Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
71 Cards in this Set
- Front
- Back
|
Alpha Adrenergic Antagonist Agents
|
Reduce peripheral vascular tone -> dilates arterioles and veins & decreases BP
Risk of orthostatic Hypotension |
|
|
ACE Inhibitors
|
Decrease BP and afterload by suppressing the enzyme that converts angiotensin I to angiotensin II
Indications - hypertension, CHF Orthostatic hypotension |
|
|
Angiotensin II Receptor Antagonist Agents
|
Block angiotension II receptors which limit vasoconstriction
Indications - Hypertension, CHF Side effects - dizziness, back and leg pain, angina pectoris |
|
|
Antiarrhythmic Agents
|
Class I - Sodium channel blockers - control cardiac excitation and conduction
Class II - Beta blockers - inhibit sympathetic activity by blocking bega adrenergic receptors Class III - Prolong repolarization by inhibiting both K and Na+ channels and are often considered the most effective antiarrhytmic agent Class IV - Calcium channel blockers - depress depolarization and slow conduction through AV node |
|
|
ECG
|
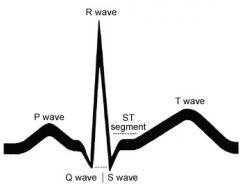
P wave - atrial depolarization
PR interval - time for atrial depolarization and conduction from SA to AV node (.12-.2") QRS complex - depolarization of ventricles It should be between 0.06-0.10 seconds QT interval - time for both ventricular depolarization and repolarization (.2-.4") ST segment - isoelectric period following QRS when the ventricles are depolarized T wave - ventricular re-polarization |
|
|
Cardiac conduction
|
SA node -> AV node -> Bundle of his -> R/L bundle branches -> Purkinje fibers
|
|
|
Anticoagulant Agents
|
Inhibit platelet aggregation and thrombus formation.
Side effects -hemorrhage, GI distress, increased risk of bleeding Examples - Heparin, Coumadin (warfarin), Lovenox (enoxaparin) |
|
|
Antihyperlipidemia Agentsh
|
5 categories
Most common - statins - inhibit enzyme action in cholesterol synthesis, break down LDL, decrease triglyceride levels, increase HDL levels. Examples - Lipitor, Zocor, Tricor Side effects - headache, GI distress, myalgia, rash Exercise can maximize the effects of drug therapy |
|
|
Antithrombic (Antiplatelet) Agents
|
inhibit platelet aggregation and clot formation
Examples - Bayer (aspirin), Plavix, Persantine T |
|
|
Thrombocytopenia
|
Decreased platelet count
A normal human platelet count ranges from 150,000 to 450,000 platelets per microlitre of blood |
|
|
Beta Blockers
(Beta-Adrenergic Blocking Agents) (LOL!) |
Decrease myocardial oxygen demand by decreasing HR and contractility via blocking B-adrenergic receptors
Indications - Hypertension, angina, arrhythmias, heart failure, migranes, essential tremor Side effects - bradycardia, arrhythmias, fatigue, depression, dizziness, weakness, blurred vision Implications for PT - HR and BP response to exercise will be diminished. RPE may be used to monitor exercise intensity. Closely monitor patients during positional changes due to an increased risk for othostatic hypotension. Examples - Tenormin (adenolol), Lopressor (metoprolol), Inderal (propanolol) - LOL |
|
|
Calcium Channel Blockers
|
Decrease entry of calcium into vascular smooth muscle cells resulting in diminished myocardial contraction, vasodilation, and decreased oxygen demand of the heart
Indications - hypertension, angina pectoris, ahhrythmias, CHF Side effects - dizziness, headache, hypotension, peripheral edema Examples - Norvasc, Procardia, Calan, Cardizem |
|
|
Diuretic Agents
|
Increase excretion of sodium and urine. This reduces plasma volume which decreases BP.
Classifications include thiazide (Diuril), loop(lasix), and K+ sparing agents (dyrenium Indications - hypetension, edema associated with heart failure, pulmonary edema, glaucoma Side effects - dehydration, hypotension, electrolye imbalance, polyuria, increased LDL, arrhythmias |
|
|
Nitrate Agents
|
Decrease ischemia through smooth muscle relaxation and dilation of peripheral vessels
Indications - angina pectoris Examples - nitrostat (Nitroglycerin), isordil (isosorbide dinitrate), Amyl nitritite solution for inhalation |
|
|
Positive Inotropic Agents
|
Increase force and velocity of contraction, slow HR, decrease conduction velocity through AV node, decrease degree of activation of sympathetic nervous system
|
|
|
Thrombolytic Agents
|
Clot dissoultion through conversion of plasminogen to plasmin (breaks down clots and allows occluded vessels to reopen)
Indications - Acute MI, PE, ischemic stroke, arterial or venous thrombosis Ex - Linlytic (urokinase), Activase (alteplase) |
|
|
Antihistamine Agents
|
Block effects of histamine to dec nasal congestion, mucosal irritation, and smptoms of the common cold, sinusitis, conjunctivitis, and allergies
Indications - allergies, cold, motion sickness, Parkinson'sl |
|
|
Anti-inflammatory Agents
|
Indications - brochospasm, asthma
Inhaled corticosteriods, leukotriene modifiers, and mast-cell stabilizers help prevent inflammatory-mediated bronchoconstriction by inhibititing production of inflammatory cells, suppressing release of inflammatory mediators (cytokines, prostaglandins, leukotrienes), and reversing capillary permeability, in turn reducing airway edema Side effects - Corticosteriod: osteoporosis, glucoma, delayed growth; Leukotriene modifier - Liver dysfunction; mast-cell stabilizer-bronchospasm, throat and nasal irritation, cough, GI distress Implications for PT- pt ed to rinse mouth after inhalation, these are not bronchodilators and are not for acute episodes of asthma |
|
|
Bronchodilators
|
Releive bronchospasm
Albuterol |
|
|
Expectorants
|
Increase respiratory secrections which helps loosen mucous. Reduces the viscosity of secreations which improve efficiency of the cough reflex and ciliary action in removing it
PT implication - perform airway clearance techniques one hour after drug administration. Take w glass of water Mucinex (guaifenesin) |
|
|
Mucolytic Agents
|
Decrease viscosity of mucous secretions by altering their composition and consistency, making them easier to expectorate
Given w nebulizer pneumonya, emphysema, chronic bronchitis, cystic fibrosis Perform airway clearance one hour after administration |
|
|
Korotkoff sounds
|
During blood pressure assessment
Phase I - first appearance of clear tapping sounds corresponds to appearance of a palpable pulse (SYSTOLIC BP) Phase II - sounds become softer and longer Phase III - sounds become crisper and louder Phase IV - sounds become muffled and softer Phase V - sounds disappear completely (DIASTOLIC BP) |
|
|
Auscultation of heart souunds - locations
|
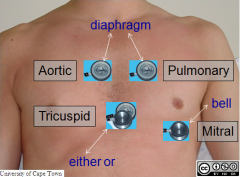
Aortic area - 2nd intercostal space at right sternal border
Pulmonic area - 2nd intercostal space at L sternal border Mitral area - 5th intercostal space, medial to left midclavicular line Tricuspid area - 4th intercostal spaceat the left sternal border |
|
|
Auscultation of heart sounds - interpretation
|
S1 (lub)
- close of mitral and tricuspid valves at onset of ventricular systole S2 (dub) -closure of aortic and pulmonary semilunar valves at onset of ventricular diasole S3 -abnormal in adults -vibrations of distended ventricle walls due to passive flow of blood from the atria during filling phase of diastole S4 - pathological sound of vibration of the ventricular wall when atria contracts and ventricle fills |
|
|
Normal breath sounds
|
Tracheal and broncheal sounds - loud, tubular sounds normally heard over the trachea
Vesicular breath sounds - high pitched, breezy sounds heard over distal airways |
|
|
Abnormal breath sounds
|
Crackle (rales) - movement of fluids or secretions during inspiration (wet crackles), or from sudden opening of closed airways (dry crackles)
- atelectasis, fibrosis, pulmonary edema, or pleural effusion Pleural friction rub Ronchi - "snoring/gurgling" Stridor - continuous high pitched wheeze, indicating upper airway obstruction Wheeze - "musical" whistling sound of variety of pitches |
|
|
Voice sounds
|
Transmission of sounds in normal lung is usually muffled. Consolidation, atelectasis, or fibrosis improve transmission of vibrations through lung tissue.
Bronchophony - increased vocal resonance with spoken words Egophony - long "E" sounds like nasally long "A" Whispered pectoriloquy - Recognition of whispered words |
|
|
Indications for terminating an exercise stress test
|
Absolute:
- 3/4 angina pain - Increasing nervous system symptoms (ataxia, dizziness) - Signs of poor perfusion (cyanosis, pallor) - Sustained ventricular tachycardia - 1.0mm ST segment elevation in leads without diagnostic Q waves Relative: - Drop in SBP >10 mm HG despite increased workload without evidence of ischemia - >2 mm ST segment depression - Arrhythmias other than sustained ventricular tachycardia including multifocal PVCs, supraventricular tachycardia, heart block or bradyarrhyhmias - Fatigue, SOB, wheezing, leg cramps, and claudication - Development of bundle branch block or intraventricular conduction delay - Increasing chest pain - Hypertensive response (SBP>250 or DBP >115) |
|
|
Heart rate norm
|
Infant - 100-130
Child - 80-100 Adult - 60-100 Bradycardia <60 Tachycardia >100 |
|
|
Volume/amplitude of pulse
|
3+ large or bouding
2+ normal or average 1+ small or reduced 0 absence |
|
|
Percussion sounds
|
Flat or dull - sounds like thigh percussion; in upper lung, suggests neoplasm, atelectasis, or consolidation of the lung
Resonance - normal Hyperressonance - intermiediate between resonance and tympany; emphysema or pneumothorax Tympany - hollow sound vaguely resembling drum beat; occurs almost exclusively with large pneumothorax |
|
|
MET Values for common physical activities
|
Light (<3) - walking around, toileting, driving, deskwork, dishes, making bed, bathing, cooking, playing instrument, fishing
Moderate (3-6) - walking 3 mph (3-4 met), walking 4 mph (4.5-7 met), washing windows or car, sweeping, vacuuming, light gardening, carrying/stacking wood, power lawn mowing, slow dancing (3.0), table tennis, fast dancing (4.5), basketball shooting, sex, golf, swimming, tennis doubles, cycling flat 10-12 mph (6) Vigorous (>6 MET) - walking 4.5 mph (6.3), Jogging = 8, Running 7 MPH (11.5), shoveling (7), carrying heavy loads (7.5), heavy farmwork (8), digging ditches (9.5), backpacking (5-11), basketball game (8), cycling 12-14 mph (8), cycling 14-16 mph (10.0) |
|
|
MET
|
Metabolic equivalent
1 MET - energy expended while sitting quietly |
|
|
Target Heart Rate
% of max HR |
Lower THR = HR max x 55%
Upper THR = HR max x 90% Method 2: Heart rate reserve (HRR) or Karvonen formula Lower THR = [(HRmax-HRrest)x40%] +HR rest |
|
|
Heart rate reserve (HRR) or Karvonen formula
|
Lower THR = [(HRmax-HRrest)x40%] +HR rest
Lower THR = [(HRmax-HRrest)x85%] +HR rest |
|
|
Cardiorespiratory response to exercise
|
- Increased O2 consumption due to increased cardiac output, increased blood flow, and oxygen utilization in the exercising skeletal muscles
- Linear increase in SBP with increasing workload (8-12 mm Hg per MET - No change or moderate change in DBP - Increased respiratory and tidal volume |
|
|
Chronic Adaptations to aerobic exercise
|
- VO2 max - increased at maximal exercise
- HR: no change or decrease at maximal exercise; decreased at submaximal exercise - Arterovenous oxygen difference - increased at maximal exercise; no change at submaximal exercise - SBP and DBP - no change or slight increase at maximal exercise; no change or slight decrease at submaximal exercise - Blood lactate - increased at maximal exercise; decreased at submaximal exercise - Oxidative capacity of muscle - increased mitochondrial number and size, capillary density, and oxidative enzymes - Maximal voluntary ventilation - increased at maximal exercise - Plasma volume - increased - Skeletal muscle blood flow - increased at maximal exercise, no change at submaximal exercise - Reduced body mass and body fat and increase in fat free body mass - Improve body heat transfer due to larger plasma volume and more responsive thermoregulatory mechanisms - Psychological benefits - reduced anxiety, stress, and depression; improved mood and self-esteem |
|
|
Apnea
|
absence of spontaneous breathing
|
|
|
Biot's
|
irregular breathing; varied depth and rate with periods of apnea; often associated with increased intracranial pressure or damage to the medulla
|
|
|
Bradypnea
|
slower than normal respiratory rate
<12 breaths per min in adults May be associated with neurologic or electrolyte disturbance, infection, or high level of cardiovascular fitness |
|
|
Cheyne-Stokes (periodic)
|
decreasing rate and depth of breathing with periods of apnea; can occur due to CNS damage
|
|
|
Eupnea
|
normal breathing
|
|
|
Hyperpnea
|
Increased rate and depth of breathing
|
|
|
Hypopnea
|
decreased rate and depth of breathing
|
|
|
Kussmaul's breathing
|
deep and fast breathing; often associated with metabolic acidosis
|
|
|
Paradoxical breathing
|
chest wall moves with inhalation and out with exhalation; due to chest trauma or paralysis of the diaphragm
|
|
|
Tachypnea
|
Faster than normal respiratory rate; >20 breaths per min in adults
|
|
|
Waist circumference
|
- Measured at level of iliac crest during normal exhalation
- Increased risk for type 2 diabetes, dyslipidemia, hypertension, and cardiovascular disease is associated with a circumference >102 CM (>40"), for men and >88 cm (>35") for women |
|
|
Obstructive vs Restrictive ventilatory impairment
|
Obstructive - decreased expiratory flows
FEV1/FVC <70% asthma, emphysema, chronic bronchitis Restrictive - reduced lung volumes and normal expiratory flow rates Inferred from spirometry when FVC is reduced and FEV1/FVC is normal or less than 80% |
|
|
When to cease exercise based on SpO2
|
<90% in acutely ill patients
<85% in patients with chronic lung disease |
|
|
Rate Pressure Product
|
AKA "double product"
Index of myocardial oxygen consumption and coronary blood flow Provides an easy to measure physiologic correlate to onset of angina pectoris or ECG abnormalities Measure SBP and HR during same exercise workload RPP = HR x SBP Usually reported as a 2 digit number (ex 22.5 x 10^3) |
|
|
RPE
|
Rate of perceived exertion
Regular scale - 6-20 Revised - 0-10 RPE of 13-14 represents about 70% max HR Early cardiac rehab - 11-13 = upper limit |
|
|
Normal Respiratory Rates
|
Newborn - 33-45 breaths/min
1 year - 25-35 breaths/min 10 years - 15-20 Adult - 12-20 |
|
|
Respiratory Rhythm
|
Normal - Inspiration is half as long as expiration (I:E = 1:2)
COPD - expiration much longer (1:3 or 1:4) |
|
|
Positions to relieve dyspnea
|
Reverse trendelenberg - decreased weight of abdominal contents on the diaphragm
Semi - Fowler's - Supine with HOB elevated to 45 degrees and pillows under the knees |
|
|
Premature atrial contractions
|
- Occur when ectopic focus in atrium initiates an impulse before the SA node
- P wave is premature with abnormal configuration - PACs are very common and generally benign, but may progress to atrial flutter, tachycardia, of fibrillation - May occur with a normal heart (from caffeine, stress, smoking, alcohol) and any type of heart disease |
|
|
Atrial flutter
|
- An ectopic, very rapid atrial tachycardia
- Atrial rate of 250-350 beats per minute; ventricular rate dependent upon AV node conduction - Saw-tooth shaped P waves (also known as atrial flutter waves) - Occurs with valvular disease (especially mitral), ischemic heart disease, cardiomyopathy, hypertension, acute MI, COPD, and pulmonary emboli - s/s include palpitations, lightheadedness, and angina due to rapid rate - Stagnation of blood may predispose to thrombi in area |
|
|
Atrial fibrillation
|
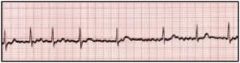
- Common arrhythmia where the atria are depolarized between 350 and 600 x/min
- ECG shows characteristically irregular undulations of ECG baseline without discrete P waves - Occurs in healthy hearts and in patients with coronary artery disease, hypertension, and valvular disease - Symptoms may include palpitations, fatigue, dyspnea, lightheadedness, syncope, and chest pain - Stagnation of blood may predispose to thrombi in the atria |
|
|
1st degree AV block
|
- PR interval longer than .2 seconds, but relatively constant from beat to beat
- No symptoms or significant change in cardiac function - PR interval may become prolonged for many reasons including medications that suppress AV conduction |
|
|
2nd degree AV block
|
- AV conduction disturbance in which impulses between the atria and ventricles fail intermittently
-Two major types: Mobitz Type I (Wenckebach)- progressive prolongation of PR interval until one impulse is not conducted (generally benign) Mobitz Type II - consecutive PR intervals are the same and normal followed by nonconduction of one or more impulses (a more serious condition). If heart rate is slow, CO will decrease with the blocked impulse. Also, 2nd degree AV block may progress to 3rd degree AV block |
|
|
3rd degree AV block (complete heart block)
|
- All impulses are blocked at the AV node and none are transmitted to the ventricles
- The atria and ventricles are paced independently; atrial rate >ventricular rate - Considered a medical emergency required a pacemaker - If the ventricular rate is too slow, the CO drops and the patient may faint - Common causes include degenerative change of the conduction systems, digitalis, heart surgery, and acute MI |
|
|
Premature Ventricular complex (PVC)
|
- Premature depolarization arising in the ventricles due to an ectopic focus
- Unfocal PVCs arise from same ectopic focus and have the same configuration - Multifocal PVCs arise from different ectopic foci and have different configurations - On ECG, the P wave is usually absent and the QRS complex has a wide and aberrant shape BIGEMINY - Normal sinus impluse followed by PVC TRIGEMINY - PVC occurs after every two normal sinus impulses Clinical significance: - A common arrhythmia that occurs in healthy and diseased hearts - Patient may be asymptomatic or have palpitations - Common causes include anxiety, caffeine, stress, smoking, and all forms of heart disease |
|
|
Ventricular tachycardia (v-tach)
|
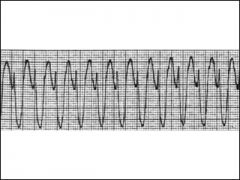
- 3 or move consecutive PVCs at a ventricular rate of >150 BPM
- P waves are absent and QRS complexes are wide and abberrant in appearance - V-tach longer than 30 seconds is a life-threatening arrhythmia and requires immediate medical intervention - Patients are not able to maintain an adequate blood pressure and eventually become hypotensive - V-tach may degenerate into ventricular fibrillation causing cardiac arrest - Common causes include: MI, cardiomyopathy, and valvular disease |
|
|
Ventricular fibrillation (v-fib)
|
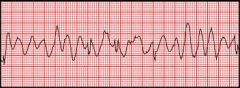
- Ventricles do not beat in a coordinated fashion, but fibrillate or quiver asynchronously and ineffectively
- No CO, patient becomes unconscious - ECG shows characteristic fibrillation waves with an irregular pattern that is either coarse or fine - A lethal tachyarrhythmie requires immediate defibrillation - Additional measures include medications to support the circulation and IV antiarrhythmic agents - Common causes include heart disease of any time, MI, and cocaine use |
|
|
Ventricular asystole
|
-Ventricular standstill with no rhythm
- ECG records straight line pattern - Requires immediate defibrillation and or meds to stimulate cardiac activity - Common causes include acute MI, ventricular rupture, cocaine use, lightning strikes, and electrical shock |
|
|
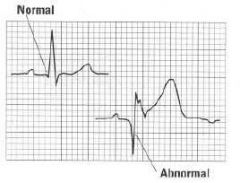
Signs of Myocardial Ischemia/Infarction
|
ST Segment Depression
ST Segment Elevation Q wave T wave inversion |
|
|
ST Segment depression
|
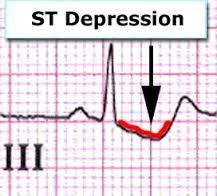
- A depressed ST segment is a sign of subendocardial ischemia, but also can be due to digitalis toxicity or hypokalemia
- The segment is evaluated relative to isoelectric baseline at 0.08 seconds after the J point - Deviations from isoelectric baseline are expressed as ST segment depression of 1mm, 2mm, etc |
|
|
J point
|
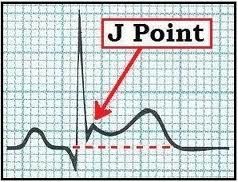
junction bewteen end of QRS complex and beginning of ST segment
|
|
|
ST segment elevation
|
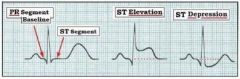
- Earliest sign of acute transmural infarction
- Can also indicate a benign early repolarization pattern in a normal heart - Deviations from isoelectric baseline are expressed as ST segment elevation of 1mm, 2mm, etc |
|
|
Q wave
|
- A characteristic marker of infarction
- Signifies the loss of positive electrical voltages due to necrosis - A significant or abnormal Q wave is longer than 0.04 msec and larger than 1/3 the amplitude of the R wave |
|
|
T wave inversion
|
- Occurs hours or days after an MI as the result of a delay in repolarization produced by the injury
- May also occur with R and L bundle branch blocks, after a CVA, and as a normal juvenile T wave pattern in children and some adults |