![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
305 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
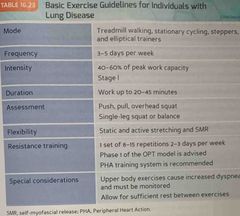
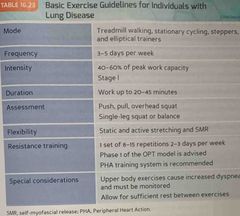
Basic exercise guidelines for individuals with lung disease : |
Back (Definition) |
|
|
|
CHD is caused by |
Atherosclerosis (plaque formation). |
|
|
|
Arthrosclerosis causes CHD, which leads to |
Narrowing of the coronary arteries & ultimately angina pectoris (chest pain), myocardial infarction (heart attack) or both. |
|
|
|
The primary cause of CHD is |
Poor lifestyle choices, primarily cigarette as smoking, Poor diet, physical inactivity. |
|
|
|
The emphasis on treating CHD is centered on improving the |
Health of the internal lining of the coronary artery, called plaque “stabilization”. |
|
|
|
The other primary focus on the treatment of CHD is through |
Medical management, including pharmaceuticals & aggressive lifestyle intervention. |
(eating better, more exercise, smoking cessation, & stress reduction) |
|
|
The risk of serious cardiovascular complications, even death, is |
Low in exercise programs that include clients with CHD. |
|
|
|
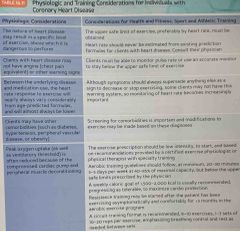
Physiologic in training considerations for individuals with CHD : |
Back (Definition) |
|
|
|
Clients must be able to find in monitor their own |
Pulse rate/use an accurate monitor to stay below their safe upper limit of exercise. |
|
|
|
The heart rate response to exercise in those with CHD can vary |
Considerably from age predicted formulas, & will often be lower. |
|
|
|
Signs and symptoms should always supersede all those as a sign to |
Decrease or stop exercising. |
|
|
|
Signs and symptoms vary greatly among individuals with CHD, so careful |
Monitoring of HR, RPE, & signs of worsening CHD (angina) are important. |
|
|
|
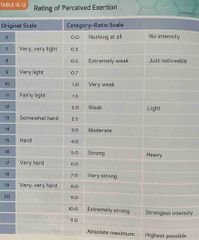
RPE : |
Back (Definition) |
|
|
|
What are the benefits of exercise for those with CHD |
Lower risk of mortality Increased exercise tolerance, muscle strength. Reduction in angina/heart failure symptoms. Improved physiological status & social judgement. |
|
|
|
Heart disease may be slowed (even reversed) when a multifactor |
Intervention program of intensive education, exercise, counseling, & lipid lowering medications are used (appropriately). |
|
|
|
What assessment should be used for those with CHD? |
Single leg balance (or squat). |
|
|
|
If possible, what position should those with CHD perform their exercises? |
In a seated or standing position because they are the easiest & safest. |
|
|
|
When using SMR on the CHD client you |
Consult with a registered/licensed physician. |
|
|
|
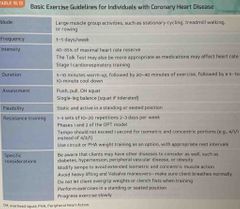
Cardio respiratory training for those with CHD should focus on what stage? |
Stage 1, Progressing only with the physicians advice. |
|
|
|
Core & resistance training exercises should be performed in what position for those with CHD? |
The standing or sitting position. |
Prone Iso-ab (planks) on an incline Standing torso cable iso-rotation Cobras in a standing position (two or single) |
|
|
What type of training would not be recommended for those with CHD in the initial months of training? |
Plyometric |
|
|
|
What faces of the OPT model would be appropriate for the CHD population? And what style of training should be performed? |
Phases 1 & 2. Circuit style or peripheral heart action (PHA) training. |
|
|
|
Basic exercise guidelines for those with coronary heart disease : |
Back (Definition) |
|
|
|
Who does osteoporosis affect & can it be treated? |
Osteoporosis affects both men & women & is treatable. |
|
|
|
Type 1 osteoporosis is most prevalent in |
Postmenopausal women because of a deficiency in estrogen (usually secondary to menopause). |
|
|
|
Osteoporosis is characterized by an increase in ___ with a decrease in ___, leading to ___. |
Increase : bone resorption (removal of old bone) Decrease : bone remodeling (formation of new bone) Leading : decrease in BMD |
|
|
|
Osteoporosis commonly affects the |
Neck of the femur & the lumbar vertebrae. |
|
|
|
Add a crease and BM D places what in a weakened state? |
The core, which is more susceptible to injury (fracture). |
|
|
|
Risk of hip fractures doubles how often in post menopausal women? |
Every five years in women over the age of 50. |
|
|
|
How many American individuals already have osteoporosis? |
10 million. |
|
|
|
How many Americans are estimated to have low bone mass? |
34 million, this place is the individuals at risk for developing osteoporosis in the future.. |
|
|
|
How many Americans does osteoporosis affect each year? How many are affected by hip fractures? |
25 million each year, 1.5 million hip fractures. |
|
|
|
Basic exercise guidelines for those with coronary heart disease : |
Back (Definition) |
|
|
|
Of the one point million hip fractures what percentage of patients return to a normal functional status?What is one of the most important risk factors that influence |
20% |
|
|
|
What is one of the most important risk factors that influence osteoporosis? |
Peak bone mass (or density). |
|
|
|
What is peak bone mass? |
The highest amount of bone mass a person is able to achieve during their lifetime. |
|
|
|
Stress placed on the musculoskeletal system. |
Stress placed on the musculoskeletal system. |
|
|
|
To maintain consistent bone remodeling, people must remain |
Active enough to ensure adequate stress on their body, especially adolescents/young adults trying to reach peak bone mass. |
|
|
|
Client should be encouraged to increase dietary |
Intake of calcium, decrease alcohol intake, & cease to smoking. |
|
|
|
Whether client has osteopenia or osteoporosis it is important to determine to what degree the client may engage in |
(Weight-bearing activities walking, jogging, dancing, stair climbing, etc.) or resistance training |
|
|
|
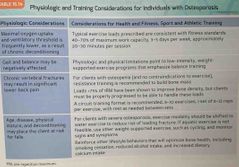
Physiologic & training considerations for individuals with osteoporosis : |
Back (Definition) |
|
|
|
There is a balance between the benefit of providing exercises that are designed to increase bone through the provision of bone stress (weight-bearing exercise or heavy resistance exercise) & the |
Risk of fracture that might be predicted by advanced osteoporosis. |
|
|
|
Osteopenia |
A decrease in calcification/density of bone & reduced bone mass. |
|
|
|
What does BMD stand for? |
Bone mineral density. |
|
|
|
What is a precursor to osteoporosis? |
Osteopenia |
|
|
|
Osteoporosis |
A decrease in bone density & mass & an increase in the space between bones, resulting in porosity & fragility. |
|
|
|
And osteoporosis BMD is reduced, |
Bone microstructure is disrupted, & the actual proteins in the bones are altered. |
|
|
|
What are the 2 types or Classes of osteoporosis? |
Type 1 (primary) Type 2 (secondary) |
|
|
|
Physiologic & training considerations for individuals with osteoporosis : |
Back (Definition) |
|
|
|
Estrogen & progesterone are involved in regulating what? |
The rate at which bone is lost. |
|
|
|
Those who participate in resistance training have a higher |
BMD than those who do not. |
|
|
|
Cardiorespiratory training should begin and stage what for those with osteoporosis? |
Stage 1 (with a walking program if tolerated). |
|
|
|
What type of activities may be more beneficial to increasing BMD? |
Weight bearing. |
|
|
|
Progression to the stage 2 cardio respiratory training should be based on what for those with osteoporosis? |
Physician’s advice & clients ability. |
|
|
|
What are some examples of core exercises in standing position? |
Prone iso-abs on incline Cobras understanding position Standing cable torso iso-rotation Medicine ball rotations |
|
|
|
Care should be taken with crunches or movements with |
Spinal flexion. |
Monitor ROM |
|
|
What training should those with osteoporosis not perform? |
Plyometrics |
|
|
|
What intensity of exercise is needed to stimulate bone formation? |
75-85% |
|
|
|
What is the determining factor in the information? |
The load (rather than the number of reps). |
|
|
|
How many months of consistent exercise at a relatively high intensity does it take before any effect on bone mass is realize?Exercise training programs for those with osteoporosis may be performed and what type of style or system |
6 months |
|
|
|
Exercise training programs for those with osteoporosis may be performed in what type of style or system? What do they focus on? |
Circuit style or PHA system Focus : hips, thighs, back, & arms. |
|
|
|
Resistance training improves BMD by no more than |
5% |
|
|
|
Progressing exercises to the standing position will help increase stress to thenl |
Hips, thighs, and back as well as increase the demand for balance. |
|
|
|
20% |
20% |
|
|
|
Training that focuses on what is more advantageous for the elderly? |
On the prevention of falls. |
|
|
|
Exercise regimens that combine what type of training would better facilitate the needs of the osteoporosis population? |
Resistance training to increase BMD with flexibility, core, & balance to enhance proprioception. |
|
|
|
If the client demonstrates the ability to move fairly well without assistance, these movement assessments may be followed : |
Overhead squat, single leg squat or balance, push, pull assessments. |
|
|
|
If a client is not able to get around very well, it is a good idea to use more |
Stable, machine based equipment during the assessment process & exercise program. |
|
|
|
When working with those with osteoporosis you must follow the kinetic chain checkpoints |
As closely as possible, (there may be degenerative changes in their posture that cannot be corrected). |
|
|
|
What position should you try to get osteoporosis clients into? |
Their own ideal position, not a general ideal position, & to exercise while seated/standing. |
|
|
|
Flexibility should be what with those with osteoporosis? |
Limited to active & static stretching. |
SMR may be contradicted |
|
|
Arthritis |
Chronic inflammation condition of the joints. |
|
|
|
Osteoarthritis |
Arthritis in which the cartilage gets soft, frayed, or thins out, as a result of trauma or other conditions. |
|
|
|
Rheumatoid arthritis |
Arthritis primarily affecting connective tissues, there’s a thickening of articulate soft tissue, & extension of synovial tissue over articular cartilage that has become eroded. |
|
|
|
What is the leading cause of disability for adults in the United States? |
Arthritis |
|
|
|
Arthritis is associated with significant |
Activity limitation Work disability Reduce the quality of life High health care |
|
|
|
What percentage of the United States population has arthritis? |
21.6% 46.4 million |
|
|
|
What are the 2 most common types of arthritis? |
Osteoarthritis Rheumatoid arthritis |
|
|
|
Arthritis |
Chronic inflammation condition of the joints. |
|
|
|
Rheumatoid arthritis may affect what? |
Joints & organ systems. |
|
|
|
What joints are most commonly affected by rheumatoid arthritis? |
Hands, wrists, knees, & feet. |
|
|
|
Osteoarthritis |
Arthritis in which the cartilage gets soft, frayed, or thins out, as a result of trauma or other conditions. |
|
|
|
Rheumatoid arthritis |
Arthritis primarily affecting connective tissues, there’s a thickening of articulate soft tissue, & extension of synovial tissue over articular cartilage that has become eroded. |
|
|
|
What is the leading cause of disability for adults in the United States? |
Arthritis |
|
|
|
Arthritis is associated with significant |
Activity limitation Work disability Reduce the quality of life High health care |
|
|
|
What percentage of the United States population has arthritis? |
21.6% 46.4 million |
|
|
|
What are the 2 most common types of arthritis? |
Osteoarthritis Rheumatoid arthritis |
|
|
|
The lack of cartilage from osteoarthritis creates a wearing on the |
Surfaces of articulating bones, causing inflammation & pain at the joint. |
|
|
|
Some of the most commonly affected joints of osteoarthritis are in theRheumatoid arthritis can cause an |
Hands, hips, knees & spine. |
|
|
|
Rheumatoid arthritis can cause what type of response in multiple joints? |
An inflammatory response, leading to pain & stiffness. |
|
|
|
Arthritis |
Chronic inflammation condition of the joints. |
|
|
|
Rheumatoid arthritis may affect what? |
Joints & organ systems. |
|
|
|
What joints are most commonly affected by rheumatoid arthritis? |
Hands, wrists, knees, & feet. |
|
|
|
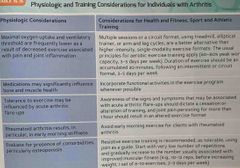
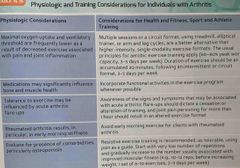
What is rheumatoid arthritis characterized by? |
Morning stiffness lasting longer than half an hour, acute or chronic, with eventual loss of joint integrity. |
|
|
|
In the presence of an arthritis flareup,What should be monitored to progress |
Even flexibility exercises may need to be postponed. |
|
|
|
What should be monitored of a client with arthritis? |
Progress, to assess the effects of the exercise program on joint pain. |
|
|
|
Pain persisting for more than one hour after exercise is an indication that |
The exercise should be modified or eliminated from the routine. |
|
|
|
What should be avoided to decrease joint aggravation in those with arthritis? |
High intensity exercises with high repetitions. |
|
|
|
Osteoarthritis |
Arthritis in which the cartilage gets soft, frayed, or thins out, as a result of trauma or other conditions. |
|
|
|
Rheumatoid arthritis |
Arthritis primarily affecting connective tissues, there’s a thickening of articulate soft tissue, & extension of synovial tissue over articular cartilage that has become eroded. |
|
|
|
What is the leading cause of disability for adults in the United States? |
Arthritis |
|
|
|
Arthritis is associated with significant |
Activity limitation Work disability Reduce the quality of life High health care |
|
|
|
What percentage of the United States population has arthritis? |
21.6% 46.4 million |
|
|
|
What are the 2 most common types of arthritis? |
Osteoarthritis Rheumatoid arthritis |
|
|
|
The lack of cartilage from osteoarthritis creates a wearing on the |
Surfaces of articulating bones, causing inflammation & pain at the joint. |
|
|
|
Some of the most commonly affected joints of osteoarthritis are in theRheumatoid arthritis can cause an |
Hands, hips, knees & spine. |
|
|
|
Rheumatoid arthritis can cause what type of response in multiple joints? |
An inflammatory response, leading to pain & stiffness. |
|
|
|
What type of program or session format is suitable for those with arthritis? |
A circuit program or multiple session format. |
|
|
|
Physiologic & training considerations for individuals with arthritis : |
Back (Definition) |
|
|
|
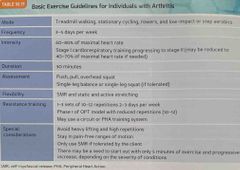
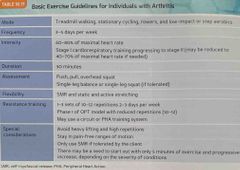
Basic exercise guidelines for individuals with arthritis : |
Back (Definition) |
|
|
|
How do you increase functional capacity in balance of clients with arthritis? |
progressing exercises so that they are performed in the seated position(without support) & standing. |
|
|
|
What type of approach is important in the assessment and activities or recommendations? Why?What should you note during activity assessments for those with |
Methodical, & to reduce reduce symptoms of flareups. |
|
|
|
What should be noted during assessments for those with arthritis? |
Pain free ROM. |
|
|
|
What exercise can assist in decreasing symptoms associated with arthritis? |
Improving muscular strength & enhancing flexibility. |
|
|
|
What forms of stretching can be used and may be better tolerated from a seated or standing position? |
Static & active stretching. |
SMR may be used if tolerated. |
|
|
Cardiorespiratory training should begin with stage? When should it be progressed? |
Stage 1, progressing to stages 2 & 3. Depending on the clients capabilities & physicians approval. |
|
|
|
Core and balance exercises will be very important for those with arthritis to |
Increased levels of joint stability & balance. |
|
|
|
Physiologic & training considerations for individuals with arthritis : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with arthritis : |
Back (Definition) |
|
|
|
What phases of the OPT model will be used for those with arthritis? |
1 |
|
|
|
How Will exercises be modified for those with arthritis? Why? |
Reps 10-12 To avoid heavy, repetitive joint loading that increase stress to the affected joints. |
|
|
|
Cancer |
Types of malignant neoplasms, may metastasize to several sites, & are likely to recur after attempted removal & to cause death of a patient unless adequately treated. |
Mostly invading surrounding tissues. |
|
|
What is the 2nd leading cause of death in United States? |
Cancer |
|
|
|
How many deaths annually does cancer cause? |
1/2 million. |
|
|
|
What percentage of probability do American men & women have of developing cancer in their lifetime? |
44% men 38% women |
|
|
|
What positive benefits does exercise have in the treatment of cancer? |
Improved aerobic & muscular fitness retention of lean body mass Less fatigue Improved quality of life Positive effects on mood & self concept |
|
|
|
Cancer’s signs & symptoms vary widely because |
It’s a collection of diseases sharing the same description (with respect to cell division, accumulation, & death) |
|
|
|
Medications used by clients with cancer can result in substantial adverse affects, what does this include? |
Nausea Peripheral nerve damage Cardiac & pulmonary problems Skeletal muscle myopathy (muscle weakness & wasting) Anemia |
There are 5 |
|
|
When cancer patients exercise it can improve |
Exercise tolerance Reduce cellular risk Improve quality-of-life |
|
|
|
People exhibiting osteoarthritis have a decrease in |
Strength & proprioception. |
|
|
|
What intensity & duration of exercise has a more positive affect on the immune system of a client with cancer? |
Low to moderate intensity for moderate durations. |
|
|
|
What type of intensity is associated with decreased incidence of morality rates for certain forms of cancer? |
High levels |
|
|
|
What assessments should be representative of the clients ability level? (Cancer) |
Push, pull, OH squat, & single leg balance (only a single leg squat can’t be performed) |
|
|
|
Individuals with arthritis have a decreased ability to |
Balance while standing. |
|
|
|
A loss in knee-extensor strength is a strong predictor of |
Osteoarthritis |
|
|
|
Patients with osteoarthritis exhibited increased |
Muscle inhibition of the knee extensors & were not able to effectively activate their knee extensor musculature to optimal levels. |
|
|
|
Balance or proprioception in muscle strength are vital components of ___ any deficit in these areas could potentially have a ___. |
Walking, negative affect on the ability to exercise & perform ADL. |
|
|
|
Individuals with arthritis advised to participate in regular |
Exercise programs following the OPT methodology for increasing stabilization, ADL, & strength, |
|
|
|
It is important to restore what in a deconditioned client who has joint limitations secondary to arthritis? |
Functional mobility & endurance. |
|
|
|
What symptoms of arthritis are heightened through inactivity. As a result of what?Muscle atrophy and lack of tissue flexibility |
Joint stiffness & pain. Muscle atrophy and lack of tissue flexibility. |
|
|
|
What type of program or session format is suitable for those with arthritis? |
A circuit program or multiple session format. |
|
|
|
Physiologic & training considerations for individuals with arthritis : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with arthritis : |
Back (Definition) |
|
|
|
How do you increase functional capacity in balance of clients with arthritis? |
progressing exercises so that they are performed in the seated position(without support) & standing. |
|
|
|
What type of approach is important in the assessment and activities or recommendations? Why?What should you note during activity assessments for those with |
Methodical, & to reduce reduce symptoms of flareups. |
|
|
|
What should be noted during assessments for those with arthritis? |
Pain free ROM. |
|
|
|
What exercise can assist in decreasing symptoms associated with arthritis? |
Improving muscular strength & enhancing flexibility. |
|
|
|
What forms of stretching can be used and may be better tolerated from a seated or standing position? |
Static & active stretching. |
SMR may be used if tolerated. |
|
|
Cardiorespiratory training should begin with stage? When should it be progressed? |
Stage 1, progressing to stages 2 & 3. Depending on the clients capabilities & physicians approval. |
|
|
|
Core and balance exercises will be very important for those with arthritis to |
Increased levels of joint stability & balance. |
|
|
|
Physiologic & training considerations for individuals with arthritis : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with arthritis : |
Back (Definition) |
|
|
|
What phases of the OPT model will be used for those with arthritis? |
1 |
|
|
|
How Will exercises be modified for those with arthritis? Why? |
Reps 10-12 To avoid heavy, repetitive joint loading that increase stress to the affected joints. |
|
|
|
Cancer |
Types of malignant neoplasms, may metastasize to several sites, & are likely to recur after attempted removal & to cause death of a patient unless adequately treated. |
Mostly invading surrounding tissues. |
|
|
What is the 2nd leading cause of death in United States? |
Cancer |
|
|
|
How many deaths annually does cancer cause? |
1/2 million. |
|
|
|
What percentage of probability do American men & women have of developing cancer in their lifetime? |
44% men 38% women |
|
|
|
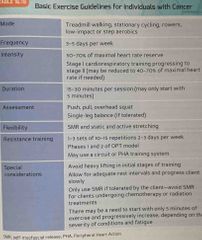
What positive benefits does exercise have in the treatment of cancer? |
Improved aerobic & muscular fitness retention of lean body mass Less fatigue Improved quality of life Positive effects on mood & self concept |
|
|
|
Cancer’s signs & symptoms vary widely because |
It’s a collection of diseases sharing the same description (with respect to cell division, accumulation, & death) |
|
|
|
Medications used by clients with cancer can result in substantial adverse affects, what does this include? |
Nausea Peripheral nerve damage Cardiac & pulmonary problems Skeletal muscle myopathy (muscle weakness & wasting) Anemia |
There are 5 |
|
|
When cancer patients exercise it can improve |
Exercise tolerance Reduce cellular risk Improve quality-of-life |
|
|
|
People exhibiting osteoarthritis have a decrease in |
Strength & proprioception. |
|
|
|
What intensity & duration of exercise has a more positive affect on the immune system of a client with cancer? |
Low to moderate intensity for moderate durations. |
|
|
|
What type of intensity is associated with decreased incidence of morality rates for certain forms of cancer? |
High levels |
|
|
|
What assessments should be representative of the clients ability level? (Cancer) |
Push, pull, OH squat, & single leg balance (only a single leg squat can’t be performed) |
|
|
|
What type of flexibility should be included in the workout for clients with cancer? |
Static & active stretching SMR if there are no complications |
|
|
|
SMR |
SMR |
|
|
|
Cardio respiratory training is important for the cancer population, but may have to start with stage two or three of cardiorespiratory training may be used on agreements |
5 minutes of stage 1 training, progressing up to 30 minutes, 3-5 days/week. |
|
|
|
Stage 2 or 3 of cardiorespiratory training maybe used on agreement of |
The client’s physician. |
|
|
|
Core $ balance exercises will be essential for those with cancer because they help in regaining |
Stabilization necessary for ADL that may have been lost (as a result of lack of activity caused by treatment). |
|
|
|
Plyometric training is not recommended until when? |
Three phases of |
The client has officially progressed performing 3 complete phase 1 workouts/week. |
|
|
Resistance training for those with cancer will include what phases of the OPT model? |
Phases 1 & 2, other phases maybe used as the client progresses & are approved by their physician. |
|
|
|
Individuals with arthritis have a decreased ability to |
Balance while standing. |
|
|
|
Basic exercise guidelines for individuals with cancer : |
Back (Definition) |
|
|
|
What are the major disparities observed in athletic performance between men & women? |
There are 4 |
|
|
|
What measures are adjusted for body composition, what changes? |
Both physiologic & performance parameters narrow considerably or completely vanish. |
|
|
|
What fears can be minimized with appropriate precautions that the fetus may be harmed? |
Increase blood circulation Thermal regulatory changes Decreased oxygen supply |
There are 3 |
|
|
What recreational pursuits are appropriate for pregnant women? |
Most recreational pursuits are appropriate for all pregnant women. |
|
|
|
Those already engaged in an exercise program before pregnancy may |
Continue with moderate levels of exercise until the 3rd trimester, a logical reduction in activity is recommended after. |
|
|
|
Basic exercise guidelines for individuals with cancer : |
Back (Definition) |
|
|
|
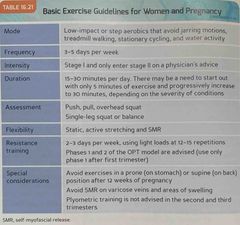
Course stabilization exercises are particularly important for pregnant women to |
Improve strength of the pelvic floor musculature. |
|
|
|
As the mother to be progresses to more advanced stages of pregnancy (2nd & 3rd trimester, or after 12 weeks) what type of exercises are not advised? |
Exercises in the prone or supine position Uncontrolled twisting motions of the torso Resistance: Hip abduction abduction |
|
|
|
What changes occur in the cardiovascular system during pregnancy? |
Decreasing work capacity, leading to necessary alterations in the cardio respiratory program Increased importance of proper hydration during aerobic activity |
|
|
|
A loss in knee-extensor strength is a strong predictor of |
Osteoarthritis |
|
|
|
Pregnant women should immediately stop exercising if they experience what symptoms? |
Abdominal pain (contractions) Excessive shortness of breath Bleeding/leakage of amniotic fluid Nausea, dizziness, & fainting |
There are 6 |
|
|
Changes that occurred during pregnancy may persist for how long? |
A month to a month & a half. |
|
|
|
Post natal women should be encouraged to re-educate their |
Posture Joint alignment Muscle imbalances Stability Motor skills Recruitment of deep core musculatures (transverse abdominis, internal oblique, pelvic floor) |
There are 6 |
|
|
What type of assessment should be used for pregnant women? |
Seated & standing assessments Single leg squat Single leg balance (if single leg squat cannot be performed) |
|
|
|
What type of flexibility exercises should pregnant women perform? |
Sitting & standing positions, especially in the 2nd & 3rd trimesters Static & active stretching SMR (if it can be tolerated) |
|
|
|
Where should SMR not be performed? |
On their varicose veins that are sore, or on areas where there is swelling (calves). |
|
|
|
When is SMR not advised for pregnant women? |
In the 2nd & 3rd trimesters in the prone or supine positions. |
|
|
|
Cardio respiratory training should consist in what stages for pregnant women? |
Stage 1, only answer stage 2 on a physician’s note. |
|
|
|
Women who have not exercised before pregnancy can begin with how many minutes of continuous aerobic activity? |
15 mins of continuous aerobic activity & gradually progress to 30 mins of low to moderate aerobic activity. |
|
|
|
What type of training is not advised for the pregnancy population after the 3rd trimester? |
Plyometric training. |
|
|
|
Patients with osteoarthritis exhibited increased |
Muscle inhibition of the knee extensors & were not able to effectively activate their knee extensor musculature to optimal levels. |
|
|
|
What phase of the OPT model maybe used in the first trimester? What phases can be used in the second and third trimesters? |
1st trimester : Phases 1 & 2 2nd & 3rd trimesters : phase 1 only |
|
|
|
Basic exercise guidelines for women & pregnancy : |
Back (Definition) |
|
|
|
What is one of the leading preventable causes of death & primary risk factor for the development of chronic lung diseases? |
Smoking |
|
|
|
What are the 2 major categories of chronic lung disease? |
Obstructive & restrictive |
|
|
|
Restrictive lung disease |
Condition of a fibrous lung tissue, resulting in a decreased ability to expand the lungs. |
|
|
|
Basic exercise guidelines for women & pregnancy : |
Back (Definition) |
|
|
|
What may have caused the decrease In Law and capability? |
Fractured ribs NM disease Obesity |
|
|
|
Balance or proprioception in muscle strength are vital components of ___ any deficit in these areas could potentially have a ___. |
Walking, negative affect on the ability to exercise & perform ADL. |
|
|
|
Individuals with arthritis advised to participate in regular |
Exercise programs following the OPT methodology for increasing stabilization, ADL, & strength, |
|
|
|
It is important to restore what in a deconditioned client who has joint limitations secondary to arthritis? |
Functional mobility & endurance. |
|
|
|
What symptoms of arthritis are heightened through inactivity. As a result of what?Muscle atrophy and lack of tissue flexibility |
Joint stiffness & pain. Muscle atrophy and lack of tissue flexibility. |
|
|
|
What type of program or session format is suitable for those with arthritis? |
A circuit program or multiple session format. |
|
|
|
Physiologic & training considerations for individuals with arthritis : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with arthritis : |
Back (Definition) |
|
|
|
How do you increase functional capacity in balance of clients with arthritis? |
progressing exercises so that they are performed in the seated position(without support) & standing. |
|
|
|
What type of approach is important in the assessment and activities or recommendations? Why?What should you note during activity assessments for those with |
Methodical, & to reduce reduce symptoms of flareups. |
|
|
|
What should be noted during assessments for those with arthritis? |
Pain free ROM. |
|
|
|
What exercise can assist in decreasing symptoms associated with arthritis? |
Improving muscular strength & enhancing flexibility. |
|
|
|
What forms of stretching can be used and may be better tolerated from a seated or standing position? |
Static & active stretching. |
SMR may be used if tolerated. |
|
|
Cardiorespiratory training should begin with stage? When should it be progressed? |
Stage 1, progressing to stages 2 & 3. Depending on the clients capabilities & physicians approval. |
|
|
|
Core and balance exercises will be very important for those with arthritis to |
Increased levels of joint stability & balance. |
|
|
|
Physiologic & training considerations for individuals with arthritis : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with arthritis : |
Back (Definition) |
|
|
|
What phases of the OPT model will be used for those with arthritis? |
1 |
|
|
|
How Will exercises be modified for those with arthritis? Why? |
Reps 10-12 To avoid heavy, repetitive joint loading that increase stress to the affected joints. |
|
|
|
Cancer |
Types of malignant neoplasms, may metastasize to several sites, & are likely to recur after attempted removal & to cause death of a patient unless adequately treated. |
Mostly invading surrounding tissues. |
|
|
What is the 2nd leading cause of death in United States? |
Cancer |
|
|
|
How many deaths annually does cancer cause? |
1/2 million. |
|
|
|
What percentage of probability do American men & women have of developing cancer in their lifetime? |
44% men 38% women |
|
|
|
What positive benefits does exercise have in the treatment of cancer? |
Improved aerobic & muscular fitness retention of lean body mass Less fatigue Improved quality of life Positive effects on mood & self concept |
|
|
|
Cancer’s signs & symptoms vary widely because |
It’s a collection of diseases sharing the same description (with respect to cell division, accumulation, & death) |
|
|
|
Medications used by clients with cancer can result in substantial adverse affects, what does this include? |
Nausea Peripheral nerve damage Cardiac & pulmonary problems Skeletal muscle myopathy (muscle weakness & wasting) Anemia |
There are 5 |
|
|
When cancer patients exercise it can improve |
Exercise tolerance Reduce cellular risk Improve quality-of-life |
|
|
|
People exhibiting osteoarthritis have a decrease in |
Strength & proprioception. |
|
|
|
What intensity & duration of exercise has a more positive affect on the immune system of a client with cancer? |
Low to moderate intensity for moderate durations. |
|
|
|
What type of intensity is associated with decreased incidence of morality rates for certain forms of cancer? |
High levels |
|
|
|
What assessments should be representative of the clients ability level? (Cancer) |
Push, pull, OH squat, & single leg balance (only a single leg squat can’t be performed) |
|
|
|
What type of flexibility should be included in the workout for clients with cancer? |
Static & active stretching SMR if there are no complications |
|
|
|
SMR |
SMR |
|
|
|
Cardio respiratory training is important for the cancer population, but may have to start with stage two or three of cardiorespiratory training may be used on agreements |
5 minutes of stage 1 training, progressing up to 30 minutes, 3-5 days/week. |
|
|
|
Stage 2 or 3 of cardiorespiratory training maybe used on agreement of |
The client’s physician. |
|
|
|
Core $ balance exercises will be essential for those with cancer because they help in regaining |
Stabilization necessary for ADL that may have been lost (as a result of lack of activity caused by treatment). |
|
|
|
Plyometric training is not recommended until when? |
Three phases of |
The client has officially progressed performing 3 complete phase 1 workouts/week. |
|
|
Resistance training for those with cancer will include what phases of the OPT model? |
Phases 1 & 2, other phases maybe used as the client progresses & are approved by their physician. |
|
|
|
Individuals with arthritis have a decreased ability to |
Balance while standing. |
|
|
|
Basic exercise guidelines for individuals with cancer : |
Back (Definition) |
|
|
|
What are the major disparities observed in athletic performance between men & women? |
There are 4 |
|
|
|
What measures are adjusted for body composition, what changes? |
Both physiologic & performance parameters narrow considerably or completely vanish. |
|
|
|
What fears can be minimized with appropriate precautions that the fetus may be harmed? |
Increase blood circulation Thermal regulatory changes Decreased oxygen supply |
There are 3 |
|
|
What recreational pursuits are appropriate for pregnant women? |
Most recreational pursuits are appropriate for all pregnant women. |
|
|
|
Those already engaged in an exercise program before pregnancy may |
Continue with moderate levels of exercise until the 3rd trimester, a logical reduction in activity is recommended after. |
|
|
|
Basic exercise guidelines for individuals with cancer : |
Back (Definition) |
|
|
|
Course stabilization exercises are particularly important for pregnant women to |
Improve strength of the pelvic floor musculature. |
|
|
|
As the mother to be progresses to more advanced stages of pregnancy (2nd & 3rd trimester, or after 12 weeks) what type of exercises are not advised? |
Exercises in the prone or supine position Uncontrolled twisting motions of the torso Resistance: Hip abduction abduction |
|
|
|
What changes occur in the cardiovascular system during pregnancy? |
Decreasing work capacity, leading to necessary alterations in the cardio respiratory program Increased importance of proper hydration during aerobic activity |
|
|
|
A loss in knee-extensor strength is a strong predictor of |
Osteoarthritis |
|
|
|
Pregnant women should immediately stop exercising if they experience what symptoms? |
Abdominal pain (contractions) Excessive shortness of breath Bleeding/leakage of amniotic fluid Nausea, dizziness, & fainting |
There are 6 |
|
|
Changes that occurred during pregnancy may persist for how long? |
A month to a month & a half. |
|
|
|
Post natal women should be encouraged to re-educate their |
Posture Joint alignment Muscle imbalances Stability Motor skills Recruitment of deep core musculatures (transverse abdominis, internal oblique, pelvic floor) |
There are 6 |
|
|
What type of assessment should be used for pregnant women? |
Seated & standing assessments Single leg squat Single leg balance (if single leg squat cannot be performed) |
|
|
|
What type of flexibility exercises should pregnant women perform? |
Sitting & standing positions, especially in the 2nd & 3rd trimesters Static & active stretching SMR (if it can be tolerated) |
|
|
|
Where should SMR not be performed? |
On their varicose veins that are sore, or on areas where there is swelling (calves). |
|
|
|
When is SMR not advised for pregnant women? |
In the 2nd & 3rd trimesters in the prone or supine positions. |
|
|
|
Cardio respiratory training should consist in what stages for pregnant women? |
Stage 1, only answer stage 2 on a physician’s note. |
|
|
|
Women who have not exercised before pregnancy can begin with how many minutes of continuous aerobic activity? |
15 mins of continuous aerobic activity & gradually progress to 30 mins of low to moderate aerobic activity. |
|
|
|
What type of training is not advised for the pregnancy population after the 3rd trimester? |
Plyometric training. |
|
|
|
Patients with osteoarthritis exhibited increased |
Muscle inhibition of the knee extensors & were not able to effectively activate their knee extensor musculature to optimal levels. |
|
|
|
What phase of the OPT model maybe used in the first trimester? What phases can be used in the second and third trimesters? |
1st trimester : Phases 1 & 2 2nd & 3rd trimesters : phase 1 only |
|
|
|
Basic exercise guidelines for women & pregnancy : |
Back (Definition) |
|
|
|
What is one of the leading preventable causes of death & primary risk factor for the development of chronic lung diseases? |
Smoking |
|
|
|
What are the 2 major categories of chronic lung disease? |
Obstructive & restrictive |
|
|
|
Restrictive lung disease |
Condition of a fibrous lung tissue, resulting in a decreased ability to expand the lungs. |
|
|
|
Basic exercise guidelines for women & pregnancy : |
Back (Definition) |
|
|
|
What may have caused the decrease In Law and capability? |
Fractured ribs NM disease Obesity |
|
|
|
What are the major obstructive lung diseases? |
Asthma Emphysema Chronic bronchitis |
There are 3 |
|
|
Asthma, chronic bronchitis, and emphysema are characterized by |
Chronic inflammation (smoking or environmental irritants) & airway obstruction via mucus production. |
|
|
|
What is the genetic disorder cystic fibrosis? |
A disease characterized by excessive mucus production. |
|
|
|
Balance or proprioception in muscle strength are vital components of ___ any deficit in these areas could potentially have a ___. |
Walking, negative affect on the ability to exercise & perform ADL. |
|
|
|
What problems may occur during exercise for individuals with restrictive or obstructive lung disease? |
Decreased ventilation Decreased gas exchange, resulting in decreased aerobic capacity & endurance. Decreased oxygen desaturation |
|
|
|
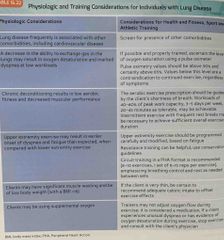
Clients with lung disease experience what at low levels of exercise? |
Shortness of breath or dyspnea. |
|
|
|
Those with emphysema are |
Frequently underweight Exhibit overall muscle wasting with hypertrophied neck muscles (excessively used to assist in labored breathing). |
|
|
|
Those with bronchitis are |
Overweight Barrel chested |
|
|
|
Exercises for those with chronic lung diseases are similar to what would be appropriate for |
The general population. |
|
|
|
What can exercise improve with in those with chronic lung disease? |
Dyspnea. |
|
|
|
What type of exercises are best tolerated for those with chronic lung disease? |
The use of lower body cardio respiratory & resistance training exercises. |
|
|
|
What type of exercises places increased stress on those with chronic lung disease? |
Upper extremity exercises places an increased stress on the secondary respiratory muscles involved in stabilizing the upper extremities. |
|
|
|
What should be insured when designing programs for those with chronic lung diseases? |
Adequate rest intervals |
|
|
|
What training system would be advised for those with chronic lung disease? |
The peripheral heart action (PHA)training system. |
|
|
|
Individuals with arthritis advised to participate in regular |
Exercise programs following the OPT methodology for increasing stabilization, ADL, & strength, |
|
|
|
Physiologic and training considerations for individuals with lung disease : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with lung disease : |
Back (Definition) |
|
|
|
Physiologic and training considerations for individuals with lung disease : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with lung disease : |
Back (Definition) |
|
|
|
The term peripheral vascular disease is also commonly used to describe |
The activity induced symptoms that characterized this disease (PAD). |
|
|
|
Intermittent claudication is characterized by what symptoms? |
Limping, lameness, pain in the lower leg during mild exercise resulting from a decrease in blood supply (oxygen) to the lower extremities. |
|
|
|
Peripheral arterial disease (PAD) |
A condition characterized by narrowing of the major arteries responsible for supplying blood to the lower extremities. |
|
|
|
What is the primary limiting factor for exercise for clients with PAD? |
Leg pain. |
|
|
|
Know the difference between intermittent claudication versus similar leg complaints such as |
Cramping Tightness Pain These may be associated with deconditioning. |
|
|
|
The symptoms I have a client diagnosed with PADI likely to be accurate for |
intermittent claudication, they still could be associated with deconditioning. |
|
|
|
It is important to restore what in a deconditioned client who has joint limitations secondary to arthritis? |
Functional mobility & endurance. |
|
|
|
When should a personal trainer referred a client to a licensed physician immediately? |
If the pain continues during exercise. |
|
|
|
PAD is associated with what diseases? |
Coronary heart disease Diabetes |
|
|
|
What may have to be decreased depending on the clients abilities? (Lung disease) |
The number of reps during assessments. |
|
|
|
What type of stretching should be used for those with lung disease? |
Static & active stretching |
SMR should not be used unless approved by a licensed physician. |
|
|
What phases of the OPT model is suggested for those with lung disease? |
Phase 1 with reps starting at 8-12, slowly progressing to 12-20. |
|
|
|
How many exercise bouts should those with lung disease initially start with? |
5-10 mins of activity, progressing slowly to 20-30 mins. |
|
|
|
Physiologic & training considerations for individuals with intermittent claudication or PAD : |
Back (Definition) |
|
|
|
Physiologic & training considerations for individuals with intermittent claudication or PAD : |
Back (Definition) |
|
|
|
Basic exercise guidelines for individuals with intermittent claudication or PAD : |
Back (Definition) |
|