![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
83 Cards in this Set
- Front
- Back
|
Differential Diagnosis - Acute Painless Loss of Vision |
Lens Lens Dislocation Posterior chamber Vitreous Hemorrhage Retina Retinal detachment Central retinal artery occlusion Retinal Vein Occlusion Optic Nerve Ischemic Optic Neuropathy |
|
|
Differential Diagnosis - Acute Painful Loss of Vision |
Temporal arteritis Optic Neuritis Retinal Vasculitis Acute Angle Closure Glaucoma Trauma - Corenal Abrasion - Iridocyclitis - Hyphema - Globe Rupture Infection |
|
|
Differential Diagnosis of Red Eye |
Episcleritis Scleritis Subconjunctival Hemorrhage Conjuntivitis Keratitis Iritis Acute Angle Closure Glaucoma |
|
|
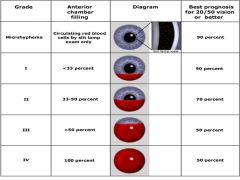
Grading of Hyphema |
|
|
|
Components of complete ED opthalmologic exam
|
Visual acuity (with correction)
Visual fields by confrontation External structure examinations Extraocular movements Pupilary Examinations Pressure determination Slit Lamp Examination Fundoscopic Examination |
|
|
Normal Intraocular pressure
|
10 - 20 mm Hg
|
|
|
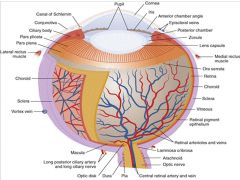
Cross Sectional Anatomy of Eye |
|
|
|
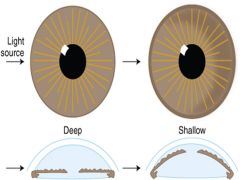
Estimating anterior chamber depth with oblique illumination |
|
|
|
Cyclopentolate |
Anticholinergic
Short-term mydriasis and cycloplegia for examination
0.5% in children, one drop; 1% in adults, one drop; onset 30 min, duration ≤24 h |
|
|
Tropicamide |
Anticholinergic
Short-term mydriasis and cycloplegia for examination
One to two drops of 0.5% or 1% solution, onset 20 min; duration of action 6 h |
|
|
Homatropine |
Anticholinergic
Intermediate-term pupil dilation, cycloplegia, treatment of iritis
One to two drops of 2% solution; onset 30 min; duration of action 2–4 d; for iritis one to two drops twice a day |
|
|
Naphazoline and pheniramine (Naphcon-A®, Visine A®) |
Antihistamine/decongestant
Conjunctival congestion/itching
One drop three to four times a day |
|
|
Olopatadine (Patanol) |
Antihistamine
Allergic conjunctivitis
0.1% solution, one drop twice daily, onset of action 30–60 min, duration 12 h |
|
|
Occular Antibiotics |
Erythromycin ophthalmic ointme 1/2 itn. applied to lower eyelid two to four times/d
Ciprofloxacin/Ciloxan®Ophthalmic Solution and Ointment Solution: one to two drops when awake every 2 h for 2 d; ointment, 1/2 in. applied to lower eyelid three times a day for 2 d
Tobramycin/Tobrex®ophthalmic solution and ointment 0.3% solution, one to two drops every 4 h; 0.3% ointment, 1/2 in. applied to lower lid two to three times/d
Gentamicin/Garamycin®/Genoptic®Conjunctiv 0.3% solution, instill one to two drops every 4 h; 0.3% ointment, 1/2 in. applied to lower lid two to three times/d
polymyxin B/bacitracin ophthalmic (Polysporin) Apply thin 1/2 thin ribbon of ointment to conjunctival sac q3-4hr for 7-10 days |
|
|
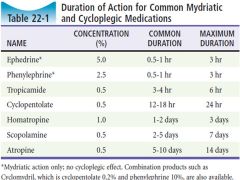
Overview of common mydriatic and cycloplegics found in some ER |
|
|
|
Most common causes of bacterial conjunctivitis |
Haemophilus influenzae, Streptococcus pneumoniae, and Staphylococcus |
|
|
DDX Caustic Contaminiation |
Caustic keratoconjunictivity |
|
|
DDX Proptosis/External Swelling |
Blepharitis Chalazion Dacrocystitis anddacroadenitis Hordeolum (a.k.a. stye) Inflammatory pseudotumor Orbital celluitis Orbital tumor Periorbital cellulitis or erysipelas Retrobulbar abscess Retrobulbar emphysema Retrobulbar hematoma* |
|
|
DDX severe pain, foreign body sensation, or limbal injection |
Keratitis* (incl abrasionand ulcer) Keratoconjunctivitis Episcleritis Scleritis Anterior uveitis and hypopyon Acute angle–closure glaucoma Hyphema Endophthalmitis* |
|
|
DDX of focal redness of bulbar conjunctiva |
Inflamed pingueculum Inflamed pterygium Scleral penetration Subconjunctival hemorrhage |
|
|
DDX Purulent Discharge |
Bacterial Conjunctivity |
|
|
DDX Itching sensation (+/- other sx) |
Allergic conjunctivitis |
|
|
DDX airborne allergen/topical med/cosmetic |
Contact dermatoconjunctivitis Toxic Conjunctivitis |
|
|
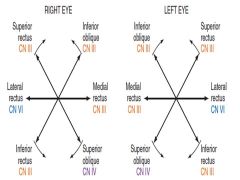
Cardinal Eye Movements |
|
|
|
S/S of restricitive/mechanical orbitopathy |
Symptoms: - Gradual onset, binocular diplopia - Mass effect/discomfort in affected eye
Signs: - Associated signs (proptosis, periorbital swelling, edema, conjunctival or scleral hyperemia, or palpebral swelling involving a single eye) - Gradual restriction of movement away from affected eye |
|
|
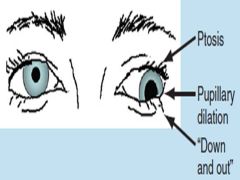
CN III PALSY |
|
|
|
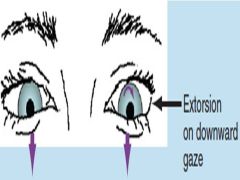
CN IV PALSY |
|
|
|
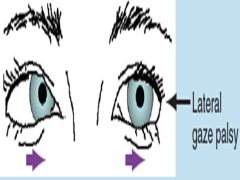
CN VI PALSY |
|
|
|
CN most commonly affected by hypertensive/diabetic vasculopathy in adults |
CN III |
|
|
Differentiating vasculopathy from CN Compression |
Vasculopathy: Pupil sparing |
|
|
Cavernous sinus contents |
Internal Carotid artery (+sympathetic plexus) Lateral wall (superior to inferior) CN III CN IV V1 V2
CNVI -> Through cavernous sinus |
|
|
Internuclear opthalmoplegia |
Disorder of conjugate lateral gaze in which affected eye shows impaired adduction and unaffected eye abducts with nystagmus
Due to lesion in Median Longitudinal Fasiculus
Convergent gaze preserved |
|
|
5 D's of posterior stroke |
Dizzy Dysphagia Dysarthria Diplopia Dysataxia/Dysmetria |
|
|
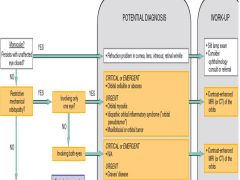
Overview of DDx/Approach to Diplopia Questions 1 & 2 |
|
|
|
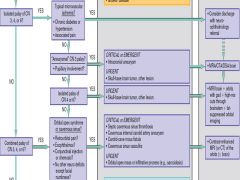
Overview of DDx/Approach to Diplopia Questions 3 |
|
|
|
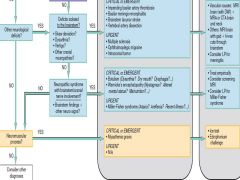
Overview of DDx/Approach to Diplopia Questions 4 & 5 |
|
|
|
Indications for ED Lateral Canthotomy
Contraindication |
Decreased visual acuity IOP >40 Proptosis
Afferent pupillary defect Opthalmoplegia Severe eye pain Optic nerve pallor Cherry red macula
Contraindication Ruptured globe |
|
|
Technique of ED Lateral Canthotomy |
1. Local anasthesia of lateral canthus 2. Crush lateral canthus with hemostat 3. Incise lateral canthus 4. Pull lower eyelid and cut inferior lateral canthal tendon 5. If not resolved, cut superior lateral canthal tendon |
|
|
Orbital Wall Fractures |
Floor: Endopthalmos, ptosis, diplopia & limitation of upward gaze (due to entrapment of inferior rectus/oblique), anesthesia of upper cheek/lip
Medial Wall: Epistaxis, emphysema, diplopia from medial rectus entrapment |
|
|
Long term complications of opthamological chemical burns |
Perforation Scarring Corneal neovasculatrization Adhesions Glaucoma Cataracts Retinal damage |
|
|
MARCUS - GUNN PUPIL |
Relative afferent pupillary defect
|
|
|
When to consider hyphema admission |
>50% anterior chamber Decreased vision Increased IOP Sickle Cell Disease |
|
|
Opthamological Medication contraindicated in sickle cell disease |
Carbonic Anhydrase Inhibitors
(Increased pH in Aqueous humor promotes sickling)
Start treatment with topical beta-blocker All others in consult with opthamology |
|
|
When are hyphemas highest risk for rebleeding |
2-5 Days out |
|
|
Medications for hyphema |
Avoid anti-coagulants/platelet agents Topical beta blocker Topical alpha-agonist +/- CAIs and Mannitol +/- TXA May be role for mydriatics |
|
|
Complications of hyphema |
Rebleeding Corneal blood staining Glaucoma Anterior/posterior synechiae formation |
|
|
Iridodialysis |
Tearing of iris root from ciliary body
Need to see optho if associated hyphema |
|
|
Traumatic iridocyclitis/uveitis |
Symptoms Photophobia Deep/Aching eye pain
Signs Ciliary Flush Cells and Flare on SLE Small poorly dilating pupil Direct and consensual photophobia
Rx with long-acting mydriatics to paralyze ciliary body |
|
|
Most common sites of globe rupture in blunt trauma |
At points where sclera is thinnest:
(1) Limbus (2) Insertion sites of EOM |
|
|
Signs of globe rupture |
Decreased Visual Acuity Irregular/tear drop shaped pupil RAPD Shallow Anterior Chamber Hyphema Positive Seidel Sign Lens dislocation Large Subconjunctival hemorrhage Hemorrhagic chemosis Uveal prolapse |
|
|
Management of suspected/Confirmed Globe rupture |
Protect Eye HOB elevated NPO Anti-emetics/analgesics Broad Spectrum AbX Tetanus Update |
|
|
Posterior segment injuries in Blunt Trauma |
Posterior Vitreous Hemorrhage Retinal Detachment Retinal Tear Commotio Retinae Optic Nerve Injury |
|
|
Complex Lid Lacerations that should be defered for specialist repair |
1. Lacerations involving the lid margins. |
|
|
Complications of occular trauma |
Corneal ulcer Endopthalmitis Sympathetic opthalmia |
|
|
Endopthlamitis |
Infection of anterior, posterior, and vitreous chambers
Occurs following: - Glove rupture - Penetrating eye injury - Foreign bodies - Occular surgery |
|
|
Opthalmia neonatorium |
Conjunctivitis within 1st month of life
Gonhorrea (2-4 days after birth) Chlamyidia (5-14 days after birth) Chemical (1-2 days after birth) |
|
|
Ptyerigum |
Wedge shaped fibrovascular tissue from conjunctiva that extends onto cornea |
|
|
Pinguecula |
Wedge shaped fibrovascular growth on conjunctiva |
|
|
Chalazion vs Hordeolum (stye) |
Hordeolum = Inflammation of Gland of Zeiss/Hair Follice with involvement of lid margin
Chalazion = Obstructed Meobmian gland within lid surface without involvement of lid margin |
|
|
Dacrocystitis |
Infection of the lacrimal sac from nasolacrimal duct obstruction
Most commonly from S aureus
Require system and oral treatment |
|
|
Signs and symptoms of orbital cellulits |
Marked pain, swelling, edema Systemically unwell Proptosis RAPD Visual acuity changes Painful/limited EOM |
|
|
Complications of Orbital Cellulitis |
Orbital - Abscess - Optic neuritis - Keratitis - CRAO
Intracranial - Meningitis - Abscess - Cavernous sinus thrombosis |
|
|
Normal Flow of Aqueous Humour |
Ciliary Processes -> posterior chamber -> Pupillary aperture -> Trabecular meshwork -> Canal of Schlem -> Episcleral veins |
|
|
Glaucoma |
Optic neuropathy caused by increased intraocular pressure |
|
|
Classifications of glaucoma |
Primary Secondary -> Inciting event/insult
Open angle - No narrowing of anterior chamber Closed angle - Narrow anterior chamber angle |
|
|
Primary open-angle glaucoma |
Chronic, insidious form of glaucoma from increased resistant to outflow of aqueous humor via trabecular meshwork |
|
|
Primary angle closure glaucoma |
Small/shallow anterior chamber predisposes to pupillary block between lens and iris precipitated by pupil dilitation |
|
|
Treatment and MOA for Acute angle closure glaucoma
|
Topical β-blocker (timolol 0.5%), one drop - Block production of aqueous humor
Topical Alpha agonist (apraclonidine 1%), one drop -Block production of aqueous humor Carbonic anhydrase inhibitor (acetazolamide) 500 milligrams IV or PO - Block production of aqueous humor Mannitol, 1–2 grams/kg IV - Reduces volume of aqueous humor Topical pilocarpine 1%–2%, one drop every 15 min for two doses once IOP is below 40 mm Hg, then four times daily Facilitating outflow of aqueous humor by constricting pupil as is a parasympathomimetic |
|
|
Risk factors central retinal artery occlusion |
Carotid stenosis hypertension cardiac disease collagen vascular disease vasculitis cardiac valvular sickle cell disease |
|
|
Central retinal artery occlusion |
Sudden, painless loss of vision RAPD Fundoscopy: Pale retina with cherry red macula |
|
|
Central Retinal Artery Occlusion - Management
|
Globe massage
Carbogen for vasodilitation Timolol & Acetazolamide to reduce IOP +/- Intra-arterial thrombolysis |
|
|
Central retinal vein occlusion
|
Painless loss of vision
Blood and thunder fund us Rx Lower IOP steroids Opthalmology consult |
|
|
Mechanisms of retinal detachment and risk factors
|
Rhegamatogenous: result from tears in neuronal layer allowing vitreous fluid to leak and separate neuronal layer from pigment epithelium
Risk: Male, older degenerative myopia, trauma Exudative: Fluid leakage from vessels within retina Risk: Hypertension, preeclampsia, CRVO, Glomerulonephritis, papilidemia, vaaculitis, choroidal tumor Traction: Contraction of fibrous bands within posterior vitreous Risk: Posterior Vitreous Hemorrhage |
|
|
Posterior vitreous detachment
|
Vitreous gel pulling away from retina in older patient
Can be complicated by retinal break/detachment and posterior vitreous hemorrhage so need Opthalmology follow-up |
|
|
Vitreous Hemorrhage
|
Bleeding into preretinal space/posterior vitreous cavity
Risk: Diabetic retinopathy Neo vascularization -> branch retinal vein occlusion Sickle cell disease Retinal detachment Posterior vitreous detachment Trauma Maculae degeneration Trauma Intraocular tumor |
|
|
Overview of neuron opthalmological vision loss |

|
|
|
Causes of neuron opthalmological vision loss |
Prechiasmal Visual Loss - Optic Neuritis - Ischemic optic neuropathy Giant cell arteritis Idiopathic (DM, HTN, Vascular Dx) - Compressive Optic Neuropathy - Toxic and Metabolic Optic Neuropathy
Chiasmal - Compression from Tumor
Post-Chiasmal - Infarction - Tumor - AVM - Migraine |
|
|
Which pupil is abnormal in anisocoria |
Accentuated in light then larger pupil is abnormal
Accentuated in dark then smaller pupil is abnormal |
|
|
Adie's tonic pupil
|
Tonic dilated pupil
Impaired sweating Decreased lower extremity reflexes Hyperreaction to weak cholinergic agent Thought to result from damage to post ganglionic parasympathetic fibers of eye Non-urgent Opthalmology f/u |
|
|
Horner's syndrome and causes
|
Ptosis, miosis, and anhydrosis resulting from sympathetic denervation
Causes - CNS CVA/tumor - Lung CA - Thyroid adenoma - Pancoast tumor - Carotid Dissection - Herpes Zoster - Brachial plexus trauma - Otitis media - Headache syndromes |
|
|
Differential diagnosis anisocoria
|
Constricted pupil (accentuated in dark) |
|
|
Upper Limit of Normal for ESR
|
Age/2 for Men
(Age+10)/2 for Women |
|
|
Cause of Papilledema |
Increased ICP transmitted to optic nerve because optic nerve sheath is continous with sub-arachnoid space |