Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
35 Cards in this Set
- Front
- Back
|
with this anaerobic bacteria you may see a distinctive double zone of hemolysis in culture...what is this bacteria?
|
Clostidium perfingens
|
|
|
where is clostidium botulinum found normally (its habitat)?
|
in the environment
can get it from eating improperly canned food |
|
|
patient comes in with Nausea, vomiting, dizziness cranial palsy, double vision, swallowing difficulties. Upon H&P you discover that the family has a fancy for canned peaches. What caused the disease?
|
Clostidium botulinum
it can grow in poorly canned foods |
|
|
how does Clostidium botulinum lead to paralysis? note the difference from tetni
*** |
get flaccid paralysis because the toxin prevents the ACh vesicles from docking at the presynaptic terminal
note that in tetni it was a spastic paralysis due to inhibition of inhibitory interneurons (say that 10x fast!) |
|
|
how is disease caused by Clostidium botulinum different in infants (as opposed to adults)
|
Ingestion of spores → exotoxin → constipation and generalized weakness (floppy baby syndrome)
baby will eventually be OKAY. |
|
|
why do you not give a child honey who is suspected of Clostidium botulinum?
|
spores can live in it
|
|
|
what are the 2 virulence factors seen in Clostridium difficile and what do they do?
** |
toxin A (enterotoxin) → fluid production and mucosal damage
toxin B (cytotoxin) → kills mucosal cells |
|
|
what do you use for treatment of Clostridium difficile?
|
metronidazole (or vancomycin if resistant)
|
|
|
Extensive tissue destruction,
Thrombosis of blood vessels, Abundant bacteria spreading through fascial planes, are features of what? |
Necrotizing Fasciitis
|
|
|
how can you differentiate necrotizing fasciitis from simple cellulitis?
|
Pain out of proportion to the clinical appearance of the skin affected
Identify those at increased risk: diabetics, others with abnormal peripheral circulation, immunocompromised, traumatic wounds, or surgical incisions High fever Toxic appearance |
|
|
describe the two types of necrotizing fasciitis
|
Type I – diabetes mellitus, abdominal surgery, perineal infection
-----Mixed infection: anerobes, anaerobic streptococci, facultative organisms (synergistic nonclostridial myonecrosis) Type 2 – Grp A streptococcus (flesh eating strain) Other etiologies: Aeromonas hydrophilia and Vibrio vulnificus |
|
|
Type I vs Type II necrotizing fasciitis
caused by Grp A streptococcus (flesh eating strain) |
Type II
|
|
|
Type I vs Type II necrotizing fasciitis
caused by diabetes mellitus, abdominal surgery, perineal infection |
Type I
|
|
|
Type I vs Type II necrotizing fasciitis
caused by mixed infection |
Type I
|
|
this infection has a very unpleasant sour odor and resembles gas gangrene. What is this?
|
Type I necrotizing fasciitis
|
|
|
this disease has Copious seropurulent exudate occurs 3-4 days after injury
Unpleasant sour odor, and If muscles involved, react to stimulation (differentiate from clostridial myonecrosis) what is it |
Type I necrotizing fasciitis
|
|
|
your colleague is trying to diagnose necrotizing fasciitis but he is unsure if it is type one or two
you see numerous streptococci, pleomorphic gram negative rods with many poly’s in the gram stain and a mixed culture which is it? |
type I
|
|
|
what is a left shift?
|
large number of WBCs (+12000)
|
|
|
Leukocytosis with a left shift and Elevated sedimentation rate can be seen in what?
|
necrotizing fasciitis
|
|
|
Elevated creatinine phosphokinase
Hypocalcemia Hypoalbuminemia Leukocytosis with a left shift Elevated sedimentation rate are all features of what? |
necrotizing fasciitis
|
|
|
what is used to treat Type II necrotizing fasciitis
|
penicillin
|
|
|
if you are trying to determine if you have Type I or II necrotizing fasciitis what is something unique you will see in the gram stain in type II?
|
gram positive cocci in chains
(streptococcus) |
|
|
if you suspect gangrene but you see no gas, what do you have? caused by?
|
necrotizing fasciitis caused by Streptococcus pyogenes
|
|
|
is Aeromonas hydrophilia oxidase positive?
|
yes it has cytochrome C
|
|
|
where do Aeromonas hydrophilia live
|
fresh water
|
|

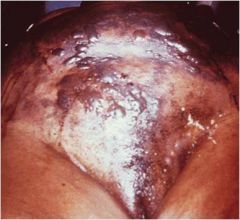
A 59 y/o white male diabetic with significant vascular disease lacerated his left thumb on a brim fish dorsal fin. He fell on his left forearm 24 hrs later, sustaining a hematoma. Twelve hrs later he presented in septic shock. Image on left shows bullae and edema of left forearm at time of presentation
|
Aeromonas hydrophilia
|
|
|
what causes gas gangrene? (usually)
|
Clostridium perfringens
|
|
|
A rapidly progressive, life- threatening, toxemic infection of subcutaneous tissue and skeletal muscle due to clostridia (usually Clostridium perfringens)
what is this? |
Gas Gangrene (Clostridial myonecrosis)
|
|
|
Accidental traumatic injury with compound fracture
Penetrating war wounds Surgical wounds (abdominal) Artery insufficiency in an extremity are predisposing factors for what? |
gas gangrene due to Clostridium perfringens
|
|
|
patient presents wtih Blebs containing sero-sanguineous fluid develop in overlying skin and areas of green-black cutaneous necrosis appear, you also see crepitus
what is this? |
gas gangrene due to Clostridium perfringens
|
|
|
your patient has Gas bubbles may be visible in the discharge, Involved muscle undergoes rapid disintegration and fails to contract upon stimulation, and Skin around wound is usually swollen and white → yellowish discoloration
what does he have? |
gas gangrene due to Clostridium perfringens
|
|
|
what causes Spontaneous, non-traumatic gas gangrene
*** |
Clostridium septicum
|
|
|
this disease is Associated with colon cancer, diverticulitis, and gastrointestinal surgery and has the clinical presentation of
Bacteremia Pain Fever what do they have? due to? |
Spontaneous, non-traumatic gas gangrene (due to Clostridium septicum)
|
|
|
outline the steps leading to Myalgia
** |
Macrophages → IL-1 + TNF → prostaglandin E2
→ muscle protease |
|

comic of the day
|
:)
|