![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
459 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
mastitis abx tx |
fluclox |
|
|
|
mastitis mgmt |
tx and dont stop breast feeding |
|
|
|
candidal infxn of breast in breast feeding mgmt |
topical miconazole apply on nipple post feed and on babies oral mucosa dont stop breast feeding Education to the mother should also be given: Good hand hygiene after nappy change, sterilisation of anything that the baby puts in their mouth (dummies, teats etc) |
|
|
|
creatinine has increased from 98 to 172 µmol/l. Which one of the following tests is most useful when determining whether there is prerenal uraemia or acute tubular necrosis? |
Urinary sodium |
|
|
|
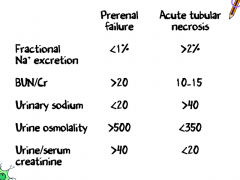
Acute kidney injury: acute tubular necrosis vs. prerenal uraemia |
Prerenal uraemia - kidneys hold on to sodium to preserve volume |
|
|
|
Acute kidney injury: acute tubular necrosis vs. prerenal uraemia |
*fractional sodium excretion = (urine sodium/plasma sodium) / (urine creatinine/plasma creatinine) x 100 **fractional urea excretion = (urine urea /blood urea ) / (urine creatinine/plasma creatinine) x 100 |
|
|
|
Acute kidney injury: acute tubular necrosis vs. prerenal uraemia |
|
|
|
|
HELLP syndrome is a severe form of |
pre-eclampsia |
|
|
|
HELLP syndrome is a severe form of pre-eclampsia whose features include: |
Haemolysis (H), elevated liver enzymes (EL), and low platelets (LP) |
|
|
|
HELLP syndrome typical patient might present with |
malaise, nausea, vomiting, and headache. Hypertension with proteinuria is a common finding, as well as epigastric and/or upper abdominal pain. |
|
|
|
Intrahepatic cholestasis of pregnancy |
pruritus bilirubin < 100 occurs in 2nd and 3rd trimester |
|
|
|
A 28 year old male smoker comes in complaining of an acute onset of excruciating pain on the left side of his head, he says that this is the 4th time this week. He states that it is non-throbbing and denies any visual disturbances or aura's. On examination there is profuse rhinorrhoea, as well as lacrimation and eyelid swelling on the left side. On closer inspection it is also noticed that the patient has partial left-sided ptosis and miosis. On further investigation the patient states that both himself and his father usually experience this pain every 2 years or so. What is the most likely diagnosis? |
Cluster headache |
|
|
|
Cluster headache risk factors |
young male smoker with a positive family history |
|
|
|
can you get horners syndrome like fxs in cluster headache |
yes mainly - rhinorrhoea, nasal congestion and lacrimation also +- ptosis and myosis |
|
|
|
The absence of visual disturbances such as blurring of vision / photophobia makes acute closed angle glaucoma less likely |
true |
|
|
|
Although it is possible to have migraines without aura, the non-throbbing nature of the pain makes this diagnosis |
less likely |
|
|
|
The unilateral pain distribution would be inconsistent with a typical tension headache - which would be described as more of a 'tight band' around the head. |
true |
|
|
|
The acute onset as well as the 2-yearly recurrence make the presence of a brain tumour less likely. |
true |
|
|
|
Cluster headache fxs |
pain typical occurs once or twice a day, each episode lasting 15 mins - 2 hours' clusters typically last 4-12 weeks intense pain around one eye (recurrent attacks 'always' affect same side) patient is restless during an attack accompanied by redness, lacrimation, lid swelling nasal stuffiness miosis and ptosis in a minority |
|
|
|
Management cluster headache |
acute: 100% oxygen, subcutaneous or a nasal triptan prophylaxis: verapamil, prednisolone NICE recommend seeking specialist advice from a neurologist if a patient develops cluster headaches with respect to neuroimaging |
|
|
|
A 9-year-old boy who is having an asthma attack is brought to surgery. Which one of the following findings would be categorise the asthma attack as life-threatening, rather than just severe, according to the British Thoracic Society guidelines? |
Peak flow 30% of best |
|
|
|
A 29-year-old pregnant woman is diagnosed as having gestational diabetes at 22 weeks gestation. Which one of the following complications is she at an increased risk of developing? |
Polyhydramnios |
|
|
|
Pregnancy: diabetes - maternal complications |
polyhydramnios - 25%, possibly due to fetal polyuria preterm labour - 15%, associated with polyhydramnios |
|
|
|
Pregnancy: diabetes - neonatal complications |
macrosomia (although diabetes may also cause small for gestational age babies) hypoglycaemia (secondary to beta cell hyperplasia) respiratory distress syndrome: surfactant production is delayed polycythaemia: therefore more neonatal jaundice malformation rates increase 3-4 fold e.g. sacral agenesis, CNS and CVS malformations (hypertrophic cardiomyopathy) stillbirth hypomagnesaemia hypocalcaemia shoulder dystocia (may cause Erb's palsy) |
|
|
|
A baby boy born 6 hours ago has an APGAR score of 10. He is not cyanosed, has a pulse of 140, cries on stimulation, his arms and legs resist extension and he has a good cry, He appears jaundiced. What is the most appropriate action? |
Measure and record the serum bilirubin level urgently. |
|
|
|
in babies suspected or who have obvious jaundice |
Measure and record the serum bilirubin level urgently (within 2 hours) in the first 24 hours of life since this is likely to be pathological rather than physiological jaundice |
|
|
|
Jaundice in the first 24 hrs of life is always pathological |
TRUE |
|
|
|
Causes of jaundice in the first 24 hrs |
rhesus haemolytic disease ABO haemolytic disease hereditary spherocytosis glucose-6-phosphodehydrogenase |
|
|
|
Jaundice in the neonate from 2-14 days is |
common (up to 40%) and usually physiological. more commonly seen in breast fed babies |
|
|
|
Jaundice in the newborn period If there are still signs of jaundice after 14 days a prolonged jaundice screen is performed, COMPRISING: |
conjugated and unconjugated bilirubin: direct antiglobulin test (Coombs' test) TFTs FBC and blood film urine for MC&S and reducing sugars U&Es and LFTs |
|
|
|
IN THE PROLONGED JAUNDICE SCREEN whats the most important test |
onjugated and unconjugated bilirubin: the most important test as a raised conjugated bilirubin could indicate biliary atresia which requires urgent surgical intervention |
|
|
|
Causes of prolonged jaundice |
biliary atresia hypothyroidism galactosaemia urinary tract infection breast milk jaundice congenital infections e.g. CMV, toxoplasmosis |
|
|
|
Jaundice in the newborn period |
first 24 hrs = pathological ALWAYS day 2-14 = usu physiological >14 days (prolonged jaundice) = can be path. |
|
|
|
pleural effusion, which one of the following is the most important factor when determining whether a chest tube is placed? |
pH of the pleural fluid |
|
|
|
The British Thoracic Society (BTS) state that the following are the main indications for placing a chest tube in pleural infection: |
frankly purulent or turbid/cloudy pleural fluid non purulent pleural fluid with +ve for gram stain bact. pH < 7.2 + pleural infxn |
|
|
|
Pleural effusion: investigation |
Imaging pleural aspiration - lights criteria: transduate/exudate diagnostic pleural fluid sampling |
|
|
|
imaging for pleural effusion |
all should get PA CXR US - for aspiration and id septations, less complications |
|
|
|
Pleural aspiration |
US guide = less complications 21G needle and 50ml syringe should be used |
|
|
|
Pleural aspiration fluid should be sent for |
pH, protein, lactate dehydrogenase (LDH), cytology and microbiology |
|
|
|
Light's criteria was developed in 1972 to help distinguish between a transudate and an exudate. The BTS recommend using the criteria for borderline cases: |
protein level of >30 g/L = exudate protein level of < 30 g/L = transudate An exudate is likely if at least one of the following criteria are met: pleural fluid protein divided by serum protein >0.5 pleural fluid LDH divided by serum LDH >0.6 pleural fluid LDH more than two-thirds the upper limits of normal serum LDH |
|
|
|
all patients with a pleural effusion in association with sepsis or a pneumonic illness require diagnostic pleural fluid sampling |
true |
|
|
|
Other characteristic pleural fluid findings: |
low glucose: rheumatoid arthritis, tuberculosis raised amylase: pancreatitis, oesophageal perforation heavy blood staining: mesothelioma, pulmonary embolism, tuberculosis |
|
|
|
Which one of the following statements regarding hyperemesis gravidarum is correct? |
Wernicke's encephalopathy is a recognised complication |
|
|
|
Hyperemesis gravidarum describes |
excessive vomiting during pregnancy. thought to be related to raised beta hCG levels |
|
|
|
Hyperemesis gravidarum is most common between 8 and 12 weeks but may persist up to 20 weeks*. |
true |
|
|
|
Hyperemesis gravidarum associations |
multiple pregnancies trophoblastic disease hyperthyroidism nulliparity obesity |
|
|
|
Hyperemesis gravidarum Smoking is associated with a decreased incidence of hyperemesis |
true |
|
|
|
Hyperemesis gravidarum mgmt |
antihistamines should be used first-line (BNF suggests promethazine as first-line) admission may be needed for IV hydration |
|
|
|
Hyperemesis gravidarum complications |
Wernicke's encephalopathy Mallory-Weiss tear central pontine myelinolysis acute tubular necrosis fetal: small for gestational age, pre-term birth |
|
|
|
Acromioclavicular joint injury moa |
fall on to the shoulder or a FOOSH (falls on outstretched hand). AC joint injuries are graded I to VI depending on the degree of separation. Grade I and II injuries are very common and are typically managed conservatively including resting the joint using a sling. grade 3 up to dr Grade IV, V and VI are rare and require surgical intervention. |
|
|
|
A 6-year-old boy is brought to surgery by his mother. For the past 2 months he has been complaining of pain in his shins and ankles at night-time. His symptoms are bilateral he is otherwise well. There is no family history of note. Clinical examination is unremarkable. What is the most likely diagnosis? |
Growing pains |
|
|
|
Growing pains |
common GP complaint leg pain with no obvious cause if no other fxs = growing pains |
|
|
|
Growing painsis a misnomer |
as the pains are often not related to growth - the current term used in rheumatology is 'benign idiopathic nocturnal limb pains of childhood' |
|
|
|
Growing pains are equally common in boys and girls and occur in the age range of |
3-12 years |
|
|
|
Features of growing pains |
never present at the start of the day after the child has woken no limp no limitation of physical activity systemically well normal physical examination motor milestones normal symptoms are often intermittent and worse after a day of vigorous activity |
|
|
|
A 7-year-old child is brought to surgery by her father after he collected her from school. She was unwell in the morning with a fever and cough but has become gradually worse during the day. His father is panicked because he has noticed a red rash on her legs which doesn't blanch following the 'tumbler test'. The girl is now also complaining of a headache and cool hands and feet. On examination she has a petechial rash on her lower legs and is pyrexial with a temperature of 38.4ºC. Her father reports she is allergic to penicillin. On reviewing the records you note she developed a rash and vomiting after been given amoxicillin for otitis media 4 years ago. What is the most appropriate next step? |
Phone 999 + administer intramuscular benzylpenicillin |
|
|
|
7 yo px with meningococcal septicaemia, has a pmhx of allergy to pencilin with vomiting and rash what is the mgmt |
Phone 999 + administer intramuscular benzylpenicillin |
|
|
|
is a pmhx of allergy to penicillin with a rash and vomiting CI for benzylpenicillinmeningococcal septicaemia |
NO, only anaphylaxis is a rash and vomiting is not anaphylaxis |
|
|
|
Withhold benzylpenicillin only in children and young people who have a clear history of anaphylaxis after a previous dose; a history of a rash following penicillin is not a contraindication. |
true |
|
|
|
Presentation of meningococcal disease: |
15% - meningitis 25% - septicaemia 60% - a combination of meningitis and septicaemia |
|
|
|
Meningococcal septicaemia |
is the leading infectious cause of death in early childhood. |
|
|
|
Meningococcal septicaemiamore specific symptoms/signs |
Non-blanching rash, altered mental state, capillary refill time more than 2 seconds, unusual skin colour, shock, hypotension, leg pain, cold hands/feet |
|
|
|
A 65-year-old female with a history of ischaemic heart disease is noted to be depressed following a recent myocardial infarction. What would be the most appropriate antidepressant to start? |
Sertraline |
|
|
|
SSRI are first line for |
depression |
|
|
|
SSRI |
citalopram fluoxetine sertraline |
|
|
|
in children and adolescents, what is the drug of choice |
fluoxetine |
|
|
|
What SSRI are preferred in depression |
citalopram (ae = LONG QT) fluoxetine |
|
|
|
what SSRI is preferred in depression for a px post MI |
sertraline |
|
|
|
most common AE of SSRI |
gastrointestinal symptoms are the most common side-effect |
|
|
|
SSRI interactions |
NSAIDs warfarin / heparin aspirin triptans |
|
|
|
when should you monitor SSRI for depression |
after 2 weeks starting <30yo = after 1 week (cuz up risk of suicide) good response = continue for 6 months |
|
|
|
For patients under the age of 30 years or at increased risk of suicide they should be reviewed after 1 week |
true |
|
|
|
When stopping a SSRI the dose should be gradually reduced over a 4 week period (this is not necessary with fluoxetine). Paroxetine has a higher incidence of discontinuation symptoms. |
Discontinuation symptoms increased mood change restlessness difficulty sleeping unsteadiness sweating gastrointestinal symptoms: pain, cramping, diarrhoea, vomiting paraesthesia |
|
|
|
A 54-year-old man is investigated for a chronic cough. A chest x-ray arranged by his GP shows a suspicious lesion in the right lung. He has no past history of note and is a life-long non-smoker. An urgent bronchoscopy is arranged which is normal. What is the most likely diagnosis? |
Lung adenocarcinoma |
|
|
|
Lung adenocarcinoma |
most common type in non-smokers peripheral lesion |
|
|
|
There are three main subtypes of non-small cell lung cancer: |
Squamous cell cancer Adenocarcinoma Large cell lung carcinoma |
|
|
|
Lung cancer: non-small cell Squamous cell cancer |
typically central associated with parathyroid hormone-related protein (PTHrP) secretion → hypercalcaemia strongly associated with finger clubbing hypertrophic pulmonary osteoarthropathy (HPOA) |
|
|
|
Lung cancer: non-small cell Adenocarcinoma |
typically peripheral most common type of lung cancer in non-smokers, although the majority of patients who develop lung adenocarcinoma are smokers |
|
|
|
Lung cancer: non-small cell Large cell lung carcinoma |
typically peripheral anaplastic, poorly differentiated tumours with a poor prognosis may secrete β-hCG |
|
|
|
Daniel is a newborn who is having his baby check done by nurse Karen, who notices that he has microcephaly with a prominent occiput, low set ears, micrognathia, palpebral fissures and wide spaced eyes. What genetic disorder are these features suggestive of? |
Edward's syndrome |
|
|
|
Edward's syndrome can also have: |
Ptosis Rocker bottom feet Undescended testes |
|
|
|
Physical features of Down's syndrome include having a |
small chin, slanted eyes, flat nasal bridge and single palmar creases. |
|
|
|
Turner's syndrome presents with a |
webbed neck, short stature and low set ears can only affect females |
|
|
|
Noonan syndrome presents with |
mainly skeletal characteristics, such as short stature, scoliosis, pectus carinatum and excavatum, winging of the scapula and joint hypermobility, among others |
|
|
|
Angelman syndrome is a condition which greatly affects functioning and behaviour, meaning these are the most prominent features. Some physical attributes can be present, including |
microcephaly, hypopigmented skin and eyes, prominent mandible and wide mouth. |
|
|
|
T4 Nipples |
T4 at the Teat Pore |
|
|
|
T10 Umbilicus |
BellybuT-TEN |
|
|
|
L1 Inguinal ligament |
L for ligament, 1 for 1nguinal |
|
|
|
L4 Knee caps |
Down on aLL fours - L4 |
|
|
|
L5 Big toe, dorsum of foot (except lateral aspect) |
L5 = Largest of the 5 toes |
|
|
|
S1 Lateral foot, small toe |
S1 = the smallest one |
|
|
|
A 39 year-old woman presents to her general practitioner with a grape-sized breast lump that she noticed one week ago whilst in the bath. It is firm and non-tender, with no surrounding skin changes. She feels well in herself with no temperatures, and has no history of breast disease. She stopped breastfeeding one month ago. An ultrasound scan shows a well-circumscribed lesion and aspiration yields a white fluid. What is the likely diagnosis? |
Galactocele |
|
|
|
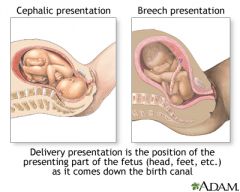
delivery presentations |
|
|
|
|
A 30-year-old woman at 32 weeks gestation presents to the Emergency Department with a small amount of painless vaginal bleeding that came on spontaneously. Obstetric examination finds a cephalic presentation with high presenting part. The uterus is non-tender. The cervical os is closed and the cervix appears normal. Which of the following diagnoses is most likely? |
Placenta praevia |
|
|
|
Placenta praevia refers to |
pathological positioning of the placenta in the lower segment of the uterus, either wholly or partly If the placenta overlies the internal cervical os then this is classed as 'major praevia', whereas in 'minor' or 'partial' praevia it does not. |
|
|
|
Placenta praevia Bleeding from the placenta can occur |
spontaneously, as a result of trauma, or at the onset of labour as the cervix opens. |
|
|
|
Placenta praevia Features that increase suspicion of this condition include |
vaginal bleeding occurring after 20 weeks gestation painless bleeding, high presenting part and abnormal fetal lie |
|
|
|
placental previa dx |
us TO ID POSITION OF PLACENTA |
|
|
|
normal appearance of the cervix can help rule out |
cervical trauma, cervical neoplasm and inevitable miscarriage |
|
|
|
Placenta praevia Associated factors |
multiparity multiple pregnancy embryos are more likely to implant on a lower segment scar from previous caesarean section |
|
|
|
A 48 year old nurse presents with a short history of epistaxis and bleeding gums. You request urgent bloods, the results of which are shown in the table below: Haemoglobin86 g/L White cells2.3 x 10^9/L Platelets18 x 10^9/L Clotting deranged Blood film bilobed large mononuclear cells dx |
Acute myeloid leukaemia |
|
|
|
Lymphoma key fx |
rubbery enlargement of lymph nodes. |
|
|
|
Von Willebrand's disease may present with epistaxis and bleeding gums in severe cases, but it is rare that there are abnormalities on blood results. |
true |
|
|
|
Acute myeloid leukaemia is the more common form of acute leukaemia in adults. It may occur as a |
primary disease or following a secondary transformation of a myeloproliferative disorder. |
|
|
|
Poor prognostic features |
> 60 years > 20% blasts after first course of chemo cytogenetics: deletions of chromosome 5 or 7 |
|
|
|
Acute myeloid leukaemia |
Classification - French-American-British (FAB) |
|
|

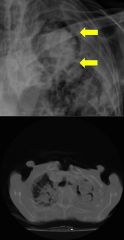
30-year-old woman who presented with a productive cough. dx |
Kartagener syndrome x-ray findings consistent with dextrocardia and bronchiectasis (tram-track opacities). Hyperinflation is also seen in this film. |
|
|
|
Kartagener's syndrome (also known as primary ciliary dyskinesia) most frequently occurs in examinations due to its association with |
dextrocardia (e.g. 'quiet heart sounds', 'small volume complexes in lateral leads') |
|
|
|
Kartagener's syndrome pathogen |
dynein arm defect results in immotile cilia |
|
|
|
Kartagener's syndrome fxs |
dextrocardia or complete situs inversus bronchiectasis recurrent sinusitis subfertility (secondary to diminished sperm motility and defective ciliary action in the fallopian tubes) |
|
|
|
Said is a 32 year old male who has recently emigrated to the UK from Indonesia. He attends his GP practice with regards to symptoms of weight gain, tiredness and hoarseness of voice. Following blood tests, including a thyroid function test, it is found that he has hypothyroidism. What is the most likely cause of hypothyroidism in this patient? |
Iodine deficiency |
|
|
|
Iodine deficiency is the leading cause of |
hypothyroidism in the world, with areas of Africa and Asia (particularly Southeast Asia) being some of the most severely affected. |
|
|
|
Hashimoto's thyroiditis is the most common cause of hypothyroidism in |
countries whose iodine consumption is adequate, generally referring to the developed countries. |
|
|
|
Toxic multinodular goitre is a cause of |
hyperthyroidism, not hypothyroidism |
|
|
|
Patients with thyroid adenomas are generally asymptomatic and are found on clinical examination or self-palpation |
true |
|
|
|
Primary hypothyroidism causes |
thyroid prob Hashimoto's thyroiditis -may cause transient thyrotoxicosis in the acute phase -10 times more common in women |
|
|
|
Secondary hypothyroidism (rare) |
pituitary prob Other associated conditions Down's syndrome Turner's syndrome coeliac disease |
|
|
|
Which one of the following findings in one of the patients would prompt you to start continuous CTG tracing while in labour? |
New onset vaginal bleed while in labour |
|
|
|
As per NICE guidelines; the following would warrant continuous CTG monitoring if any of the following are present or arise during labour; |
suspected chorioamnionitis or sepsis, or a temperature of 38°C or above severe hypertension 160/110 mmHg or aboveoxytocin usethe presence of significant meconiumfresh vaginal bleeding that develops in labour - this was a new point added to the guidelines in 2014 |
|
|
|
chorioamnionitis define |
usu. rupture of membranes due to ascending bact. infxn nb rare but can have the infxn without the rupture |
|
|
|
the most common cause of antepartum haemorrhage is |
placental rupture 2nd = placental previa |
|
|
|
Cardiotocography (CTG) records pressure changes in the uterus using internal or external pressure transducers |
The normal fetal heart rate varies between 110 - 150 / min |
|
|
|
A 66-year-old female starts colchicine to try to settle the symptoms of gout which are not being controlled with diclofenac. What side-effect is it most important to warn her about? |
Diarrhoea |
|
|
|
cholchicine most important AE |
diarrrhoea |
|
|

|
Lung collapse |
|
|
|
A 4-year-old girl is reviewed by her GP due to poor control of asthma. She currently takes a regular steroid inhaler and a salbutamol inhaler as required. What is the next step in management? |
Trial of a leukotriene receptor antagonist |
|
|
|
child < 5yo asthma px on saba and ICS what next |
2-5yo Trial of a leukotriene receptor antagonist (if this fails then refer to resp peds) <2yo refer to resp pediatrician |
|
|
|
Children aged over 5 years (similar to adult guidance) |
true |
|
|
|
Which one of the following is not a risk factor for sudden infant death syndrome? |
Female sex |
|
|
|
risk factor for sudden infant death syndrome? |
Hyperthermia Social classes IV and V Prematurity Bottle feeding |
|
|
|
Sudden infant death syndrome is the commonest cause of death in |
the first year of life. It is most common at 3 months of age |
|
|
|
Sudden infant death syndrome Risk factors |
prematurity parental smoking hyperthermia (e.g. over-wrapping)putting the baby to sleep pronemale sex multiple births bottle feeding social classes IV and V maternal drug use incidence increases in winter |
|
|
|
Why would magnesium sulphate be given to a 18-year-old primigravida at 36 weeks gestation who has had a tonic-clonic seizure during labor? |
Prevention of seizures |
|
|
|
Eclampsia def |
Preeclampsia + Seizures |
|
|
|
Eclampsia tx |
Immediate delivery and magnesium sulphate prevents eclamptic seizures |
|
|
|
pre-eclampsia is defined as: |
condition seen after 20 weeks gestation pregnancy-induced hypertension proteinuria |
|
|
|
Eclampsia Magnesium sulphate is used to |
both prevent seizures in patients with severe pre-eclampsia and treat seizures once they develop |
|
|
|
Magnesium sulphate monitoring |
urine output, reflexes, respiratory rate and oxygen saturations should be monitored during treatment |
|
|
|
in eclampsia how long should you give mg sulphate |
treatment should continue for 24 hours after last seizure or delivery (around 40% of seizures occur post-partum) Other important aspects of treating severe pre-eclampsia/eclampsia include fluid restriction to avoid the potentially serious consequences of fluid overload |
|
|
|
A 34-year-old man with a history of ankylosing spondylitis presents with a painful right eye associated with mild photophobia: Cycloplegic drops have recently been given. What is the most likely diagnosis? |
Anterior uveitis |
|
|
|
Ankylosing spondylitis is associated with what eye prob |
anterior uveitis |
|
|
|
Anterior uveitis |
Anterior uveitis is one of the important differentials of a red eye. It is also referred to as iritis. |
|
|
|
Anterior uveitisAssociated conditions |
ankylosing spondylitis reactive arthritis ulcerative colitis, Crohn's disease Behcet's disease |
|
|
|
anterior uveitis mgmt |
urgent review by ophthalmology cycloplegics (dilates the pupil which helps to relieve pain and photophobia) e.g. Atropine, cyclopentolate steroid eye drops |
|
|
|
A 68-year-old female presents with a two week history of intermittent headaches and lethargy. Blood tests reveal the following:ESR67 mm/hrWhat is the most likely diagnosis? |
Temporal arteritis headache (found in 85%) jaw claudication (65%) |
|
|
|
Temporal arteritis tx |
high-dose prednisolone and urgent ophthalmology review |
|
|
|
A 65-year-old man with a history of ischaemic heart disease is admitted with chest pain. The 12-hour troponin T is negative. During admission his medications were altered to reduce the risk of cardiovascular disease and to treat previously undiagnosed type 2 diabetes mellitus. Shortly after discharge he presents to his GP complaining of diarrhoea. Which one of the following medications is most likely to be responsible? |
Metformin |
|
|
|
Gastrointestinal problems are a common side-effect of many medications but are frequently seen in patients taking |
metformin |
|
|
|
For a patient undergoing an elective splenectomy, when is the optimal time to give the pneumococcal vaccine? |
Two weeks before surgery |
|
|
|
Following a splenectomy patients are particularly at risk from |
pneumococcus, Haemophilus, meningococcus and Capnocytophaga canimorsus* infections nb Capnocytophaga canimorsus* usu from dog bites |
|
|
|
SplenectomyVaccination |
if elective, should be done 2 weeks prior to operation Hib, meningitis A & C annual influenza vaccination pneumococcal vaccine every 5 years |
|
|
|
Splenectomy
Antibiotic prophylaxis |
penicillin V generally accepted though that penicillin should be continued for at least 2 years and at least until the patient is 16 years of age, although the majority of patients are usually put on antibiotic prophylaxis for life |
|
|
|
A 48-year-old man presents with a 'droopy eyelid' on the right side. You also notice that his right pupil appears smaller than the left: dx |

Horner's syndrome |
|
|
|
Horner's syndrome Distinguishing between causes |
heterochromia (difference in iris colour) is seen in congenital Horner's anhydrosis: see below |
|
|
|
Horner's syndrome Central lesions |
Anhydrosis of the face, arm and trunk causes = Stroke Syringomyelia Multiple sclerosis Tumour Encephalitis |
|
|
|
Horner's syndrome Pre-ganglionic lesions |
Anhydrosis of the face Causes Pancoast's tumour Thyroidectomy Trauma Cervical rib |
|
|
|
Horner's syndrome Post-ganglionic lesions |
No anhydrosis Carotid artery dissection Carotid aneurysm Cavernous sinus thrombosis Cluster headache |
|
|
|
A 44-year-old farmer presents with headache, fever and muscle aches. He initially thought he had a bad cold but his symptoms have got progressively worse over the past week. During the review of systems he reports nausea and a decreased urine output. On examination his temperature is 38.2ºC, pulse 102 / min and his chest is clear. Subconjunctival haemorrhages are noted but there is no evidence of jaundice. What is the most likely diagnosis? |
Leptospirosis The main clue in the question is the patients occupation. Mycoplasma and Legionella are less likely due to the absence of chest symptoms and signs. Liver failure is seen in only 10% of patients with leptospirosis.. |
|
|
|
Leptospirosis also known as |
Weil's disease*, leptospirosis is commonly seen in questions referring to sewage workers, farmers, vets or people who work in abattoir |
|
|
|
Leptospirosis |
It is caused by the spirochaete Leptospira interrogans (serogroup L icterohaemorrhagiae), classically being spread by contact with infected rat urine. Weil's disease should always be considered in high-risk patients with hepatorenal failure |
|
|
|
Leptospirosis fxs |
fever flu-like symptoms renal failure (seen in 50% of patients) jaundice subconjunctival haemorrhage headache, may herald the onset of meningitis |
|
|
|
Leptospirosis mgmt |
high-dose benzylpenicillin or doxycycline |
|
|
|
You are discussing conception with two parents who both have achondroplasia. They ask you what the chances are that a child of theirs would be of normal height. What is the correct response? |
25% Many questions relating to autosomal dominant conditions are based around one of the parents being affected. With achondroplasia both parents are often affected which can make the interpretation slightly trickier. |
|
|
|
As an autosomal dominant condition, two affected parents can expect: |
1 in 4 chance of an unaffected child 1 in 2 chance of an affected heterozygous child 1 in 4 chance of an affected homozygous child. With achondroplasia children unfortunately don't live past the first few months of life |
|
|
|
Achondroplasia is an autosomal dominant disorder associated with |
short stature |
|
|
|
chondroplasia is an autosomal dominant disorder associated with short stature. It is caused by |
mutation in the fibroblast growth factor receptor 3 (FGFR-3) gene |
|
|
|
Achondroplasia is an autosomal dominant disorder associated with short stature. It is caused by a mutation in the fibroblast growth factor receptor 3 (FGFR-3) gene. This results in abnormal cartilage giving rise to: |
short limbs (rhizomelia) with shortened fingers (brachydactyly) large head with frontal bossing midface hypoplasia with a flattened nasal bridge 'trident' hands lumbar lordosis |
|
|
|
A team evaluating a new screening test for ovarian cancer present evidence that its use improves survival time. However, critics of their research say that the apparent increased length of survival time is just due to cases being identified earlier rather than a true improvement. This in an example of what kind of bias? |
Lead time bias |
|
|
|
A 4-year-old boy is reviewed in the Paediatric Admissions Unit. He has had a fever for the past week. On examination he has red, sore lips and conjunctival injection. He also has swollen, red hands. Blood tests show:Hb13.1 g/dlWBC12.7 *109/lPlatelets520 *109/lCRP96 mg/LWhat is the likely diagnosis? |
Kawasaki disease |
|
|
|
Kawasaki diseasepotentially serious complications, including |
high-grade fever which lasts for > 5 days. Fever is characteristically resistant to antipyretics conjunctival injection bright red, cracked lips strawberry tongue cervical lymphadenopathy red palms of the hands and the soles of the feet which later peel |
|
|
|
ManagementKawasaki disease |
high-dose aspirin* intravenous immunoglobulin echocardiogram (rather than angiography) is used as the initial screening test for coronary artery aneurysms |
|
|
|
Kawasaki diseaseComplications |
coronary artery aneurysm Kawasaki disease is one of the few indications for the use of aspirin in children. Due to the risk of Reye's syndrome aspirin is normally contraindicated in children. |
|
|
|
A 34-year-old female presents due to a number of 'funny-dos'. She describes a sensation that her surroundings are unreal, 'like a dream'. Following this she has been told that she starts to smack her lips, although she has no recollection of doing this. What is the most likely diagnosis? |
Complex partial seizure |
|
|
|
With simple partial seizures there is no disturbance of |
consciousness or awareness |
|
|
|
Lip smacking is an example of an automatism - an automatic, repetitive act |
true |
|
|
|
Epilepsy: classification basics |
two main categories are generalised and partial seizures partial seizures may progress to general seizures other types: myoclonic, atypical absence, atonic and tonic seizures are usually seen in childhood |
|
|
|
Epilepsy: classification Generalised - no focal features, consciousness lost immediately |
grand mal (tonic-clonic) petit mal (absence seizures) myoclonic: brief, rapid muscle jerks partial seizures progressing to generalised seizures |
|
|
|
Epilepsy: classification Partial - focal features depending on location |
simple (no disturbance of consciousness or awareness) complex (consciousness is disturbed) temporal lobe → aura, déjà vu, jamais vu; motor → Jacksonian |
|
|
|
which one of the following clinical signs is most commonly found in patients with a pulmonary embolism? |
Tachypnoea |
|
|

dx |
Left-sided pneumothorax (no tension) |
|
|
|
A 30-year-old man comes to surgery. He has been handed a slip from an ex-girlfriend stating she has tested positive for Chlamydia. He last slept with her 2 months ago. He has no symptoms of note, in particular no dysuria or discharge. What is the most appropriate management? |
Offer Chlamydia testing and antibiotic treatment immediately without waiting for the results Treatment is given on the basis of exposure to infection rather than proven infection |
|
|
|
. Which of the following adverse effects do antipsychotics increase the risk of in elderly patients? |
Stroke |
|
|
|
Antipsychotics in the elderly - increased risk of |
stroke and VTE |
|
|
|
A 6-year-old boy is reviewed in clinic due to nocturnal enuresis. His mother has tried using a star-chart but unfortunately this has not resulted in any significant improvement. Of the following options, what is the most appropriate initial management strategy? |
Enuresis alarm 'Do not restrict fluids. The child should have about eight drinks a day, spaced out throughout the day, the last one about 1 hour before bed.' |
|
|
|
The majority of children achieve day and night time continence by |
3 or 4 years of age |
|
|
|
Enuresis may be defined as the |
'involuntary discharge of urine by day or night or both, in a child aged 5 years or older, in the absence of congenital or acquired defects of the nervous system or urinary tract' |
|
|
|
Nocturnal enuresis can be defined as either primary (the child has never achieved continence) or secondary (the child has been dry for at least 6 months before) |
true |
|
|
|
an enuresis alarm is first-line for children under the age of 7 years |
true |
|
|
|
desmopressin may be used first-line for children over the ago 7 years, particularly if short-term control is needed or an enuresis alarm has been ineffective/is not acceptable to the family |
true |
|
|
|
enuresis mgmt |
stop any triggers/causes educate on fluid intake, diet and toilet behavior reward systems enuresis alarm desmopressin >7yo = 1st line |
|
|
|
A 2-month-old baby girl is admitted to hospital with suspected meningitis. Her parents describe her becoming pyrexial and drowsy over the past 24 hours. On examination her temperature is 39.2ºC, heart rate is 160/min and respiratory rate is 50.min. Her anterior fontanelle is bulging. No petechial rash is seen. In addition to cefotaxime, what antibiotic should be given intravenously? |
Amoxicillin |
|
|
|
Meningitis in children < 3 months: give |
IV amoxicillin in addition to cefotaxime to cover for Listeria |
|
|
|
Contraindication to lumbar puncture (any signs of raised ICP) |
focal neurological signs papilloedema significant bulging of the fontanelle disseminated intravascular coagulation signs of cerebral herniation |
|
|
|
For patients with meningococcal septicaemia lumbar puncture is |
contraindicated - blood cultures and PCR for meningococcus should be obtained |
|
|
|
Meningitis in children 1. Antibiotics |
< 3 months: IV amoxicillin + IV cefotaxime > 3 months: IV cefotaxime |
|
|
|
Meningitis in childrenManagement 2. Steroids |
if > 1 month and Haemophilus influenzae then give dexamethasone |
|
|
|
Meningitis in childrenManagement 3. Fluids |
treat any shock, e.g. with colloid |
|
|
|
Meningitis in children 4. Cerebral monitoring |
mechanical ventilation if respiratory impairment |
|
|
|
Meningitis in children 5. Public health notification and antibiotic prophylaxis of contacts |
rifampicin |
|
|
|
A 30 year-old lady with a diagnosis of asthma is reviewed in general practice. She is currently taking a salbutamol inhaler as required along with inhaled corticosteroid 200micrograms twice a day.After a recent review she had been prescribed salmeterol 100µg twice a day. There was some improvement with this but she is currently continuing to require her salbutamol inhaler 2-6 times/day.Which of the following medication adjustments is the most appropriate? |
Increase regular inhaled steroid dose |
|
|
|
A 26-year-old woman presents to the sexual health clinic with a 2 week history of purulent vaginal discharge. Microscopy of an endocervical swab sample shows Gram-negative diplococci. Tests for other pathogens are negative. The patient has no comorbidities or allergies. Which of the following antibiotic choices is most appropriate? |
Azithromycin + ceftriaxone |
|
|
|
The combination of purulent discharge and endocervical Gram-negative diplococci indicates a diagnosis of |
gonorrhoea |
|
|
|
overview of some STI and meds |
Doxycycline is an appropriate choice for chlamydia or syphilis, metronidazole is recommended for bacterial vaginosis, benzylpenicillin is used in treating syphilis, and erythromycin can be used to treat chlamydia. |
|
|
|
Gonorrhoea Features |
males: urethral discharge, dysuria females: cervicitis e.g. leading to vaginal discharge rectal and pharyngeal infection is usually asymptomatic |
|
|
|
Gonorrhoea tx of choice |
ceftriaxone IM as a single dose with azithromycin oral |
|
|
|
complications of gonorrhoea |
Disseminated gonococcal infection (DGI) and gonococcal arthritis may also occur, with gonococcal infection being the most common cause of septic arthritis in young adults. Initially there may be a classic triad of symptoms: tenosynovitis, migratory polyarthritis and dermatitis. Later complications include septic arthritis, endocarditis and perihepatitis (Fitz-Hugh-Curtis syndrome) |
|
|
|
Initially there may be a classic triad of symptoms: |
tenosynovitis, migratory polyarthritis and dermatitis |
|
|
|
Key features of disseminated gonococcal infection |
tenosynovitis migratory polyarthritis dermatitis (lesions can be maculopapular or vesicular) |
|
|
|
A nurse informs you of a 30 year old woman who is 38 weeks pregnant. She says that the patient has a blood pressure reading of 155/90 mmHg. Her previous blood pressure 2 days ago was 152/85 mmHg. A 24 hour urine collection is requested which shows a urinary protein excretion of 0.7g / 24 hours. She was previously healthy prior to becoming pregnant. After giving her oral labetalol, what is the next line management in this situation? |
Plan delivery of the foetus within 48 hours |
|
|
|
According to the current guidelines, pregnant women who have mild or moderate gestational hypertension, are more than 37 week pregnant, and are showing signs of pre-eclampsia, should be recommended to |
give birth within 24 - 48 hours. |
|
|
|
she has antiphospholipid syndrome but no other past medical history. This is her first pregnancy. What medication should be started from 12 weeks' gestation until birth? |
Aspirin |
|
|
|
Antiphospholipid syndrome is an |
autoimmune disorder which predisposes patients to venous and arterial thrombosis |
|
|
|
Antiphospholipid syndrome is associated with various problems in pregnancy, including |
intrauterine growth restriction and pre-eclampsia |
|
|
|
It is thought that antiphospholipid syndrome can cause pre-eclampsia when a thrombus forms in one of the umbilical vessels. |
true |
|
|
|
A 72-year-old man presents with a painful, red eye to the Emergency Department. Due to the severity of his symptoms and reduced visual acuity he is referred on to ophthalmology who make a diagnosis of acute glaucoma. Which of the following should be the aims of treatment? |
Reducing aqueous secretion + inducing pupillary constriction |
|
|
|
Glaucoma is a group disorders characterised by |
optic neuropathy due, in the majority of patients, to raised intraocular pressure (IOP) nb It is now recognised that a minority of patients with raised IOP do not have glaucoma and vice versa |
|
|
|
In acute angle closure glaucoma (AACG) there is a rise in IOP secondary to |
an impairment of aqueous outflow. |
|
|
|
Factors predisposing to AACG include: |
hypermetropia (long-sightedness) pupillary dilatation lens growth associated with age |
|
|
|
Acute angle closure glaucoma fxs |
severe pain: may be ocular or headache decreased visual acuity symptoms worse with mydriasis (e.g. watching TV in a dark room) hard, red eye haloes around lights semi-dilated non-reacting pupil corneal oedema results in dull or hazy cornea systemic upset may be seen, such as nausea and vomiting and even abdominal pain |
|
|
|
Acute angle closure glaucoma mgmt |
urgent referral to an ophthalmologist management options include reducing aqueous secretions with acetazolamide and inducing pupillary constriction with topical pilocarpine |
|
|
|
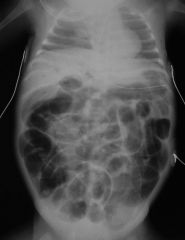
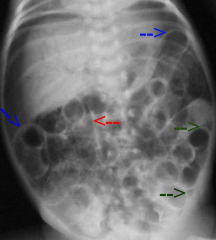
Henry is a 29 week premature baby who was born 2 weeks ago. Over the past week it has been noted that he has had bloody stool, abdominal distension and has not been feeding well. Physical examination reveals an increased abdominal girth with reduced bowel sounds. Abdominal X-ray shows dilated asymmetrical bowel loops and bowel wall oedema. What is the likely diagnosis? |
Necrotising enterocolitis |
|
|
|
Necrotising enterocolitis is one of the leading causes of |
death among premature infants |
|
|
|
Necrotising enterocolitis initial symptoms can include |
feeding intolerance, abdominal distension and bloody stools, which can quickly progress to abdominal discolouration, perforation and peritonitis. |
|
|
|
Abdominal x-rays are useful when diagnosing necrotising enterocolitis, as they can show: |
dilated bowel loops (often asymmetrical in distribution) bowel wall oedema pneumatosis intestinalis (intramural gas) portal venous gas pneumoperitoneum resulting from perforation air both inside and outside of the bowel wall (Rigler sign) air outlining the falciform ligament (football sign) |
|
|
|
Inflammatory bowel disease is unlikely to affect an infant as young |
true |
|
|
|
whats more likely in premature infants hirschsprungs dis or necrotising enterocolitis |
nec. enterocolitis |
|
|
nec. enterocolitis |
nec. enterocolitis |
|
|
|
You see a worried mum with her 6 month old baby boy. She is concerned that his skull shape is not normal. His development and birth have been normal and there are no conditions in the family. On examination his head circumference is at the 40th centile with his height and weight at the 30th centile. His occiput is flattened on the left, his left ear mildly protruding forward and his left forehead more prominent than the right. No other abnormality is detected. What is the most appropriate management? |
Reassurance |
|
|
|
His occiput is flattened on the left, his left ear mildly protruding forward and his left forehead more prominent than the right dx |
Plagiocephaly |
|
|
|
Plagiocephaly |
is more common since there have been campaigns to encourage babies to sleep on their back to reduce the risk of sudden infant death syndrome (SIDS) |
|
|
|
Plagiocephaly is a skull deformity producing unilateral occipital flattening, which pushes the ipsilateral forehead ear forwards producing a 'parrallelogram' appearance. |
true |
|
|
|
Plagiocephalyvast majority improve by age 3-5 due to the adoption of a |
more upright posture Turning the cot around may help the child look the other way and take the pressure off the one side. Other simple methods include giving the baby time on their tummy during the day, supervised supported sitting during the day, and moving toys/ mobiles around in the cot to change the focus of attention. Ensure all advice is in line with prevention of SIDS. |
|
|
|
Skull problems in children |
Plagiocephaly Craniosynostosis |
|
|
Plagiocephaly |
parallelogram shaped head the incidence of plagiocephaly has increased over the past decade. This may be due to the success of the 'Back to Sleep' campaign |
|
|
|
Craniosynostosis |
premature fusion of skull bones |
|
|
|
Which one of the following features is least consistent with Trichomonas vaginalis |
Vaginal pH < 4.5 |
|
|
|
Trichomonas vaginalis + bacterial vaginosis are associated with |
a pH > 4.5 |
|
|
|
Trichomonas vaginalis is a highly motile, flagellated protozoan parasite Features |
vaginal discharge: offensive, yellow/green, frothy vulvovaginitis strawberry cervix pH > 4.5 in men is usually asymptomatic but may cause urethritis |
|
|
|
Trichomonas vaginalisInvestigation |
microscopy of a wet mount shows motile trophozoites |
|
|
|
Trichomonas vaginalisManagement |
oral metronidazole |
|
|
|
A 57-year-old woman presents with a three month history of right-sided hip pain. This seems to have come on spontaneously without any obvious precipitating event. The pain is described as being worse on the 'outside' of the hip and is particularly bad at night when she lies on the right hand side.On examination there is a full range of movement in the hip including internal and external rotation. Deep palpation of the lateral aspect of the right hip joint recreates the pain.An x-ray of the right hip is reported as follows:Right hip: Minor narrowing of the joint space otherwise normal appearanceWhat is the most likely diagnosis? |
Greater trochanteric pain syndrome |
|
|
|
Greater trochanteric pain syndrome is now the preferred term for |
trochanteric bursitis. Whilst the x-ray shows joint space narrowing this is not an uncommon finding. Osteoarthritis would also be less likely given the palpable nature of the pain and relatively short duration of symptoms. |
|
|
|
Referred lumbar spine pain |
Femoral nerve compression may cause referred pain in the hip Femoral nerve stretch test may be positive - lie the patient prone. Extend the hip joint with a straight leg then bend the knee. This stretches the femoral nerve and will cause pain if it is trapped |
|
|
|
Greater trochanteric pain syndrome (Trochanteric bursitis) |
Due to repeated movement of the fibroelastic iliotibial band Pain and tenderness over the lateral side of thigh Most common in women aged 50-70 years |
|
|
|
Meralgia paraesthetica |
Caused by compression of lateral cutaneous nerve of thigh Typically burning sensation over antero-lateral aspect of thigh |
|
|
|
Pubic symphysis dysfunction |
Common in pregnancy Ligament laxity increases in response to hormonal changes of pregnancy Pain over the pubic symphysis with radiation to the groins and the medial aspects of the thighs. A waddling gait may be seen |
|
|
|
Transient idiopathic osteoporosis |
An uncommon condition sometimes seen in the third trimester of pregnancy Groin pain associated with a limited range of movement in the hip Patients may be unable to weight bear ESR may be elevated |
|
|
|
BMI = weight (kg) / height (m) squared |
BMI = weight (kg) / height (m) squared |
|
|
|
BMI |
Underweight < 18.49 Normal 18.5 - 25 Overweight 25 - 30 Obese class 1 30 - 35 Obese class 2 35 - 40 Obese class 3 > 40 |
|
|
|
A 29-year-old man presents to the Emergency Department with dyspnoea. He has no past medical history of note other than a fractured ankle five months ago. On examination he has reduced breath sounds on the left side. The trachea is central and oxygen saturations are 98% on room air. A chest x-ray shows a pneumothorax on the left-side with a 3.5cm rim of air. There is no midline shift. What is the most appropriate initial management? |
Aspiration |
|
|
|
chest x-ray shows a pneumothorax on the left-side with a 3.5cm rim of air. There is no midline shift. What is the most appropriate initial management? |
Aspiration |
|
|
|
A 28-year-old man is diagnosed with having ankylosing spondylitis. He presented with a six month history of back pain. On examination there is reduced lateral flexion of the spine but no evidence of any other complications. Which one of the following is he most likely to offered as first-line treatment? |
Exercise regime + NSAIDs |
|
|
|
can you use anti-TNF drugs in AS |
YES The anti-TNF drugs are currently only used for patients with severe ankylosing spondylitis which has failed to respond to NSAIDs. |
|
|
|
Which one of the following is not associated with thrombophilia? |
von Willebrand's disease |
|
|
|
Thrombophilia: causes Inherited OR Acquired |
Inherited activated protein C resistance (factor V Leiden): most common cause antithrombin III deficiency protein C deficiency protein S deficiency Acquired antiphospholipid syndrome the Pill |
|
|
|
A 79-year-old man presents with a history of lower back pain and right hip pain. Blood tests reveal the following:Calcium2.20 mmol/lPhosphate0.8 mmol/lALP890 u/LWhat is the most likely diagnosis? |
Paget's disease |
|
|
|
Paget's disease |
old man, bone pain, raised ALP The normal calcium and phosphate combined with a raised alkaline phosphate points to a diagnosis of Paget's |
|
|
|
Paget's disease of the bone Predisposing factors |
increasing age male sex northern latitude family history |
|
|
|
Paget's disease of the bone Clinical features - only 5% of patients are symptomatic |
bone pain (e.g. pelvis, lumbar spine, femur) classical, untreated features: bowing of tibia, bossing of skull raised alkaline phosphatase (ALP) - calcium* and phosphate are typically normal skull x-ray: thickened vault, osteoporosis circumscripta |
|
|
|
Paget's disease of the bone indications for tx |
bone pain, skull or long bone deformity, fracture, periarticular Paget's |
|
|
|
Paget's disease of the bone tx |
bisphosphonate (either oral risedronate or IV zoledronate) |
|
|
|
Paget's disease of the boneComplications |
deafness (cranial nerve entrapment) bone sarcoma (1% if affected for > 10 years) fractures skull thickening high-output cardiac failure |
|
|
|
A 20-year-old student drinks around 500 ml of vodka at a party. The next morning he feels thirsty and finds he is passing more urine than normal. Which one of the following best explains why people who drink excessive amounts alcohol develop polyuria? |
Ethanol inhibits ADH secretion |
|
|
|
Ethanol reduces the calcium-dependent secretion of |
anti-diuretic hormone (ADH) by blocking channels in the neurohypophyseal nerve terminal. |
|
|
|
Nausea associated with hangovers is mainly due to |
vagal stimulation to the vomiting centre |
|
|
|
Following a particular severe episode of alcohol excess people may experience |
tremors. These are due to increased glutamate production by neurones to compensate for the previous inhibition by ethanol. |
|
|
|
Alcohol - problem drinking: management |
oral thiamine if their 'diet may be deficient' benzodiazepines for acute withdrawal disulfram: promotes abstinence acamprosate |
|
|
|
Alcohol - problem drinking: management |
benzodiazepines for acute withdrawal disulfram: promotes abstinence - alcohol intake causes severe reaction due to inhibition of acetaldehyde dehydrogenase. Patients should be aware that even small amounts of alcohol (e.g. In perfumes, foods, mouthwashes) can produce severe symptoms. Contraindications include ischaemic heart disease and psychosis acamprosate: reduces craving, known to be a weak antagonist of NMDA receptors, improves abstinence in placebo controlled trials |
|
|
|
A 22 year old woman who was admitted 2 days ago to the obstetrics ward because of preterm premature rupture of membranes (PPROM) has started to complain of abdominal pain, uterine contractions and 'flu-like symptoms'. Her history reveals that she is currently 24 weeks pregnant and has not had any complications up until the current admission. On examination she looks unwell with a fever of 39 degrees. A gynaecological examination reveals a foul-smelling discharge originating from the cervix which is subsequently collected and sent for analysis. At this point, what is the most likely diagnosis? |
Chorioamnionitis |
|
|
|
Chorioamnionitis (which can affect up to 5% of all pregnancies) is a potentially life-threatening condition to both mother and foetus and is therefore considered a |
medical emergency |
|
|
|
Chorioamnionitis def |
is usually the result of an ascending bacterial infection of the amniotic fluid / membranes / placenta major risk factor in this scenario is the preterm premature rupture of membranes |
|
|
|
Chorioamnionitis mgmt |
Prompt delivery of the foetus (via cesarean section if necessary) and administration of intravenous antibiotics is widely considered the mainstay of initial treatment for this condition. |
|
|
|
Pulmonary embolus |
pH 7.45, pO2 7.2 kPa, pCO2 2.5 kPa, HCO3 24 mEq/L |
|
|
|
Pulmonary embolus |
A combination of hypoxia and respiratory alkalosis should suggest a pulmonary embolus. The respiratory alkalosis is due to hyperventilation associated with the pulmonary embolism. |
|
|
|
High output ureterosigmoidostomy |
pH 7.25, pO2 8.9 kPa, pCO2 3.2 kPa, HCO3 10 mEq/L |
|
|
|
High output ureterosigmoidostomy |
There is acidosis. To compensate the patient will attempt to raise the pH level in the blood by hyperventilating, hence the low CO2 level . |
|
|
|
Widespread mesenteric infarction |
pH 7.25, pO2 8.9 kPa, pCO2 3.2 kPa, HCO3 10 mEq/L |
|
|
|
Widespread mesenteric infarction |
pH 7.25, pO2 8.9 kPa, pCO2 3.2 kPa, HCO3 10 mEq/L |
|
|
|
Metabolic acidosis is commonly classified according to |
anion gap. |
|
|
|
Normal anion gap ( = hyperchloraemic metabolic acidosis) |
gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula renal tubular acidosis drugs: e.g. acetazolamide ammonium chloride injection Addison's disease |
|
|
|
Raised anion gap metabolic acidosis |
lactate: shock, hypoxia ketones: diabetic ketoacidosis, alcohol urate: renal failure acid poisoning: salicylates, methanol |
|
|
|
Metabolic alkalosis |
Metabolic alkalosis may be caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of the kidney or gastrointestinal tract |
|
|
|
Metabolic alkalosisCauses |
vomiting / aspiration (e.g. peptic ulcer leading to pyloric stenos, nasogastric suction) diuretics liquorice, carbenoxolone hypokalaemia primary hyperaldosteronism Cushing's syndrome Bartter's syndrome congenital adrenal hyperplasia |
|
|
|
Respiratory acidosis |
Respiratory acidosis may be caused by a number of conditions |
|
|
|
Respiratory acidosis |
COPD decompensation in other respiratory conditions e.g. life-threatening asthma / pulmonary oedema sedative drugs: benzodiazepines, opiate overdose |
|
|
|
Respiratory alkalosisCommon causes |
anxiety leading to hyperventilation pulmonary embolism salicylate poisoning CNS disorders: stroke, subarachnoid haemorrhage, encephalitis altitude pregnancy |
|
|
|
A 25-year-old man presents to his GP demanding a CT scan of his abdomen. He states it is 'obvious' he has cancer despite previous negative investigations. This is an example of a: |
Hypochondrial disorder |
|
|
|
Unexplained symptoms |
Somatisation = Symptoms hypoChondria = Cancer |
|
|
|
You are reviewing the results of an ambulatory blood pressure monitor (ABPM) for a 57-year-old man with suspected hypertension. In the meantime you have arranged an ECG, blood tests and a urine dipstick, all of which have been within normal limits. His 10-year cardiovascular risk is 11% according to QRISK. The ABPM results show an average daytime reading of 146/92 mmHg. What is the most appropriate course of action? |
Diagnose stage 1 hypertension and advise about lifestyle changes |
|
|
|
A 58-year-old woman with a history of left hip osteoarthritis presents for review. She is currently taking co-codamol 30/500 for pain on a regular basis but this is unfortunately not controlling her symptoms. There is no past medical history of note, in particular no asthma or gastrointestinal problems. What is the most suitable next step in management? |
Add oral ibuprofen + proton pump inhibitor |
|
|
|
NICE recommend co-prescribing a PPI with NSAIDs in all patients with |
osteoarthritis
Topical NSAIDs are only indicated for osteoarthritis of the knee or hand. |
|
|
|
A 67 year patient with known emphysema presents to the Emergency Department with a two week history of cough productive of blood stained sputum. Chest X-Ray shows a circular area of dense right upper lobe consolidation. Despite seven days of intravenous antibiotics (piperacillin and tazobactam) his condition has not improved. An urgent inpatient bronchoscopy reveals no endobronchial lesion but broncho-alveolar lavage reveals an underlying pathogenic organism. Ziehl-Nielson staining is negative. What organism would you suspect? |
Aspergillus fumigatus |
|
|
|
Aspergilloma |
An aspergilloma is a mycetoma (mass-like fungus ball) which often colonises an existing lung cavity (e.g. secondary to tuberculosis, lung cancer or cystic fibrosis) |
|
|
|
AspergillomaUsually asymptomatic but features may include |
cough haemoptysis (may be severe) |
|
|
Aspergilloma inv |
chest x-ray containing a rounded opacity high titres Aspergillus precipitins |
|
|
|
A 31-year-old woman presents for review. For the past few months she has been feeling generally tired and has not had a normal period for around 4 months. Prior to this she had a regular 30 day cycle. A pregnancy test is negative, pelvic examination is normal and routine bloods are ordered:FBCNormalU&ENormalTFTNormalFollicle-stimulating hormone41 iu/l ( < 35 iu/l)Luteinizing hormone33 mIU/l (< 20 mIU/l)Oestradiol70 pmol/l ( > 100 pmol/l)What is the most likely diagnosis? |
Premature ovarian failure |
|
|
|
Premature ovarian failure def |
onset of menopausal symptoms and elevated gonadotrophin levels before the age of 40 years. |
|
|
|
Premature ovarian failure causes |
idiopathic - the most common cause chemotherapy autoimmune radiation |
|
|
|
Premature ovarian failure fxs |
climacteric symptoms: hot flushes, night sweats infertility secondary amenorrhoea raised FSH, LH levels |
|
|
|
Jacky, 30, has had a range of persisting symptoms, which doctors believe is down to hypoadrenalism. Which of the following of Jacky's symptoms would distinguish between primary adrenal failure and secondary adrenal insufficiency? |
Skin hyperpigmentation |
|
|
|
Primary adrenal failure is where the problem is located in the |
adrenal gland |
|
|
|
Primary adrenal failure pathophys |
As the adrenal gland isn't functioning as normal it is secreting a smaller amount of cortisol than it should be. This leads to the pituitary gland responding to this drop in cortisol by secreting more ACTH |
|
|
|
ACTH is derived from a |
larger precursor called pro-opiomelanocortin (POMC), which also happens to be a precursor for beta-endorphin (which isn't important in this case) and melanocyte stimulating hormone (MST). MST, as the name suggests, stimulates melanocytes giving the hyperpigmentation that can be seen in primary adrenal failure. |
|
|
|
hyperpigmentation not seen in secondary adrenal insufficiency, as the underlying mechanism of this is |
hypopituitarism the prob = lack of ACTH (lack of ACTH = lack of POMC and hence MST) |
|
|
|
The prodrome is characterised by fever, irritability and conjunctivitis |
Measles |
|
|
|
May cause a crop of white spots on the inside of the mouth |
Measles |
|
|
|
May cause vesicles in the mouth and on the palms |
Coxsackie A16 |
|
|
|
A 28-year-old woman is seen at her booking visit. She has a family history of first degree relative with type I diabetes mellitus and is concerned about the development of gestational diabetes. When should this patient be offered screening with a 75g 2-hour oral glucose tolerance test (OGTT) ? |
Next anenatal visit and repeat at 24-28 weeks if first OGTT was normal |
|
|
|
A 25-year-old woman presents as she has noticed an unusual appearance of her tongue. This has been present for the past few weeks. She reports getting a burning sensation when she eats spicy food. DX |

Geographic tongue Management reassurance about benign nature |
|
|
|
A 46-year-old female presents with a burning sensation over the antero-lateral aspect of her right thigh. A diagnosis of meralgia paraesthetica is suspected. Which nerve is most likely to be affected? |
Lateral cutaneous nerve of thigh |
|
|
|
Burning thigh pain |
? meralgia paraesthetica - lateral cutaneous nerve of thigh compression |
|
|
|
Meralgia paraesthetica |
caused by compression of lateral cutaneous nerve of thigh typically burning sensation over antero-lateral aspect of thigh |
|
|
|
A 22-year-old woman delivers a baby boy at full term having had an uncomplicated pregnancy and labour. However, 4 hours after delivery the neonate develops a temperature of 38.0 degrees Celsius and becomes less responsive. Which organism is the commonest cause of severe, early-onset (under 7 days of age) neonatal infection? |
Streptococcus agalactiae |
|
|
|
Streptococcus agalactiae - also known as group B streptococcus - is the commonest cause of |
severe, early-onset neonatal infection |
|
|
|
Risk factors for Group B Streptococcus (GBS) infection: |
prematurity prolonged rupture of the membranes previous sibling GBS infection maternal pyrexia e.g. secondary to chorioamnionitis nb Women found to have GBS infection in the antenatal period should be treated with intravenous antibiotics during labour. This has been shown to reduce early-onset GBS disease in the neonate |
|
|
|
You are reviewing a patient with chronic obstructive pulmonary disease. Which one of the following best describes the vaccinations they should receive? |
Annual influenza + one-off pneumococcal |
|
|
|
A 33-year-old female presents with a vaginal discharge. Which one of the following features is not consistent with bacterial vaginosis? |
Strawberry cervix |
|
|
|
Which one of the following features is consistent with bacterial vaginosis? |
Vaginal pH > 4.5 Thin, white homogenous discharge Clue cells on microscopy Positive whiff test |
|
|
|
A 53 year old woman presents with mood swings and hot flushes for 13 months. Which of the following would be a contraindication for starting hormonal replacement therapy (HRT)? |
Previous history of breast carcinoma |
|
|
|
contraindication for starting hormonal replacement therapy (HRT)? |
Previous history of breast carcinoma |
|
|
|
Hormone replacement therapy: adverse effects |
nausea breast tenderness fluid retention and weight gain |
|
|
|
Hormone replacement therapy Potential complications |
increased risk of breast cancer: increased by the addition of a progestogen increased risk of endometrial cancer: reduced by the addition of a progestogen but not eliminated completely. The BNF states that the additional risk is eliminated if a progestogen is given continuously increased risk of venous thromboembolism: increased by the addition of a progestogen increased risk of stroke increased risk of ischaemic heart disease if taken more than 10 years after menopause |
|
|
|
Which one of the following statements regarding cerebral palsy is correct? |
It is the most common cause of major motor impairment in children It affects 2 in 1,000 live births 20% of children have hearing impairment Postnatal factors account for 10% of cases Around 30% of children with cerebral palsy have epilepsy |
|
|
|
Cerebral palsy may be defined as |
disorder of movement and posture due to a non-progressive lesion of the motor pathways in the developing brain |
|
|
|
Cerebral palsy |
is the most common cause of major motor impairment |
|
|
|
Cerebral palsyPossible manifestations include: |
abnormal tone early infancy delayed motor milestones abnormal gait feeding difficulties |
|
|
|
Children with cerebral palsy often have associated non-motor problems such as: |
learning difficulties (60%) epilepsy (30%) squints (30%) hearing impairment (20%) |
|
|
|
Cerebral palsyCauses |
antenatal (80%): e.g. cerebral malformation and congenital infection (rubella, toxoplasmosis, CMV) intrapartum (10%): birth asphyxia/trauma postnatal (10%): intraventricular haemorrhage, meningitis, head-trauma |
|
|
|
Cerebral palsyClassification |
spastic (70%): hemiplegia, diplegia or quadriplegia dyskinetic ataxic mixed |
|
|
|
Cerebral palsyManagement |
multidisciplinary approach is needed treatments for spasticity include oral diazepam, oral and intrathecal baclofen, botulinum toxin type A, orthopaedic surgery and selective dorsal rhizotomy anticonvulsants, analgesia as required |
|
|
|
You are called to see a 33-year-old patient complaining of vaginal bleeding 12 hours after a vaginal delivery. On arrival, she is alert, complaining of breathlessness and giddiness. Her blood pressure is 97/73 mmHg. She has no history of a bleeding disorder, and you are told she did not tear. She has a blue cannula in situ with nothing attached, and the midwife has bleeped the registrar on call. What is your immediate course of action? |
Insert a large bore cannula |
|
|
|
Post-partum haemorrhage should be managed with an |
ABC approach. Cannula Flow rate (mL/min) Blue (22G)31 Pink (20G)55 Green (18G)90 White (17G)135 Grey (16G)170 Orange (14G)265 |
|
|
|
Which one of the following is least recognised in patients with Meniere's disease |
Symptoms triggered by sudden change in head position |
|
|
|
A 41-year-old female presents with lethargy and pain all over her body. This has been present for the past six months and is often worse when she is stressed or cold. Clinical examination is unremarkable other than a large number of tender points throughout her body. A series of blood tests including an autoimmune screen, inflammatory markers and thyroid function are normal. Given the likely diagnosis, which one of the following is most likely to be beneficial? |
Cognitive behavioural therapy |
|
|
|
Fibromyalgia |
is a syndrome characterised by widespread pain throughout the body with tender points at specific anatomical sites. The cause of fibromyalgia is unknown |
|
|
|
Fibromyalgia fxs |
chronic pain: at multiple site, sometimes 'pain all over' lethargy sleep disturbance, headaches, dizziness are common |
|
|
|
FibromyalgiaDiagnosis is clinical and sometimes refers to |
the American College of Rheumatology classification criteria which lists 9 pairs of tender points on the body. If a patient is tender in at least 11 of these 18 points it makes a diagnosis of fibromyalgia more likely |
|
|
|
The management of fibromyalgia is often difficult and needs to be tailored to the |
individual patient |
|
|
|
management of fibromyalgia partly based on consensus guidelines from the European League against Rheumatism (EULAR) published in 2007 and also a BMJ review in 2014. |
explanation aerobic exercise: has the strongest evidence base cognitive behavioural therapy medication: pregabalin, duloxetine, amitriptyline |
|
|
|
The chest x-ray below is from a 67-year-old woman with a history of rheumatoid arthritis. She has taken immunosuppressants for a number of years: dx |

Lung abscess |
|
|
|
Chest x-ray: cavitating lung lesion Differential |
abscess (Staph aureus, Klebsiella and Pseudomonas) squamous cell lung cancer tuberculosis Wegener's granulomatosis pulmonary embolism rheumatoid arthritis aspergillosis, histoplasmosis, coccidioidomycosis |
|
|
|
A 24 year-old woman, who is 35 weeks pregnant is found to have a blood pressure of 165/108 mmHg at a routine GP appointment. She is otherwise well. Her only regular medication is 200mg labetalol. Urinalysis reveals 2+ proteinuria. Cardiotocography is normal.Blood tests are as follows:Hb14 g/lPlatelets270 * 109/lWBC5.6 * 109/lNa+140 mmol/lK+3.9 mmol/lUrea2.4 mmol/lCreatinine21 µmol/lWhat is the most appropriate step in her management? |
Admit the patient to hospital as an emergency |
|
|
|
A 62-year-old man complains of pain in his right hip which is worse when he walks. Heberden's nodes are noted on examination of the distal interphalangeal joints |
Osteoarthritis |
|
|
|
A 34-year-old man with a history of ulcerative colitis complains of pain and stiffness in his left hip which is worse in the mornings |
Inflammatory arthritis |
|
|
|
A 29-year-old man who is a keen jogger complains of pain on the lateral aspect of his left hip. On examination there is a full range of movement but tenderness is noted on the anterolateral aspect of the joint |
Trochanteric bursitis |
|
|
|
Which one of the following statements regarding macular degeneration is true? |
Wet macular degeneration carries the worst prognosis |
|
|
|
Which one of the following statements regarding endometrial cancer is incorrect? |
Has a poor prognosis |
|
|
|
Endometrial cancer usually has a good prognosis |
true |
|
|
|
Which one of the following conditions is least associated with HLA-B27? |
Crohn's disease |
|
|
|
Seronegative spondyloarthropathies Common features |
associated with HLA-B27 rheumatoid factor negative - hence 'seronegative' peripheral arthritis, usually asymmetrical sacroiliitis enthesopathy: e.g. Achilles tendonitis, plantar fasciitis extra-articular manifestations: uveitis, pulmonary fibrosis (upper zone), amyloidosis, aortic regurgitation |
|
|
|
Seronegative spondyloarthropathies |
ankylosing spondylitis psoriatic arthritis Reiter's syndrome (including reactive arthritis) enteropathic arthritis (associated with IBD) |
|
|
|
Which one of the following statements regarding pregnant who are obese is correct? |
NICE do not recommend that pregnant women diet during pregnancy to reduce weight Obese women should take folic acid 5mg od. |
|
|
|
Pregnancy: obesity def |
usually defined as a body mass index (BMI) >= 30 kg/m² at the first antenatal visit. |
|
|
|
Maternal risks of obesity |
miscarriage venous thromboembolism gestational diabetes pre-eclampsia dysfunctional labour, induced labour postpartum haemorrhage wound infections There is also a higher caesarean section rate. |
|
|
|
Fetal risks of maternal obesity |
congenital anomaly prematurity macrosomia stillbirth increased risk of developing obesity and metabolic disorders in childhood neonatal death |
|
|
|
With respect to weight loss, NICE state: |
Explain that they should not try to reduce this risk by dieting while pregnant and that the risk will be managed by the health professionals caring for them during their pregnancy |
|
|
|
preg obesity mgmt |
folic acid all screened for gest. DM with OGTT at 24-28 weeks BMI>35 = give birth BMI >40 obstetric anaesthetist consultation |
|
|
|
A 58 year-old male is seen in cardiology outpatients clinic. He has a background of type 2 diabetes and hypercholesterolaemia. He complains of a 6 month history of a constricting discomfort in the front of his chest, precipitated by walking up the hill to his house. The pain is relieved by rest within about 5 minutes. He is currently prescribed a sublingual nitrate spray and is taking 10mg bisoprolol once a day. Cardiovascular and respiratory examination is unremarkable. a 12-lead ECG is normal.What would be the most appropriate additional medication? |
Amlodipine |
|
|
|
first-line treatment for stable angina |
Offer either a beta blocker or a calcium channel blocker nb If the person cannot tolerate the beta blocker or calcium channel blocker, consider switching to the other option (calcium channel blocker or beta blocker). or if not controlled try the other or combo |
|
|
|
management of stable angina If the person cannot tolerate beta blockers and calcium channel blockers or both are contraindicated, consider monotherapy with one of the following drugs: |
A long-acting nitrate Ivabradine Nicorandil Ranolazine |
|
|
|
The management of stable angina comprises |
lifestyle changes, medication, percutaneous coronary intervention and surgery |
|
|
|
Angina pectoris: drug management |
all patients should receive aspirin and a statin if no CI sublingual glyceryl trinitrate to abort angina attacks + either BB/CCB first line poor response = max dosing still sxs = monotx with BB/CCB still sxs = try new antianginals PCI/CABG |
|
|
|
concerning CCB and BB for stable angina mgmt |
if a calcium channel blocker is used as monotherapy a rate-limiting one such as verapamil or diltiazem should be used. If used in combination with a beta-blocker then use a long-acting dihydropyridine calcium-channel blocker (e.g. modified-release nifedipine). Remember that beta-blockers should not be prescribed concurrently with verapamil (risk of complete heart block) |
|
|
|
A 30-year-old female with a past history of asthma presents to the Emergency Department with pleuritic chest pain. She is not short-of-breath and her oxygen saturations on room air are 99%. Chest x-ray shows a right-sided pneumothorax with a 1.5cm rim of air and no mediastinal shift. What is the most appropriate management? |
Aspiration |
|
|
|
A 54-year-old man with a history of type 2 diabetes mellitus presents with a history of right shoulder pain. On examination there is limited movement of the right shoulder in all directions. What is the most likely diagnosis? |
Adhesive capsulitis |
|
|
|
Diabetic amyotrophy affects the lower limbs |
true |
|
|
|
You review a 60-year-old woman in the COPD clinic. She was diagnosed with COPD four years ago and is currently maintained on a salbutamol inhaler as required and a tiotropium inhaler regularly. She has recently managed to give up smoking and her latest FEV1 was 42% of predicted. Despite her current therapy she is have frequent exacerbations. What is the most appropriate next step in her management? |
Combined salmeterol + fluticasone inhaler |
|
|
|
A 38-year-old 12 week pregnant woman has recently had the combined test in order to assess her fetus' risk of having Down's syndrome. The risk is found to be 1 in 50 and so amniocentesis is offered to enable a definitive diagnosis to be made. The woman and her partner wish to know what danger the procedure would pose to the baby. What is the percentage additional risk of miscarriage that should be quoted to the couple in relation to this procedure? |
1% |
|
|
|
Amniocentesis is a procedure used in prenatal diagnosis. It may be offered after screening tests have indicated a high risk of fetal abnormality or in women considered to be at |
high risk, for example if > 35 years old. |
|
|
|
Amniocentesis |
Around 20 ml of fluid is removed by transabdominal needle under ultrasound guidance. Fetal cells present in the amniotic fluid are then studied to aid the diagnosis of a number of conditions. |
|
|
|
Amniocentesis is usually performed at |
16 weeks and the risk of fetal loss is 0.5-1% The karyotype results typically take 3 weeks. It is known the karyotype may be wrong in 1/1000 cases due to maternal cells being present |
|
|
|
amniocentesis can be used for |
karyotyping |
|
|
|
AmniocentesisConditions which may be diagnosed |
neural tube defects (raised AFP levels in the amniotic fluid) chromosomal disorders inborn errors of metabolism |
|
|
|
normal range for intraocular pressure? |
10-21 mmHg |
|
|
|
A 32 year old woman with gestational diabetes undergoes a difficult spontaneous vaginal delivery. During her strenuous efforts she unfortunately suffers a perineal tear. Examination reveals it involves structures from the vaginal mucosa to approximately 70% of the external anal sphincter.What degree of tear is this? |
3rd degree - subcategory B |
|
|
|
According to the current classification of perineal tears, the involvement of more than 50% of the external anal sphincter (but not the internal sphincter) is classified as |
a 3rd degree - subcategory B tear. |
|
|

classification of perineal tears: |
first degree: superficial damage with no muscle involvement second degree: injury to the perineal muscle, but not involving the anal sphincter third degree: injury to perineum involving the anal sphincter complex (external anal sphincter, EAS and internal anal sphincter, IAS): 3a: less than 50% of EAS thickness torn 3b: more than 50% of EAS thickness torn 3c: IAS torn fourth degree: injury to perineum involving the anal sphincter complex (EAS and IAS) and rectal mucosa |
|
|
|
Risk factors for perineal tears |
primigravida large babies precipitant labour shoulder dystocia forceps delivery |
|
|
|
A mother brings her 8-month-old infant to the GP due to the development of a nappy rash. On examination an erythematous rash with flexural sparing is seen. What is the most likely cause? |
Irritant dermatitis |
|
|
|
Causes of a napkin ('nappy') rash include the following: |
Irritant dermatitis Candida dermatitis Seborrhoeic dermatitis Psoriasis Atopic eczema |
|
|
|
Causes of a napkin ('nappy') rash include the following: Irritant dermatitis |
The most common cause, due to irritant effect of urinary ammonia and faeces Creases are characteristically spared |
|
|
|
whats the most common cause of napkin/nappy rash |
Irritant dermatitis |
|
|
|
Causes of a napkin ('nappy') rash include the following: Candida dermatitis |
Typically an erythematous rash which involve the flexures and has characteristic satellite lesions |
|
|
|
Causes of a napkin ('nappy') rash include the following: Seborrhoeic dermatitis |
Erythematous rash with flakes. May be coexistent scalp rash |
|
|
|
Causes of a napkin ('nappy') rash include the following: Psoriasis |
A less common cause characterised by an erythematous scaly rash also present elsewhere on the skin |
|
|
|
Causes of a napkin ('nappy') rash include the following: Atopic eczema |
Other areas of the skin will also be affected |
|
|
|
Napkin rashesGeneral management points |
disposable nappies are preferable to towel nappies expose napkin area to air when possible apply barrier cream (e.g. Zinc and castor oil) mild steroid cream (e.g. 1% hydrocortisone) in severe cases |
|
|
|
A 20-year-old primiparous woman is in the final stages of delivery. The baby's leading shoulder becomes impacted behind her pelvis. The midwife rings the emergency call bell. What is the first step in management? |
Flex and abduct the hips as much as possible (McRobert's manoeuvre) |
|
|
|
An 18 year old man is admitted to the emergency department with an episode of acute asthma. He is unable to complete sentences, tachycardic (118 beats per minute) and tachypnoiec (respiratory rate 30). He has received salbutamol, ipratopium bromide nebulisers and intravenous hydrocortisone through a large bore cannula in the right antecubital fossa. Despite another salbutamol nebuliser there is no improvement in his condition. What medication would be most appropriate to add? |
Magnesium sulphate |
|
|
|
acute severe asthma. |
inability to complete sentences, tachycardia and tachypnoea. |
|
|
|
acute severe asthma mgmt |
SIGN guidelines give clear instructions on how to escalate care. 1. Oxygen 2. Salbutamol nebulisers 3. Ipratropium bromide nebulisers 4. Hydrocortisone IV OR Oral Prednisolone 5. Magnesium Sulfate IV 6. Aminophylline/ IV salbutamol |
|
|
|
Asthma in children: management of acute attacks |
Children with severe or life threatening asthma should be transferred immediately to hospital. |
|
|
|
For children with mild to moderate acute asthma: |
Bronchodilator therapy (saba) + Steroid therapy nb severe asthma = admit |
|
|
|
You review a 61-year-old woman who has type 2 diabetes mellitus. She is currently taking metformin therapy but her HbA1c is 54 mmol/mol (7.1%). You are considering prescribing a DPP-4 inhibitor. Which one of the following best describes the side-effect profile? |
Weight neutral + no hypoglycaemia |
|
|
|
A couple in their 20s come into there GP after failing to conceive despite having regular sexual intercourse for 6 months, and ask you for advice. What is the most appropriate course of action for you to take? |
Wait until they have been having regular intercourse for 12 months |
|
|
|
Alice, an 80 year old recently widowed woman, attends your GP practice with her daughter, who is worried about her mother's memory. For the past few months she's been forgetting appointments and conversations that they had only a few days ago, needing prompting often to remember to remember recent events. After talking to Alice she tells you she doesn't have much of an appetite nowadays is waking up earlier than she used to. She denies any hallucinations or movement problems. On mini mental state exam Alice scores 23, you notice she's not properly concentrating on your questions, answering many of the questions with 'i don't know'. What is the most likely diagnosis? |
Depression |
|
|
|
The main symptoms that point to depression here are: |
Recent loss of a spouse Loss of appetite Early morning wakening Poor concentration |
|
|
|
MMSE scores: |
24-30- no cognitive impairment 18-23- mild cognitive impairment 0-17- Severe cognitive impairment |
|
|
|
Factors suggesting diagnosis of depression over dementia |
short history, rapid onset biological symptoms e.g. weight loss, sleep disturbance patient worried about poor memory reluctant to take tests, disappointed with results mini-mental test score: variable global memory loss (dementia characteristically causes recent memory loss) |
|
|

A 1-year-old girl is investigated for recurrent urinary tract infections. A micturating cystourethrogram is ordered: |
Vesicoureteric reflux |
|
|
|
Vesicoureteric reflux (VUR) is the |
abnormal backflow of urine from the bladder into the ureter and kidney |
|
|
|
Vesicoureteric reflux (VUR) |
relatively common abnormality in kids predisposes to UTIs in 30% kids - As around 35% of children develop renal scarring it is important to investigate for VUR in children following a UTI |
|
|
|
Pathophysiology of VUR |
ureters are displaced laterally, entering the bladder in a more perpendicular fashion than at an angle therefore shortened intramural course of ureter vesicoureteric junction cannot therefore function adequately |
|
|
|
The table below summarises the grading of VUR |
I = Reflux into the ureter only, no dilatation II = Reflux into the renal pelvis on micturition, no dilatation III = Mild/moderate dilatation of the ureter, renal pelvis and calyces IV = Dilation of the renal pelvis and calyces with moderate ureteral tortuosity V = Gross dilatation of the ureter, pelvis and calyces with ureteral tortuosity |
|
|
|
Investigation of VUR |
normally diagnosed following a micturating cystourethrogram DMSA scan may also be performed to look for renal scarring |
|
|
|
Iron deficiency anaemia post delivery is defined as a total haemoglobin of |
less than 100 g/L. Risk factors include pre-existing anaemia, Caesarean section and post-partum haemorrhage. A full blood count and ferritin level should be taken within 48 hours of delivery in these patients, and for any patients demonstrating symptoms of anaemia, such as tiredness, shortness of breath and tachycardia.If a woman is found to have a haemoglobin level below 100 g/L, but greater than 80 g/L, she should be treated with 200 mg of oral ferrous sulphate three times daily for 3 months. Full blood count and ferritin should be repeated three weeks post delivery.In women with a haemoglobin lower than 80 g/L, parental iron should be considered initially, followed by a three month course of oral iron. Intravenous iron results in a faster recovery in haemoglobin and ferritin stores than oral iron, and should be considered before blood transfusion. Below 70 g/L, blood transfusion should be considered, depending on symptoms and after consultation with the woman, but intravenous iron is also an option. |
|
|
|
A 60-year-old man who is investigated for exertional chest pain is diagnosed as having angina pectoris. Which one of the following drugs is most likely to improve his long-term prognosis? |
Aspirin Strong evidence exists supporting the use of aspirin in stable angina. The benefit of ACE inhibitors and beta-blockers are significant in patients who've had a myocardial infarction but modest in those with stable angina. |
|
|
|
A 18-year-old man who is known to have hereditary spherocytosis is admitted to hospital with lethargy. Admission bloods show the following:Hb 4.7 g/dlRetics 0.3%What is the most likely explanation for these findings? |
Parvovirus infection This man has had an aplastic crisis secondary to parvovirus infection. |
|
|
|
Hereditary spherocytosisBasics |
most common hereditary haemolytic anaemia in people of northern European descentautosomal dominant defect of red blood cell cytoskeletonthe normal biconcave disc shape is replaced by a sphere-shaped red blood cellred blood cell survival reduced as destroyed by the spleen |
|
|
|
Hereditary spherocytosis presentation |
failure to thrivejaundice, gallstonessplenomegalyaplastic crisis precipitated by parvovirus infectiondegree of haemolysis variableMCHC elevated |
|
|
|
Hereditary spherocytosis dx |
osmotic fragility test |
|
|
|
Hereditary spherocytosis mgmt |
folate replacement splenectomy |
|
|
|
G6PD deficiency |
Gender male (X linked recessive) Ethnicity African + mediterranean descent Typical hx • Neonatal jaundice • Infection/drugs precipitate haemolysis • Gallstones Blood film Heinz bodies Diagnostic test Measure enz activity of G6PD |
|
|
|
Hereditary spherocytosis |
Gender Equal (AD) Ethnicity Northern European descent Typical history • Neonatal jaundice • Chronic symptoms although haemolytic crises may be precipitated by infection • Gallstones • Splenomegaly is common Blood film Spherocytes (round, lack of central pallor) Diagnostic test Osmotic fragility test |
|
|
|
Most common AE of progesterone only pill |
irreg bleeds |
|
|
|
Acoustic neuroma (more correctly called vestibular schwannomas) Features can be predicted by the affected cranial nerves cranial nerve VIII: hearing loss, vertigo, tinnitus cranial nerve V: absent corneal reflex cranial nerve VII: facial palsy
Bilateral acoustic neuromas are seen in neurofibromatosis type 2 |
. |
|
|
|
Te woman is describing having migraines with aura - a condition that can increase using the COCP. Women who have migraine with aura should stop the pill immediately - this is because the oestrogen component of the COCP can increase the risk of the women having an ischaemic stroke. A progesterone-only contraceptive pill is therefore the only alternative contraceptive medication that can be prescribed, as the others have oestrogen. |
.. |
|
|
|
Acoustic neuroma (more correctly called vestibular schwannomas) Features can be predicted by the affected cranial nerves cranial nerve VIII: hearing loss, vertigo, tinnitus cranial nerve V: absent corneal reflex cranial nerve VII: facial palsy
Bilateral acoustic neuromas are seen in neurofibromatosis type 2 |
. |
|
|
|
Te woman is describing having migraines with aura - a condition that can increase using the COCP. Women who have migraine with aura should stop the pill immediately - this is because the oestrogen component of the COCP can increase the risk of the women having an ischaemic stroke. A progesterone-only contraceptive pill is therefore the only alternative contraceptive medication that can be prescribed, as the others have oestrogen. |
.. |
|
|
|
Trigeminal neuralgia is a pain syndrome characterised by severe unilateral pain. The vast majority of cases are idiopathic but compression of the trigeminal roots by tumours or vascular problems may occur
The International Headache Society defines trigeminal neuralgia as: a unilateral disorder characterised by brief electric shock-like pains, abrupt in onset and termination, limited to one or more divisions of the trigeminal nerve the pain is commonly evoked by light touch, including washing, shaving, smoking, talking, and brushing the teeth (trigger factors), and frequently occurs spontaneously small areas in the nasolabial fold or chin may be particularly susceptible to the precipitation of pain (trigger areas) the pains usually remit for variable periods
|
Management carbamazepine is first-line failure to respond to treatment or atypical features (e.g. < 50 years old) should prompt referral to neurology |
|
|
|
Acoustic neuroma (more correctly called vestibular schwannomas) Features can be predicted by the affected cranial nerves cranial nerve VIII: hearing loss, vertigo, tinnitus cranial nerve V: absent corneal reflex cranial nerve VII: facial palsy
Bilateral acoustic neuromas are seen in neurofibromatosis type 2 |
. |
|
|
|
Te woman is describing having migraines with aura - a condition that can increase using the COCP. Women who have migraine with aura should stop the pill immediately - this is because the oestrogen component of the COCP can increase the risk of the women having an ischaemic stroke. A progesterone-only contraceptive pill is therefore the only alternative contraceptive medication that can be prescribed, as the others have oestrogen. |
.. |
|
|
|
Trigeminal neuralgia is a pain syndrome characterised by severe unilateral pain. The vast majority of cases are idiopathic but compression of the trigeminal roots by tumours or vascular problems may occur
The International Headache Society defines trigeminal neuralgia as: a unilateral disorder characterised by brief electric shock-like pains, abrupt in onset and termination, limited to one or more divisions of the trigeminal nerve the pain is commonly evoked by light touch, including washing, shaving, smoking, talking, and brushing the teeth (trigger factors), and frequently occurs spontaneously small areas in the nasolabial fold or chin may be particularly susceptible to the precipitation of pain (trigger areas) the pains usually remit for variable periods
|
Management carbamazepine is first-line failure to respond to treatment or atypical features (e.g. < 50 years old) should prompt referral to neurology |
|
|
|
A 61-year-old man presents with a two-week history of a sharp, stabbing pain over his right cheekbone. He describes the pain as 'very severe' and 'coming in spasms'. It typical lasts for around one minute before subsiding. The pain can be triggered by shaving and eating. Examination of his eyes, cranial nerves and mouth is unremarkable. What is the most likely diagnosis?
|
Trigeminal neuralgia |
|
|
|
A 19-year-old man comes for review after burning himself with an iron. On examination he has a 4 by 3 cm area of pale pink skin the left forearm. In the middle of the area there are two small, fluid filled blisters. What is the most accurate description for this type of injury? |
Partial thickness (superficial dermal) burn |
|
|
|
Treatment of secondary hyperparathyroidism involves addressing the |
Underlyn cause |
|
|
|
individuals with chronic kidney disease, this being the most common cause of |
secondary hyperparathyroidism |
|
|
|
Acoustic neuroma (more correctly called vestibular schwannomas) Features can be predicted by the affected cranial nerves cranial nerve VIII: hearing loss, vertigo, tinnitus cranial nerve V: absent corneal reflex cranial nerve VII: facial palsy
Bilateral acoustic neuromas are seen in neurofibromatosis type 2 |
. |
|
|
|
Te woman is describing having migraines with aura - a condition that can increase using the COCP. Women who have migraine with aura should stop the pill immediately - this is because the oestrogen component of the COCP can increase the risk of the women having an ischaemic stroke. A progesterone-only contraceptive pill is therefore the only alternative contraceptive medication that can be prescribed, as the others have oestrogen. |
.. |
|
|
|
Trigeminal neuralgia is a pain syndrome characterised by severe unilateral pain. The vast majority of cases are idiopathic but compression of the trigeminal roots by tumours or vascular problems may occur
The International Headache Society defines trigeminal neuralgia as: a unilateral disorder characterised by brief electric shock-like pains, abrupt in onset and termination, limited to one or more divisions of the trigeminal nerve the pain is commonly evoked by light touch, including washing, shaving, smoking, talking, and brushing the teeth (trigger factors), and frequently occurs spontaneously small areas in the nasolabial fold or chin may be particularly susceptible to the precipitation of pain (trigger areas) the pains usually remit for variable periods
|
Management carbamazepine is first-line failure to respond to treatment or atypical features (e.g. < 50 years old) should prompt referral to neurology |
|
|
|
A 61-year-old man presents with a two-week history of a sharp, stabbing pain over his right cheekbone. He describes the pain as 'very severe' and 'coming in spasms'. It typical lasts for around one minute before subsiding. The pain can be triggered by shaving and eating. Examination of his eyes, cranial nerves and mouth is unremarkable. What is the most likely diagnosis?
|
Trigeminal neuralgia |
|
|
|
A 19-year-old man comes for review after burning himself with an iron. On examination he has a 4 by 3 cm area of pale pink skin the left forearm. In the middle of the area there are two small, fluid filled blisters. What is the most accurate description for this type of injury? |
Partial thickness (superficial dermal) burn |
|
|
|
Treatment of secondary hyperparathyroidism involves addressing the |
Underlyn cause |
|
|
|
individuals with chronic kidney disease, this being the most common cause of |
secondary hyperparathyroidism
treatment consists of dietary restriction of phosphorous, supplemented with active vitamin D and phosphate binders. Most patients will improve following renal transplantation. |
|
|
|
Basic problems in chronic kidney disease |
low vitamin D (1-alpha hydroxylation normally occurs in the kidneys) high phosphate low calcium: due to lack of vitamin D, high phosphate secondary hyperparathyroidism: due to low calcium, high phosphate and low vitamin D |
|
|
|
Basic problems in chronic kidney disease |
low vitamin D (1-alpha hydroxylation normally occurs in the kidneys) high phosphate low calcium: due to lack of vitamin D, high phosphate secondary hyperparathyroidism: due to low calcium, high phosphate and low vitamin D |
|
|
|
Several clinical manifestations of chronic renal failure may result:
|
Osteitis fibrosa cystica aka hyperparathyroid bone disease
Adynamic reduction in cellular activity (both osteoblasts and osteoclasts) in bone may be due to over treatment with vitamin D
Osteomalacia due to low vitamin D
Osteosclerosis
Osteoporosis |
|
|
|
Several clinical manifestations of chronic renal failure may result:
|
Osteitis fibrosa cystica aka hyperparathyroid bone disease
Adynamic reduction in cellular activity (both osteoblasts and osteoclasts) in bone may be due to over treatment with vitamin D
Osteomalacia due to low vitamin D
Osteosclerosis
Osteoporosis
X-ray of a Brown tumour caused by secondary hyperparathyroidism in a young female with chronic kidney disease |
|
|
|
A woman presents asking for the 'morning after pill'. Up to what period following intercourse is levonorgestrel licensed to be used? |
72hrs |
|
|
|
Several clinical manifestations of chronic renal failure may result:
|
Osteitis fibrosa cystica aka hyperparathyroid bone disease
Adynamic reduction in cellular activity (both osteoblasts and osteoclasts) in bone may be due to over treatment with vitamin D
Osteomalacia due to low vitamin D
Osteosclerosis
Osteoporosis
X-ray of a Brown tumour caused by secondary hyperparathyroidism in a young female with chronic kidney disease |
|
|
|
A woman presents asking for the 'morning after pill'. Up to what period following intercourse is levonorgestrel licensed to be used? |
72hrs |
|
|
|
Levonorgestrel fxs |
should be taken as soon as possible - efficacy decreases with time must be taken within 72 hrs of unprotected sexual intercourse (UPSI)* single dose of levonorgestrel 1.5mg (a progesterone) mode of action not fully understood - acts both to stop ovulation and inhibit implantation 84% effective is used within 72 hours of UPSI levonorgestrel is safe and well tolerated. Disturbance of the current menstrual cycle is seen in a significant minority of women. Vomiting occurs in around 1% if vomiting occurs within 2 hours then the dose should be repeated can be used more than once in a menstrual cycle if clinically indicated |
|
|
|
Intrauterine device (IUD) |
must be inserted within 5 days of UPSI, or if a women presents after more than 5 days then an IUD may be fitted up to 5 days after the likely ovulation date may inhibit fertilisation or implantation prophylactic antibiotics may be given if the patient is considered to be at high-risk of sexually transmitted infection is 99% effective regardless of where it is used in the cycle may be left in-situ to provide long-term contraception. If the client wishes for the IUD to be removed it should be at least kept in until the next period |
|
|
|
Intrauterine device (IUD) |
must be inserted within 5 days of UPSI, or if a women presents after more than 5 days then an IUD may be fitted up to 5 days after the likely ovulation date may inhibit fertilisation or implantation prophylactic antibiotics may be given if the patient is considered to be at high-risk of sexually transmitted infection is 99% effective regardless of where it is used in the cycle may be left in-situ to provide long-term contraception. If the client wishes for the IUD to be removed it should be at least kept in until the next period |
|
|
|
A 26-year-old female is admitted to hospital with palpitations. ECG shows a shortened PR interval and wide QRS complexes associated with a slurred upstroke seen in lead II. What is the definitive management of this condition? |
Accessory pathway ablation |
|
|
|
Wolff-Parkinson White syndrome, definitive treatment. |
accessory pathway ablation
Nb medical therapy: sotalol***, amiodarone, flecainide
sotalol should be avoided if there is coexistent atrial fibrillation as prolonging the refractory period at the AV node may increase the rate of transmission through the accessory pathway, increasing the ventricular rate and potentially deteriorating into ventricular fibrillation |
|
|
|
WPW ecg fxs |
Possible ECG features include: |
short PR interval wide QRS complexes with a slurred upstroke - 'delta wave' left axis deviation if right-sided accessory pathway* right axis deviation if left-sided accessory pathway* |
|
|
Associations of WPW |
HOCM mitral valve prolapse Ebstein's anomaly thyrotoxicosis secundum ASD |
|
|
|
A 51-year-old female presents to the Emergency Department following an episode of transient right sided weakness lasting 10-15 minutes. Examination reveals the patient to be in atrial fibrillation. If the patient remains in chronic atrial fibrillation what is the most suitable form of anticoagulation? |
Warfarin, target INR 2-3
The CHA2DS2-VASc for this patient is 3 - 2 for the transient ischaemic attack and 1 for being female. She should therefore be offered anticoagulation with warfarin. Rate, discuss and give feedback on this question Next question |
|
|
|
A 51-year-old female presents to the Emergency Department following an episode of transient right sided weakness lasting 10-15 minutes. Examination reveals the patient to be in atrial fibrillation. If the patient remains in chronic atrial fibrillation what is the most suitable form of anticoagulation? |
Warfarin, target INR 2-3
The CHA2DS2-VASc for this patient is 3 - 2 for the transient ischaemic attack and 1 for being female. She should therefore be offered anticoagulation with warfarin. Rate, discuss and give feedback on this question Next question |
|
|
|
management of atrial fibrillation (AF) in 2014. They suggest using the CHA2DS2-VASc score to determine the most appropriate anticoagulation strategy. This scoring system superceded the CHADS2 score. |
C Congestive heart failure 1 H Hypertension (or treated hypertension) 1 A2 Age >= 75 years 2 Age 65-74 years 1 D Diabetes 1 S2 Prior Stroke or TIA 2 V Vascular disease (including ischaemic heart disease and peripheral arterial disease) 1 S Sex (female) |
|
|
|
A 51-year-old female presents to the Emergency Department following an episode of transient right sided weakness lasting 10-15 minutes. Examination reveals the patient to be in atrial fibrillation. If the patient remains in chronic atrial fibrillation what is the most suitable form of anticoagulation? |
Warfarin, target INR 2-3
The CHA2DS2-VASc for this patient is 3 - 2 for the transient ischaemic attack and 1 for being female. She should therefore be offered anticoagulation with warfarin. Rate, discuss and give feedback on this question Next question |
|
|
|
management of atrial fibrillation (AF) in 2014. They suggest using the CHA2DS2-VASc score to determine the most appropriate anticoagulation strategy. This scoring system superceded the CHADS2 score. |
C Congestive heart failure 1 H Hypertension (or treated hypertension) 1 A2 Age >= 75 years 2 Age 65-74 years 1 D Diabetes 1 S2 Prior Stroke or TIA 2 V Vascular disease (including ischaemic heart disease and peripheral arterial disease) 1 S Sex (female) |
|
|
|
The table below shows a suggested anticoagulation strategy for AF based on the score: |
0 No treatment 1 Males: Consider anticoagulation Females: No treatment (this is because their score of 1 is only reached due to their gender) 2 or more Offer anticoagulation |
|
|
|
Once youve done CHADSVAS, and want to assess bleeding risk on anticoag you use |
HASBLED
H Hypertension, uncontrolled, systolic BP > 160 mmHg 1 A Abnormal renal function (dialysis or creatinine > 200) Or Abnormal liver function (cirrhosis, bilirubin > 2 times normal, ALT/AST/ALP > 3 times normal 1 for any renal abnormalities
1 for any liver abnormalities S Stroke, history of 1 B Bleeding, history of bleeding or tendency to bleed 1 L Labile INRs (unstable/high INRs, time in therapeutic range < 60%) 1 E Elderly (> 65 years) 1 D Drugs Predisposing to Bleeding (Antiplatelet agents, NSAIDs) Or Alcohol Use (>8 drinks/week) |
|
|
|
A 51-year-old female presents to the Emergency Department following an episode of transient right sided weakness lasting 10-15 minutes. Examination reveals the patient to be in atrial fibrillation. If the patient remains in chronic atrial fibrillation what is the most suitable form of anticoagulation? |
Warfarin, target INR 2-3
The CHA2DS2-VASc for this patient is 3 - 2 for the transient ischaemic attack and 1 for being female. She should therefore be offered anticoagulation with warfarin. Rate, discuss and give feedback on this question Next question |
|
|
|
management of atrial fibrillation (AF) in 2014. They suggest using the CHA2DS2-VASc score to determine the most appropriate anticoagulation strategy. This scoring system superceded the CHADS2 score. |
C Congestive heart failure 1 H Hypertension (or treated hypertension) 1 A2 Age >= 75 years 2 Age 65-74 years 1 D Diabetes 1 S2 Prior Stroke or TIA 2 V Vascular disease (including ischaemic heart disease and peripheral arterial disease) 1 S Sex (female) |
|
|
|
The table below shows a suggested anticoagulation strategy for AF based on the score: |
0 No treatment 1 Males: Consider anticoagulation Females: No treatment (this is because their score of 1 is only reached due to their gender) 2 or more Offer anticoagulation |
|
|
|
Once youve done CHADSVAS, and want to assess bleeding risk on anticoag you use |
HASBLED
H Hypertension, uncontrolled, systolic BP > 160 mmHg 1 A Abnormal renal function (dialysis or creatinine > 200) Or Abnormal liver function (cirrhosis, bilirubin > 2 times normal, ALT/AST/ALP > 3 times normal 1 for any renal abnormalities
1 for any liver abnormalities S Stroke, history of 1 B Bleeding, history of bleeding or tendency to bleed 1 L Labile INRs (unstable/high INRs, time in therapeutic range < 60%) 1 E Elderly (> 65 years) 1 D Drugs Predisposing to Bleeding (Antiplatelet agents, NSAIDs) Or Alcohol Use (>8 drinks/week)
There are no formal rules on how we act on the HAS-BLED score although a score of >= 3 indicates a 'high risk' of bleeding, defined as intracranial haemorrhage, hospitalisation, haemoglobin decrease >2 g/L, and/or transfusion. |
|