![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
42 Cards in this Set
- Front
- Back
|
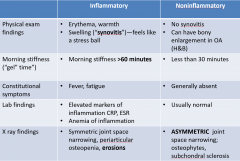
Articular vs non-articular
|
Art: Pain on active & passive ROM, limited ROM, swelling, crepitus, instability Non-art: Pain on active ROM only, focal tenderness outside articular, rare swelling/crepitus/instab |
|

|
|
|
|
Heberden's vs Bouchard's nodes? indicative of? |
Heberden's: DIP joint Bouchard's: PIP joint Both in OA |
|
|
DDx monoarticular arthritis |
Crystalline (Gout/pseudogout) Septic Traumatic hemarthrosis |
|
|
DDx oligoarticular arthritis (2-4 joints) |
OA Spondyloarthropathy RA Lupus Gonorrhea |
|
|
DDx diffuse poly arthritis |
Acute Viral Infections RA Spondyloarthropathy Lupus |
|
|
Most common locations for OA |
Knee Hip CMC, PIP, DIP Spine Shoulder sometimes |
|
|
Hand joint involvement of OA vs RA |
OA: CMC (wrist), PIP, DIP RA: MCP, PIP |
|
|
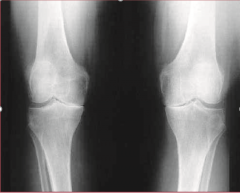
How to diagnose OA? x-ray findings? |
Chronic pain/ loss of fn Morning stiffness <30min H&P Xray: Asymmetric joint space narrowing osteophytes, cortical bone thickening, subchon cysts |
|
|
OA |
|
|
57 yo manpresents with bilateral knee pain that he has struggled with “for years”. He notes he works in the Army Corp ofEngineers and is on his feet a lot at job sites. The pain is worse at the end of the day whenhe has been walking and standing all day. His only PMHx isHTN and obesity. He takes only lisinopril forhis BP. ROSnegative for redness, swelling, fever Exam: NAD, no appreciable effusion of knee, noerythema, no warmth. Significantcrepitus with extension of bilateral knees. Mild ttp overjoint line. Dx? |
OA |
|
|
•A48 yowoman who is very active presents with a 2 week hx of bilateral knee pain, R>L. •Shenotes she gets the pain while doing Crossfit which she does at least 4x per week•Shedescribes the pain as a burning, “stinging” pain below both knees that is worsewith doing squats and tire throws•Examreveals no crepitus, erythema, or warmth but she does note mild “soreness” overmedial aspect of proximal tibia bilaterally; no bony prominence or swelling ispresent Dx? |
Pes Anserine Bursitis |
|
|
Pes anserine bursitis sx? dx? |
Pain just below knee at anteromedial aspect of tibia that occurs when exercising or climbing stairs Exam reveals TTP over pes anserine bursa |
|
|
53 yo manpresents to clinic after traveling to Disney World with his family one weekago. He notes that during a parade, hewas standing still and turned with his body, but his right knee did not turnwith him. He heard a pop and since thenhis knee has been swollen. He feels thathis knee is going to “give out” and it will occasionally lock on him. Stairs are “out of the question”. Examreveals mild swelling of right knee, no erythema, minimal warmth Dx? tests? |
Meniscal injury +McMurray's test |
|
|
Meniscal injury sx |
Painusually occurs acutely and/or is associated with trauma A/wbuckling and “locking” of knee Exam:tenderness over joint line, effusion (hemarthrosis) McMurray+: clicking felt when knee compressed & rotated during varus & valgus stress |
|
|
•60yowoman comes in with 12 months of left hip discomfort, worse with standing forlong periods of time. She feels the painas a dull ache but notes that a lot of her pain is actually in her groin area. She has no PMHx.•Examreveals decreased ROM of flexion at her left hip and pain when logrolling herhip. Dx? |
OA |
|
|
42 yowoman presents with 3 month history of pain over her right hip that is worse atnight. In fact, it wakes her from sleep if she rolls onto that side. She denies any radiation of the pain. It is somewhat better with ibuprofen.•Examreveals normal ROM; logrolling does not produce pain. She is tender to palpation over the greatertrochanter dx? |
Trochanteric bursitis |
|
|
36yowoman presents with ache in her lower right back and into her hip. She notes it is worse with sitting crosslegged with her kids. Pain is worse withactivity. FABERtest is positive on the right. ROMnormal; logrolling does not produce pain. dx? |
Sacroiliitis |
|
|
Test for shoulder OA |
NFL sign: see if pt can raise arms above head. Compare sides. OA: not smooth, discomfort, inability to complete |
|
|
Biceps tendonitis caused by? confirmatory test? |
Due to impingement or instability. Pain f/ lifting, pulling, or repetitive overhead movements TTP in bicipital groove suggests tendonitis |
|
|
45 yo presents with right shoulder stiffness and inability to get things from the topshelf of his pantry.•Ptstates he hurt his shoulder last summer while weed eating and it “hasn’t feltright since”•Onexam, he is wearing a navy over the shoulder sling. The pt has been wearing it around the house to“help with the pain” Dx? |
Adhesive capsulitis/ Frozen Shoulder |
|
|
Adhesive capsulitis/ Frozen Shoulder sx & tests? |
ROM limited on active & passive motion Usually painless Apley Scratch Test: reduced ROM (asses ROM f/ above to back & below to back) Touchdown Sign is expected (inability tofully raise effected arm) |
|
|
40man comes in with right shoulder pain that came on gradually over the last fewweeks. Ptnoticed that pain is worsened after playing in church softball league and atNIGHT.•Onexam he has full ROM, pain with drop arm maneuver but able to smoothly controlhis arm, no TTP over biceps tendon.•Strengthis 5/5 in bilateral UE, DTR’s are 2+ and symmetric Dx? |
Rotator cuff tendonitis (most common shoulder pain seen) No hx of trauma Nighttime sx present |
|
|
54 yopsychologist sees you for finger pain. She notes it has been going on for “years”. She thinks that her hands and wrists are“fine” but her the joints of her fingers just keep getting bigger such that shecannot wear any of her rings. She deniesany erythema or warmth. PE reveals bony enlargement of DIP and PIP on 2nd and3rd digits bilaterally, no warmth orerythema. Dx? |
OA |
|
|
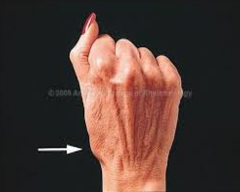
CMC squaring: OA |
|
|
45yoobese woman with PMHx ofRA comes in with bilateral hand pain and numbness•Sheworks as a machinist in a factory•Shereports hand and wrist pain worse at night thatgets better after “shaking it out”, both hands are affected. Shenotes that she sometimes feels clumsy with her hands and notes numbnessalong her middle fingers. dx? |
Carpal tunnel syndrome |
|
|
Dx/tests for Carpal tunnel? |
Median n dermatomal numbness Phalens test: fully flex both hands placing back of palms together for 60s. + is pain/paresthesia Tinel's test: Tap firmly on median nerve. + is pain/paresthesia Abduction weakness: Hand palm up, try to raise thumb against resistance |
|
|
35yowoman G2P1 comes into your office c/o wrist and thumb pain•Sheis 3months pregnant andaccompanied by her 11 month old daughter •PMHxnoncontributory•Ptnoticed pain while knitting her new baby a blanket•Reportspainis along thumb and wrist atbase of thumb, sharp “pinching” pain•Whatis your diagnosis? |
DeQuervain’sTenosynovitis |
|
|
DeQuervain’s Tenosynovitis cause? sx? dx? |
Extensive wrist/thumb action (gripping/grasping) Tenderness at snuff box Finkelstein maneuver: thumb in fist, ulnar deviation, (+) = pain |
|
|
43yowoman presents with pain at the base of her fingers x 4 weeks. She notes the pain is worse first when shewakes up and that it takes a few hours for her hands to “loosen up”. She reports that her fingers have also feltswollen over this time. •Examreveals swelling and synovitis of 2nd MCP joints bilaterally and 4th PIP on right hand. dx? |
RA |
|
|
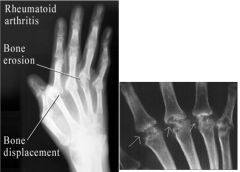
RA features? xrays? tests? |
Symmetric polyarthritis w/ prolonged morning stiffness Xray: Periarticular osteopenia, erosions, symmetric joint space narrowing elevated RF & Anti-CCP |
|

|
End stage RA: ulnar drift, MCP involvement |
|

|
|
|
|
26yowoman with PMHx ofporiasis presents with right 3rdfinger swelling. She notes that thefinger had occasionally felt “kinda sore” for months, but this morning whenshe got up her whole finger looked like a “bratwurst”. Shedenies any fevers, chills.PE reveals diffuse dactylitis ofright 3rd finger. dx? |
Psoriatic arthritis |
|

|
Dactylitis "sausage finger" psoriatic arthritis |
|

|
Pencil in cup deformity: psoriatic arthritis |
|
|
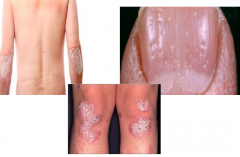
Psoriasis |
|
|
Finkelstein maneuver |
pain elicited by flexing thumb into palm, closing fingers over thumb, then bending wrist in ulnar direction; a confirmatory test in DeQuervain’s tenosynovitis (also look for tenderness at anatomic snuffbox) |
|
|
Drop arm test? |
the patient raises arm to 90 degrees of abduction and lower it slowly. A suddenly dropped arm is considered positive and suggestive of a rotator cuff tear. |
|
|
Drawer sign test? |
knee flexed to 90 degrees and examiner pulls lower leg anteriorly; ability to move leg > 1 cm is consistent with ACL tear |
|
|
Gout |
causedby uric acid crystal deposition in joint, this disease usually begins acutelywith intense pain and inflammatory joint finding. 90% of patients have great toeinvolvement. Rarely occurs inpremenopausal women. |
|
|
McMurray test? |
palpable clicking with knee compression and rotation during varus and valgus stress; positive test indicates meniscal injury (acute onset of pain, often with trauma, buckling or locking sensation) |