Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
41 Cards in this Set
- Front
- Back
|
Plasma cell disorders are often called __________.
|
Plasma cell dyscrasias
|
|
|
What is multiple myeloma?
|
Malignant proliferation of plasma cells in marrow.
|
|
|
What is the most common primary malignancy of bone?
|
Multiple myeloma
|
|
|
In multiple myeloma, what serum molecule is often seen in high concentrations?
|
IL-6
|
|
|
IL-6 is an important growth factor for ______________.
|
plasma cells
|
|
|
Multiple myeloma plasma cells can activate what other cell type? What is the result?
|
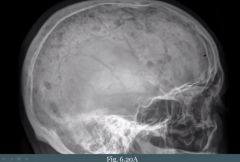
Osteoclasts through their RANK receptor (Osteoclast Activating Factor). They eat away at bone resulting in 'punched-out' lesions seen on X-ray. Increased risk of fracture. Lesions results in bone pain and hypercalcemia.
|
|
|
Where do we typically see the 'punched-out' lytic bone lesions associated with multiple myeloma?
|
(1) Vertebrae
(2) Skull |
|
|
The plasma cells of multiple myeloma can produce what?
|
(1) Osteoclast activating factor
(2) Immunoglobulins. |
|
|
A patient has increased serum protein and you can't determine the cause. What could you do?
|
Serum Protein Electrophoresis (SPEP)
|
|
|
How is the gamma band on SPEP in normal circumstances? How does it look in multiple myeloma?
|
Wide and not as high as albumin peak.
A sharp tall spike in the gamma region. |
|
|
What does M-spike in multiple myeloma mean?
|
Monoclonal
|
|
|
The M-spike on SPEP in multiple myeloma is most commonly due to what Ig?
|
Monoclonal IgG or IgA
|
|
|
What is an important complication of multiple myeloma?
|
Monoclonal plasma cells --> Lacks antigenic diversity --> Infection is the MC cause of death
|
|
|
What is a complication of multiple myeloma involving having too much protein in the blood?
|
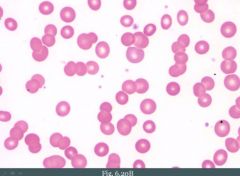
Rouleax formation on smear. Increased serum protein decreases charge between RBCs.
|
|
|
Aside from infection and rouleax formation, what is another possible complication of multiple myeloma?
|
Primary AL amyloidosis. Free light chains circulates in serum and deposit in tissue.
|
|
|
The proteins in primary amyloidosis associated with multiple myeloma can deposit in tissues. What else can the free chains do?
|
Excreted in urine as Bence-Jones protein (proteinuria). Deposition in kidney tubules leads to risk of renal failure (myeloma kidney).
|
|
|
You see a patient in your clinic with a high serum protein. SPEP shows M spike. You suspect MM. You don't find any lytic lesions, hypercalcemia, amyloid or proteinuria. What is going on?
|
MGUS; Monoclonal Gammopathy of Undetermined Significance
|
|
|
MGUS is common in the ___________.
|
elderly
|
|
|
MGUS is seen in ___% of ____-year-old individuals.
|
5%; 70yo
|
|
|
__% of patients with MGUS develop multiple myeloma each year.
|
1%
|
|
|
MGUS could almost be described as being a __________.
|
dysplasia
|
|
|
What is Waldenströms macroglobulinemia?
|
B-cell LYMPHOMA with monoclonal IgM production (macroglobulin = IgM, because it is big)
|
|
|
How do patients with Waldenströms macroglobulinemia present as?
|
(1) Generalized LAD (it is a lymphoma); lytic bone lesions would be absent
(2) Increased serum protein with M spike (comprised of IgM) (3) Hyperviscosity due to high IgM. Visual and neurologic deficits show (e.g., retinal hemorrhage or stroke). (4) Bleeding (defective PLT aggregation in hyperviscosity) |
|
|
When patients have acute complications in Waldenstroms macroglobulinemia we can treat them with?
|
Plasmapheresis. Removes IgM from serum.
|
|
|
Langerhans cells are _______?
|
Specialized dendritic cells found predominantly in the skin.
|
|
|
Langerhans cells are derived from?
|
Bone marrow monocytes
|
|
|
Langerhans cell present antigens to?
|
Naive T-cells
|
|
|
A tumor of langerhans cells is called?
|
Langerhans cell histiocytosis
|
|
|
What is characteristically seen in Langerhans cell histiocytosis?
|
Birbeck graunles on EM (tennis rackets).
|
|
|
Cells in langerhans cell histiocytosis have what markers?
|
CD1a+, S100+ by immunohistochemistry.
|
|
|
How many subtypes of langerhans cell histiocytosis do we have?
|
3
|
|
|
How could you know that a langerhans cell histiocytosis disease is malignant?
|
If the disease is named after someone, the proliferation is usually malignant.
|
|
|
Malignant proliferations in langerhans cell histiocytosis usually involve what?
|
The skin. Shows up as a rash.
|
|
|
Memory help: If the langerhans cell histiocytosis has two names in it, it is usually seen in?
|
It will usually be seen in children less than 2 (infants)
If there is three peoples names it is usually seen in children greater than the age of 3. |
|
|
Letterer-Siwe classic presentation?
|
Classically presents as skin rash and cystic skeletal defects in an infant (infant < 2 yrs old).
|
|
|
What organs are involved in Letterer-Siwe disease? What is the prognosis?
|
Multiple organs may be involved.
Letterer-Siwe is rapidly fatal. |
|
|
Eosinophilic granuloma is a ___________ (benign/malignant) proliferation of _____________ in _________.
|
benign (no name in disease name); Langerhans cells; bone
|
|
|
Classic presentation of eosinophilic granuloma?
|
Pathologic fractures in adolescent; skin is not involved (benign, so it does not involve skin)
|
|
|
What does a biopsy of a eosinophilic granuloma show?
|
Biopsy shows Langerhans cells with mixed inflammatory cells, including eosinophils.
|
|
|
If you got a patient with pathologic fractures that's an adolescent (tenåring, ungdom), you would start to think about what?
|
(1) Osteosarcoma
(2) Eosinophilic granuloma |
|
|
Classic presentation of Hand-Schüller-Christian disease?
|
Classic presentation is scalp rash (malignant, not benign, so it involves skin), lytic skull defects, diabetes insipidus and exopthalmos. Classically seen in people greater than the age of 3.
|