Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
119 Cards in this Set
- Front
- Back
|
Requirement thyroid FNA adequacy?
|
6 groups of 10 follicular cells
OR Abundant colloid OR Diagnostic tissue |
|
What are these cells?
|
Hurthle cells/ oncocytes
Metaplastic follicular cells with abundant mitochondria |
|
|
What conditions do you see MNGCs in the thyroid?
|
subacute thyroiditis
granulomatous diseases benign follicular nodules with cystic degeneration papillary carcinoma undifferentiated (anaplastic) carcinoma. |
|
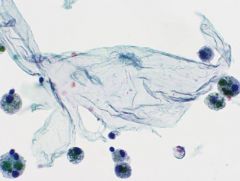
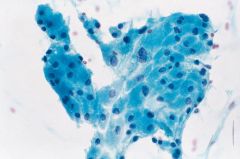
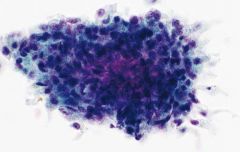
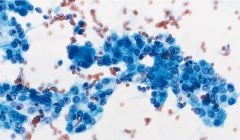
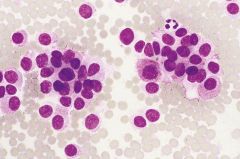
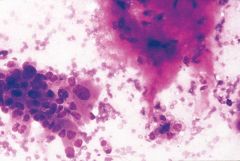
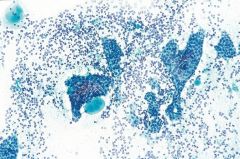
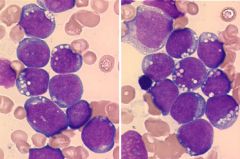
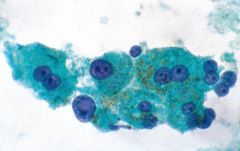
Thyroid FNA
|
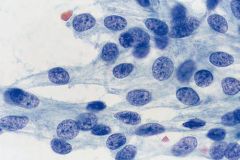
Benign follicular nodule
(meaning either: MNG or FA) • predominantly macrofollicles & colloid • fragmented (flat sheets) • intact spheres • low to moderate cellularity • cohesive cells, uniform, evenly spaced follicular cells • coarse chromatin • Hürthle cells in 50%, macrophages and cyst lining cells |
|
thyroid
|
BFN
|
|
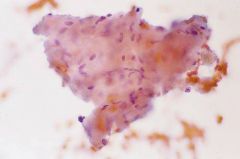
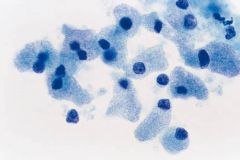
thyroid
|

BFN
ABUNDANT COLLOID (TISSUE PAPER) |
|
|
Follicular carcinoma genetics
|
t(2;3)(q13;p25), which results in a PAX8-PPARγ gene fusion
|
|
When to worry about Hurthle cell neoplasm?
|
NOT here
MNG can have focal hurthle cell change with some atypical features Worry when ALL you see are Hurthle cells, especially isolated forms |
|
95% female preponderance, 40-60y.
|
Hashimoto's thyroiditis (most are HYPOthyroid)
Predominance lymphoid cells NOT monomorphic! Heterogeneous population, tingible body macrophages Scant colloid Hurthle cell change (may get clearing and grooves!) |
|
|
Antibodies in HT?
|
Anti-TPO
Anti-thyroglobulin |
|
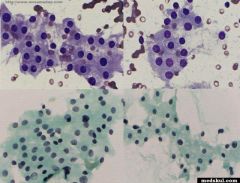
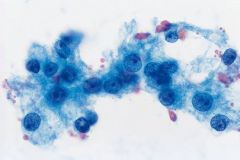
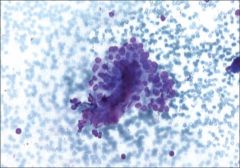
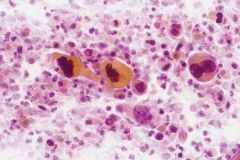
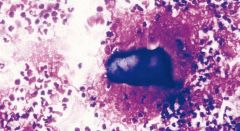
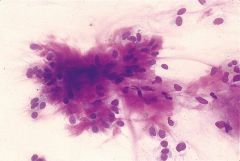
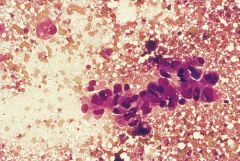
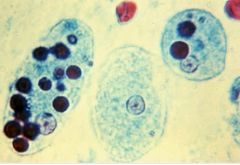
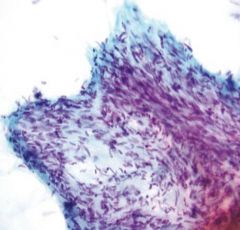
Painful thyroid
|
Subacute (de Quervian) thyroiditis
-Early hypothyroid -Self-limited, last months -Usually viral related ***multinucleated giant cells! Striking. With dense granular cyt (vs foamy in MNG) Lymphs & Rare granulomas (pic) |
|
|
Dry tap of hard thyroid nodule
|
Reidel thyroiditis
Rare Clinically mimics anaplastic ca Dense fibrosis replaces parenchyma and extends beyond; myofibroblasts |
|
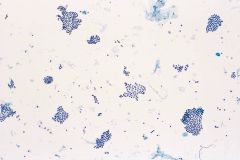
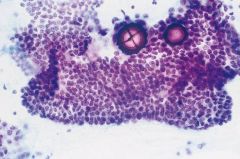
Thyroid FNA
|
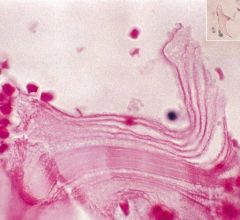
Amyloid goiter
Similar to colloid BUT has fibriblast nuclei within. Dx with Congo red stain. Can be seen in medullary ca |
|
Thyroid FNA. Association?
|
Black thyroid
Tetracycline antibiotics!!!! for acne Brown pigment, darker than heme. STAINS WITH FONTANA MASSON |
|
thyroid FNA
Association? What drugs can cause this? |
Radiation change
(Large cells, large nuc, cyt vacs. maintain N:C) methimazole and carbimazole can cause these changes (used for Graves) |
|

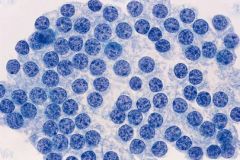
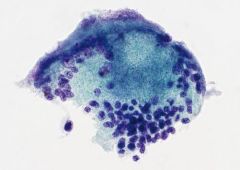
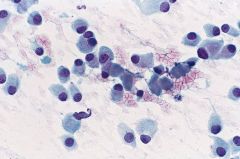
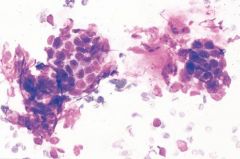
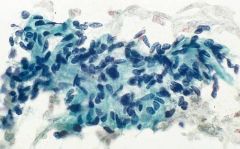
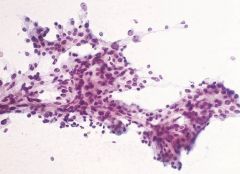
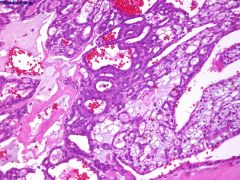
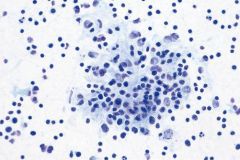
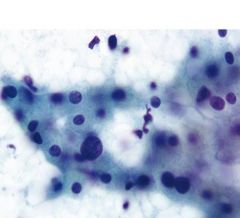
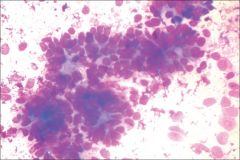
Thyroid FNA
|
Suspicious for follicular neoplasm
30% have follicular carcinoma on excision (Need vascular or capsular invasion!) • marked cellularity predominantly microfollicles or trabeculae (pic) • enlarged, crowded follicular cells • scant colloid |
|
|
great mimickers of follicular carcinoma on FNA
|
Renal cell carcinoma (mimics rare clear cell variant of FC), need hx
Parathyroid adenoma! identical. need TTF1. |
|
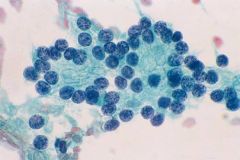
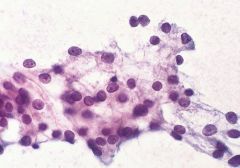
thyroid fna. Clin sig?
|
Suspicious for Hurthle Cell Neoplasm
Meaning either adenoma or carcinoma Generally older patients Use when have a pure Hürthle cell population, dyshesive, ****prominent nucleolus!!! (vs MTC) Can have ***pseudopsammoma bodies 30% hurthle ca have LN mets! (vs rare in follicular ca) |
|
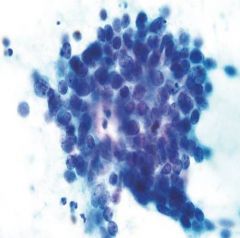
Thyroid FNA
|
RCC! identical to Hurthle cell ca! need hx.
medullary ca (both have dispersed pattern of plasmacytoid cells) but MC does NOT have macronucleoli. also MC has red granules (vs blue HC) and calcitonin+ (vs Thyroglobulin1+) (remember MTC is + for TTF1, - thyroglobulin) |
|
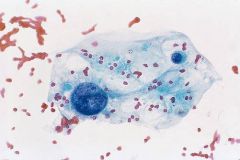
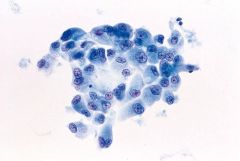
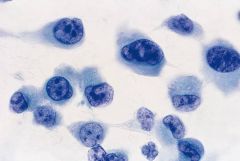
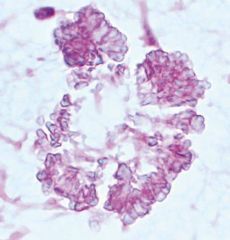
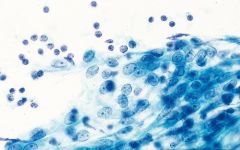
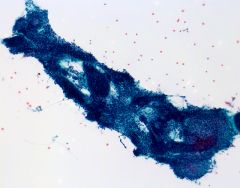
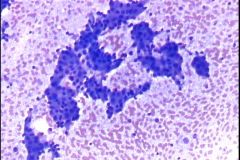
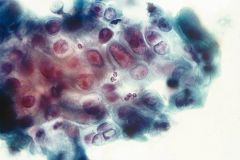
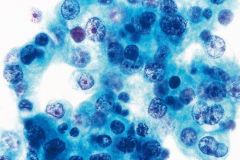
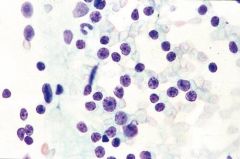
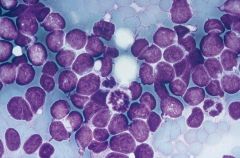
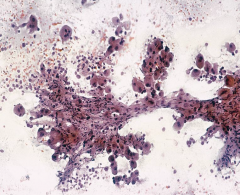
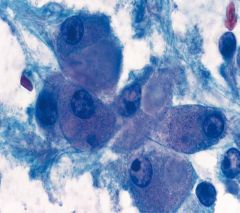
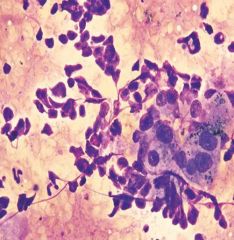
thyroid fna 30F
|
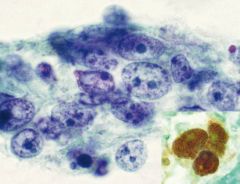
Papillary thyroid ca!
Dx nuclear changes: • “powdery” chromatin • grooves • pseudoinclusions • nucleolus • membrane thickening and irregularity • nuclear crowding or molding psammoma bodies in 50% histiocytes, including multinucleated giant cells (CD68 POSITIVE) |
|
|
genetics of PTC?
|
RET/PTC gene rearrangement chromosome 10
Also point mutations in BRAF and TRK gene |
|
|
Management of PTC? Px?
|
Can be multifocal, so usually thyroidectomy.
Excellent px: >90% 10-yr survival |
|
|
Variants of PTC
|
-Follicular variant, which contains virtually no papillary structures
-Macrofollicular variant -Oncocytic variant -“Warthin-like” PC, with abundant lymphoid infiltrate and strong association with HT -Clear cell variant -Diffuse sclerosing variant, young adults and infiltrates in a diffuse rather than nodular pattern, with abundant squamous metaplasia and numerous psammoma bodies -Tall cell variant, cells are 3x tall:wide -Columnar cell variant, with pseudostratified columnar cells -Solid variant -Cribiform carcinoma, in ADENOMATOUS POLYPOSIS AND GARDNER SYNDROME -PC with fasciitis-like stroma |
|
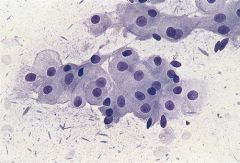
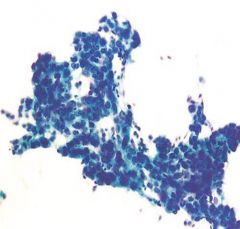
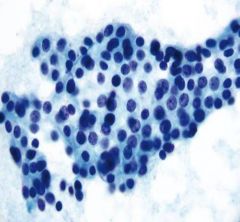
thyroid fna
|
Follicular variant of PTC
Pale chromatin not char of FC |
|
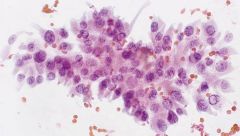
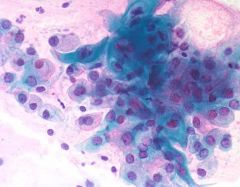
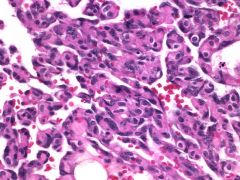
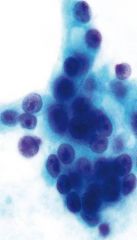
Thyroid fna
|
PTC, oncocytic variant
|
|
thyroid fna
|
tall cell PTC
|
|
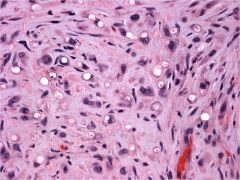
thyroid fna
|
Hyalinizing trabecular tumor
NOW REGARDED AS RARE VARIANT OF PTC has nuclear features of ptc + whorling, parallel array of elongated cells; amorphous hyaline material that is not amyloid; cytoplasmic “yellow bodies”; and perinucleolar clear zone RET/PTC gene |
|
|
Features of poorly differentiated carcinoma
|
ISOLATED CELLS. may have nuclear features of PTC but isolated cells in PTC is rare. Also more pleomorphism. May resemble medullary ca (isolated!) but Thyroglobulin+/calcitonin-.
|
|
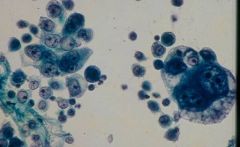
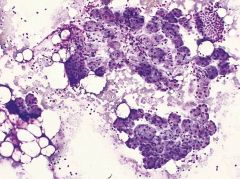
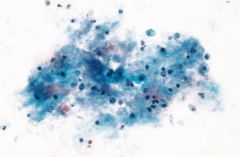
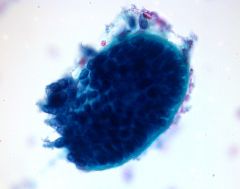
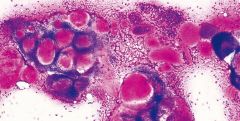
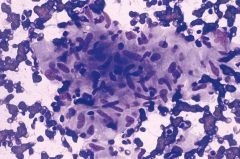
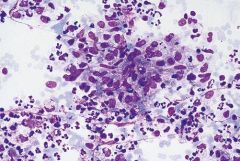
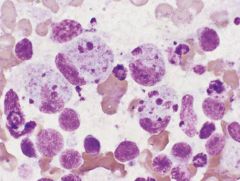
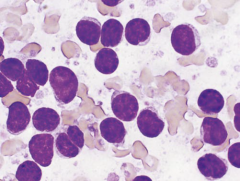
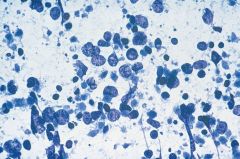
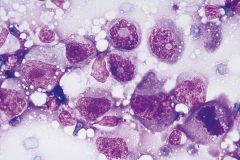
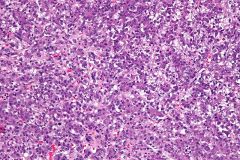
Thyroid FNA 65M
|
Undifferentiated (anaplastic) carcinoma
Accounts for <5% thyroid malignancies but >50% deaths. RAPID GROWTH Mostly isolated cells. Spindled & epithelioid cells with OSTEOCLAST-LIKE GIANT CELLS. Marked nuclear PLEOMORPHISM. Tumor diathesis. 30% have more differentiated thyroid ca. IHC: +cytoker, -TTF1 usually |
|
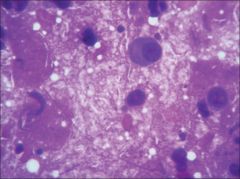
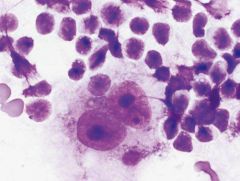
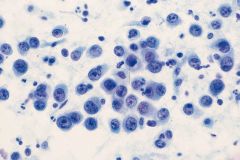
thyroid FNA
|
anaplastic thyroid ca
GIANT CELLS |
|
70M thyroid FNA
px? |
SCC thyroid
Dismal px |
|
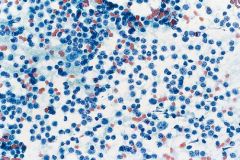
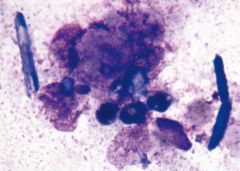
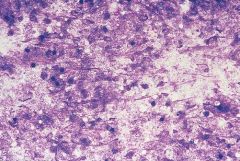
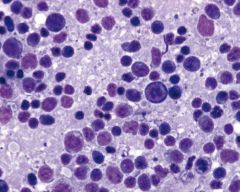
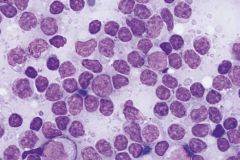
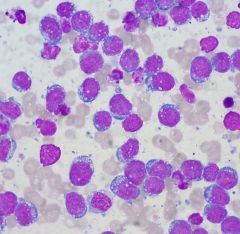
Thyroid FNA
IHC? |
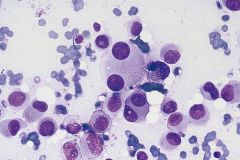
Medullary thyroid carcinoma
From parafollicular C cells 90% sporadic. 50% with LN mets Highly variable. Numerous isolated cells and loose clusters; epithelioid, plasmacytoid, or spindle-shaped cells; salt&pepper chromatin; nuc pseudoinclusions (50%); red cytoplasmic granules (70%) AMYLOID CEA+/CALCITONIN+/TTF1+... Thyroglobulin NEG! |
|
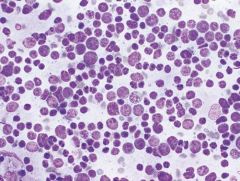
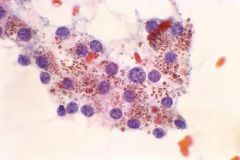
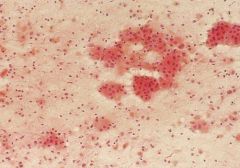
Thyroid FNA
syndromes? |
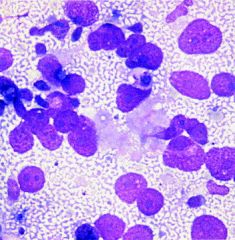
MTC. Characteristic RED cytoplasmic granules on airdry
Get in kids with MEN2 a: SIPPLE: MTC, pheo, PTH adenoma b: MTC, pheo, mucosal neuromas, marfanoid |
|
|
When do you see lymphomas of the thyroid?
What type? |
Associated with Hashimoto, ~20y after dx. Enlarging mass.
3 types: ENMZL, DLBCL, and mixed-type. |
|
Salivary gland. Significance?
|
Tyrosine crystals. No significance. Can be seen in PA, or other tumors.
Amylase crystals (pic) usu seen in inflam Lots of crystals can occur in salivary, none are specific. |
|
|
Types of acinar cells in parotid? submandibular? minor?
|
Parotid: Serous
SM: Serous & Mucinous Minor: Mucinous |
|
Salivary gland
Types of ductal cells? |
Normal salivary gland should have BOTH acini (arrow) and ductal cells (arrowhead). Also should have FAT.
Ductal cells can be: intercalated duct cells (sm cuboidal) oncocytic duct cells collecting duct cells (ciliated) metaplastic (squamy, mucinous) |
|
Salivary gland FNA painful parotid
|
Acute sialadenitis
NEUTROPHILS STONES scant ductal epithelium Usu viral, fungal, bacterial Most often in parotid |
|
Salivary gland FNA painful submandibular mass
|
Chronic sialadenitis
Most often submandibular, from stones or radiation • scant cellularity • small sheets and tubules of basaloid ductal cells with sharp borders • paucity of acinar elements • blood, proteinaceous debris, mature lymphocytes • fragments of fibrous tissue |
|
|
Causes of granulomatous sialadenitis
|
fungi, mycobacteria, toxoplasmosis, and cat scratch
disease, sarcoidosis, cyst rupture, and rarely neoplasia |
|
|
What is sialadenosis?
|
non-neoplastic, noninflammatory enlargement of the salivary gland that more commonly affects the parotid gland and is often bilateral.
Aspirates of sialadenosis appear normal except that the constituent acinar cells are significantly larger than normal acinar cells, and inflammatory cells tend to be absent |
|
salivary gland FNA
|
LESA (lymphoepithelial sialadenitis) aka Mikulicz disease
Usually women, usually parotid. Autoimmue. Cellular aspirate, mixed inflam. Characteristic lymphoepithelial islands (large, cohesive sheets of pale, overlapping, ductal-type cells infiltrated by lymphocytes); often metaplastic ductal cells All pts with Sjogrens have LESA; not all pts with LESA have sjogrens |
|
Salivary gland cyst
|
Benign squamous lined cyst
Congenital cyst (branchial cleft, dermoid) Simple lymphoepithelial cyst (Parotid gland middle age men) HIV associated cystic lymphoepithelial lesion (multiple, bilateral) • cellular aspirate • histiocytes • keratin debris and anucleate squames • small clusters of squamous (or columnar) cells • mixed population of lymphocytes |
|
|
Salivary cyst with lymphoepithelial island?
|
LESA
HIV-associated cystic lymphoepithelial lesion |
|
|
DDx of mucin containing cyst?
|
• mucocele
• retention cyst • chronic sialadenitis with mucinous metaplasia of ducts • mucoepidermoid carcinoma |
|
FNA salivary gland
|
Pleomorphic adenoma
MOST OFTEN PAROTID • epithelial cells • myoepithelial cells • chondromyxoid matrix (best on airdry - MAGENTA!) (green on pap) • tyrosine crystalloids (non-specific) CELLS EMBEDDED IN MATRIX (vs adenoid cystic - cells SURROUND matrix) |
|
|
What should you think about if PA shows marked atypia?
|
Carcinoma ex pleomorphic adenoma
|
|
Salivary gland lesion
IHC? |
Myoepithelioma
basically a monomorphic PA - lacks matrix & epithelial cells IHC for myoeps: p63*, keratin, SMA, GFAP, calponin Uncommon |
|
Salivary gland FNA
|
Basal cell adenoma
Note lack of fibrillar, chondromyxoid stroma seen in PA Can see peripheral palisading and rim of basement membrane-type material PAROTID |
|
|
Specific types of basal cell adenomas to know?
|
canalicular type - upper lip
membranous type - AD syndrome |
|
salivary gland cyst
|
Warthin tumor
PAROTID MEN 50-70y MOTOR OIL fluid lymphocytes, oncocytes, granular debris granular pink cytoplasm on pap; blue on air |
|
saliv gland
|
oncocytoma
rare, benign, parotid, old men oncocytes. Clean background. no lymphs (vs WT) |
|
|
Most common salivary gland malignancy in adults? kids? Major or minor salivary glands?
|
Mucoepidermoid
#1 malignancy in KIDS & ADULTS, MAJOR & MINOR LG usu cystic, HG usu solid & infiltrative Need mucous cells, squamous cells, intermediate cells |
|
salivary gland tumor
|
LG Mucoepidermoid carcinoma
Low grades have more mucinous cells Note the lavender mucin in the background and the bland nuclear features. There are also two populations of cells, one with dense cytoplasm (squamous) and the other with more vacuolated cytoplasm (glandular) |
|
salivary gland tumor
|
HG mucoepidermoid carcinoma
high grades have more squames Get mucicarmine to find mucin |
|
|
DDx high grade carcinomas of the salivary gland
|
HG mucoepidermoid
carcinoma ex PA salivary duct carcinoma oncocytic carcinoma mets (SCC) |
|
44F parotid tumor
|
Acinic cell carcinoma
Loosely cohesive cells, lacking the "grape" appearance of normal acini, and also lacking DUCTAL cells and FAT Usually low grade. usually women, parotid. |
|
Painful submandibular mass
|
Adenoid cystic carcinoma
More common in submandibular Commonly invades NERVES = PAIN Poor long term survival 3D large acellular matrix globules with sharp borders(on airdry)(cant see on pap); BASALOID cells cells SURROUND matrix (vs PA- embedded) SOLID VARIANT INDISTINGUISHABLE FROM BCA |
|
|
What are the 3 types of malignant mixed tumors of the salivary glands?
|
1. Carcinoma ex PA
2. Metastasizing mixed tumor (cytologically benign PA at distant site) 3. Carcinosarcoma (rare) |
|
Rapid enlargement of a longstanding mass
|
Carcinoma ex PA
Usually high grade adenoca of ductal type, but NEED preexisting benign PA. |
|
Elderly man parotid mass
|
Salivary duct carcinoma
Malignant tumor, usually parotid Looks like COMEDO DCIS OF BREAST |
|
Minor salivary gland lesion
px? |
PLGA (polymorphous low grade adenoca)
Occurs exclusively in minor salivary glands UNIFORM NUCLEI! Triad of infiltrative growth, multiple architectural growth patterns, cellular uniformity. Favorable px, despite propensity for perineural invasion |
|
|
How can we diagnose basal cell adenocarcinoma on cytology?
|
Can't. looks like basal cell adenoma. Need histology to identify infiltrative growth.
Usually parotid. Locally recurs. |
|
Parotid mass 62y.o. female
|
Epithelial-Myoepithelial carcinoma
Rare Locally aggressive, low-grade -two cell types: small, inner duct lining cells and larger, peripheral myoepithelial cells -3D clusters cells surrounded by homogeneous ACELLULAR BASEMENT MEMBRANE material **NAKED NUCLEI** Mimics adenoid cystic (acellular material too) |
|
|
Name some other rare salivary gland tumors and pertinent features.
|
Clear cell ca, NOS (dx of exclusion)
Primary small cell carcinoma (dx of exclusion) Lymphoepithelial carcinoma (EBV. Greenland & S China & Intuits. ave age 40y. r/o nasopharyngeal met) |
|
Salivary gland
|
Lymphoma
usually MALT, usually parotid. Arises in background of LESA or Sjogrens. |
|
Lymph node FNA
|
Reactive lymphoid hyperplasia
Mixture of normal elements |
|
Lymph node FNA
|
Sarcoidosis
Non-necrotizing granulomas with epithelioid histiocytes, asteroid bodies, clean background |
|
Matted lymph node in a kid
|
Cat scratch
Bartonella henselae NEUTROPHILS TIGHT GRANULOMAS NECROSIS Cat scratch is most common. BUT these can also look like this: Francisella tularensis Chlamydia trachomatis (LGV) Yersinia enterocolitica |
|
LN
|
Mycobacteria
Negative staining Granulomas, necrosis AFB STAIN |
|
LN kid bilateral painless cervical LAD
Sx? lab findings? IHC? |
Rosai Dorfman disease
Emperipoiesis kids Bilateral painless cervical lymphadenopathy B SYMPTOMS! Lab: POLYCLONAL HYPERGAMMAGLOBULINEMIA LEUKOCYTOSIS histiocytes CD68+, S100+ |
|
|
Characteristics of Langerhans cell histiocytosis
|
S100+, CD1a+
histiocyte nuclei have reniform shapes (unlike RDD - round) and GROOVES No emperipoiesis Eos |
|
young Asian female
sx? lab finding? |
Kikuchi / Histiocytic necrotizing lymphadenitis
Self-limited Asian patients, young, cervical adenopathy, painful, fever LYMPHOCYTOSIS cyto: necrotic debris, karyorrhexis, small histiocytes with angulated nuclei, TBM, NO NEUTROPHILS, |
|
16M tender cervical lymphadenopathy
Complication? |
EBV
h/o pharyngitis Can have splenic rupture Increased immunoblasts, centroblasts, plasmacytoid lymphocytes |
|
|
Clinical features of cHL vs NLP-HL
|
cHL: 95%. Bimodal curve with pk at 15-35y & later in life.
RS cells CD15&30+ NLPHL: Men 30-50. L&H cells (POPCORN CELLS) CD20&45+, EMA50% |
|
|
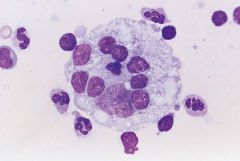
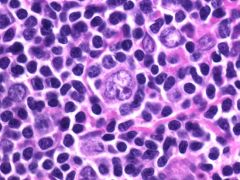
Reed Sternberg cell of classical Hodgkin lymphoma
|
|
|
L&H or POPCORN CELL of NLPHL
**NLPHL is hard to dx on cytology. Flow can help by showing a population of double positive (CD4/8) cells. Helpful but not specific. |
|
|
a. CD5+, CD10−, CD23+
b. CD5+, CD10-, CD23- c. CD5-, CD10+, CD23+-, bcl6+ d. CD5-, CD10-, CD23- |
a. SLL/CLL. dissem at dx. 20% transform (MIB>30%)
b. MCL. dissem at dx. M>>F. t(11;14), cyclinD1. poor px. c. FL. dissem at dx. 30% transform. t(14:18) d. MZL / MALT. indolent. t(11;18). HT, hpylori, sjogren. lymphoepithelial lesions. d. LPL. dissem at dx. monocl IgM. indolent |
|
|
Follicular lymphoma
Clefted nuclei LYMPHOGLANDULAR BODIES |
|
|
LPL vs Waldenstrom
|
IgM > 3 g/dL in Waldenstrom
Potential complications from hyperviscosity |
|
|
Marginal zone lymphoma
Only one that does not have homogeneous population. Has mixture of small lymphs, centrocytes, and monocytoid B cells |
|
|
Small cell carcinoma
MIMIC OF LYMPHOMA **MOLDING, necrosis, paranuclear blue bodies |
|
|
DLBCL
background has T cells |
|
Types?
Genetics? |
Burkitt Lymphoma
1. Endemic form in Africa & Asia (EBV!!) 2. Sporadic form in US 3. Immunodeficiency form cmyc protooncogene chrom 8 t (8;14): 80% t (2;8): 15% t (8;22): 5% |
|
Features?
IHC? |
Burkitt lymphoma.
Smears are monotonously hypercellular TBM mimic starry sky Apoptosis & dirty background Vacuolated cytoplasm CD19+/20+/10+ |
|
|
Flow cytometry clues to T cell lymphoma
|
loss of CD2,3,5,7
loss both CD4, CD8 Coexpression CD4, CD8 (also in NLPHL) |
|
|
Anaplastic large cell lymphoma
HALLMARK CELL (horseshoe shaped nucleus) Donut shapes Necrosis EBV negative EMA+, clusterin+ 70% ALK+ better px t(2;5)(p23;q35) |
|
Anterior mediastinal mass in 10M
|
Think lymphoblastic lymphoma; TdT+
|
|
|
Which nonlymphoid tumors can have lymphoglandular bodies?
|
Seminoma
Nasopharyngeal carcinoma |
|
|
PTLD fun facts
|
Usually within 1-year post transplant
EBER+ 80% 4 forms Most commonly involve GI tract Most resolve with reduction of immunosuppression |
|
|
Rare histiocytic and dendritic cell neoplasms
... study these later... |
Histiocytic sarcoma: CD68, CD163
LCH& sarcoma: S-100, CD1a, Birbeck granules Interdigitating dendritic cell sarcoma: S-100 Dendritic cell sarcoma, NOS:S-100, CD1a, no Birbeck granules Follicular dendritic cell sarcoma: CD21, CD23, CD35 |
|
Lymph node
|
Nasopharyngeal carcinoma
mimics lymphoma HAS LYMPHOGLANDULAR BODIES keratin+/cd45- ALL ARE EBV+ |
|
Lymph node
|
Malignant melanoma
the great masquerader <50% have melanin Dispersed isolated cells Eccentric nuclei DMINS! (Double mirror image nuclei!!) NO lymphoglandular bodies |
|
lymph node
|
Metastatic seminoma
TIGROID BACKGROUND Dispersed large cells Macronucleolus voluminous cytoplasm peripheral vacuoles with blister like quality granulomas LYMPHS AND LYMPHOGLANDULAR BODIES |
|
|
Sarcomas that can met to LN
|
• synovial sarcoma (most common. (pic)bland ovoid nuc with fine chrom, smooth contours)
• epithelioid sarcoma • angiosarcoma • rhabdomyosarcoma • Kaposi sarcoma (CD31,CD34+) • follicular dendritic cell sarcoma (rare. young adults. CD21/23/35+; CD45-) |
|
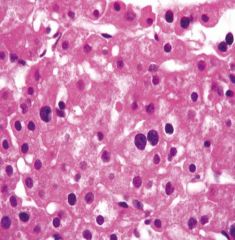
FNA liver
|
normal hepatocytes
• large polygonal cells • isolated cells, thin ribbons (trabeculae), or tissue fragments • centrally placed, round to oval, and variably sized nucleus • commonly binucleated • prominent nucleolus • intranuclear pseudoinclusions • abundant granular cytoplasm • Lipofuscin pigment |
|
|
Liver pigments
|
Lipofuscin: common. aging. Golden on pap/ brown air
heme: dark brown / blue on air bile: cholestasis. dark green both. |
|
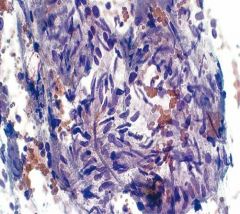
liver FNA
|
Amebic abscess of the liver
Rare in US. Entamoeba histolytica • “anchovy paste” (necrotic debris) • little if any acute inflammation • amebic trophozoites resemble histiocytes: • round nucleus • peripheral chromatin margination • abundant ovoid cytoplasm containing ingested red blood cells |
|
liver cyst
|
Hydatid cyst
Echinococcus / dog tapeworm Fragments of laminated membrane, scolices, hooklets |
|

30F
|
focal nodular hyperplasia
central scar looks nl on FNA |
|
25F on OCPs with abdominal pain
|
Liver cell adenoma
may rupture through capsule LACK portal triads |
|
|
von Meyenberg complex
|
bile duct hamartoma - multiple small nodules of haphazard bile ducts
(bile duct adenoma - solitary subcapsular nodule <1cm) |
|
Liver mass
|
hemangioma.
#1 benign tumor of liver blood, hepatocytes, bland spindle cells |
|
features?
IHC? |
Angiomyolipoma
vessels, fat, smooth muscle. rare in liver 50% of AMLs in liver have EMH! (not in kidney) HMB45+ Can rupture DDx: HCC (has prom cell border), myelolipoma (lacks myoid cells) |
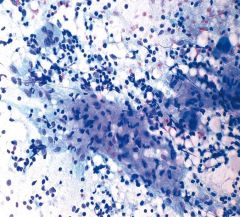
|
|
HCC
highly cellular. isolated cells or cords/nests/sheets. ENDOTHELIAL WRAPPING increased N:C BILE Large round nucleus with prom nucleolus INCIs Naked nuclei |
|

|
HCC
resemble normal hepatocytes but increased N:C numerous naked nuclei |
|
|
Special stains for HCC
|
Mucin (negative)
polyclonal CEA (highlights bile ducts)(vs adeno-diffuse) BCA-225 neg MOC31 HepPar1 CAM5.2, CK8, CK18 (vs cholangioca is neg) TTF1+! (-)CK7, CK19, CK20 |
|
liver mass
|
Fibrolamellar HCC
Young patients Good px No cirrhosis Very large hepatocytes hyaline globules Dense fibrosis around tumor cells |
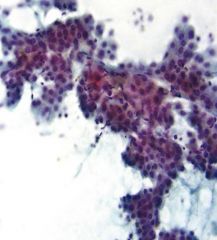
|
liver mass
|
Cholangiocarcinoma
looks like adeno... looks like a met crowded sheets & clusters Irregular arrangement ACINAR STRUCTURES Irregular nuc membranes |
|
liver mass
|
Angiosarc of liver
rare assoc with cirrhosis exposure to POLYVINYL CHLORIDE THOROTRAST well-diff to poorly-diff Massive bleeding with FNA very atypical CD31+/CD34+ |
|
liver mass
|
epithelioid hemangioendothelioma
rare less aggressive than angiosarc |
|

liver mass
|
Metastatic colon ca
picket fence dirty necrotic background pronounced hyperchromasia |
|
liver mass
|
Metastatic prostate
acini prominent nucleoli |
|
liver mass
|
Metastatic GIST
|
|
liver mass
|
Metastatic carcinoid
Loose clusters Hyperchromatic salt and pepper chromatin |
|
liver mass
|
metastatic small cell
Small blue cells scant cytoplasm Molding benign hepatocytes high N:C Granular chromatin |
|
2y.o. liver mass
|
hepatoblastoma
#1 liver neoplasm in kids <3y cells range from poorly diff to adult hepatocytes endothelial cells surround abnormal trabecular cords > 3 cell layers thick Mits EMH! |
|
|
Multiple bilateral parotid cysts?
|
Lymphoepithelial cysts in HIV+ patients
|
|
|
most specific feature papillary thyroid cancer?
|
INCI!
|