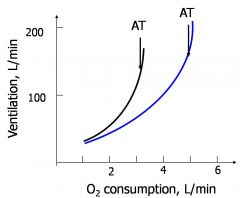
trained vs. untrained o2 consumption curve
|
|
|
|
exercise
|
O2 consumption reliably measures the intensity of exercise
~ 5 kcal of metabolic work per liter O2 During the most strenuous exercise we spend ~20 kcal/min, and consume 4-5 L O2/min Ventilation increases to 120-150 L/min, in proportion with the aerobic (oxidative) metabolism - both inspiration and expiration become active processes Ventilation increases faster when we reach the anaerobic threshold (AT) |
|
|
glycolysis
|
glucose > 2 pyruvate or 2 lactic acid
2 ADP + 2 Pi +NAD > 2ATP + 2 NADH |
|
|
oxidative phosphorylation
|
glucose +602 > 6co2 + 6 h20
30 adp + 30 pi > 30 atp + 30 H + 30h20 process is 32 percent effective |
|
|
fatty acids can only be used in what metabolism?
|
aerobic
|
|
|
where does glucose come from
|
glycogen or dietary intake
|
|
|
what and where can lactic acid be converted to
|
glucose by the liver
|
|
|
cardiovascular adjustments to exercise
|
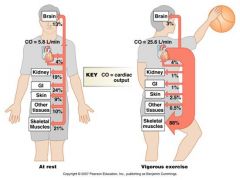
Cardiac output increases 4-5 times (to 20-25 L/min)
- SV increases insignificantly - HR increases up to 200 beats/min - Systemic filling pressure (SFP) increases from 7 to 18 mm Hg, a small increase in pulmonary AP occurs - blood is diverted from skin and other organs (but perfusion remains constant in the brain) - TPR decreases 4-5 times, in some muscles perfusion increases 40 times - Due to SFP and TPR, the venous return matches CO - BP increases insignificantly (~20%) |
|
|
energy supply
|
1. Easily consumable energy is stored in fat (adipose tissue)
2. Carbohydrates (glycogen) is consumed next. We have 55-90 g in liver and 12g/kg in muscles 3. Under extreme conditions ~ 10 kg of muscle protein is available too (consumed under exhaustion) At <60% of work load: 80% extramuscular fat is consumed, 20% glycogen (aerobic slow-twitch) 60-90% of load: 30% extramuscular carbohydrate, 70% local glycogen >90% load - mostly local glycogen (glycolytic metabolism) |