Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
134 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
After what stage are these hormonal changes common, breast EP and lobules proliferate and stroma becomes edematous?
a. ovulation b. menstruation c. lactation d. premenopausal |
ovulation due to the surge of E and P
|
|
|
|
After what stage are these changes noted, regression of lobules and stroma edema?
a. ovulation b. menstruation c. lactation d. premenopausal |
menstruation
|
|
|
|
After what stage are these changes noticed, full functional activity w/an increase in the gland to stromal ratio so the breast is composed almost of glands, EP becomes vacuolated.
a. ovulation b. menstruation c. lactation d. premenopausal |
only lobular cell produce milk, this stage is preparing for milk secretion or lactation (10d postpartum = colostrum and then milk high in protein and calories)
|
|
|
|
During what stage are these changes notec, lobules and intralobular strom begin to involute, later leading to complete lobular atrophy replacing dense interlobular CT with fat, allowing better mammorgraphy?
a. ovulation b. menstruation c. lactation d. premenopausal |
premenopausal (after third decade and into later years) just before mempause
|
|
|
|
Although breast cancer can metastasize into lymph nodes which are more dangerous?
a. internal mammary b. supraclavicular c. axillary d. thoracic |
axillary b/c the breast cancer is often missed there leading to aggressive spread to the rest of the body
|
|
|
|
Malignancy increases with age, often 10% in women , 40y/o and what percentage in women > 50 y/o?
a. 40% b. 50% c. 60% d. 70% |
60%
|
|
|
|
Although cyclic pain (mastodynia) is often benign, noncyclic pain that is localized can be a result of rupture of cyst, injury or infection. What percentage of women with pain result in breast cancer?
a. 5% b. 10% c. 15% d. 20% |
10% of breast cancer are painful, whild 95% painful masses are benign
|
|
|
|
What differential diagnosis are common in women complaining of redness, dimpling, retraction, and ulceration around breast, EXCEPt?
a. fungal infection b. dermatologic disorder c. infection d. underlying malignancy |
all except fungal infection (not specific for these symptoms)
|
|
|
|
Galactorrhea in women is often associated with all, EXCEPT?
a. elevated PRL b. malignancy c. hypothyroidism, medications d. repeated nipple stimialtion |
malignancy does not result in galactorrhea in women; it's usually benign
medications that can lead to galactorrhea include: oral contraceptives, tCA, methyldopa, phenothiazine) |
|
|
|
What is the most common cause of blood discharge?
a. large duct papilloma b. actue mastitis c. mammary duct ectasia d. lymphocytic mastopathy |
large duct papilloma often benign
|
|
|
|
Why is mammorgraphy better appreciated in older women?
a. > dense CT and < fat b. < dense CT and > fat c. >dense CT and > fat d. < dense CT and < fat |
< dense CT and > fat leading to increased translucency; which is beneficial since malignancy increase in incidence with age
|
|
|
|
What is the triple test include:
a. BSE (breast self exam) b. physical exam c. mammography d. biopsy |
physical exam (detect fibrocystic changes0, mammography (abnormal calcifications and masses), and biopsy (evaluate masses and calcifications) (but all MUST correlate, if not excision biopsy is indicated)
|
|
|
|
Ultrasound is often used to identify:
a. abnormal calcifications b. masses c. fluid filled cyst d. dense breast tissue |
fluid filled cyst
|
|
|
|
When is MRI effective for diagnosis of breast disease/
a. after a palpable mass is identified b. fluid filled cyst c. high risk pt and those with dense breast tissue d. fibrocystic change detections |
high risk pts with dense breast tissue (or younger population)
|
|
|
|
23y/o female recent had a child 2wks age presents with complaints of redness and painful breast. Upon further inquiry, she admits she has been lactating her newborn. You suspect an infection with Staph aures or Strep, what does she have?
a. acute mastitis b. periductal mastitis c. mammary duct ectasia d. fat necrosis |
acute mastitis due to her lactation she is infected with Staph or Strep and need to continue lactating after dose of antibiotics to relieve infection
|
|
|
|
27y/o female students complains of painful, swollen, and tender breast. Pt denies lactating at this time. Although she reports a hx of smoking for the past 6 years. If this is a result of an abscess, what is the pathology most likely?
a. perareolar mass leading to duct dilation, imsipissation of secretion, periductal fibrosis and stromal inflammation b. squamous metaplasia of nipple duct w/dialtion and rupture of duct, surrounding inflammation and superimposed infection c. palpable, bilateral masses with lymphocytic inflammation surrounding lobules and blood vessels d. infection with Staph or Strep |
a. perareolar mass leading to duct dilation, imsipissation of secretion, periductal fibrosis and stromal inflammation (mammary duct ectasia)
b. squamous metaplasia of nipple duct w/dialtion and rupture of duct, surrounding inflammation and superimposed infection (periductal mastitis ***** prevalent in SMOKERS c. palpable, bilateral masses with lymphocytic inflammation surrounding lobules and blood vessels (lymphocytic mastopathy) d. infection with Staph or Strep (acute mastitis) |
|
|
|
45 y/o female presents stating she thinks she is entering menopause. Pt complaining of breast discharge (dirty white/green) and some tenderness. Due to hormonal changes she is experiencing you dx?
a. acute mastitis b. periductal mastitis c. mammary duct ectasia d. lymphocytic mastopathy |
mammry duct ectasia (blocking of mammary ducts) resulting in tenderness; send her for a mammography if there is a mass, since this can mimic carcinoma
|
|
|
|
34y/o female is presenting for a follow up after 3 months of radiation therapy. she notices a mass, and upon further inquire you notice histology: show necrotic fat cells surrounded by foamy histocytes, what is a possible inflammatory disorder of the breast, although these symptoms can mimic carcinoma?
a. acute mastitis b. periductal mastitis c. fat necrosis d. lymphocytic mastopathy |
fat necrosis often results after trauma, radiation therapy, and prior surgery (presenting as a mass or as density/calcifications on mammography)
|
|
|
|
32 y/o DMI female is f/u after a palpable mass, also seen on mammorgraphy. The micro report suggests inflammation surrounding lobules and blood vessels. What inflammatory disorder of the breast is suggestive
a. acute mastitis b. periductal mastitis c. mammary duct ectasia d. lymphocytic mastopathy |
lymphocytic mastopathy
often common in DMI and autoimmune dx such as thyroid dx |
|
|
|
The most common abnormalities of the breast are detected via the use of?
a. physical exam and US b. physical exam and mammography c. US and mammorgraphy d. US and biopsy |
physical exam and mammorgraphy
|
|
|
|
Which fibrocystic changes detected in breast tissue, can mimic cancer grossly and microscopicdally?
a. non-proliferative b. proliferative c. papilloma d. sclerosing adenosis |
sclerosing adenosis results in proliferation of small ductules or aicni with intralobular fibrosis; lobules become distorted by the fibrosis
can mimic tubular carcinoma |
|
|
|
What type of fibrocytic change results in epithelial hyperplasia?
a. non-proliferative b. proliferative c. papilloma d. sclerosing adenosis |
proliferative changes w/out atypia results in > 2 cell layers (luminal and myoepithelial cells filling and distending ducts and lobules)
|
|
|
|
What fibrocystic change often results in bloody discharge?
a. non-proliferative b. proliferative c. papilloma d. sclerosing adenosis |
papilloma due to infarction
|
|
|
|
What fibrocystic changes resemble carcinoma in situ, although they lack sufficient qualitative and quantitative features for a dx of carcinoma?
a. non-proliferative b. proliferative c. papilloma d. sclerosing adenosis |
proliferative changes with atypia: atypical ductal or atypical lobular
|
|
|
|
This fibrocystic change oftne resembles ductal carcionma in situ (DCIS), can be distinguished via limiting extent and only partially filling ducts.
a. atypical lobular hyperplasia b. atypical ductal hyperplasia c. papilloma d. sclerosing adenosis |
atypical ductal hyperplasia
|
|
|
|
This fibrocytstic change is often an incidental finding from biopsies (<5%) with similarities with LCIS, with less distension into lobule.
a. atypical lobular hyperplasia b. atypical ductal hyperplasia c. papilloma d. sclerosing adenosis |
atypical lobular hyperplasia
|
|
|
|
Why is fibrocystic change clinically important, eXCEPT?
a. precursor for cancer b. cause a mass c. produce microcalcifications d. increased risk of cancer |
it is not necessarily a precursor for cancer, but it can increase your risk, cause a mass, and produce microcalcification (detected with mammorgraphy)
|
|
|
|
What can reduce risk of cancer, upon diagnosis of a fibrocystic change, eXCePt?
a. bilateral prophylactic mastectomy b. treatment w/estrogen c. antagonist (tamoxifen) d. biopsy |
all eXCEPT biopsy
|
|
|
|
Malignant breast lumps are often, EXCEPT?
a. hard, gritty b. fixed c. circumscribed d. irregular borders |
hard, gritty, fixed and irregular borders, EXCEPT circumscribed and mobile (benign)
|
|
|
|
What fibrocystic change places a women with a significant increased risk of breast pathology?
a. nonproliferative changes b. sclerosing adenosis c. atypical hyperplasia d. small duct papillomas |
atypical hyperplasia is a significant increased risk
sclerosing adenosis, moderate to florid EP hyperplasia, and small duct papilloma (slight increased risk) non-proliferative changes (cysts, aprocrine metaplasia, fibrosis) and mild epithelial hyperplasia (no increased risk) while carcinoma in situ has a high relative risk X8-10, with an absolute life risk of 25-30% |
|
|
|
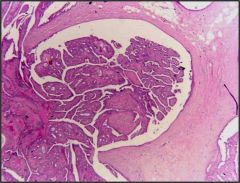
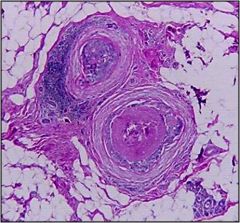
25y/o female presents with firm, circumscribed, mobile mass on her left breast. Upon a mammograph, showing a circumscribed density pushing the surrounding tissue. What is the most common benign tumor of the female breast?
a. fibroadenoma b. intraductal papilloma c. atypical ductal hyperplasia d. atypical lobular hyperplasia |
fibroadenoma arising from specialized stroma of the breast and produces lesion composed of both stromal and epithelial elements
|
|
|
|
Although most intraductal papillary lesions are benign, intraductal papillary carcinoma does exist, what are common presenting symptoms, EXCEPT?
a. blood nipple discharge b. subareolar mass c. mobile mass d. nipple retraction |
benign papillary EP proliferation w/in a duct (subareolar) presents with bloody nipple discharge, a subareolar mass, or nipple retraction
NOT mobile mass that is common in fibroadenoma |
|
|

25y/o female presents with firm, circumscribed, mobile mass on her left breast. Upon a mammograph, showing a circumscribed density pushing the surrounding tissue. What is the most common benign tumor of the female breast?
a. fibroadenoma b. intraductal papilloma c. atypical ductal hyperplasia d. atypical lobular hyperplasia |
fibroadenoma
|
|
|
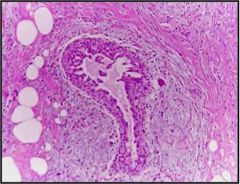
Often benign due to EP proliferation w/in a duct and usually subareolar. Clincally presents with bloody discharge, subareolar mass, and nipple retraction?
a. fibroadenoma b. intraductal papilloma c. papilloma d. atypical lobular hyperplasia |
intraductal papilloma
|
|
|
|
What are the chances a women will develop cancer in the US given a lifespan of 85years?
a. 1:5 b. 1:8 c. 1:100 d. 1:10,000 |
1:8 !! and 1/3 of these women will die of breast cancer
|
|
|
|
About how many new cases of invasive breast cancer are discovered each year?
a. 100,000 b. 175, 000 c. 250, 000 d. 500, 000 |
175, 000 and > 40,000 deaths per year
|
|
|
|
These risk factors increased breast cancer EXCEPT?
a. gender b. age c. family history d. breast feeding |
gender, age, and family hx increase chances of breast cancer (while breast feeding actually decreases the chances)
|
|
|
|
45y/o Caucasion female, discusses her medical history stating she started menarche at an early age, had her first child at 32y/o, smoked for 10 years, and breast feed all her 3 children. She has a family history of breast cancer, stating her mother died of breast cancer at an early age of 42y/o. She want to know what her current risk of breast cancer include.
a. gender b. length of reproductive life c. family history d. race/ethnicity |
all of the above gender, length of repro life (early menarche, family hx, and race/ethnicity.. although breast feeding is beneficial .. other factors that would of increased her risk are age of first live birth (older higher risk), atypical hyperplasia
|
|
|
|
What percentage of breast cancer is usually attributed to inheritance?
a. 5% b. 10% c. 12% d. 20% |
12% to BRCA1 and BRCA2
|
|
|
|
What is the mechanism of action of BRCA1 and BRCA2, EXCEPt?
a. tumor suppression b. transcription regulation c. DNA repair d. blocking mitosis |
tumor suppression, transcription regualtion, and DNA repair.. except mitosis block
|
|
|
|
32y/o caucasian women presents with concerns regarding her chances of developing ovarian cancer due to her mutation in BRCA1, what can she be informed of?
a. 20-40% chance b. 50-60% chance c. 70% chance d. 5% chance |
20-40% chance of developing ovarian cancer, although she is also at high risk of developing pancreas and fallopian tube carcinoma
present as triple negative phenotype: ER/PR negative, no HER2/neu over-expression |
|
|
|
Women have a 10-20% of developing ovarian cancer with BRCA2 mutation, in addition it is high risk for, EXCEPT?
a. prostate b. pancreas c. fallopian tube carcinoma d. male breast cancer |
BRCA2 mutation often associated to male breast cancer, with a 10-20% of female ovarian cancer, high risk for prostate, pancras, stomach and gallbladder, bile duct, pharynx cancer and melanoma
|
|
|
|
Most women who develop sporadic breast cancer have all, EXCEPT?
a. significant family hx b. related hormonal exposure c. postmenopausal d. express E receptors |
related hormonal exposure, postmenopausal, and express E receptors, NO significant family history (except significant family hx0
|
|
|
|
95% of women with breast cancer have:
a. adenocarcinoma b. ductal carcinoma in situ c. comedocarcinoma d. lobular carcinoma in situ |
adenocarcinoma: non-invasive or invasive (ductal or lobular)
|
|
|

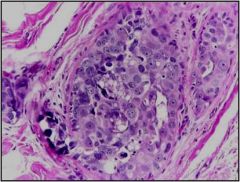
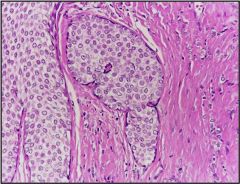
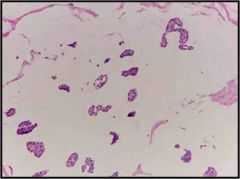
The difference between invasive ductal (figure) and lobular adenocarcinoma is reflected in growth pattern and in tumor biology, more specifically in
a. E-cadherin adhension proteins b. BRCA1 c. BRCA2 d. E receptor susceptibility |
E-cadherin found in invasive ductal only
|
|
|
Considered high grade DCIS with central necrosis included calcification and necrosis
a. adenocarcinoma b. papilloma c. comedocarcinoma d. colloid carcinomaa |
comedocarcinoma
|
|
|
The progression of DCIS is thought to be related to cytologic grade.
a. high grade DCIS b. low grade DCIS c. DCIS calcifications d. comedocarcinoma |
high grade DCIS
|
|
|
The progression of DCIS is thought to be related to cytologic grade.
a. high grade DCIS b. low grade DCIS c. DCIS calcifications d. comedocarcinoma |
low grade DCIS
|
|
|
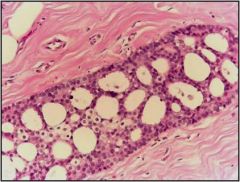
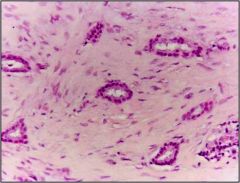
DCIS of malignant glands going through BM
The progression of DCIS is thought to be related to cytologic grade. a. high grade DCIS b. low grade DCIS c. microinvasion d. comedocarcinoma |
microinvasions
|
|
|
40y/o female undergoing a biopsy after calcification were found on breast tissue (mammorgram). She did NOT notice a mass.
Results from abnormal proliferation EP cells in the terminal duct or acini. What are her risk. a. invasive ductal carcinoma b. invasive lobular carcinoma c. neither, she is not at high risk d. medullary carcinoma |
both invasive ductal and lobular carcinoma upto 9X; these can result in the loss of E-cadherin expression; possible treatment includes bilateral prophylactic mastectomy, tamoxifen, or more typical close clinical f/u and mammorgraphic screening
|
|
|
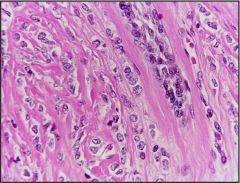
This type of breast cancer accounts for 5-10% (bilateral same percentage) often multicentric, commonly characterized via loss of adhesion protein (E-cadherin)
a. ductal EP cells invade the surrounding stroma showing variable degree of gland formation b. macroscopic patten diffusely infiltrating sometimes with little desmoplasia; uniform cells in single file cords c. associated with lymphocytic inflammation d. soft, gelitanous, rubbary tumors |
a. ductal EP cells invade the surrounding stroma showing variable degree of gland formation (invasive DuCTAL carcinoma)
b. macroscopic patten diffusely infiltrating sometimes with little desmoplasia; uniform cells in single file cords (invasive LOBULAR carcinoma) c. associated with lymphocytic inflammation d. soft, gelitanous, rubbary tumors |
|
|
this type of cancer often has a pattern of spread to all, EXCEPT?
a. lungs b. peritoneal c. retroperitoneal d. ovaries |
peritoneal, retroperitoneal, GI and ovaries seen in invasive lobular carcinoma (remember loss of E-cadherin proteins)
also check CSF due to possible metastisis into brain (leptomeninges) |
|
|
this is a high survival with good prognosis type of breast cancer often seen in older women (median age 71), often grows slowly. how is it usually described
a. ductal EP cells invade the surrounding stroma showing variable degree of gland formation b. macroscopic patten diffusely infiltrating sometimes with little desmoplasia; uniform cells in single file cords c. associated with lymphocytic inflammation d. soft, gelitanous, rubbary tumors |
soft, gelitanous rubbary tumor (colloid -mucinous) the other two with good prognosis include medullary and tubular carcinoma (well formed tubules)
|
|
|
This tumor is often detected in late 40s, with an excellent prognosis due to few metastasis, absent myoepithelial cell layer; tumor is in direct contact with stroma often mistaken for what benign lesion?
a. non proliferative b. proliferative without atypia c. sclerosing adenosis d. proliferative with atypia |
this is tubular carcinoma (well formed tubules) mistaken for benign sclerosing lesion
|
|
|
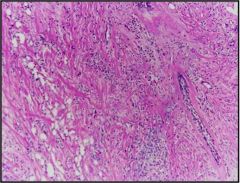
Often associated with poor prognosis, but can be confused for inflammation as it invades DERMAL lymphatics. As a result of the obstruction the breast skin is RED and area is swollen. However, don't be fooled it is NOT inflammation on biopsy.
a. medullary b. inflammatory carcinoma c. tubular carcinoma d. colloid carcinoma |
inflammatory carcinoma (terrible prognosis 3-10% 3yr survival), while the others medullary (associated w/lymphocytic inflammation, soft, circumscribed), colloid (soft, gelatinous, rubbary found in older women), and tubular (few metastasize absent myoEP tumor is in direct contact with stroma)
|
|
|
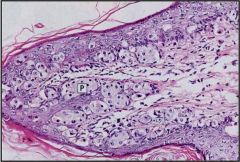
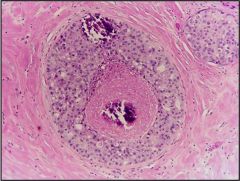
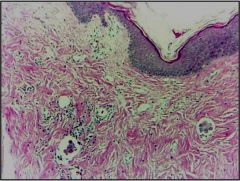
36y/o women presents with fissures, ulces and oozing, wiht unilateral erythematous eruption w/scale crust. After review of the histology you determine that it is more than just eczema. What did you find
a. ductal EP cells invade the surrounding stroma showing variable degree of gland formation b. ductal carcinoma cells infliltrate the epidermis of the nipple so that malignant glandular cells are scattered amid normal squamous cell of epidermis c. proliferation of abnormal EP cells in the terminal ducts or acini d. macroscopic patten diffusely infiltrating sometimes with little desmoplasia; uniform cells in single file cords |
Paget's disease: malignant ductal carcinoma cells infliltrate the epidermis of the nipple so that malignant glandular cells are scattered amid normal squamous cell of epidermis
this condition is a presupposes existence of at least DCIS, while underlying invasive carcinoma may be present (stage determines prognosis) a.invasive ductal carcinoma c.lobular carcinoma in situ d. invasive lobular carcinoma |
|
|
|
males often experience gynecomasstia, enlargement of the breast due to some hormonal imbalance. what is a pathologic cause?
a. hyperestrinism b. etoh OD c. mass d. exogenous hormones |
hyperestrinism often due to cirrhosis of the LIVER, unable to metabollize ESTROGEN, other causes include drug use such as: etoh, marijuana, heroin, anabolic steroids, and some psychoactive drugs
may also be seen with functioning testicualr tumor or PRL secreting pituitary adenoma |
|
|
|
What chromosomal disorder manifests with gynecomastia?
a. Downs syndrome b. Fragile X syndrome c. Klinefelters Syndrome d. Edward's syndrome |
Klinefelter's syndrome (XXY karyotype)
|
|
|
Often found in males due to cirrhosis of the liver, etoh, marijuana, heroine or use of anabolic steroids. In addition, seen in kleinfelters syndrome or due to PRL secreting pituitary tumor.
a. stromal tumor b. phyllodes tumors c. gynecomastia d. fat necrosis |
gynecomastia
males have scant amount of breast tissue, so tumor invasion on the chest wall is more common, and men usually present with higher stage disease |
|
|
|
What is the most common STD in adult females?
a. n. gonorrhea b. chlamydia trachomatis c. treponemia pallidum d. herpes simplex II |
chlamydia trachomatis
|
|
|
|
25y/o female complains of a painless single chancre on the vulva, about 9 mm. She has noticed that it is beginning to ulcerate. You proceed to use what test for identification.
a. biopsy b. giemsa stain c. darkfield d. PAS stain |
treponemia pallidum usually presents as a painless single chancre, often seen with darkfield microscopy; give her PCN for txt; while HSVII is multiple vesicles become ulcerated PAiNFUL
|
|
|
|
There are several conditions that often simulate dystrophies of the vulva, EXCEPT:
a. inflammatory dermatosis (eczema, psorosis) b. carcinoma in situ c. syhillis d. Paget's disease |
NOT syphillis, this leads to single painless Chancres
|
|
|
|
After her gyne exam, you ntotice a vulvar area become smooth with a glazed red appearance. 58y/o women is menopausal, noticed skin becoming pale gray, patchement like (thining). What can be suspected histologically, with increased risk for infection and trauma?
a. atrophic dystrophy b. hyperplastic dystrophy c. hyperplastic EP changes d. condyloma acuminatum |
atrophic dystrohy common in menopausal women may have a small risk of developing squamous cell CA
the opposite is EP thickening of hyperplasia (hyperkeratosis) |
|
|
|
Because 1-5% of pt with atypia develop carcionma, when is biopsy indicated?
a. all vulvar lesions with atrophic dystrophy b. all vulvar lesions appearing as white plaque c. all vulvar lesions with marked hyperkeratosis d. all vulvar lesions with hyperplastic changes |
all vulvar lesions appearing as white plaque
|
|
|
|
The most common vulvar cancer is, squamous cell carcinoma potential risk factors, EXCEPT
a. IUD use b. HPV type 16 c. smoking d. immune deficiency |
all EXCEPT IUD use
|
|
|
|
What causes condyloma acuminatum, wart like epidermal manifestation?
a. HPV b. HSVII c. chlamydia trachomatis d. treponema pallidum d. |
HPV
|
|
|
|
This condition common in 20-24y/o is often confused with a more serious condition, verrucous carcinoma highly differentiated, but rarely metastasizes appears treelike proliferation of stratified sq EP and vacuolization of EP (koilocytosis) ?
a. extramammary Paget's disease b. condyloma acuminatum c. lymphogranuloma venereum d. malignant melanoma |
condyloma acuminatum (epidermal manifestation) wart-like due to HPV
|
|
|
|
This condition is often treated via wide excision due to its rare metastasize, although it is highly differentiated.
a. extramammary Paget's disease b. verrucous carcinoma c. lymphogranuloma venereum d. malignant melanoma |
verrucous carcinoma
|
|
|
|
65 y/o female presents with red, crusted, sharply demarcated, map-like area on labia majora. After a histology of the are you notice large anaplastic tumor cells lying singly or in cluster w/in the epidermis and appendages. You see clear halo of cytoplasmic mucopolysaccheride. what test did you use to identify disorder?
a. darkfield b. biopsy c. PAS stain d. giemsa stain |
may be underlying infiltrating carcinoma
PAS stain to diagnose extramammary Paget's disease |
|
|
|
63y/o female presents with similar complaints often seen with Paget's disease (extramammary). You get a negative PAS stain, what alternate test can be used resulting in brown cytoplasmic granules?
a. biopsy b. giemsa c. darkfield d. fontana stain |
fontana stain useful with melanomas -- malignant melanoma stains for melanin
|
|
|
|
After completing a gyne exam, you describe a suppurative green, but superficial inflammation. The vagina and cervical mucosa are bright, fiery red (strawberry appearance). You are concerned that this infection can extend into vulva, perineum, or even the bladder. Upon review of lab it is noted that this is a Jerky Motile organims?
a. chlamydia trachomatis b. treponema pallidum c. neisseria gonorrhea d. trichomonas vaginalis |
trichomona vaginalis large, flagellated, protozoan
|
|
|
|
Squamous cell carcinoma compromises 95% of vaginal carcinomas, affecting the upper posterior vaginal most often, risking invasion into cervix, bladder, and rectum. Clinical symptoms are often irregular spotting, discharge, urinary or rectal fistulas> Upper lesions often metastasize to?
a. iliac nodes b. inguinal nodes c. lumbar nodes d. mesenteric nodes |
iliac nodes, while lower 2/3 of the vagina metastasize to inguinal nodes
|
|
|
|
16y/o presents with a tumor on the anterior wall of the upper vagina?
a. clear cell adenocarcionma b. adenocarcinoma c. vaginal adenosis d. sarcoma botryoids |
adenocarcionma (rare) occur in anterior vaginal wall
|
|
|
|
35y/o female states 6 years ago she was treated with DES during pregnancy to prevent an abortion. What king of tumor is she at risk for?
a. composed of vacuolated, gland forming cells with large clear cytoplasm |
clear cell carcinoma: composed of vacuolated, gland forming cells w/large clear cytoplasm in the CERVIX, rare unless exposed to DES
|
|
|
|
This condition often leads to clear cell carcinoma, often linked to the use of DES, preventing aborting. Glandular EP is present beneath the squamous EP or replacing squamous EP?
a. gartner's duct cyst b. thrichomonal vaginitis c. vaginal adenosis d. clear cell adenocarcinoma |
vaginal adenosis often leads to clear cell carcinoma due to its association with DES-exposure (inhibits Mullerian structure develoment: uterus, cervix, tubes, upper 1/3 vagina)
|
|
|
|
Extension of cervical carcinoma to the vagina is much more common than primary malignancies of the vagina.
a. true b. false |
true
|
|
|
|
4y/o girl brought in by her mom, stating there are "grape-like clusters" protruding from daughters vagina (polypoid, round, bulky masses). What is the danger of these tumors?
a. penetrate into peritoneal cavity b. poor development c. obstruct urinary tract d. hemorrhage |
penetrate into peritoneal cavity and obstruct the urinary tract
|
|
|
|
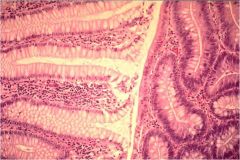
Endometrial hypeplasia (glands > stroma, irregular gland shape and size) is often seen in near menopause or post menopausal women due to the prolonged Estrogenic stimulation of cells. What clinical manifestations are common:
a. pelvic pain b. excessive uterine bleeding c. dysuria d. asymptomatic |
excessive uterine bleeding due to the increased E stimulation on the endometrium
|
|
|
|
Because complex atypical hyperplasia of endometrium is pre-cancerous (adenocarcionma risk) it is important to differentiate it from complex and simple hyperplasia, what are distinguishing features?
a. glands separated by abundant stroma b. less stroma, glands crowded c. enlarged nuclei with prominent nucleoi and coarse chromatin d. cystic glandular dilation |
a. simple hyperplasia
b. complex hyperplasia c. atypical hyperplasia -enlarged nuclei with prominent nucleoi and coarse chromatin d. simple hyperplasia |
|
|
|
Why is it important to get further evaluation of enlarged ovaries in a postmenopausal women?
a. in postmenopausal women the endometrium normally atrophies b. in postmenopaual women there is a higher risk breast cancer c. in postmenopausal women the endometrium normally hypertrophies d. in postmenopausal women there is an decreased risk for endometrial polyps |
a. in postmenopausal women the endometrium normally atrophies (true) so any deviation from this is suspicious for cancer
b. in postmenopaual women there is a higher risk breast cancer (false) c. in postmenopausal women the endometrium normally hypertrophies (false) it atrophies d. in postmenopausal women there is an decreased risk for endometrial polyps (false) endometrial polyps are more common at or near menopause |
|
|
|
Endometrial polyps result in funcitonal endometrium and hyperplastic endometrium, they are often asymptomatic and larger ones can ulcerate or bleed, when are they more prevalent?
a. during menstruation in young adults b. during early puberty c. premenopausal only d. at or near menopause |
at or near menopause
|
|
|
|
How can you differentiate between benign and malignant tumors of the uterus and ovaries, microscopically, malignant will have?
a. few mitosis b. irregular nuclei (pleomorphic) c. cells resemble cells from which they arose d. regular nuceli |
irregular neuclie (pleomorphic), many mitosis, cells difficult to identify as to orgin
all other are benign characteristics: few mitosis, regular nuclei, cells resemble cells from which they arose |
|
|
|
30y/o pregnant female presents asymptomatic, although she has 2 leiomyomas (fibroids), what can you say about their microscopic make up?
a. sessile soft masses that project into the endometiral cavity b. mild glandular crowding and cystic glandular dilation c. well-differentiated, regular, spindle shaped smooth muscle cells associated w/hyalinization d. glandular architecture with admixed solid areas |
c. leiomyoma (fibroid) often stimulated via E, rapidly increase during pregnancy and shrink during menopause -- often have multiple lesions and may cause early onset of labor
can be asymptomatic or profused menstrual bleeding or irregular bleeding a. endometrial polyps b. simple hyperplasia w/out atypia d. endometrial carcionoma (moderately differentiated0 |
|
|
|
With the increase of endometrial carcinoma to about 10% of cancers in women, when do they mostly occur?
a. pre menopause b. post menopause c. child bearing years d. any stage of reproduction |
post menopause, because they are often stimulated via Estrogen often present as localized polypoid tumors or diffusely involving endometrial surface
|
|
|
|
With the increase of endometrial carcinoma (EP origin) to about 10% of cancers in women, what are targeted risk factors, EXCEPT?
a. obesity b. DM/HTN c. hx anovulatory cycle (infertility) d. smoker |
a. obesity
b. DM/HTN c. hx anovulatory cycle (infertility) d. smoker (NO!!) |
|
|
|
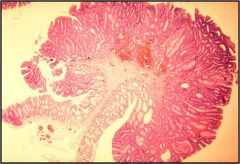
Endometrial adenocarcionma often presents as :
a. sharply circumscribed round firm gray-white matter b. fungating mass in the fundus of the uterus c. numerous clear cysts d. glandular and stromal elements differentiate into muscle, cartilage, and even bone |
FUNGATING mass in the fundus of the uterus
a. leiomyoma (fibroid) c. polyctystic ovaries d. mixed mesodermal tumor (rare) |
|
|
|
The grade of the tumor often describes:
a. the extent of the disease b. the organization of the tumor c. how much the tumor looks like normal tissue d. the size of the tumor |
how much the tumor looks like normal tissue, all the other are describing the STAGE of the tumor
|
|
|
|
The stage of the tumor often describes the extent of the disease, includes all, EXCEPT:
a. size of tumor b. lymph involvement c. metastesis d. poorly differentiated |
poorly differentiated describes the grade of the tumor or how much it looks like normal often described as the behavior of the tumor, while the stage of the tumor is the organization/extent of the tumor such as the size, invasive/non-invasive, lymph involvement, metastesis etc.
|
|
|
|
56y/o post menopausal women complains of irregular vaginal bleeding accompanied by leukorrhea (purulent discharge). What is a MAJOR determinant of this prognosis, if microscopically you see malignant glandular and squamous elements.
a. grade b. stage c. grade and stage equally d. neither are important |
b. stage if it is confined to the corpus uteri or extends outside the uterus and true pelvis involving mucosa of the bladder or rectum (poor prognosis)
She has mixed adenosquamous carcionoma as presented via irregular bleeding accompanied by leukorrhea (purulent discharge), although it can often be asymptomatic. Her prognosis is dependent on the clinical STAGE of the disease, and a lesser extent by the grade (differentiation) |
|
|
|
56y/o female presents with postmenopausal bleeding. She adds that she had radiation treatment about 2 years age for breast cancer. You suspect a highly malignant and aggressive cancer, although it is rare. What type of cells will you find.
a. mullerian mesodermal b. myometrium c. squamous elements d. glandular |
a. mullerian meosdermal consist of glandular (adenocarcionoma) and stromal (sarcoma) elements that often differentiate into muscle, cartilage, and even bone
mixed mesodermal tumor, although rare they are very aggressive b/c can spread outside the uterus and metastasize (25-30% 5 yr survival) |
|
|
|
23y/o female present with lower abdominal pain 6 weeks after previous menstrual period. You diligently get a pregnancy test, with increased beta hCG. What are possible complications?
a. suppurative salpingiits b. rupture and intrauterine bleed c. hydatid cyst of morgagni d. follicular cyst |
she has an ectopic pregnancy possible causes include PID, endometriosis, altered tubal mobility can result in hematosalpinx (blood in tube)
complications include: RUPTURE and INTRAUTERINE BLEED suppurative salpingitis (infection) hyatid cyts of morgagni (rare carcinoma) follicular cyst (comm benign in ovaries not fallopian tubes) |
|
|
|
These cysts are very common, often originating in unruptured graafian follicle, or ruptured follicles that immediately seal. Often with a bright yellow wall and blood in lumen, consistent with corpus luteum cyst.
a. non-neoplastic cyst b. follicular cyst c. polycystic cyst |
follicular cyst very common (BENIGN)
|
|
|
|
Polycystic ovaries are associated with these 3 syndromes, often occurring during the second or third decade of life, EXCEPT:
a. Stein-Leventhal syndrome b. metabolic syndrome c. abndomral bleeding d. virilism |
a. Stein-Leventhal syndrome YES
b. metabolic syndrome NO c. abndomral bleeding YES d. virilism YES |
|
|
|
Anovulation is common with polycystic ovaries, as the cystic walls consist of granulosa cells w/leutinizing theca interna, what is absent?
a. Graafian follicle b. LH c. Estrogen d. corpora lutea |
corpora lutea resulting in anovulation, LH is being secreted in a continues basis rather than cyclic; syndrome can be corrected via ovarian wedge resection -- making a hole allowing ovulation to occur!!
|
|
|
|
The ovaries are often enlarged, contain multiple cysts and show a thick tough white outer tunica. clinically presenting as anovulation, and associated with Stein-Leventhal syndrome, abnormal bleeding, and virilism.
a. non-neoplastic cyst b. follicular cyst c. polycystic ovaries |
polycystic ovaries
|
|
|
|
23y/o female presents to the clinic stating she recently got married and is having a hard time getting pregnant. In addition, she is complaining of amenorrhea, obesity, hirstuism. What is key during the physical exam?
a. listen heart sounds b. complete a pregnancy test c. palpate ovaries d. percuss lungs |
palpate ovaries she might have polycystic ovaries resulting in anovulation where she can't ovulate and is at risk for infertility
|
|
|
|
Metastasis to the ovaries is frequently from?
a. breast and liver b. liver and abdomen c. lung and liver d. breast and abdomen |
breast and abdomen (Krukenberg- singlet ring cells hematogenous spread of gastric CA)
|
|
|
|
What three areas of the ovaries are often inflicted with malignant cells, EXCEPT?
a. stroma b. surface epithelial c. sex cord stroma d. ovum or germ cells b. |
a. stroma NO
b. surface epithelial YES c. sex cord stroma YES d. ovum or germ cells YES |
|
|
|
Common surface EP cell ovarian tumors, EXCEPT:
a. teratoma b. serous tumor c. mucinious tumor d. clear cell tumor |
a. teratoma GERM CELL
b. serous tumor EP c. mucinious tumor EP d. clear cell tumor EP |
|
|
|
Sex cord tumors of the ovaries, EXCEPT:
a. choriocarcinoma b. fibroma c. granulosa theca cell d. Sertoli-Leydig cell |
a. choriocarcinoma -- GERM CELL
b. fibroma - SCS c. granulosa theca cell - SCS d. Sertoli-Leydig cell - SCS |
|
|
|
This is a common bilateral tumor of the ovaries, often differentiated due to the presence of ciliated EP and Psammoma bodies (concentric calcifications). An indication of malignancy is often due to papillary tendency, solid EP surface projecting masses, solid lobules, nodulating of capsule, and infiltration. Malignant lesions have a 10--20% 10yr survival.
a. serous tumor b. mucinous tumor c. cystadenfibroma d. clear cell tumor |
Yes all are surface EP cell tumors of the ovaries, but this one in particular has ciliated EP (sometimes) lined by tall, columnar cells with Psammoma bodies ** malignancy is often represented via papillary tendancy and infiltration
a. serous tumor b. mucinous tumor c. cystadenfibroma d. clear cell tumor |
|
|
|
Unlike serous tumors of the ovaries that are more malignant (55%) than benign (30%) and bilateral. These are benign> malignant and unilateral. They do share Psammoma bodies characteristic, but also differ in their cell type as these have non-ciliated tall columnar cells. What other two distinctions are important for diagnosis?
a. they result in increased papillary infiltration b. they produce larger cystic masses c. multilocular d. small masses |
Mucionus tumors produce LARGE cystic masses, unlike serous tumors which result in smaller masses and often multiple cavities (multiocular)
They are often difficult to differentiate b/w histologically benign, borderline, and malignant unlike serous which are more straight forward |
|
|
|
This ovarian tumor has a five year survival is very uncommon, often characterized via large EP cells w/abundant clear cytoplasm. Often of mullerian duct origin?
a. serous b. mucinous c. clear cell d. cystadenofibroma |
clear cell carcinoma (uncommon), while cystadenofibroma is benign
|
|
|
|
One of the benign tumors of the EP surface of ovaries, showing fibrous stroma with pronounced proliferation and malignant transformation is rare.
a. clear cell b. mucinous c. cystadenofibroma d. brenner |
cystadenofibroma (ENIGN)
|
|
|
|
Often is the 2% of ovarian tumors of EP surface, usually solid and unilateral, benign. Characterized via dense fibrous strom punctuated by nests of TRANSITIONAL cells resembling those lining the bladder.
a. clear cell b. mucinous c. cystadenofibroma d. brenner |
brenner (BENIGN)
|
|
|
|
43y/o female presents with abdominal pain and abdominal enlargement. As you examine the abdomen you discover large, bulky masses evoking acute abdomen. What is one of you major concerns?
a. surface EP ovarian carcionma b. germ cell carcinoma c. sex cord stroma carcinoma d. metastasis to ovaries |
surface EP ovarian carcinoma
|
|
|
|
23y/o female presents with abdominal pain and mass, with some GI complaints or menstrual disturbances. You diagnose it as a dermoid cyst as it contains skin with adnexal structrure?
a. carcinoid b. dysgermimona c. teratoma d. choriocarcinoma |
teratoma (BENIGN) rarely malignant (less than 1% transform)
remember there are also monodermal teratomas such as: a. struma ovarii: mature thyroid tissue (hyperfunciton) b. carcinoid (intestinal EP) carcinoid syndrome 5HT |
|
|
|
18y/o female presents with a SOLID ovarian tumor. Do to her age, you are concerned of a malignancy and METASTASES. An ovarian tumor that often contains embryonic elements of 3 germ layers, often includes this distinguishing element?
a. dermoid cyst b. neuroEP c. thyroid tissue d. intestinal EP |
neuro EP because if it is in this young age and malignant/metastese it is immature (malignant) teratoma rare, but with metasteses potential
|
|
|
|
26y/o female presents with menstrual bleeding frequently, as well as positive hCG, although she sates she is not pregnant as she is on OC's. After micro exam of cells you notice distinct polyhedral tumor cells composed of large, vesicular cells with cleared cytoplasm with well defined cell boundaries and centrally placed regular nuclei. IN addition, there are fibrous stroma infiltrated via lymphcytes!!
a. mondermal teratoma b. immature teratoma c. dysgerminoma d. choriocarcinoma |
dysgerminoma (counterpart of seminoma in testes)
this is a malignant tumor but only 1/3 are aggressive |
|
|
|
6y/o girl presents with abdominal pain and pelvic mass. After histology review, you notice distinguishing Schiller-Duvall bodies (papillary structures focallly). You are concerned about tumor groiwng rapidly and aggressively. What do you suspect, although is is rare?
a. increased 5HT b. neuroEP c. ovarian teratoma d. rich in fetoprotein and antitrypsin |
rich in fetoprotein and antitrypsin (endodermal sinus (yolk sac) tumor
|
|
|
|
30y/o female recently recovered from an ectopic pregnancy, what is an adjunct cancer you must keep on the look out for?
a. teratoma b. endodermal sinus c. choriocarcinoma d. dysgerminoma |
choriocarcinoma
|
|
|
|
THese ovarian tumors are often endocrinologically active secreting Estrogen or androgens, although only one form results in malignancy. What kind of ovarian tumors?
a. surface EP b. germ cell c. sex-cord stromal d. ovarian metastasis |
sex cord stromal tumor: granulosa-theca cell tumors (chance of malignancy in GRANULOSA cell type)
|
|
|
|
32y/o female presents with Meig's syndrome, as a result of a 6cm fibroma, or sex cord stromal tumor, solid, hard, gray white mass covered by intact ovarian serosa. What two clinical findings are helpful with diagnosis?
a. abdominal pain and pelvic mass b. ascites and RS pleural effusion c. menstrual bleeding and increased hCG d. abdominal pain and GI complaints |
ascites and RS pleural effusion (hydrothorax)
a. abdominal pain and pelvic mass --endodermal sinus tumor c. menstrual bleeding and increased hCG --dysgerminoma d. abdominal pain and GI complaints -- teratoma |
|
|

74 year-old woman with gastrointestinal bleeding. Colonoscopy demonstrated this 1cm polyp on a stalk, amidst several diverticula. The polyp grossly appeared to be a pedunculated adenoma on a broad stalk, or even a lipoma, but histologically proved to be hyperplastic (and therefore not a "true" polyp).
a. non-neoplastic polyp b. neoplastic polyp c. inflammatory polyp d. hamartomatous polyps |
non-neoplastic polyps (or hyperplastic polyps are often have NO malignant potential)
Adenomatous polyps, but not hyperplastic polyps, traditionally are considered to be precursors of colorectal cancer. But new research suggests that hyperplastic polyps also may be associated with some colorectal cancers. These cancers are particularly likely to have microsatellite instability (MSI) -- an abnormality in non-protein-coding portions of DNA -- and tend to occur in the right side of the colon. |
|
|
Neoplastic polyps, adenomatous can carry malignant potential since the dysplasia carries gene mutations leading to the development of invasive CA. The malignant risk correlate with:
a. size b. severity of dysplasia c. amount of villous architecture d. potential to invade strom |
they DO not have the potential to invade stroma, but malignant risk is correlated with:
a. size b. severity of dysplasia c. amount of villous architecture remember they also DO NOT metastasize |
|
|
Often related to malignancy risk, amount of villous architecture:
a. tubular adneoma b. villous adenoma c. tubulovillous adenoma d. peduncated |
tubular adenoma round gland like architecture
|
|
|
neoplastic adenomatous dysplasia has a higher malignant correlation based on this amount of villous architecture?
a. tubular adenoma b. villous adenoma c. tubulovillous adenoma d. hyperplastic polyp |
villous adenoma (finger-like architecture)
|
|
|
neoplastic adenomatous dysplasia has a higher malignant correlation based on this amount of villous architecture, more importantly has a larger and higher risk for malignancy?
a. tubular adenoma b. villous adenoma c. tubulovillous adenoma d. hyperplastic polyp |
villous adenoma HIGHER risk for malignancy
|
|
|

autosomal DOMINANT, familial adenomatous polyposis, results in the collection of innumerable adenomatous polyps in the colon progressing to colon adenocarcionma about 100% of the tiime. What is appropriate treatment?
a. biopsy b. chemotherapy c. resection d. colectomy |
colectomy
|
|
|

18 y/o female presents to the clinic with non-specific symptoms such as rectal bleeding (hematochezia), diarrhea, or abdominal pain. Because she is such a young pt you get her history and realized her family has a condition, which suggests 100% risk of colon adenocarcinoma. what would you want to test in this pt.
|
a. FAP
b. HNPCC c. gastric CA d. esophageal CA |
most likely familial adenomatous polyposis (innumerable adenomatous polyps)
|
|
|
48-year-old woman has noted a small amount of irregular vaginal bleeding for the past 2 months. She has a pelvic examination that reveals no cervical lesions, and a Pap smear that shows no abnormal cells. Next, an endometrial biopsy is performed, and there is microscopic evidence for endometrial hyperplasia. An abdominal ultrasound reveals a solid right ovarian mass. Which of the following neoplasms is this woman is most likely to have?
a. Mature cystic teratoma b. Choriocarcinoma c. Sertoli-Leydig cell tumor d. Granulosa-Theca cell tumor e. Krukenberg tumor f. Cystadenocarcinoma |
D, Granulosa-Theca cell tumors characteristically produce estrogen which can lead to endometrial hyperplasia or carcinoma.
|
|
|
|
36-year-old woman has had episodes of lower abdominal and pelvic pain for the past 10 years. A bimanual pelvic examination reveals no abnormalities. A Pap smear is negative. She has an abdominal ultrasound scan that reveals no abnormalities. Finally, she undergoes laparoscopy, and her physician notes the presence of several 0.2 to 0.5 cm brown lesions located over the serosal surfaces of the uterus, fallopian tubes, and appendix. These lesions are excised. Which of the following microscopic findings is most likely to be present in these lesions?
a. Endometrial glands and stroma b. Mesothelioma c. Metastatic carcinoma d. Small capillary proliferation e. Caseating granulomas |
endometrial glands and stroma
endometriosis |
|
|
|
28-year-old woman goes to her physician for a routine examination. She is sexually active. Pelvic examination reveals no abnormalities. A Pap smear is obtained. The cytopathology report indicates the presence of severely dysplastic cells. A biopsy of the cervix is performed, and on microscopic examination shows cervical intraepithelial neoplasia III (CIN III). Infection with which of the following organisms is most likely to cause her disease?
a. Herpes simplex virus infection b. Epstein-Barr virus c. Candida albicans d. Human papillomavirus e. Trichomonas vaginalis f. Gardnerella vaginalis |
HPV
|
|
|
|
23-year-old woman goes to the emergency room because of the sudden onset of lower abdominal pain. Pelvic examination reveals a normal sized uterus and normal appearing cervix and vagina. However, there is marked tenderness upon palpation of the left adnexal region. A transvaginal ultrasound demonstrates no intrauterine gestational sac, but there is a 2 cm left adnexal mass. Culdoscocentesis yields bloody fluid. Which of the following is most useful procedure to perform at this point for the patient?
a. Serum complement determination b. Urinalysis with microscopic examination c. Pap smear d. Serum beta-HCG e. Endometrial biopsy f. WBC count |
D, you would strongly suspect ectopic pregnancy in this case.
|
|
|
|
39-year-old woman had noted intermenstrual spotting of blood for the past 3 months. On pelvic examination, she is found to have a nodular 2 x 3 cm mass in the upper vagina. Biopsy of the mass is performed and on microscopic examination shows a clear cell carcinoma. Which of the following risk factors probably preceded development of this carcinoma?
a. Human papilloma virus infection b. Previous endometriosis c. Irregular menstrual cycles d. Exposure to diethylstilbestrol in utero e. Precocious pseudopuberty |
exposure to diethylstilbestrol in utero
|
|
|
|
32-year-old G3 P2 pregnant woman goes for a routine prenatal check at 12 weeks. On physical examination she is found to be large for dates, and no fetal heart tones are audible. An ultrasound is performed and revealed that no fetus was present, only many echogenic cystic areas within the uterus. Which of the following is the most likely diagnosis?
a. Invasive mole b. Partial hydatidiform mole c. Placental site trophoblastic tumor d. Choriocarcinoma e. Complete hydatidiform mole |
E, complete moles are composed entirely of grape-like chorionic villi as opposed to partial moles which do contain a fetus (it is triploid like the trophoblast tissue and thus abnormal).
|
|
|
|
38-year-old woman goes to her physician for a routine checkup. On physical examination there are no abnormal findings. A Pap smear is taken and cytologically there are dysplastic cells present. A cervical biopsy is performed. Microscopic examination shows dysplasia involving the full thickness of the cervical epithelium. Which of the following is the most likely diagnosis?
a. Cervical intraepithelial neoplasia III b. Severe chronic cervicitis with Herpes simplex virus c. Previous diethylstilbestrol (DES) exposure d. Endocervical adenocarcinoma e. Extramammary Paget disease |
cervical intraEP neoplasia III
|
|
|
|
38 year old female has dysmenorrhea for months. The uterus appears to be symmetrically enlarged on pelvic examination and by ultrasound. This microscopic appearance of a section from the myometrium is most consistent with:
a. Invasive mole b. Endometriosis c. Ectopic pregnancy d. Teratoma e. Adenomyosis |
adenomyosis
|
|
|
|
27 year old woman who is actively training for a marathon presents with the new onset of a painful lump in the upper outer quadrant of her right breast. A mammogram shows an irregular mass with focal areas of calcification. An excised biopsy reveals a localized area of granulation tissue and numerous lipid-laden macrophages surrounding necrotic adipocytes. Which of the following is the most likely diagnosis?
a. Acute mastitis b. Ectasia c. Enzymatic fat necrosis d. Foreign-body reaction e. Traumatic fat necrosis |
traumatic fat necrosis
|
|
|
|
breast lesion shown here grossly was palpable in the upper outer quadrant of a 28 year old female. The lesion was firm, rubbery, and movable. No axillary lymph nodes were palpable. Mammography confirmed the presence of the lesion, which had no microcalcifications, and revealed no lesions of the opposite breast. The best diagnosis is:
a. Phyllodes tumor b. Lobular carcinoma in situ c. Fibroadenoma d. Paget's disease of breast e. Infiltrating ductal carcinoma |
fibroadenoma
|
|
|
|
23-year old woman presents with a rubbery, freely movable 2-cm mass in the upper outer quadrant of the left breast. Which of the following histologic features is most likely to be seen when examining a biopsy specimen from this mass?
a. Large numbers of neutrophils b. Large numbers of plasma cells c. Duct ectasia with inspisssation of breast secretions d. Necrotic fat surrounded by lipid-laden macrophages e. A mixture of fibrous tissue and ducts |
a mixture of fibrous tissue and ducts
|
|
|
|
46-year old woman presents with a 4-month history of discharge from the nipple. An excisional biopsy of the nipple area reveals infiltration of the nipple by large cells with clear cytoplasm. These cells are found both singly and in small clusters in the epidermis and are PAS-positive and diastase-resistant. Which of the following is the most likely diagnosis?
a. Ductal papilloma b. Eczematous inflammation c. Mammary duct ectasia d. Paget’s disease e. Inflammatory carcinoma |
mammary duct ectasia
|
|
|
|
35 year old woman who underwent a modified radical mastectomy of her right breast for infiltrating ductal carcinoma 2 years ago presents with enlargement of her right breast. The breast has a swollen, red-discolored appearance. It is diffusely indurated and tender on palpation. Multiple axillary lymph nodes are palpable in the lower axilla. The working clinical diagnosis is inflammatory carcinoma. Which of the following histologic features is most characteristic of this clinical diagnosis?
a. Duct ectasia with numerous plasma cells b. Extensive invasion of dermal lymphatics c. Infiltrating malignant ducts surrounded by numerous neutrophils d. Malignant vascular tumor forming slit-like spaces e. Marked dermal desmoplasia |
extensive invasion of dermal lymphatics
|
|
|

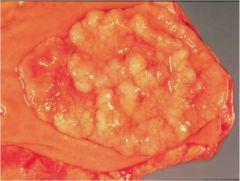
6. The skin overlying the breast of a 61 year old female is indurated, roughened, and reddish-orange. There is nipple retraction. The gross appearance of the cut surface of the mastectomy specimen is shown here. The best diagnosis is:
a. Infiltrating ductal carcinoma b. Intraductal carcinoma c. Phyllodes tumor d. Lobar carcinoma in situ e. Sclerosing adenosis |
infiltrating ductal carcinoma
|
|