Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
62 Cards in this Set
- Front
- Back
|
In Vaughan-Williams classification (antidysrhythmic drugs), what is each class ' general mechanism?
A. Class I B. Class II C. Class III D. Class IV |
A. Class I : Na channel blockers (Subclasses IA, IB, IC for moderate, minimal and marked Phase 0 blockage)
B. Class II: beta blockers C. Class III: K channel blockers D. Class IV: Ca channel blockers |
|
|
Quinidine
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. procainamide
|
|
|
Procainamide
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Quinidine
|
|
|
Lidocaine
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Phenytoin
|
|
|
Phenytoin
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Lidocaine
|
|
|
Flecainide
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Ecainide
|
|
|
Encainide
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Flecainide
|
|
|
Propranol
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Metoprolol, Sotalol, Esmolol
|
|
|
Amiodarone
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Sotalol, Ibutilide, Bretylium
|
|
|
Verapamil
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Diltiazem, Nifedipine
|
|
|
Nifedipine
A. what class of antidysrhythmic drug? B. what are other drugs in its group? |

B. Verapamil, Diltiazem
|
|
|
Conduction in damaged/abnormal heart tissue is usually [ decreased / increased]. Antidysrhythmics work [ better /worse ] on Na channels in depolarized cells and decrease recovery.
|
Conduction in damaged/abnormal heart tissue is usually DECREASED. Antidysrhythmics work BETTER on Na channels in depolarized cells and decrease recovery.
|
|

What channels are open, closed or leaky in each phase?
A. phase 0: Fast upstroke B. phase 1: partial repolarization C. phase 2: plateau D. phase 3: repolarization E. phase 4: forward current |

A. phase 0 : Na channels open resulting in fast inward current, accounting for upstroke. Those are rapidly inactivated (upstroke ends).
B. phase 1: Initial rapid phase of repolarization is due to inactivationof sodium channels AND K channels rapidly open and close causing a transient outward current. So, Na channels closed, K+ channels transiently open/close. C. phase 2: plateau. Voltage sensitive Ca++ channels open, resulting in slow inward (depolarizaing) current that balances the slow (polarizing) outward leak of K+. So, Ca channels open; K channels leaky. D. phase 3: repolarization: Ca++ channels close. K+ further open resulting in an outward current leading to membrane repolarization. So, Ca channels close; K open. E. phase 4: forward current. Potassium channel closes. |
|
|
The general strategy for antidysrhythmic drugs is suppression of dysrhythmias by altering three of the following. Which is NOT a strategy by which antidysrhythmics work?
A. alter automaticity B. alter conduction velocity C. alter contractility D. alter refractory period |
C. alter contractility
note: A. alter automaticity: by decreasing slope of Phase 4 depolarizations, increase the threshold potential, or decrease resting potential B. alter conduction velocity: by decrease of phase 0 upstroke, decrease rate of rise of Phase 4 depol, decrease membrane resting potential D. alter refractory period: increase phase 2 plateau, increase phase 3 repolarization, increase action potential duration |
|
|
The general strategy for antidysrhythmic drugs is suppression of dysrhythmias by altering automaticity, conduction velocity or refractory period. Name three specifics with regards to the phases of ion permeability for each strategy.
|
1. alter automaticity by
- decreasing slope of Phase 4 depolarizations - increase the threshold potential - decrease resting potential 2. alter conduction velocity by: - decrease of phase 0 upstroke - decrease rate of rise of Phase 4 depol - decrease membrane resting potential 3. alter refractory period by: - increase phase 2 plateau - increase phase 3 repolarization - increase action potential duration |
|
|
According to the Vaughan-Williams classification for antidysrhythmic drugs, which class/subclass is described? Give at least two examples of drugs from that class.
Moderate block Phase 0. slow conduction, increase APD and increase QT interval. |

Class Ia: Sodium channel blockers.
Ex. Quinidine, Procainamide |
|
|
According to the Vaughan-Williams classification for antidysrhythmic drugs, which class/subclass is described? Give at least two examples of drugs from that class.
Minimal phase 0 block; slow conduction; shorten phase 3 repolarization, decreases APD |

Class IB Na channel blocker.
Ex. Lidocaine, Phenytoin. |
|
|
According to the Vaughan-Williams classification for antidysrhythmic drugs, which class/subclass is described? Give an example of a drug from that class.
Marked Phase 0 block. Slow conduction. No change in APD or repolarization. Increased suppression of Na channels. |

Class IC Na channel blocker.
Ex. Flecainide |
|
|
According to the Vaughan-Williams classification for antidysrhythmic drugs, which class/subclass is described? Give at least two examples of drugs from that class.
decrease adrenergic input. No effect APD, suppress phase 4 depolarization, slow conduction. Can affect phase 0 too to some extent but for our purposes, just focus on this drug class as affecting phase 4. |

Class II , Beta blockers! "-olols" .
Ex. propranolol, metoprolol, sotalol, esmolol |
|
|
According to the Vaughan-Williams classification for antidysrhythmic drugs, which class/subclass is described? Give at least two examples of drugs from that class.
Prolongs repolarization/ refractory period other means than exclusively INa block (mainly K channel blockade), increases QT interval. |

Class III, K channel blockade.
Ex. Amiodarone, Sotalol, Ibutilide, Bretylium. |
|
|
According to the Vaughan-Williams classification for antidysrhythmic drugs, which class/subclass is described? Give at least two examples of drugs from that class.
Slow conduction and increase effective refractory period in normal tisue (AV node) and Calcium dependent slow responses of depolarized tissue (atria, ventricle, Purkinjie). |

Class IV . Calcium channel blockers.
Ex. Verapamil, diltiazem, Nifedipine |
|
|
Which two groups of antidysrhythmic drugs increase the QT interval?
|
Class IA sodium channel blockers like Quinidine and Procainamide; Class III potassium channel blockers like Amiodarone, Sotalol, Ibutilide, Bretylium.
|
|
|
With regards to sodium channel blockers in antidysrhythmic drugs, describe the degree of phase 0 blocking (minimal, moderate, marked) and the effect on APD for Class Ia, Class Ib, Class Ic.
|
Class IA : moderate phase 0 block, increase in APD (due to increase QT interval)
Class IB: minimal phase 0 block, decrease in APD (due to shortened phase 3 repol) Class IC: marked phase 0 block, no affect on APD |
|
|
For the arrhythmia drugs, what are the shortcomings of the Vaughan-Williams system (V-W system)? (3-5)
|
- based on drugs that modify the electrophysiological characteristics of NORMAL CARDIAC TISSUE. (Instead of diseased tissue which is what we actually use em for!)
- the system is incomplete and does not include adenosine, digitalis, cholinergic agonists, alpha adrenergic blockers or agents that modulate gap junctions, ion pumps or exchangers. it also ignores actions of metabolites of the drugs. - some drugs can be put into multiple classes (ex. Amiodarone, can be put in all classes!) - Does not consider drugs that activate channels or recpetors - does not incorporate varying modes of action like slowing tachys, terminating dysrhythmias or preventing them |
|
|
Which of the following statements about key aspects of antidysrhythmic drug action and therapy is FALSE?
A. Antidysrhythmic drug action is state-dependent; drug effects depend on the molecular states of the channel. B. Can be prodysrhythmic under certain circumstances C. Can have significant cardiac and extracadriac toxicity D. Often affect the autonomic nervous system and have hemodynamic effects and effects on cardiovascular reflexes. E. All of the above are true |
E. All of the above are true
|
|
|
Antidyshrythmic drugs affect different parts of the heart.
A. Which is selective for AV and SA nodes? B. Which is useful for treating premature ventricular contractions (PVCs) in the Purkinje fibers? C. Which affects both atrial and ventricular dysrhythmias but is used moreso to treat atrial fibrilation? |
A. selective for AV and SA nodes = Calcium channel blockers (Class IV). B/c calcium action potentials predminate. Thus good for treating AV reentrant tachycardias.
B. for treating premature ventricular contractions (PVCs) in the Purkinje fibers = Lidocaine (Class IB) b/c longer APDs in purkinje yield more inactivated Na channels. Lidocaine selectively blocks inactivated state Na channels. C. affects both atrial and ventricular dysrhythmias but is used moreso to treat atrial fibrilation = quinidine (Class IA) |
|
Of the antiarrhythmic drugs, which two are the only ones to possibly increase automaticity?
A. Amiodarone B. Bretylium C. Digitalis D. Esmolol E. Flecainide |
B. Bretylium, C. Digitalis
all others decrease automaticity |
|
|
Of all the antiarrhythmics, which groups are the ones to NOT have any effect on conduction velocity? What type of effect do all others have on conduction velocity?
|
Groups that DO NOT affect conduction velocity are:
Class IB (Lidocaine, Phenytoin), and Bretylium (a drug in Class III). All other antiarrythmics decrease conduction velocity. |
|
|
Of all the antiarrhythmic drugs, which decrease refractory period?
|
Class IB (Licodaine, Phenytoin), Class II (beta blockers), and digitalis (can both increase or decrease) decrease refractory period. All other antiarrhythmics increase the refractory period.
|
|
|
Of all the anntiarrythmic drugs, which decreases the action potential duration and which does not have any affect on APD?
|
APD are decreased with Class IB, Class IIs, and again digitalis can swing either way. Class IC does not affect APD.
|
|
|
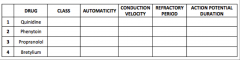
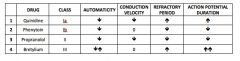
What antiarrhythmic drugs:
A. can increase automaticity? B. have no affect on conduction velocity? C. decrease the refractory period? D. decrease the action potential duration? E. do not have an effect on the action potential duration? |
A. can increase automaticity? BRETYLIUM, DIGITALIS
B. have no affect on conduction velocity? Class IB, Bretylium C. decrease the refractory period? Class IB, Class II, Digitalis D. decrease the action potential duration? Class IB, Class II, Digitalis E. do not have an effect on the action potential duration? Class IC |
|
|
The T1/2 are special for emolol, amidoarone, and adenosine. Match em.
1. 15 seconds 2. 9 minutes 3. 25 days |
1. 15 seconds : Adenosine is ultrashort!!
2. 9 minutes: Esmolol 3. 25 days: Amiodarone prettty long |
|
|
Which antidysrhythmic is the DOC for atrial fibrillation?
|
Class II Beta blockers
Related use regarding dysrhythmias is also for supraventricular tachys. But NOT ventric tachys. |
|
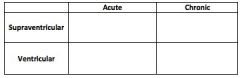
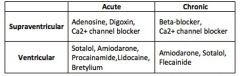
What are the 3 acute-supravent, 2 chronic-supravent, 5 acute-vent, 3 chronic-vent drugs?
|
|
|
|
This antidysrhythmic drug greatly lengthens QT intervals and thus is associated with Torsades de Pointe! Other adverse effects include GI effects like diarrhea and vomiting, CNS effects like HA, nausea, dizziness and tinnitus. A drug intrxn to note is that this displaces digoxin from binding sites. This is useful for chronic dysrhythmias in general requiring outpatient treatment.
A. Esmolol B. Lidocaine C. Flecainide D. Procainamide E. Quinidine |
E. Quinidine
|
|
|
What is the antidysrhythmic drug that can yield drug-induced SLE?
|
Procainamide!
Other noteable thing about procainamide is that it has a metabolite, NAPA, that is a weak sodium channel blocker (Class III activity). Other two drugs are: hydralazine, isoniazid |
|
|
This drug has a metabolite, NAPA, that is a weak sodium channel blocker (Class III activity).
A. Quinidine B. Procainamide C. Lidocaine D. Phenytoin E. FLecainide |
B. Procainamide
|
|
|
This drug has very low toxicity and good therapeutic index. Used IV since there is extensive first pass hepatic metabolism. T1/2 = 0.5-4 hours. Effective in suppressing dysrhythmia associated with depolarized tissue (ischemia; digitalis toxicity). Is also used as a local anesthetic and works on nerves at higher doses.
A. Quinidine B. Procainamide C. Lidocaine D. Phenytoin E. Flecainide |
C. Lidocaine
|
|
|
This drug is a second-line antiarrhythmic. Effective for supraventric AND ventirc tachys as well as digitalis-induced dysrhythmias. Other notables about the drug: Non-sedative anticonvulsant used in treating epilepsy; One of three drugs whose use is associated with gingival hyperplasia.
A. Quinidine B. Procainamide C. Lidocaine D. Phenytoin E. Flecainide |
D. Phenytoin
Gingival hyperplasia can be seen also with other two are cycolosporin and nifedipine. |
|
|
Used primarily for ventricular dysrhythmias but effective for atrial and supraventricular arrhythmias and prevention of atrial fib /flutter. BUT, that said, Associated with signif mortality; marked tendency to exacerbate or precipitate dysrhythmias, thus used as last resort!
A. Quinidine B. Procainamide C. Lidocaine D. Phenytoin E. Flecainide |
E. Flecainide
|
|
|
This is a non-selective beta blocker. Is CI in patients with ventricular failure (can lead to AV block) but others in its same class are sometimes recommended for HF.
|
Propranolol.
|
|
|
This drug prolongs refractory period by blocking potassium channels; is a structural analog of thyroid hormone, contains iodine, very lipophilic.
|
Amiodarone, Class III K channel blocker (also belongs to IA, II, IV) .
Other notable: has very long half life of 13 days -15 weeks! Is a CYP3A4 substrate and inhibitor and thus may enhance the effect of other CYP3A4 substrates like Warfarin, Simvastatin, Verapamil. Also, increases QT interval so risk of TdP. |
|
|
Amiodarone, Class III K channel blocker (also belongs to IA, II, IV) .
This antiaarythmic drug has a very long half life of 13 days -15 weeks! Is a CYP3A4 substrate and inhibitor and thus may enhance the effect of other CYP3A4 substrates like Warfarin, Simvastatin, Verapamil. |
Amiodarone
|
|
|
This drug originally was used as an antiHTN but its availability is now limited. Now is used in emergencies only as it can cause ventricular fibrillation due to QT lengthening.
A. Bretylium B. Ibutilide C. Sotalol D. Verapamil |
A. Bretylium
|
|
|
This is a class III drug that is generally well tolerated and actually has a low incidence of TdP despite being a Class III drug! Most effective current agent to convert atrial fibrillation and flutter of recent onset to normal rhythm.
A. Bretylium B. Ibutilide C. Sotalol D. Verapamil |
B. Ibutilide
|
|
|
This is a drug that is a nonselective beta blocker but also has the characteristic of increasing APD by incresing QT intervals.
A. Ibutilide B. Bretylium C. Sotalol D. Verapamil |
Those characteristics indicate both Class II and Class III characteristics. The only drug that is both of those is Sotalol.
|
|
|
Note that dihydropyridine types of this drug are poor antiarrythmics!!
|
Calcium channel blockers. The calcium blockers used in treating dysrhythmias MUST be non-dihydropiyridines! (Verapamil, Diiltiazem, Nifedipine. Amlodipine IS a DHP.)
|
|
|
This drug for dysrhythmia has side effects of flushing due to vasodilation, hypotension, shortness of breath or burning sensation in chest. It is administered as an IV bolus and has a super short half life of 15 SECONDS!
|
Adenosine
|
|
|
True or False:
Digoxin is used to treat atrial flutter and fibrillation, since slows ventric responses by slowing AV node conduction. |
True
|
|
|
This is used to treat Torsades de Pointe.
A. Adenosine B. Potassium K+ ions C. Digoxin D. Mg |
D. Mg
|
|
|
Which of the following are used for acute supraventricular tachycardias?
A. Adenosine, digoxin, Ca2+ channel blocker B. Beta-blocker, Ca2+ channel blocker C. Sotalol, amiodarone, procainamide, lidocaine, bretylium D. Amiodarone, Sotalol, Flecainide |
A. Adenosine, digoxin, Ca2+ channel blocker
|
|
|
Which of the following are used for chronic supraventricular tachycardias?
A. Adenosine, digoxin, Ca2+ channel blocker B. Beta-blocker, Ca2+ channel blocker C. Sotalol, amiodarone, procainamide, lidocaine, bretylium D. Amiodarone, Sotalol, Flecainide |
B. Beta-blocker, Ca2+ channel blocker
|
|
|
Which of the following groups is use to treat acute, ventricular tachycardias?
A. Adenosine, digoxin, Ca2+ channel blocker B. Beta-blocker, Ca2+ channel blocker C. Sotalol, amiodarone, procainamide, lidocaine, bretylium D. Amiodarone, Sotalol, Flecainide |
C. Sotalol, amiodarone, procainamide, lidocaine, bretylium
|
|
|
Which of the following are used to treat chronic ventricular tachycardias?
A. Adenosine, digoxin, Ca2+ channel blocker B. Beta-blocker, Ca2+ channel blocker C. Sotalol, amiodarone, procainamide, lidocaine, bretylium D. Amiodarone, Sotalol, Flecainide |
D. Amiodarone, Sotalol, Flecainide
|
|
|
What drug has the following adverse effects/ toxicity:
- syncope/ fainting (due to disorganized ventricular tachy) - associated with prolonged QT interval - negative ionotropic action (decreases contractility) - GI: diarrhea, vomiting - CNS: headaches, nausea, dizziness, tinnitus A. Amiodarone B. Bretylium C. Flecainide D. Ibutilide E. Lidocaine F. Phenytoin G. Procainamide H. Quinidine |
H. Quinidine
Note: Procainamide, also a Class IA antidysrhythmic, has similar SE but no GI or CNS effects. |
|
|
What three drugs can yield drug-induced SLE?
|
Procainamide, hydrasalazine, isoniazid
|
|
|
Which three drugs yields drug-induced gingival hyperplasia?
|
Phenytoin, Caclium channel blocker nifedipine, cyclosporin
|
|
|
New drug of choice for ventricular dysryhtymias is
A. Amiodarone B. Bretylium C. Lidocaine D. Phenytoin |
A. Amiodarone
|
|
|
What are important side effects / toxicities of Amiodarone? (Cardiac = 3 ; Non-cardiac = 9)
|
Amiodarone SE and toxicities
Cardiac: prolonged QT interval, sinus bradycardia, negative ionotropic action due to block of Ca channels and beta receptors (but can improve heart vailure via vasodilation) Non-cardiac: - reduces clearance of drugs like procainamide, flexainide, digitalis, quinidine, diltiazem - THYROID DYSFUNCTION (hypo or hyper) since contains iodine - PULMONARY FIBROSIS (most serious adverse effect) - paresthesias - photosensitivity - blurred vision - ataxia, dizziness, tremor - anorexia, nausea |
|
|
Though this class III antidysrhythmic drug increases APD, it has a low incidence of Torsades de Pointe compared to other drugs. Also, this drug is more effective for atrial flutter than fibrillation and is generally well tolerated.
A. Amiodarone B. Bretylium C. Ibutilide D. Sotalol |
C. Ibutilide
|
|
|
True or False:
Dihydropyridine (DHPs) Ca channel blockers (ie. Nifedipine) are poor antiarrythmics. |
TRUE
|
|
|
What drug has the following side effects?
- flushing (due to vasodilation) - hypotension - shortness of breath or burning sensation in chest A. Adenosine B. Amiodarone C. Bretylium D. Phenytoin |
A. Adenosine
Note: Amiodarone has a LOT. Cardiac: prolonged QT interval, sinus bradycardia, negative ionotropic action due to block of Ca channels and beta receptors (but can improve heart vailure via vasodilation) Non-cardiac: - reduces clearance of drugs like procainamide, flexainide, digitalis, quinidine, diltiazem - THYROID DYSFUNCTION (hypo or hyper) since contains iodine - PULMONARY FIBROSIS (most serious adverse effect) - paresthesias - photosensitivity - blurred vision - ataxia, dizziness, tremor - anorexia, nausea |