Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
305 Cards in this Set
- Front
- Back
|
Which area of the spine has the least motion and the most motion?
|
Cervical has most, Thoracic spine has least.
|
|
|
when does the thoracic Primary curve develop?
|
present at birth.
|
|
|
is the thoracic primary curve relatively mobile?
|
no. immobile
|
|
|
What are Two anatomic causes for relative immobility of the thoracic spine?
|
1. intimate connection of the T spine to the rib cage, ribs and sternum, via the costovertebral articulations.
2. ratio of intervertebral disk height to vertebral body height is small(1:5) which greatly reduces intersegmental motion. |
|
|
which two vertebrae are the inferior transition from the cervical lordosis?
|
T1 - T2
|
|
|
which thoracic vertebrae are part of the forward bent kyphosis?
|
T3-T12
|
|
|
where is the apex of the thoracic kyphosis?
|
T5 - T6
|
|
|
|
|
|
Which vertebrae are the transition from the thoracic kyphosis to the lumbar lordosis?
|
T10 - T12
|
|
|
What is the cervical transition area of the spine?
|
OA
|
|
|
Each vertebrae is ossified from ___ primary centers
|
three
|
|
|
During the ____ week, scleotomal cells (mesoderm) migrate medially to surround the spinal cord and notochord.
|
fourth
|
|
|
After proliferation of the caudal portion of the sclerotomes, the vertebrae are formed, each consisting of the _____ (caudal/cephalic) part of one sclerotome and the _____ (caudal/cephalic) part of the next.
|
caudal, then cephalic
|
|
|
The ___ persists in the areas between the vertebral bodies forming the nucleus pulposus. This with the surrounding circular fibers of the annulus fibrosus forms the intervening disk.
|
notochord
|
|
|
Spinal nerve bundles are gathered with formation of the vertebrae to pass out between the ____ ____.
|
intervertebral foramina
|
|
|
Segmentalization via ____.
|
somites
|
|
|
Bones, connective tissue, muscles are derived from ____.
|
mesenchyme
|
|
|
What are the atypical ribs?
|
1,10,11,12
|
|
|
|
|
|
How many transverse process facets are on the atypical ribs 1,10,11,12?
|
0 on 11 and 12. 1 on 1 and 10.
|
|
|
Most common SD for a coronary artery bypass graft IS _____ ribs on the side done. The ribs twists and actually point into the vert body.
|
Inhale the Cabbage, inhaled rib same side.
|
|
|
Intervertebral disc herniation is Not very common in thoracic spine. Its Limited by ____ longitudinal ligament, ribs
|
posterior
|
|
|
Rotatores are often responsible for which type of mechanic?
|
Type II SD’s.
|
|
|
Which type of mechanic is responsible for pain?
|
Type II SD’s.
|
|
|
|
|
|
Trapezius, Latissimus dorsi, Rhomboid minor, Rhomboid major, Levator scapulae - all receive nerve supply from ___ rami of the ____ nerves.
|
anterior, cervical
|
|
|
Trapezius, Latissimus dorsi, Rhomboid minor, Rhomboid major, Levator scapulae - all connect ___ ___ to trunk and work primarily on ____ ____.
|
upper limb
|
|
|
which muscles connect upper limb to trunk and receive nerves from anterior rami of cervical nerve?
|
TRRLL - Trapezius, Rhomboid minor, Rhomboid major, Levator scapula, Latissimus dorsi
|
|
|
Serratus posterior superior & inferior - have mostly ____ function with some minor respiratory function
|
proprioceptive
|
|
|
Muscles of back proper, (intrinsic), from cranium to pelvis, are innervated by what?
|
Innervated by the posterior rami of spinal nerves T2-T12
|
|
|
|
|
|
|
|
|
Muscles of back proper, (intrinsic), from cranium to pelvis, are the cause of what?
|
Responsible for many of the TART changes seen in somatic dysfunction
|
|
|
Muscles of back proper, (intrinsic), from cranium to pelvis, act to do what?
|
maintain posture and control movement of the vert column.
|
|
|
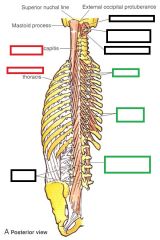
what is the superior attachment of the intrinsic back muscle fascia?
|
At the skull inferior to the superior nuchal line
|
|
|
what are the 2 lateral attachment of the intrinsic back muscle fascia?
|
1. Laterally at cervical and lumbar transverse processes. 2. Laterally at angles of ribs
|
|
|
Thoracolumbar fascia is part of this complex and forms the sheath of the ____ ____ muscle which becomes thinner as it ascends in the thorax.
|
erector spinae
|
|
|
Thoracolumbar fascia envelops the spinal _____.
|
extensors
|
|
|
thoracolumbar fascia In the lumbar region consists of ____ layers.
|
three
|
|
|
thoracolumbar fascia Provides origin for the ____ ____ and some of the abdominal muscles.
|
Latissimus dorsi
|
|
|
thoracolumbar fascia In the cervical region blends laterally with the ____ ____ .
|
prevertebral fascia
|
|
|
thoracolumbar fascia Provides a ____ for separating muscle groups
|
plane
|
|
|
|
|
|
When you Breath in what happens to the diaphragm? AP, transverse, vertical diameters? Abdominal Pressure?
|
Flattens. AP, vertical, transverse diameter increases. Abdominal pressure increases. Reverse on exhalation.
|
|
|
Superior angle of scapula is at the level of which vertebral body?
|
T2
|
|
|
Inferior angle of scapula is at the level of which vertebral body?
|
T7
|
|
|
Jugular notch is at the level of which vertebral body?
|
T2
|
|
|
Sternal angle (manubrosternal joint, aka angle of Louis) is where the ____ costal cartilages attach. It lies at the level of the IV disc between T4 & T5
|
2nd
|
|
|
Sternal angle (manubrosternal joint, aka angle of Louis) is where the 2nd costal cartilages attach. It lies at the level of the IV disc between vert bodies ___ and ___.
|
T4 - T5
|
|
|
spine of scapula at what vert level?
|
T3
|
|
|
inf angle of scapula at what vert level?
|
T7
|
|
|
rotational motion in the thoracic spine is limited by what?
|
multiple ligamentous tensions
|
|
|
SB/lateral motion in the thoracic spine is limited by what?
|
articular processes on the side of movement, contralateral ligamenta flava, intertransverse ligaments, RIBS and STERNUM
|
|
|
|
|
|
flexion motion in the thoracic spine is limited by what?
|
extensor mm., interspinous ligaments, ligamenta flava, posterior longitudinal ligament, RIBS
|
|
|
extension motion in the thoracic spine is limited by what?
|
the impact of the articular processes and the spinous processes (shingle effect)
|
|
|
what muscle(s) handles Backward bending (extension)?
|
Interspinales thoracis
|
|
|
what muscle(s) handles Backward bending (extension) when acting Bilaterally?
|
Intertransversari thoracis, Multifidus, Longissimus thoracis, Iliocostalis thoracis
|
|
|
what muscle(s) handles Backward bending & Rotation (to opposite side)?
|
Semispinalis thoracis, Rotatores thoracis
|
|
|
what muscle(s) handles Sidebending (lateral flexion)?
|
Longissimus thoracis, Intertransversari thoracis, Iliocostalis thoracis
|
|
|
what muscle(s) handles Sidebending and Rotation (to opposite side)?
|
Multifidus
|
|
|
|
|
|
what muscle(s) handles Flexion?
|
abdominal muscles
|
|
|
When sidebending is introduced into a neutral spine, the bodies of the vertebra will rotate towards the side of _____.
|
convexity. Fryette's 1st.
|
|
|
When sidebending is introduced into a non-neutral spine, the bodies of the vertebrae will rotate toward the side of ____.
|
concavity. Fryette's 2nd.
|
|
|
|
|
|
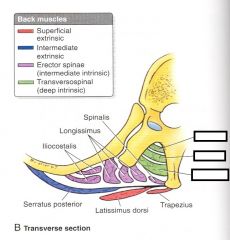
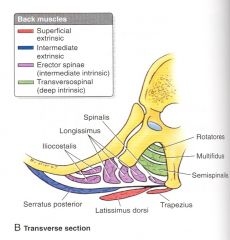
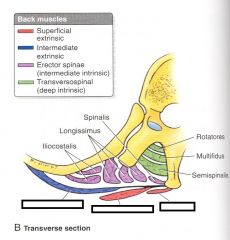
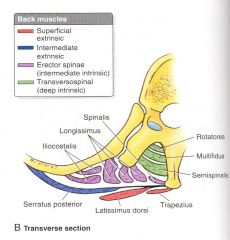
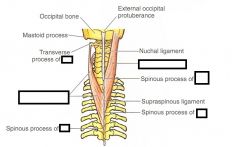
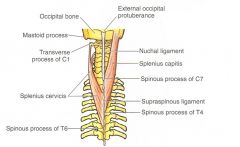
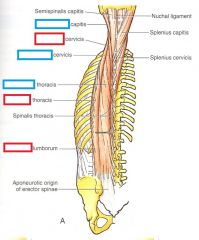
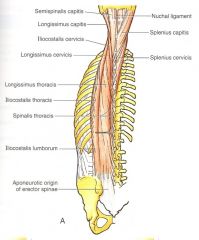
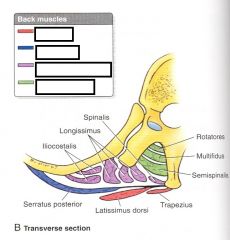
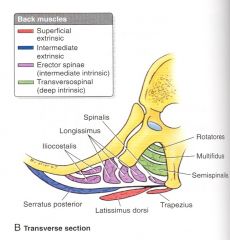
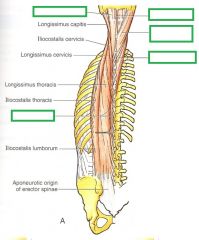
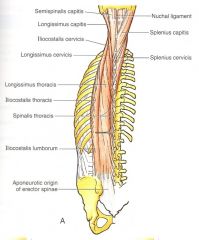
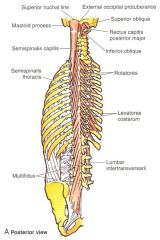
What are two superficial intrinsic muscles of the back?
|
Splenius cervicis and capitis
|
|
|
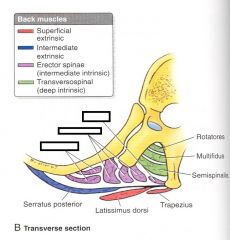
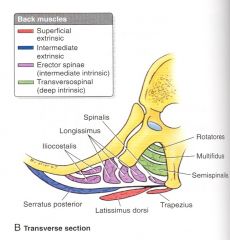
intermediate intrinsics are what muscles?
|
Erector spinae - These lie in a ‘groove’ on each side of the vertebral column (between spinous processes and rib angles). 1. illiocostalis. 2. Longissiumus. 3. Spinalis
|
|
|
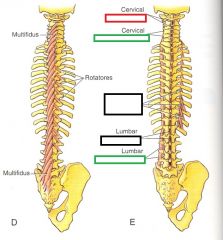
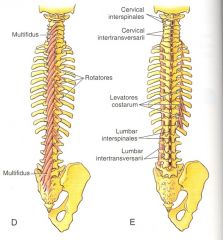
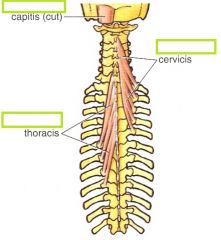
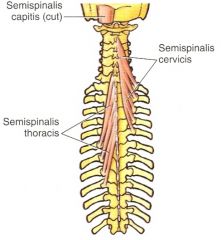
Semispinalis superficial,spans __ to __ segments
|
4 to 6
|
|
|
what muscle has a span of 4-6 segments?
|
Semispinalis
|
|
|
Multifidus mid depth, spanS ___ to ___ segments
|
2 to 4
|
|
|
what muscle has a span of 2-4 segments?
|
Multifidus
|
|
|
|
|
|
Rotatores deepest, spans __ to __ segments
|
1 to 2
|
|
|
what muscle has a span of 1 to 2 segments?
|
Rotatores
|
|
|
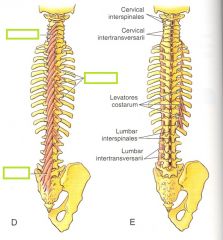
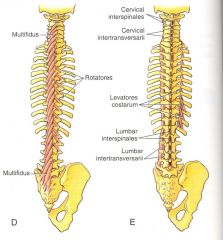
which muscle group spans from the transverse processes of vertebrae to spinous processes of one or more superior vertebrae.
|
Deep intrinsics
|
|
|
Deep intrinsics span from the ___ processes of vertebrae to ____ processes of one or more superior vertebrae.
|
transverse , spinous
|
|
|
|
|
|
____ are the best developed in the thoracic region.
|
Rotatores
|
|
|
Rotatores are the best developed in the ____ region.
|
thoracic
|
|
|
Smaller or larger muscles have lower density of muscle spindles - sensors of proprioception?
|
larger
|
|
|
It is proposed that these (larger or smaller) muscles maintain somatic dysfunction, especially non-neutral somatic dysfunction, most often occuring in single segments.
|
smaller
|
|
|
Celiac ganglion anteriorly receives innervation from what nerves?
|
T5-T9
|
|
|
Superior mesenteric ganglgion get which nerves?
|
T10-T11
|
|
|
There is a problem at T10, which ganglion is affected?
|
Superior mesenteric
|
|
|
T12-L2 is associated with what ganglion?
|
Inferior mesenteric ganglion
|
|
|
The sympathetic chain ganglia lie ___ and ___ to the vertebral bodies of their corresponding levels, attached to the associated spinal nerve by the white and grey rami communicantes. This is also directly anterior to the corresponding rib head and it’s associated fascia.
|
anterior and lateral
|
|
|
The majority of outflow of the sympathetic system originates in the _____ region. Distribution of the sympathetic system to almost every tissue and area of the body makes this a very important one for all body functions. (Esp immune function). Disturbances of the thoracic vertebrae and their associated musculature that affect the function of the sympathetic system can have widespread consequences.
|
thoracic
|
|
|
sympathetic autonomic innervation to the head and neck is from what nerves?
|
T1-4
|
|
|
sympathetic autonomic innervation to the heart and lungs is from what nerves?
|
T1-6
|
|
|
sympathetic autonomic innervation to the stomach, duodenum, liver, gall bladder, pancreas, spleen, is from what nerves?
|
T5-9
|
|
|
sympathetic autonomic innervation to the small intestines, kidney, ureters, gonads, right colon, is from what nerves?
|
T10-11
|
|
|
sympathetic autonomic innervation to the left colon and pelvic organs, (bladder and prostate), is from what nerves?
|
T12-L2
|
|
|
In what nerve roots would cutting, touch, or cold pain from the heart be directed to?
|
none. Only metabolic products (via ischemia) stimulating nerve endings in the myocardium could cause pain.
|
|
|
The afferent pain fibers of the heart run centrally in the ____ and ____ cervical branches and especially in the ____ cardiac branches of the sympathetic trunk.
|
middle and inferior cervical branches. thoracic cardiac branches.
|
|
|
The axons of the afferent heart pain fibers primary sensory neurons enter spinal cord segments T1–T4 or T5, especially on the ___ side.
|
left
|
|
|
Visceral pain is transmitted by visceral afferent fibers accompanying ____ fibers and is typically referred to somatic structures or areas such as the upper limb having afferent fibers with cell bodies in the same spinal ganglion, and central processes that enter the spinal cord through the same ____ roots.
|
sympathetic, posterior.
|
|
|
The thoracic cavity communicates with the neck and upper limb through what?
|
the superior thoracic aperture also known as the (boney) thoracic inlet
|
|
|
What passes through the thoracic inlet?
|
Trachea, esophagus, major vessels and nerves pass through here
|
|
|
Lymphatic drainage for the whole body drains into the venous system immediately posterior to what?
|
the medial end of the clavicle and 1st rib
|
|
|
Inferiorly, the thoracic cavity communicates with the abdomen through what?
|
the anatomic thoracic outlet, closely associated with the abdominal diaphragm.
|
|
|
thoracic inlet boundary posteriorly?
|
T1 vertebrae
|
|
|
thoracic inlet boundary laterally?
|
Laterally by medial margins of 1st ribs and costal cartilaces
|
|
|
thoracic inlet boundary anteriorly?
|
Anteriorly by superior/posterior border of manubrium
|
|
|
what covers the thoracic inlet? From what muscle group is it from?
|
The cervicothoracic (diaphragm) fascia. It is the deep fascia of the scalenus muscle group. Including variably fibrous bands, this fascia inconsistently includes muscle fibers from scalenus minimus. This fascial covering of the superior dome of the lung is also referred to as Sibson’s Fascia (Grey’s Anatomy)
|
|
|
What is Sibson's fascia?
|
The cervicothoracic (diaphragm) fascia covering the thoracic inlet. It is the deep fascia of the scalenus muscle group. Including variably fibrous bands, this fascia inconsistently includes muscle fibers from scalenus minimus. This fascial covering of the superior dome of the lung is also referred to as Sibson’s Fascia (Grey’s Anatomy)
|
|
|
The ____ fascia covering the thoracic inlet. It is the deep fascia of the scalenus muscle group. Including variably fibrous bands, this fascia inconsistently includes muscle fibers from scalenus minimus. This fascial covering of the superior dome of the lung is also referred to as Sibson’s Fascia (Grey’s Anatomy)
|
cervicothoracic (diaphragm)
|
|
|
The thoracic ____ is often referred to the area bounded by the scapulae, 1st ribs and the clavicles.
|
outlet
|
|
|
The thoracic outlet is often referred to the area bounded by what structures?
|
the scapulae, 1st ribs and the clavicles.
|
|
|
A compression syndrome can act upon the neurovascular bundle as it travels from the ___ ___ to the neck.
|
scalene triangle
|
|
|
thoracic outlet syndrome can compress the neurovascular bundle, squeezing the ___ vein and artery and the ____ plexus.
|
subclavian, brachial
|
|
|
arch of aorta lies superior to what vert level?
|
T4
|
|
|
anterior portion of 2nd rib lies at what vert level?
|
T4
|
|
|
bifurcation of trachea lies at what vert level?
|
T4
|
|
|
Umbilicus vert level?
|
L3/L4
|
|
|
What are 6 soft tissue techniques?
|
1. Inhibition 2. Prone Stretching 3. Rhomboid Stretching 4. Prone Kneading 5. Lateral Recumbent Kneading 6. Supine Kneading
|
|
|
what type of technique is Inhibition?
|
Soft Tissue
|
|
|
what type of technique is Prone Stretching?
|
Soft Tissue
|
|
|
what type of technique is Rhomboid Stretching?
|
Soft Tissue
|
|
|
what type of technique is Prone Kneading?
|
Soft Tissue
|
|
|
what type of technique is Lateral Recumbent Kneading?
|
Soft Tissue
|
|
|
what type of technique is Supine Kneading?
|
Soft Tissue
|
|
|
Direct pressure applied to an area of soft tissue change/“tightness” is which technique?
|
Inhibition
|
|
|
Force applied in the direction of the muscle fibers is which technique?
|
Stretching
|
|
|
Force applied in the direction perpendicular to the muscle fibers s which technique?
|
Kneading
|
|
|
Tenderness of supraspinous ligament is a common finding of which type of SD? SB, FB/BB, or rotation?
|
FB/BB - also found is a Separation or approximation of spinous processes
|
|
|
a flexed SD is equivalent to a BB ____.
|
BB restriction = F SD = Flexed.
|
|
|
In FB SD, the SP of the Flexed vertebrae will approximate (get closer to) the vert above or below it?
|
ABOVE. SP will not approximate with SP on segment below during extension if there is SD.
|
|
|
In BB SD, the SP of the Flexed vertebrae will approximate (get closer to) the vert above or below it?
|
BELOW. E SD SP will not separate from the SP of segment below during flexion when there is SD.
|
|
|
an extended SD is equivalent to a FB ____.
|
FB restriction = E SD = Extended SD.
|
|
|
Sidebending is determined by the direction of ease of motion and named for the side of ____.
|
concavity
|
|
|
Rotation is determined by the direction of ease of motion and named by movement of a point on the ___/____ surface of the vertebral body
|
superior/anterior
|
|
|
If a posteriorly rotated process moves anteriorly with flexion it is what type of mechanic?
|
Type 2. the diagnosis is FRxSx
|
|
|
If a posteriorly rotated process moves anteriorly with extension it is what type of mechanic?
|
Type 2. the diagnosis is ERxSx
|
|
|
If rotational component does not change with either maneuver, it is what type of mechanic?
|
Type 1. the diagnosis is NSxRy
|
|
|
Still technique steps?
|
Indirect. Pressurize. Move thru Neutral to Direct. Release when there is release.
|
|
|
One of the most common thoracic Type I somatic dysfunctions is at ___ .
|
T1. To treat this use the head and neck as if you were performing a treatment on the neck.
|
|
|
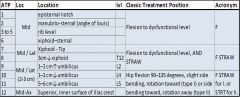
What is the location for the AT1 tenderpoint(s)?
|
Midline episternal notch
|
|
|
What is the location for the AT2 tenderpoint(s)?
|
Midline, junction of manubrium and sternum (angle of Louis)
|
|
|
What is the location for the AT3-AT5 tenderpoint(s)?
|
Midline at level of corresponding rib;
|
|
|
What is the location for the AT6 tenderpoint(s)?
|
Midline xiphoid–sternal junction
|
|
|
What is the location for the AT7 tenderpoint(s)?
|
Midline or inferolateral to tip of xiphoid;
|
|
|
What is the location for the AT8 tenderpoint(s)?
|
3 cm below xiphoid at level of T12, midline or lateral
|
|
|
What is the location for the AT9 tenderpoint(s)?
|
1–2 cm above umbilicus at level of L2, midline or 2–3 cm lateral
|
|
|
What is the location for the AT10 tenderpoint(s)?
|
1–2 cm below umbilicus at level of L4, midline or 2–3 cm lateral
|
|
|
What is the location for the AT11 tenderpoint(s)?
|
5–6 cm below umbilicus below level of iliac crests at superior L5 level, midline or 2–3 cm lateral
|
|
|
What is the location for the AT12 tenderpoint(s)?
|
Superior, inner surface of iliac crest at mid-axillary line
|
|
|
Which tenderpoint is the following location referring to? ( Midline episternal notch ).
|
AT1
|
|
|
Which tenderpoint is the following location referring to? ( Midline, junction of manubrium and sternum (angle of Louis) ).
|
AT2
|
|
|
Which tenderpoint is the following location referring to? ( Midline at level of corresponding rib;).
|
AT3-AT5
|
|
|
Which tenderpoint is the following location referring to? ( Midline xiphoid–sternal junction ).
|
AT6
|
|
|
Which tenderpoint is the following location referring to? ( Midline or inferolateral to tip of xiphoid;).
|
AT7
|
|
|
Which tenderpoint is the following location referring to? ( 3 cm below xiphoid at level of T12, midline or lateral).
|
AT8
|
|
|
Which tenderpoint is the following location referring to? ( 1–2 cm above umbilicus at level of L2, midline or 2–3 cm lateral ).
|
AT9
|
|
|
Which tenderpoint is the following location referring to? ( 1–2 cm below umbilicus at level of L4, midline or 2–3 cm lateral).
|
AT10
|
|
|
Which tenderpoint is the following location referring to? ( 5–6 cm below umbilicus below level of iliac crests at superior L5 level, midline or 2–3 cm lateral).
|
AT11
|
|
|
Which tenderpoint is the following location referring to? ( Superior, inner surface of iliac crest at mid-axillary line ).
|
AT12
|
|
|
What is the classic treatment position for AT1 - AT6? Abbreviation?
|
Flexion to dysfunctional level. F
|
|
|
What is the classic treatment position for AT7? Abbreviation?
|
Flexion to dysfunctional level, side bending toward and rotation away F St RA
|
|
|
What is the classic treatment position for AT8? Abbreviation?
|
Flexion to dysfunctional level, side bending toward and rotation away F St RA
|
|
|
What is the classic treatment position for AT9? Abbreviation?
|
Flexion to dysfunctional level, side bending toward and rotation away F St RA
|
|
|
What is the classic treatment position for AT10? Abbreviation?
|
Hip flexion 90–135 degrees, slight side bending, rotation toward (type I) or side bending toward, rotation away (type II) F St RT or F St RA
|
|
|
What is the classic treatment position for AT11? Abbreviation?
|
Hip flexion 90–135 degrees, slight side bending, rotation toward (type I) or side bending toward, rotation away (type II) F St RT or F St RA
|
|
|
What is the classic treatment position for AT12? Abbreviation?
|
Hip flexion 90–135 degrees, slight side bending, rotation toward (type I) or side bending toward, rotation away (type II) F St RT or F St RA
|
|
|
How many secondary curves are there?
|
2. the primary curve is a kyphosis. The secondary curves are the lordoses of the cervical and lumbar area.
|
|
|
when does the cervical curve develop?
|
child begins to hold its head up
|
|
|
when does the lumbar curve develop?
|
child begins to stand and walk
|
|
|
What is the normal Ferguson angle?
|
30-40 degrees
|
|
|
Sagittal plane orientation of the facets favors which movements?
|
F and E, not so much Rotation and SBing
|
|
|
what percent of the population have congenital osseous asymmetry? And which one is most common? (sacralization, lumbarization, spina bifida occulta, facet asym)
|
40% and facet asym
|
|
|
what is facet asym?
|
facet is in a different plane
|
|
|
where is the most likely place on the vertebral body for a compression fracture and why?
|
Anterior triangle becomes weak link for compression fracture due to lack of bone deposition. (wolfe's law points out bone deposition along line of stress, which this area does not usually have any).
|
|
|
what is the batwing deformity?
|
sacralization
|
|
|
of the nucleus propulsus, the annulus is embryogically from ____.
|
mesenchyme
|
|
|
of the nucleus propulsus, the notocord (soon to be propulsus) is embryogically from ____.
|
ectoderm
|
|
|
what does the nucleus propulsus have a high content of?
|
water
|
|
|
Decreased disc thickness causes an increased weight load on the ___ joint
|
facet
|
|
|
what position applies the greatest load possible to the IV disc?
|
sitting with poor posture
|
|
|
which ligament around the spine is broad and limits extension?
|
ant longitudinal ligament
|
|
|
which ligament around the spine is narrow and limits flexion?
|
posterior longitudinal ligament
|
|
|
superiorly, the ant longitudinal ligament continues on as what?
|
atlanto-Axial ligament, running straight up
|
|
|
superiorly, the post longitudinal ligament continues on as what?
|
tectorial membrane, (runs just over the transverse ligament).
|
|
|
the iliolumbar ligaments are commonly strained in traumatic injuries. What are their superior attachment points?
|
transverse processes of L4 and L5
|
|
|
what is the attachment point of the diaphragm's left crus?
|
L1-L2
|
|
|
what is the attachment point of the diaphragm's right crus?
|
L1-L3
|
|
|
what is the origin and insertion of Quadratus lumborum?
|
Originates on inf. border of 12th rib and tips of lumbar transverse processes. Inserts on Iliolumbar ligament and iliac crest.
|
|
|
what is the origin and insertion of Psoas major?
|
Originates on transverse process of T12-L5. Inserts on lesser trochanter of femur.
|
|
|
what is the origin and insertion of Psoas minor?
|
Originates on transverse process of T12-L1. Inserts on Pectineal line.
|
|
|
what is the origin and insertion of Latissimus dorsi?
|
Originates on Humerus (intertubecular groove). Inserts on T7-12,Iliac crest, Thoracolumbar fascia.
|
|
|
what is the origin and insertion of Gluteus maximus?
|
Originates in Thoracolumbar fascia and on dorsal sacrum. Inserts on Iliotibial band and femur.
|
|
|
what is the innervation of Quadratus lumborum?
|
Innervation T12,L1-4 ventral rami
|
|
|
what is the innervation of Psoas major?
|
Innervation L1-3(2-4) ventral rami
|
|
|
what is the innervation of Psoas minor?
|
Innervation L1 ventral rami
|
|
|
what is the innervation of Latissimus dorsi?
|
Innervation: Thoracodorsal nerve (C6-8)
|
|
|
what is the innervation of Gluteus maximus?
|
Innervation: Inferior Gluteal nerve (L5,S1-2)
|
|
|
what is the function of Quadratus lumborum?
|
Extension and sidebending
|
|
|
what is the function of Psoas major?
|
Flexes and internally rotates hip
|
|
|
what is the function of Psoas minor?
|
Flexes hip
|
|
|
what is the function of Latissimus dorsi?
|
Humerus motion and raises body to arms during climbing
|
|
|
what is the function of Gluteus maximus?
|
Extends hip and stabilizes torso
|
|
|
what are the dirty half-dozen coined by Phil Greenman for "failed back"?
|
4S's, Type 2, and Psoas muscle imbalance. S's are 1. Shear - Pubic. 2. Shear - Sup inominate (as in pregos). 3. Sacrum ext. 4. Shorty leg
|
|
|
in radiology, a "bulging" disc means what?
|
an incomplete disc herniation, (not ruptured).
|
|
|
Disc herniations occur most often in which direction and in what part of the spine?
|
Posterio-lateral herniation most common. Why? narrow posterior longitudinal ligament. 98% will be in L4-L5-S1
|
|
|
which Nerve Root exits the foramina inferior to the superior pedicle of L4's vertebral body and superior to the intervertebral disc of L5?
|
L4
|
|
|
L4-L5 compression will compromise which nerve root?
|
L5. X+1 rule. Nerve root X will have already exited the foramina and will be unaffected
|
|
|
What are the 3 things to test for in L4 neuro exam?
|
1. Foot inversion (Tibialis anterior) 2. Patellar reflex 3. Medial aspect of foot sensation
|
|
|
What are the 2 things to test for in L5 neuro exam?
|
1. Great toe extension (Extensor Hallicus longus) 2. Dorsum of foot sensation
|
|
|
What are the 3 things to test for in S1 neuro exam?
|
1. Foot eversion (Peroneus longus and brevis) 2. Achilles tendon reflex 3. Lateral foot sensation
|
|
|
Positive Babinski reflex indicates what?
|
upper motor neuron problems, specifically pyrimidal tract.
|
|
|
Positive Babinski reflex indicates a problem in the Upper motor neurons. What are three spots this could have occurred?
|
cortical, subcortical, spinal cord.
|
|
|
What is the origin and insertion of Piriformis?
|
Originates on the anterior lateral border of the sacrum. Insertion is on the upper border of the greater trochanter.
|
|
|
what is the function of piriformis?
|
Action is external rotation of extended thigh and abduction of flexed thigh
|
|
|
what is the only muscle to bridge the anterior SI joint?
|
piriformis
|
|
|
What is the innervation to piriformis?
|
Innervation is L4-S3
|
|
|
the Left Colon is innervated by?
|
T12 - L2
|
|
|
the bladder is innervated by?
|
T12 - L2
|
|
|
the prostate is innervated by?
|
T12 - L2
|
|
|
the lower extremity is innervated by?
|
T12 - L2
|
|
|
Ileus is associated with an increase in parasymps or symps?
|
sympathetics
|
|
|
Constipation is associated with an increase in parasymps or symps?
|
sympathetics
|
|
|
Abdominal pain is associated with an increase in parasymps or symps?
|
sympathetics
|
|
|
Flatulence is associated with an increase in parasymps or symps?
|
sympathetics
|
|
|
Distension is associated with an increase in parasymps or symps?
|
sympathetics
|
|
|
Colitis is associated with an increase in parasymps or symps?
|
parasympathetics
|
|
|
Crohn’s is associated with an increase in parasymps or symps?
|
parasympathetics
|
|
|
IBS (both inc.) is associated with an increase in parasymps or symps?
|
parasympathetics
|
|
|
Diarrhea is associated with an increase in parasymps or symps?
|
parasympathetics
|
|
|
Vomiting is associated with an increase in parasymps or symps?
|
parasympathetics
|
|

Name the 1. test, 2. procedure, 3. positive sign, and 4. indication.
|
Spurling's Test
E, rotates/SBs it to one side w/ compression. Positive sign: pain ipsilateral arm (side of symptoms). Indicates: cervical disc disease/nerve root irritation |
|
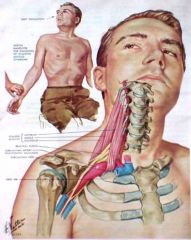
Name the 1. test, 2. procedure, and 3. indication.
|
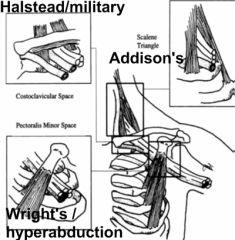
1. Adson’s test
2. Neck extended turned toward affected side 3. Compression of brachial plexus & subclavian artery between anterior & middle scalene |
|
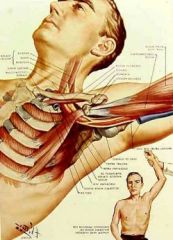
Name and assessment of this test?
|
Wright's test. Compression of neurovascular bundle between pectoralis minor muscle and thoracic cage
|
|
Name this test and assessment?
|
Halstead or Military Test. Compression of neurovascular bundle between the clavicle and the first rib
|
|

Which test would you use for each impingement site for a thoracic outlet syndrome?
|
|
|
|
In Straight leg raise test, doc raises leg to what degrees?
|
70 to 90
|
|
|
what is a good follow up test to the straight-leg test? What do you do? What does it indicate?
|
Braggard's test. Lower leg and then dorsiflex foot. If negative, but Straight leg test was positive, you might have tight hamstrings.
|
|
|
Whats the thomas test?
|
knee to chest, monitor the back of knee for lift. (shortened psoas m.)
|
|
|
Hipdrop test screens for the ability of what?
|
the lumbar and lumbothroacic region to sidebend away from the side of the hip drop
|
|
|
what is a positive hip drop sign?
|
the plane of the iliac crests drops less than 20 degrees and/or the lumbar and thoracolumbar spine does not side bend with a smooth lateral curve; named to the side being tested
|
|
|
Which ribs are true?
|
1 through 7
|
|
|
Which ribs are false?
|
8 thru 10
|
|
|
what are the attachments points to the anterior chest for the true and false ribs?
|
True Attach directly to the sternum via costochondral cartilage. False Attach via a synchondroses to the costochondral cartilage of rib 7
|
|
|
which ribs are floating?
|
11 thru 12
|
|
|
what are the typical ribs?
|
three thru 10
|
|
|
what are the atypical ribs?
|
1,2,11,12
|
|
|
which part of the typical rib articulates with corresponding costotransverse process (one articulation)?
|
Tubercle
|
|
|
which part of the typical rib is the costovertebral articulation with corresponding and immediately superior vertebrae via demifacets (two articulations). (Also a strong ligamentous attachment to the annulus of the intervertebral disk )
|
head
|
|
|
which part of the typical rib is an area between tubercle and head
|
neck
|
|
|
Which rib is broad and flat and articulates via a unifacet, and has no angle? It is the lateral boundary of the thoracic inlet and has multiple types of dysfunction.
|
rib 1
|
|
|
which rib is atypical because of large tuberosity on shaft for serratus anterior?
|
Rib 2. Anteriorly it articulates by a strong cartilaginous attachment with the manubriogladiolar junction of the sternum at the Angle of Louis. The second rib articulates by two demifacets with T1 and T2.
|
|
|
which ribs are atypical b/c they articulates only with corresponding vertebrae, and have a lack of tubercles?
|
Ribs 11,12
|
|
|
Alteration of the Rib ____ profoundly influences' the function of the sternum and frequently contributes to pain syndromes in the upper extremity.
|
rib 2
|
|
|
Which ribs are both associated with the muscles of the posterior abdominal wall?
|
ribs 11 and 12
|
|
|
The quadratus lumborum muscle attaches to the inferior margin of the rib ____.
|
rib 12
|
|
|
The ____ rib is frequently asymmetric in length. Neither attaches to a costal arch.
|
rib 12
|
|
|
The costochonral articulations are primarily what type of joint?
|
cartilaginous
|
|
|
Ribs 6-9 interchondral articulations are ____ joints and 9-10 is mainly a ____ joint.
|
synovial. fibrous .
|
|
|
Rib 1 is a synchondrosis, which is synovial or not?
|
not
|
|
|
Ribs 2-7 are synovial joints or not?
|
Synovial articulations
|
|
|
which muscle Attaches to ribs 3-5 anterior and the coracoid process of the scapula? (This can be implicated in shoulder SD or various impingement syndromes. )
|
pec minor
|
|
|
four muscles of inspiration?
|
scalenes, SCM, diaphragm, intercostals (mainly external)
|
|
|
Diaphragm (The primary respirator) attaches to which ribs?
|
Attaches to the lower 6 or seven ribs. Pulls these ribs inferiorly and flattens abdominal contents
|
|
|
Pectoralis Major attaches to which ribs?
|
2 thru 6
|
|
|
serratus anterior works especially hard on which ribs during inspiration?
|
7 thru 9
|
|
|
which muscle is involved in inspiration and Originates on the SP of C7-T3 Inserts Ribs 2-5?
|
Seratus posterior superior
|
|
|
With arm above head, activation of this muscle pulls ribs 11 & 12 superiorly and laterally.
|
lat dorsi
|
|
|
name the muscles involved in quiet breathing exhalation.
|
none. Elastic recoil of lungs.
|
|
|
name the muscles involved in active breathing exhalation.
|
1. Intercostalis int. 2. Rectus abdominis. 3. Obliques, int. & ext. 4. Transversus abdominis
|
|
|
which muscle Originates on the SPs of T10-L2, Inserts on ribs 9-12?
|
serratus posterior inferior
|
|
|
which muscle Pulls the 12th and 11th ribs inferiorly?
|
quadratus lumborum
|
|
|
Diaphragmatic _____ (relaxation/contraction) increases relative negative pressure of thoracic cage and increases relative positive pressure in abdomen. Pressure gradient between the thoracic and abdominal cavities allow lymphatic and venous fluids to flow from the body to the upper thoracic area.
|
contraction
|
|
|
Which ribs are involved in Pump-Handle motion?
|
Primarily ribs 1-5
|
|
|
Which ribs are involved in Bucket-Handle motion?
|
Primarily ribs 6-10
|
|
|
Which ribs are involved in Caliper motion?
|
Primarily ribs 11,12
|
|
|
which type of motion is being described? 1. Ribs move laterally and increase transverse diameter with inhalation 2. Motion predominantly in coronal plane 3. Best palpated at mid-axillary line 4. Axis of motion is a costovertebral-costosternal line
|
BUCKET HANDLE
|
|
|
which motion is being described?1. Ribs move anterior and superior with inhalation 2. Motion predominantly in sagittal plane 3. Best palpated at mid-clavicular line 4. Axis of motion is costovertebral-costotransverse line
|
PUMP Handle
|
|
|
which motion is being described? 1. Ribs externally rotate with inhalation 2. Motion predominantly in transverse plane 3. Best palpated 3-5 cm lateral to transverse processes 4. Axis of motion is vertical line
|
Caliper motion
|
|
|
inhalation strain is synonymous with inhalation or exhalation rib dysfunction?
|
inhalation rib dysfunction.
|
|
|
There's an inhalation SD at ribs 4-6. which rib is key to treatment?
|
rib 6, last rib
|
|
|
theres a gap at ribs 6-7. what are the two possible SD's?
|
Rib 6 has inhalation SD. OR rib 7 has exhalation SD.
|
|
|
Scalane muscle check uses what test?
|
Addsons'. Checks same side impingement.
|
|
|
Thoracic outlet syndrome has five possible sources. List them. Important.
|
1. Entrapment between the Scalenus anterior and medius. 2. Entrapment between the clavicles and the first rib. 3. Entrapment between tendon of Pectoralis minor and ribs. 4. Cervical ribs. 5. Fascial distortions.
|
|
|
Anterior - sternal-xiphoid junction is at which rib?
|
rib 7
|
|
|
There's an exhalation SD at ribs 7-9. which rib is key to treatment?
|
rib 7, first rib
|
|
|
Ant and Mid scalenes is/are associated with which rib(s)?
|
1
|
|
|
post scalene is/are associated with which rib(s)?
|
2
|
|
|
pec minor is/are associated with which rib(s)?
|
3 to 5
|
|
|
Serratus anterior is/are associated with which rib(s)?
|
6 to 9
|
|
|
lat dorsi is/are associated with which rib(s)?
|
10 and 11
|
|
|
quadratus lumborum is/are associated with which rib(s)?
|
12
|
|
|
Rib 1 is associated with which muscle(s)?
|
Ant and Mid scalenes
|
|
|
Rib 2 is associated with which muscle(s)?
|
post scalene
|
|
|
Rib 3 to 5 is associated with which muscle(s)?
|
pec minor
|
|
|
Rib 6 to 9 is associated with which muscle(s)?
|
Serratus anterior
|
|
|
Rib 10 and 11 is associated with which muscle(s)?
|
lat dorsi
|
|
|
Rib 12 is associated with which muscle(s)?
|
quadratus lumborum
|
|
|
A somatic dysfunction is “an impairment or altered function of related components of the somatic (body framework) system" including what?
|
SAM VLN. Skeletal, Arthroidal, and Myofascial structure and related Vascular, Lymphatic, and Neural elements.
|
|
|
muscle spindles measure muscle ___ (tension/length) in ___ (parallel/series).
|
length, parallel
|
|
|
Golgi tendons measure muscle ___ (tension/length) in ___ (parallel/series).
|
tension, series
|
|
|
Chronic pain will Shift from sensory cortex to regions such as ____ ___ associated with affective-motivational processing
|
cingulate gyrus
|
|
|
Chronic pain will Shift from sensory cortex to regions such as cingulate gyrus associated with ___-____ processing
|
affective-motivational
|
|
|
3 factors of muscle imbalance are what?
|
shortening, weakness, altered proprioception
|
|
|
weakness of a muscle affecting muscle imbalance usually involves what type of muscles?
|
phasic, fast-twitch
|
|
|
What’s the differential diagnosis for left upper extremity paresthesia?
|
V.I.N.N.D.I.C.A.T.E.S. Vascular . Inflammatory . Neoplastic . Neurologic . Drugs. Idiopathic. Congenital. Autoimmune. Traumatic . Endocrine/Metabolic. Skeletal/Musculoskeletal.
|
|
|
definition of a trigger point?
|
Discrete, focal, hyperirritable spots located in a taut band of skeletal muscle
|
|
|
Draw the Anterior Tender Points Chart
|
|