![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
|
NS development |
**plasticity in children >> can outgrow cerebral palsy
• environmental, e.g. nutrition, hormones, maternal life-style • neuro tube, e.g. neural plate, groove, folds, tube • any disruption during embryonic development >> CNS DO |
|
|
neurodevelopmental history |
• health • behavior • psychosocial • school performance • developmental history |
|
|
T/F. Children >4 y/o should be able to tandem walk. |
False; >5 years old |
|
|
neuro symptom |
• vision, hearing, sensory loss • change in weight • n/v • headache, memory loss • fainting, blackouts • hyperactivity • weakness in one part of the body • clumsiness • changes in bowel/bladder habits • neck pain • gait problems |
|
|
types of neuro exams |
• neurological • neuropsychological • neurodevelopmental |
|
|
landau kleftner |
• normal EEG • neurodevelopmental regression • lost milestones |
|
|
localization |
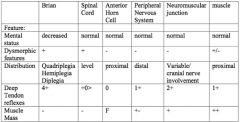
• thinking/memory >> hemispheres, cerebral • coordination >> cerebellum • arms/legs w/ bladder/bowel control >> spinal cord • speech >> L hemisphere
>>if a lot of problems that do not localize to one area >> psychosocial |
|
|
hyperreflexia v. hyporeflexia |
hyperreflexia- CNS hyporeflexia- PNS |
|
|
What is the normal muscle reflex for muscular dystrophy? |
Patients initially have normal reflexes >> hyporeflexive. |
|
|
neuro PE |
** 1/ overall inspection 2/ general cerebral function 3/ cranial nerves 4/ reflexes 5/ motor strength 6/ sensory 7/ proprioception & cerebellar function 8/ soft sign |
|
|
neuro inspection |
• neurocutaneous lesions • muscle atrophy • gait weakness; hands should swing • abnormal positioning, e.g. cortical thumb • handedness in infants; normal in children >2 y/o • large calves compared to thighs >> muscular dystrophy, esp. if child has pelvic girdle weakness • (+) lumbar curve • hand/tongue tremors >> spinal muscular atrophy • hypermobility • foot asymmetry >> diastematomyelia |
|
|
neurocutaneous signs |
• ash leaf spot >> tuberus sclerosis • café au lait >> 6+ may indicate neurofibromatosis • flammeus nevus |
|
|
glaucoma |
• tearing • large pupils |
|
|
sturge webber |
• unilateral flammeus nevus • glaucoma • lesion of CN-V trigeminal |
|
|
marie charcot tooth syndrome |
• thin, long, legs • loss of peripheral nerves >> does not feel cut |
|
|
myopathy v. neuropathy |
• myoppathy- central weakness • neuropathy- distal weakness, e.g. marie charcot syndrome |
|
|
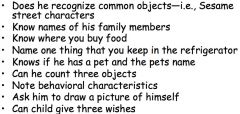
How do you test for cerebral function? |
**neurodevelopmental exam • don't ask something they have to learn, e.g. color • teach child something and evaluate learning ability
• judgement, problem solving; 5-6 y/o • orientation to time/space; school age • memory • affective disturbances • calculation disturbances (+/-) |
|
|
preschool child |
|
|
|
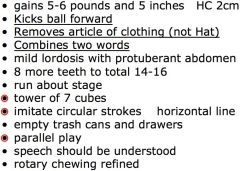
2 years |
|
|
|
3-5 years |
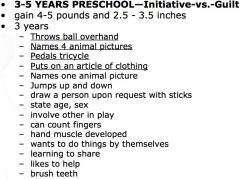
stick figure drawing-- • need all 5 fingers for full credit • 1 point for each parts, e.g. 2 eyes, nose, mouth, head, body |
|
|
4 years |
|
|
|
5 years |
• dresses w/o supervision • copies cross • draws person • puts object on, under, in front of, and behind when asked • hops on one foot 2+ times |
|
|
school age |
**industry v. inferiority **6-12 y/o
• mastering skills needed as adult • winning approval from peers & adults • building self esteem, positive self concept • adopting moral standard |
|
|
1st grade |
|
|
|
ages & shapes |
3- circle 4- cross 5- square 6- triangle |
|
|
tandem walk: black v. white |
African Americans tandem walk by age 4 due to early myelination. Whites tandem walk by age 6. |
|
|
CN-I |
**olfactory
• test after direct blow to forehead above nasal bridge; may be cribiform plate fracture • adults can develop anesomia w/ age; children DO NOT |
|
|
CN-II |
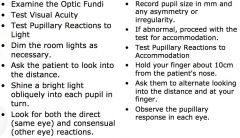
**optic
• test after head trauma • shape of pupil • follow penny w/ eyes |
|
|
horner's syndrome |
• lack of sweat • pupillary defect |
|
|
CN-III, IV, IV |
III- oculomotor IV- trochlear VI- abducens
• inspect eyelids for drooping • pupils' size for equality and reaction to light & accomodation • 6 cardinal gaze |
|
|
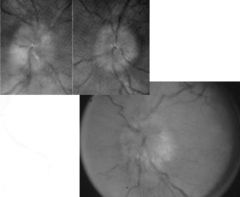
blurred border |
|
|
|
papilledema |

|
|
|
paralysis of CN-III |
• horizontal nystagmus a/w labyrinthine, cerebellar, or brainstem pathology • vertical nystagmus a/w cerebellar or brainstem pathology • medication toxicity can cause both |
|
|
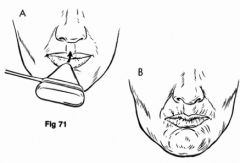
CN-V |
"make monster face for me"
• inspect face for muscle atrophy & tremors • palpate jaw muscles as jaws clenched • test for touch and temperature sensation |
|
|
CN-VII |
• facial symmetry • smile & frown • close eye tight • puff cheeks |
|
|
central v. peripheral CN-VII |
central-- • can elevate eyebrows • can close both eyes
peripheral-- • cannot elevate eyebrow on R • bell's phenomenon- R eye cannot close & eyeball turns up |
|
|
CN-VIII |
• turning fork can be difficult to use in younger child • screen for hearing 500 to 6000/8000 |
|
|
weber test |
• place vibrating tuning fork on middle of forehead >> heard on both sides? • unilateral neurosensory hearing loss >> best in normal ear • unilateral conductive loss >> best in abnormal ear |
|
|
rinne test |
**comparing bone conduction to air conduction AC > BC is normal |
|
|
conductive v. sensorineural hearing loss |
conductive-- • eustachian tube dysfunction • ear fluid • hole in eardrum • fixed middle ear bone
sensorineural-- • noise induced • prebycusis • meniere's disease • tumors |
|
|
CN-IX |
**glossopharyngeal • ability to swallow • gag reflex; not routinely done in school setting • sweet/sour taste |
|
|
CN-X |
**vagus • vocal quality • look for rise of soft palate as child says "HAHA" |
|
|
testing CN-IX and X |

|
|
|
CN-XI |
**accessory • head rotation against resistance to test sternocleidomastoid • upward shoulder movement tests trapezius |
|
|
CN-XII |
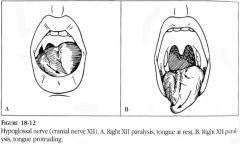
**hypoglossal • inspect tongue; look for symmetry, tremors, & atrophy • pressure the tongue against cheeck & check strength • quality of lingual sounds; l,t,d,n • potruded tongue deviates toward affected weaker side >> unilateral lesion |
|
|
reflexes |
• patient should be relaxed • don't use more force than necessary • can be reinforced by having patient perform isometric contractions • evaluate for equality & spread |
|
|
reflex grading scale |
0 absent 1+ hypoactive 2+ normal 3+ hyperactive w/o clonus 4+ hyperactive w/ clonus
newborns may have clonus up to 3-4 weeks s/p birth |
|
|
clonus |
>> support knee in partly flexed position >> when patient relaxes, quickly dorsiflex foot >> observe for rhythmic oscillations |
|
|
bicep & tricep reflex |
bicep-- • C5, C6 • partially flexed @ elbow w/ palm down • should feel response even if not visible
tricep-- • C6, C7 • support upper arm & let forearm hang free • if patient is sitting/lying down >> flex arm at elbow and hold close to chest |
|
|
brachioradialis reflex |
• C5, C6 • rest forearm on abdomen or lab • strike radius ~1-2 inches above wrist • watch for flexion/supination of forearm |
|
|
abdominal reflex |
• above umbilicus- T8, T9, T10 • below umbilicus- T10, T11, T12 • stroke abdomen lightly w/ blunt object on each side in an inward & downward direction • note contraction & deviation of umbilicus towards stimulus |
|
|
knee reflex |
• L2, L3, L4 • note contraction of quadraceps & knee extension |
|
|
ankle reflex |
• S1, S2 • have patient lean on chair w/ one knee • dorsiflex foot of ankle >> strike achilles • watch & feel for plantar flexion |
|
|
babinski reflex |
**fanning/outward motion is normal in children who cannot walk |
|
|
chaddock v. oppenheimer reflex |
chaddock-- • stroke side of foot from external malleolus to small toe • (+) if dorsiflexion of great toe
oppenheimer-- • firmly press down on shin & run along anterior medial tibia toward foot • (+) if dorsiflexion of great toe |
|
|
snouting reflex |
|
|
|
motor strength |
**test according to developmental milestone • infant- tone, hip control • toddler- walk is broad based • older child- fine v. gross motor
includes-- • posture, gait • balance • coordination • writing |
|
|
intention tremor |
• child tremors before block placement • sign of cerebellar disease
causes of tremor-- • familial • hyperthyroidism |
|
|
gowers sign |
**uses push up to get off the floor |
|
|
grading motor strength |
0/5 no muscle movement 1/5 no movement @ joint 2/5 not against gravity 3/5 not against resistance 4/5 less than normal 5/5 normal strength |
|
|
myotonic v. neuropathy |
myotonic disease-- • spinal muscular atrophy • musuclar dystrophy • myotonic dystrophy; worse w/ every generation
neuropathic disease-- • marie charcot tooth |
|
|
myotonia |
sustained contractions |
|
|
duchenne muscular dystrophy |
boys-- • difficulty climbing stairs • running, frequent falls • jumping from standing position
slow motor milestones-- • starts walking @ 18 mos • clumsy @ 2-3 yrs • difficulty keeping up with peers @ 3-5 yrs
consistent weakness-- • proximal muscles >> distal muscles • legs >> arms • extensors >> flexors |
|
|
duchenne muscular dystrophy progression |

• toe walking • calf pseudohypertrophy • (+) gowers • lumbar lordosis from muscle weakness • multifocal contractures • trendelenburg gait • fatigue |
|
|
pronator drift |
**upper motor neuron disease **unable to maintain supination |
|
|
sensory |
**perform all 4 extremities
• pain • light touch • vibratory sense • hot/cold • sharp/dull |
|
|
proprioceptive & cerebellar function |
**stand for 40s; if unable to perform >> cerebellar weakness
• intentional tremor during block stacking • tandem gait • balance • gait--wide based & ataxic |
|
|
coordination & gait |
• rapid alternating movements • point-to-point movements • romberg • gait |
|
|
two point discrimination |
• done on older children • used opened paper clip to touch patient's finger pads in two places simultaneously |
|
|
graphesthesia. v. stereognosis |
graphesthesia-- • draw large number on patient's palm • ask to identify
stereognosis-- • older child, use as alternative • place familiar object in patient's hand • ask to identify |
|
|
soft sign |
• nonstop talking, constant motion • L to R confusion; identify by age 8 • hand preference; established by age 3 • dystonic posturing • proximal inhibition |
|
|
T/F. Left hand preference or mixed hand preference are neurodevelopmental markers. |
True |
|
|
dystonic posturing |
stiffening of extremities during stressed gait or rhythmic movements, e.g. hop in place/toe walk w/ penny on nose |
|
|
proximal inhibition |
• inability to inhibit proximal musculature while using distal muscles • screen by instructing child to rapidly alternate opening & closing of fists w/ arms extended or by rapidly roatating wrist while holding arms and hands above the head |
|
|
neuropsych eval |
• used for learning disabilities • parent's observations • formal observation, e.g. watch child copy designs, pronounce words, etc. |
|
|
skull fractures |
simple aka linear-- • most common
depressed-- • hematoma @ site • may need surgery
compound-- • laceration & depressed skull fracture • dura usually pierced • skull fragments may be displaced into brain tissue
basilar-- • break in posteroinferior portion • produces dural tears resulting in leakage of CSF >> (+) dextrose stick |
|
|
epidural hematoma |
**blood b/w dural surface and skull; usually result of tearing of meningeal artery • more common in older children & toddlers; miningeal artery is not yet embedded in bony surface of skull prior to age 2 • slow growing
s&s-- • headache • (-) LOC • fever • dilation of pupil on affected side |
|
|
basilar skull fracture |
early signs-- • blood behind typmanic membrane • nerve palsy • deafness, ringing in ear • dizziness, n/v
late signs-- • battle sign- bruising over temporal area • racoon sign |
|
|
quick neuro check |
• LOC • motor function • pupillary response • VS • ICP • glasgow coma scale |
|
|
glasgow coma |
• eye opening response 1-4 • motor response 1-6 • verbal response 1-5 |
|
|
bacterial meningitis |
**child's age is predominant determinant of common bacteria cause • headache, fever • stiff neck • toxic
if child is <2 y/o-- • NO stiff neck • (-) LOC • otitis media • focal seizures |
|
|
meningitis history |
• progression • exposure • history of otitis media • underlying health problems • seizures--focal v. generalized |
|
|
menigitis signs |
kernig's sign-- • complains of lower back pain • flex hip and knee >> straightening knee will cause excessive pain & resistance • complains of lower back pain
brudzinki sign-- • tests for nuchal rigidity • flexion of neck causes flexion of hips and knees |
|
|
T/F. Patients with VP shungs have classic signs of menigitis. |
False; they present differently-- • low grade ventriculitis • headaches • nausea • minimal fever • malaise |
|
|
viral meningitis |
• less toxic • more common in summer • treated @ home unless patient is vomiting and needs fluids |