Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
295 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Who were the pioneers of PNF? ***
|
1940’s-50’s
- Dr. Herman Kabat - physiatrist - Margaret Knott, PT – pioneer of PNF - Dorothy Voss, PT – pioneer of PNF |
|
|
|
What are the roots of PNF? ***
|
- theory based on motor development and neurophysiology
- most work done on neuro patients - adult with neuro injury likened to baby in development; based adult rehab on early human development |
|
|
|
What is PNF? ***
|
- Proprioceptive Neuromuscular Facilitation
- a treatment approach that uses methods of promoting or hastening the response of the neuromuscular mechanism through stimulation of the proprioceptors |
|
|
|
Proprioceptive ***
|
receiving stimulation from within tissues of the body (GTO and muscle spindle) – receptor in body that gives CNS info about muscle tension spatial awareness
|
|
|
|
Neuromuscular ***
|
pertaining to nerves and muscles
|
|
|
|
Facilitation ***
|
promoting or hastening a natural process
|
|
|
|
PNF treatment approach ***
|
- PNF has its own philosophy and techniques
- based on anatomy and normal motor development - includes mass movement and functional activities - “The brain knows nothing of individual muscle action, but knows only of movement.” |
|
|
|
Stages of motor control ***
|
- random mobility
- stability - controlled mobility - skill |
|
|
|
What is random mobility? ***
|
- movement in the first few months of life
- largely reflexive |
|
|
|
How does a human move from random mobility to stability? ***
|
- gains abilities such as head control and sitting balance
- begins centrally with the head, neck and trunk |
|
|
|
What is controlled mobility? ***
|
- imposing movement on stability
- movement of COG within or outside of BOS |
|
|
|
What is skill? ***
|
- manipulation and exploration of environment
- lifelong (learning to walk, then run, etc.) |
|
|
|
Sequence of development ***
|
- cephalo-caudal
- proximo-distal - strength - stability, control, motor function, and sensation (e.g., baby learns head control before sitting, gains strength in shoulder before wrist) |
|
|
|
What is the philosophy behind PNF? ***
|
- all humans respond in accordance with demand (we do what we have to do)
- whatever demands we place on the body, it tends to meet - our bodies are geared to do what we demand of them - existing potentials may be developed more fully; we all have certain potentials that can be developed - potential is there and we can develop it (everyone to their own degree) - movements must be specific and directed toward a goal - activity is necessary for the best development of coordination, strength, and endurance - stronger body parts strengthen weaker parts through cooperation and lead toward a goal of optimum function |
|
|
|
PNF movements are based on ***
|
- mass movement patterns
- that are spiral (rotatory) and diagonal (abduction and adduction) - these patterns are functional in nature - diagonals consist of synergistic muscle groups |
|
|
|
A PNF pattern has what three components? ***
|
- flexion or extension
- toward or away from midline (abduction or adduction) - rotation (internal or external) |
|
|
|
Describe the basics of PNF patterns. ***
|
- two diagonals for the (head & neck), trunk, and extremities
- diagonal crosses through the proximal joint - 2 antagonistic patterns for each diagonal - groove is 45 degrees off the perpendicular |
|
|
|
Describe the pattern for scapular and pelvic PNF. ***
|

- anterior elevation (1--D1F) to
- posterior depression (7--D1E) - posterior elevation (11--D2F) to - anterior depression (5--D2E) |
|
|
|
What are the 8 PNF extremity patterns? ***
|
- D1F, UE
- D1E, UE - D2F, UE - D2E, UE - D1F, LE - D1E, LE - D2F, LE - D2E, LE |
|
|
|
List and describe the scapular PNF patterns. ***
|
- anterior elevation - acromion to nose
- posterior depression - acromion to ipsilateral ischial tuberosity (back pocket) - posterior elevation - acromion to behind ear - anterior depression - acromion to umbilicus |
|
|
|
What type of contact should be given when conducting PNF? ***
|
- firm, not painful
- facilitate agonist - touch - usually, one proximal and one distal |
|
|
|
What type of resistance should be given when conducting PNF? ***
|
Maximal Resistance
- give resistance that allows normal, functional movements - greatest amount that still allows smooth movement Optimal Resistance - resistance graded appropriately for intention |
|
|
|
How is a quick stretch used in PNF? ***
|
when followed by resistance it facilitates muscle contraction
(activates the muscle spindle) |
|
|
|
How is traction used in PNF? ***
|
it facilitates isotonic movement of phasic muscle groups
|
|
|
|
How is approximation used in PNF? ***
|
stimulates co-contraction, stabilization, extension and tonic muscle response
|
|
|
|
What is important to be mindful of with regards to verbal commands during PNF? ***
|
- tone
- volume (I would also say succinct and diminishing as the patient gets into the rhythm) |
|
|
|
What is important about visual cues during PNF? ***
|
they enhance movement and control
|
|
|
|
What is successive induction? ***
|
- when muscle contracts and reaches shortened range, the antagonist is prepared to contract
- suggests that voluntary motion of one muscle can be facilitated by the action of another (e.g., biceps contraction, followed by triceps contraction, results in increased response of biceps) |
|
|
|
What is cross-transfer? ***
|
maximal contraction on one side heightens excitability of muscle on other side
|
|
|
|
What is normal timing? ***
|
- distal to proximal
- promotes coordination |
|
|
|
What is important to remember about therapist's body position during PNF? ***
|
- align along diagonal planes
- use body weight for resistance - watch your own posture |
|
|
|
What is rhythmic initiation? ***
|
- "getting in the groove"
- used to begin patterns of movement - usually starts with passive motion (the therapist doing all the movement/positioning) - effective technique for assisting initiation of motion - facilitates learning to appropriately contract muscle(s) again |
|
|
|
What is another term for irradiation? ***
|
overflow
|
|
|
|
What is a slow reversal hold? ***
|
use of gradually applied isometric contraction introduced at a point in range
|
|
|
|
What is contract-relax (autogenic inhibition)? ***
|
combination of isotonic (rotatory component) and isometric (other two) contractions
|
|
|
|
What is hold-relax (autogenic inhibition)? ***
|
isometric contraction all components
|
|
|
|
What is reciprocal inhibition (agonist contraction)? ***
|
contraction of muscle causing gain in ROM will also cause relaxation of antagonist
|
|
|
|
What is timing for emphasis? ***
|
- blocking normal timing of muscle contractions to focus on recruitment, strength or coordination of a specific muscle or group, often in a particular portion of the ROM
- to affect specific points in a range (e.g., pattern initiated, at strongest point pt does isometric hold; therapist applies quick stretch to one portion while isometric hold is maintained everywhere else; repeat the quick stretch 2-3 times, then apply quick stretch to entire pattern to facilitate movement trough entire pattern) |
|
|
|
What is resisted progression? ***
|
- stretch, approximation and tracking resistance applied manually to facilitate pelvic motion and progression during locomotion
- level of resistance is light so as to not disrupt the patient's momentum, coordination and velocity - can also be applied using elastic band resistance |
|
|
|
How is "physical fitness" defined? ***
|
ability to perform physical work that requires:
- cardiorespiratory endurance - muscular endurance - muscular strength - flexibility |
|
|
|
What are the benefits of being physically fit? ***
|
being fit allows:
- daily activities without undue fatigue - ability to respond effectively to emergency |
|
|
|
What terms are used for physical fitness? ***
|
- cardiovascular endurance
- aerobic endurance - cardiorespiratory fitness - aerobic fitness |
|
|
|
What is cardiorespiratory endurance training? ***
|
- ability of whole body to sustain prolonged repetitive movements of large muscle groups
- requires circulatory and respiratory systems - whole body endurance |
|
|
|
How much moderate-intensity physical activity should all adults do? ***
|
- all adults should accumulate at least 30 min of moderate intensity physical activity on most, preferably all, days of the week.
per the: - US Department of Health and Human Services - Center for Disease Control and Prevention - American College of Sports Medicine - National Council on Physical Fitness & Sports |
|
|
|
How is the "talk test" used to determine activity level/energy expenditure? ****
|
- light - can sing
- medium - can converse with some effort - vigorous - cannot talk |
|
|
|
What HR range is used for moderate intensity? Vigorous intensity? ***
|
- 50% - 70% of max HR
- 70% - 85% of max HR |
|
|
|
How is energy expenditure quantified? ***
|
MET - metabolic equivalent
the amount of oxygen consumed (mL) per kilogram of body weight per minute (mL/kg/min) |
|
|
|
What are some MET levels for activity (based on 143-lb male)? ***
|
1 MET- seated at rest
2 MET- strolling 1 mph 5 MET- walking 3 1/2 mph 8 MET- 5 mph 15 MET- 9 mph 17 MET- 10 mph |
|
|
|
What MET levels are considered "moderate intensity"? Vigorous? ***
|
- 3-6 MET is considered moderate (thus what we should strive for most, if not all, days of the week for 30 minutes
- over 6 MET is considered vigorous |
|
|
|
What is VO2 max? ***
|
- maximum oxygen consumption
- volume of oxygen consumed by body per minute, usually during maximum exertion of activity - more fit = higher VO2 max |
|
|
|
What are our fuel sources for energy? ***
|
- carbohydrates (body's preferred source)
- fat - protein - all of these must be broken down to ATP, which can be used at the cellular level. |
|
|
|
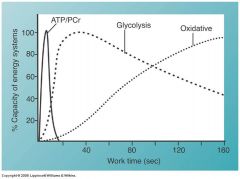
What are the three metabolic (energy) pathways? ***
|
- ATP-Phosphocreatine (ATP-PC) system
- glycolytic system - oxidative system |
|
|
|
How do the three metabolic pathways work? ***
|
|
|
|
|
Another name for ATP-PC ***
|
Phosphagen
|
|
|
|
How does the ATP-PC system produce energy? ***
|
- phosphocreatine is fuel source
- phosphocreatine (PCr) – compound in muscles that splits, giving phosphate molecule to ADP to create ATP - 1 molecule PCr >> 1 molecule ATP - replenishes ATP in working muscle - no O2 required in chemical reaction, but the pathway can occur in the presence of O2 - short, quick bursts of energy (15 sec max.) |
|
|
|
What is the fuel source for the ATP-PC system? ***
|
phospocreatine (PCr)
|
|
|
|
Is oxygen required in the ATP-PC system? ***
|
no
|
|
|
|
How long-lasting is the energy produced by the ATP-PC system? ***
|
15 seconds maximum
|
|
|
|
How does the glycolytic system work? ***
|
- glucose (from carbohydrates in food) and glycogen (stored in liver) are fuel source
- anaerobic - 1 molecule glucose >> 2 molecules ATP - 1 molecule glycogen >> 3 molecules ATP - lactic acid is by-product - energy for moderate intensity, short duration activity (1-2 min) |
|
|
|
What are the fuel sources for the glycolytic system? ***
|
- glucose
- glycogen (from liver) |
|
|
|
In the glycolytic energy system, how many molecules of ATP does 1 molecule of glucose produce? 1 molecule of glycogen? ***
|
- 2 molecules of ATP
- 3 molecules of ATP |
|
|
|
What is the byproduct of glycolytic energy production? ***
|
lactic acid (which produces "the burn")
|
|
|
|
For what is the energy produced by the glycolytic system most suitable (intensity and duration of activity)? ***
|
moderate intensity, short duration activity (1-2 min)
|
|
|
|
How does the oxidative energy system work? ***
|
- glycogen, fat, protein (min) are fuel sources
- aerobic - involves Kreb’s cycle, electron transport chain - 1 molecule glucose >> 38 molecules ATP - low intensity exercise for prolonged time |
|
|
|
Which form of energy production requires oxygen (is aerobic)? ***
|
oxidative energy production
|
|
|
|
What are the energy sources for oxidative energy production? ***
|
- glycogen
- fat - protein (minimal) |
|
|
|
How many molecules of ATP does 1 molecule of glucose produce in the oxidative system? ***
|
38 molecules of ATP
|
|
|
|
For what is the energy produced by the oxidative system most suitable (intensity and duration of activity)? ***
|
low-intensity exercise over long periods of time
|
|
|
|
Characteristics of slow-twitch (type I -- SO) muscle fibers ***
|
- slow contractile response
- high oxidative capacity - recruited for endurance activities - low-intensity |
|
|
|
Characteristics of fast-twitch (type IIB -- FG) muscle fibers ***
|
- fast contractile response
- recruited for power - glycolytic |
|
|
|
Characteristics of slow-twitch (type IIA -- FOG) muscle fibers ***
|
- has some characteristics of both I and II
- both aerobic & anaerobic activity |
|
|
|
What is the body's normal response to acute aerobic exercise? ***
|
- heart rate increases
- stroke volume increases - cardiac output increases (HR X SV = CO) - arterial-venous oxygen difference increases - blood flow to heart, skeletal muscles, skin increases, but no change to brain - systolic BP increases - diastolic BP doesn't change, or slightly decreases - respiratory rate and tidal volume increase |
|
|
|
Product of heart rate and stroke volume = ***
|
cardiac output
|
|
|
|
Abnormal responses to aerobic exercise ***
|
- no rise in HR with increased intensity
- no increase in SBP with increase in activity - decrease in SBP of 20 mmHg - increase or decrease in DBP of 15 mmHg - pain in chest, arm, jaw, neck - labored respirations, SOB - abnormal diaphoresis - signs of fatigue, confusion, pain or distress - complaints of nausea & dizziness - problems with coordination & equilibrium - facial pallor - leg cramps |
|
|
|
What chronic changes occur with aerobic conditioning? ***
|
- heart increases in weight and volume
- left ventricle size/thickness increases - stroke volume increases - plasma blood volume increases (primarily due to hormone release--ADH and aldosterone--promoting fluid retention, and increase in plasma proteins--albumin) - greater capillarization in trained muscles and more efficient blood flow to active muscles - size & number of mitochondria increase - myoglobin content increases - improved use of fat & carbs - hypertrophy of Type I muscle fibers |
|
|
|
What adaptive changes occur with aerobic conditioning? ***
|
- weight and volume of heart increase
- thickness and chamber size of left ventricle increase - HR returns to normal after exercise more quickly (good indicator of progress) - resting HR decreases - resting SV increases - resting CO does not change* - resting respiration rate decreases - resting ventilation does not change - resting lung volume does not change - resting systolic/diastolic BP decreases (in hypertensive persons) - resting VO2 max does not change * because the HR decrease and SV increase offset ---------------------------------------------------------------------------------------------------------------- - maximum HR does not change - maximum SV increases - maximum CO increases - maximum respiration rate increases - maximum ventilation increases - maximum lung volume increases - maximum systolic/diastolic BP do not change - maximum VO2 max increases |
|
|
|
What are the benefits of aerobic conditioning/training? ***
|
- depression & anxiety reduced
- fatigue reduced - prevention of chronic diseases - mood & well-being improved - performance at work improved - blood lipid profile improved - immune function improved |
|
|
|
What are some clinical guidelines for aerobic conditioning? ***
|
- screening (ACSM recommendations and PAR-Q & You on pg 264)
- supervision (none required if healthy, needed if 2 or more risk factors) |
|
|
|
What is the ACSM's definition of low risk? ***
|
men <45 yo and women <55 yo with no more than one coronary disease risk factor and without sx or known coronary disease
|
|
|
|
What is the ACSM's definition of moderate risk? ***
|
men 45 or > and women 55 or > or with two or more coronary disease risk factors
(these persons should see a physician before beginning an exercise program) |
|
|
|
What is the ACSM's definition of high risk? ***
|
one or more sx of cardiopulmonary disease; or with CV, pulmonary or metabolic disease
(these persons should see a physician before beginning an exercise program) |
|
|
|
What parameters are included in an exercise prescription? ***
|
- intensity
- duration - frequency - mode - progression |
|
|
|
What is exercise intensity? ***
|
- age-adjusted target HR (THR)
HR max = (220-age) HR max X (60%-90%) = THR |
|
|
|
What is the Karvonen formula for determining target HR? ***
|
(HR max - HR resting) X (50% - 85%) + HR resting
|
|
|
|
Describe the Borg's Scale? ***
|
- rate of perceived exertion
7 - very, very light 9 - very light 11- fairly light 13 - somewhat hard 15 - hard 17 - very hard 19 - very, very hard - training range is 12-16 |
|
|
|
What is the optimum training range on the Borg's Scale? ***
|
12-16
somewhere between fairly light (11) and very hard (17) |
|
|
|
What is the normally prescribed duration and frequency of exercise for aerobic conditioning? ***
|
20-60 minutes per session
(several 12-minute bouts can be prescribed if they cannot do 20 mins) 3-5 times per week |
|
|
|
What modes of exercise are normally prescribed for aerobic conditioning? ***
|
rhythmic activities w/ large muscle groups
- walking - running - hiking - cycling - rowing - swimming |
|
|
|
What are the levels of progression for aerobic conditioning? ***
|
- initial stage
- improvement stage - maintenance stage |
|
|
|
What are the parameters for the initial stage of aerobic conditioning? ***
|
- 1 – 6 wks
- RPE 11 – 12 - 40% – 60% intensity - 15 – 30 min - 3 – 4 X per wk (intensity, duration, frequency) (mode and progression not defined, except as to improvement stage) |
|
|
|
What are the parameters for the improvement stage of aerobic conditioning? ***
|
- 4 – 8 months
- 50% – 85% intensity - 30 – 40 min (increased up to 20% per week) - 5 – 6 X per week (ensure pt can complete 2 weeks w/o signs of musculoskeletal overuse or excessive fatigue) (intensity, duration, frequency) (mode and progression not defined, except as faster than in initiation stage; to maintenance stage) |
|
|
|
What are the parameters for the maintenance stage of aerobic conditioning? ***
|
- lifelong compliance
- maintain aerobic fitness above 50% - 20 – 60 minutes - 3 – 5 X per week |
|
|
|
How does aging affect aerobic conditioning? ***
|
- aerobic capacity declines with aging
- maximal HR declines with age - in older adults, improvement can occur with training at 50% HR reserve |
|
|
|
How does youth affect aerobic conditioning? ***
|
- children are less mechanically efficient than adults
- children lose more energy than adults when performing the same activity - children have a poorer ability to dissipate heat than adults when exercising in hot environments; they also generate more metabolic heat per unit body size, have lower sweating rates and slower onset of sweating related to rise in core temperature |
|
|
|
What are some contraindications for aerobic conditioning? ***
|
- severe CAD
- uncontrolled arrhythmias - uncontrolled hypertension - recent pulmonary embolism or DVT |
|
|
|
The Achilles tendon is common to what two muscles? ***
|
- gastrocnemius
- soleus |
|
|
|
What activities can cause Achilles tendinitis? ***
|
- athletic activities such as running
- especially jumping - can occur in anyone with tissue overuse |
|
|
|
Etiology of Achilles tendinitis ***
|
- gradual onset usually
- can progress to moderate pain during activity, then to severe pain preventing activity - can result from partial tear or rupture - hypovascularity 3-5 cm proximal to insertion is believed to be the cause |
|
|
|
What increases the need for surgery for Achilles tendinitis? ***
|
sedentary lifestyle
|
|
|
|
Signs and symptoms of Achilles tendinitis ***
|
- dull aching pain in area of tendon, usually proximal to insertion into calcaneus
- pain may be present at rest, most often with activity - pain on palpation & with weight bearing - crepitus may be felt on repeated plantar flexion & dorsiflexion - possible edema & thickening of Achilles tendon - weakness & diminished push off strength - chronic |
|
|
|
How is Achilles tendinitis typically managed? ***
|
- initially - control symptoms, edema, & inflammation using P.R.I.C.E.
- prescribed medication for pain & inflammation - acute inflammation – running should be stopped - transverse friction massage - soft tissue mobilization of muscle-tendon junction - ultrasound & e. stim - stretching exercises – leaning forward for 30 sec. - heel lift can decrease stress by shortening tendon during weight bearing - foot orthotics if body mechanics contribute to the onset or recurrence - walking boot may be necessary – worn for six weeks - operation – if inflamed longer than six months - after rest – swimming, bicycling, water jogging |
|
|
|
What is IT band syndrome? ***
|
IT band (and bursa between lateral femoral condyle and IT band) becomes irritated and inflamed and no longer glides across femur as easily as it should
|
|
|
|
What is the IT band and where does it attach? ***
|
- a thick, matted band of connective tissue that runs along the outside of the thigh from the iliac crest to the lateral tubercle of the tibia
- gluteal muscles and TFL attach to the top - lower part attaches just below the knee at Gerdy’s tubercle |
|
|
|
What is the function of the IT band? ***
|
The function of the IT band is to
- stabilize the hip and knee - flex the hip - internally rotate the hip - abduct the hip |
|
|
|
Who is most at risk of IT band syndrome? ***
|
especially:
- runners (esp those who increase their mileage, run downhill, run on banked surfaces, or on tracks in only one direction) - cyclists also: - MMA athletes - weightlifters (squats and deadlifts) - racquet sports players - military personnel - aerobic exercisers |
|
|
|
Etiology of IT band syndrome ***
|
- repetitive knee flexion and extension causing excessive friction between IT band and underlying lateral femoral condyle; associated movement brings pain at lateral knee
- overtraining - high weekly mileage, interval training, track training - biomechanical problems (different leg lengths, bowlegs, overpronation) - weak hip abductors (gluteus medius). - pre-existing IT band tightness - makes up 12% of running overuse injuries |
|
|
|
Signs and symptoms of IT band syndrome? ***
|
- most common symptom is progressive lateral knee pain that starts diffuse, then progresses to sharp and localized
- pain begins during/after a run/ride, going up/down stairs, getting out of car, after sitting for long periods of time w/knee flexed - referred hip pain - tenderness of IT band overlying lateral femoral condyle and possible swelling - sometimes accompanied by clicking sensation as IT band snaps across knee joint during running |
|
|
|
Testing for IT band syndrome ***
|
- physical exam
- cortisone injection may prove diagnostic if it relieves symptoms - MRI to confirm thickness and/or fluid at lateral femoral condyle - Noble Compression Test (from picture looks like squeezing IT band at lateral femoral condyle) |
|
|
|
Treatment of IT band syndrome -- acute ***
|
alleviate inflammation
- rest, ice NSAIDs - education (decrease knee flexion, extension) - activity modification (swimming or pool running vs. running on track) - ultrasound - iontophoresis - cortisone injection |
|
|
|
Treatment of IT band syndrome -- sub-acute ***
|
begin stretching IT band
- ST mobilization, including friction massage, full length of band (daily to 2-3 X per week) post stretching without pain, initiate strengthening and stabilization program - address specific muscle weaknesses, particularly hip abductors (gluteus medius) - side-lying leg lifts, knee stabilizers, clams to strengthen gluteus medius |
|
|
|
HEP and return to regular exercise for IT band ***
|
- continue IT Band stretches, also calf, hamstring, quad, glute
- continue strength training: side leg lifts w/ therabands, clams, knee stabilizers - gradually progress back to “normal” routine - run on level surfaces, not on crowned surfaces or on tracks in only one direction - increase milage slowly - wear appropriate shoes, use orthotics to decrease lateral knee stresses - patient compliance is key to recovery!!! - expected recovery 3-6 weeks for severe cases |
|
|
|
Last-resort treatment for IT band syndrome ***
|
- surgery to remove bursa and "release" the IT band to reduce friction
- usually good outcome, but may result in a "floppy" knee |
|
|
|
What is piriformis syndrome? ***
|
painful musculoskeletal condition in which sciatic pain manifests in the buttock and radiates down the thigh, even as distal as the foot
|
|
|
|
Another name for piriformis syndrome ***
|
Also known as:
- “Hip Pocket Neuropathy” or - “Wallet Neuritis” |
|
|
|
Theories explaining symptoms of piriformis syndrome ***
|
The Sciatic Nerve is Compressed:
- (1) Between the inflamed Piriformis muscle & bony pelvis - (2) Between two inflamed fascicles of the Piriformis muscle |
|
|
|
What condition is responsible for 5-6% of low back pain? ***
|
piriformis syndrome
|
|
|
|
In what ways can the piriformis irritate the sciatic nerve? ***
|
- can be irritated by overlying piriformis muscle
- can be trapped under the muscle and against the ischium - can be entrapped within the muscle belly itself |
|
|
|
Piriformis syndrome is usually determined by excluding what other conditions? ***
|
- lumbar disease
- nerve root impingement - herniated nucleus pulposus - tumors or abscesses - possible gluteal atrophy |
|
|
|
How is piriformis syndrome confirmed? ***
|
- piriformis sign
- FADIR (or FAIR) Test + Lasegue’s Sign + Freiberg’s Sign + Pace’s Sign - Beatty’s Maneuver - CT scans & Myeography tests used but not totally reliable |
|
|
|
Etiology of piriformis syndrome ***
|
anatomic abnormalities of sciatic nerve and piriformis muscle
- sometimes the sciatic nerve portions (tibial and peroneal) are not enclosed and one can pierce the muscle - sometimes the muscle is split & one or both parts of sciatic nerve pass through the muscle belly |
|
|
|
Types of piriformis syndrome ***
|
- primary
- secondary |
|
|
|
Characteristics of primary piriformis syndrome ***
|
- intrinsic pathology of piriformis itself
- hypertrophy of piriformis muscle - anatomical variations (sciatic nerve passes through piriformis) - myofascial pain - spastic, inflamed or myofascial syndrome - myositis ossificans - trauma (50% of cases) - one leg of shorter length (rare occurrence) |
|
|
|
Characteristics of secondary piriformis syndrome ***
|
- herniated disc
- facet syndrome - S-I joint dysfunction - trochanteric bursitis - flexion contracture at the hip - ischial bursitis - other conditions impinging sciatic nerve - endometriosis - pseudoaneurysm of inferior gluteal artery |
|
|
|
Signs and symptoms of piriformis syndrome ***
|
- gluteal pain radiating down affected leg
- pain with walking, limping & squatting - acute pain with stooping & lifting - intolerance to long periods of sitting - low back pain (sometimes) - palpable sausage-shaped mass, tender to palpation over the piriformis muscle - possible “falling asleep” of legs & feet during prolonged sitting, but resolves after rising & moving around - usually there is gradual onset of S & S - generally affected unilaterally - can occur several months post trauma |
|
|
|
Management of piriformis syndrome? ***
|
- correction of biomechanical abnormalities
- lifestyle modifications to avoid irritable activities - massage to tender area of piriformis - specific stretches of piriformis and hip abductors (supine and standing) - NSAIDs - US and e. stim - "spray and stretch" techniques - injections (trigger point; caudal epidural steroid; Botox: type A and B, which appear to last longer than steroids, allowing pts to tolerate aggressive modalities) - surgery as a last resort |
|
|
|
What are the four types of hip bursitis? ***
|
- trochanteric bursitis
- iliopsoas bursitis - gluteus medius bursitis - ischiogluteal bursitis |
|
|
|
What is the most common type of hip bursitis? ***
|
trochanteric bursitis
|
|
|
|
What muscle passes over the deep trochanteric bursa? ***
|
gluteus medius
|
|
|
|
Etiology of trochanteric bursitis ***
|
- bursa inflamed
- synovial lining thickens and produces fluid from chronic overuse trauma - more common (4:1) in women 30-60 - excess weight is a factor |
|
|
|
Risk factors for trochanteric bursitis ***
|
- repetitive trauma (overuse injuries)
- sudden trauma (fall on trochanter) - problems of normal walking (length disparity in limbs or spinal scoliosis) - rheumatoid arthritis - previous surgeries - bone spurs (osteoarthritis) - rarely but possible: gout |
|
|
|
Signs and symptoms of trochanteric bursitis ***
|
- pain in the hip, radiating down the leg or inward of the hip
- inability to sleep lying on side - physically you can feel a “pointer” or bump on your hip - joint pain and stiffness and/or loss of ROM - redness and warmth to touch (this can also indicate underlying tissue infection) |
|
|
|
Diagnosis of trochanteric bursitis ***
|
patient history
- falls, inability to bear weight when ambulating, difficulty getting up from a sitting position, difficulty with prolonged walking, standing, stair climbing, or walking on slanted surfaces physical exam - may have uneven leg lengths, gait may revel lateral pelvic tilt - patient may report feeling a “snapping” sensation in the outer hip - Obert’s Test: patient lies on unaffected side and the PT stretches the affected leg front to back (flexion, abduction, and extension); positive test when upper leg does not drop into adduction, meaning IT band is tight and compressing the bursa - x-ray - bone scan - MRI - ultrasound |
|
|
|
Interventions for trochanteric bursitis ***
|
- remove cause by strengthening soft tissue of lateral thigh (IT band/TFL)
- focus on flexibility of hip flexors and external rotators; also quadriceps - strengthen hip abductors - heat - ultrasound - transverse friction massage - orthotics if biomechanical faults |
|
|
|
Treatment for acute trochanteric bursitis ***
|
- RICE and NSAIDs
- sleep on unaffected side with pillow between legs - avoid stairs, long walks, repetitive rising and sitting - weight loss if obese |
|
|
|
Treatment for chronic trochanteric bursitis ***
|
- corticosteroid injection into bursa
|
|
|
|
Surgical interventions for trochanteric bursitis ***
|
- bursaectomy
or - lengthening of gluteus maximus tendon or removing the section rubbing directly on greater trochanter |
|
|
|
Post-surgical treatment for trochanteric bursitis ***
|
- CPM for 1st week
- crutches thereafter - ice and e. stim to reduce pain and swelling - exercises for hip |
|
|
|
What is a sprain? ***
|
refers to damage of ligament fibers or its attachment from a violent force
|
|
|
|
What is the most common musculoskeletal injury? ***
|
sprain
|
|
|
|
90% of sprains are _____ in nature. ***
|
lateral
|
|
|
|
Who is most commonly affected by sprains? ***
|
persons between 15-45 years of age
|
|
|
|
Causes of lateral ankle sprains ***
|
- sudden trauma
- catastrophic inversion of the foot - severity depends on force of injury - no evidence of degenerative causes found; however, once a severe injury has occurred, ankle laxity and recurrent ankle problems are common for the injured individual. |
|
|
|
Signs and symptoms of lateral ankle sprain ***
|
- pain – severe throbbing during acute stage and upon palpation of injured site; especially at end range of inversion movement
- swelling – usually around the lateral malleoli; but can spread to the medial aspect of the ankle and the Achilles tendon region depending on severity - warmth and redness – due to increased blood flow to the area |
|
|
|
Diagnosis of lateral ankle sprain ***
|
Physical Examination - full assessment needed for an accurate diagnosis
- physician will observe and palpate injury site ---- discoloration ---- swelling ---- tenderness ---- change in temperature - range of motion ---- active – patient goes through full ROM and any limitation will be noted ---- passive – physician takes pt through full ROM and notes any limitations or pain; helps determine if there is injury to the muscles or tendons which should not be painful due to lack on muscle contraction - anterior draw - helps determine stability of the ankle joint; the more movement allowed while pushing the ankle anteriorly, the more unstable the joint |
|
|
|
3 degrees of lateral ankle sprain ***
|
1st degree – mild - involves tearing some ligamentous fibers without loss of stability
2nd degree - moderate - a measured tear in the affected ligament 3rd degree – severe – complete tear of the affected ligament and total loss of joint stability |
|
|
|
Acute treatment for lateral ankle sprain ***
|
for 3-4 days after injury –
- PRICE formula is recommended (Protection, Rest, Ice, Compression, Elevation) |
|
|
|
Treatment for lateral ankle sprain in sub-acute phase ***
|
4 days to 6 weeks –
- pulsed US or laser can be used to promote healing - light resistive exercises (therabands, balance boards, heel and toe raises) - hot packs and contrast baths |
|
|
|
Treatment of lateral ankle sprain in maturation phase ***
|
6 weeks to 18 months –
- return to function exercises - weight bearing (heel raises, squats, walking/running forwards, backwards, and sideways as tolerated) - eventually moving to running, jumping, and hopping exercises that use one or both legs |
|
|
|
Prevention of future lateral ankle sprains ***
|
- awareness of surroundings and caution navigating uneven ground
- bracing |
|
|
|
What is the plantar fascia? ***
|
- thick band of tissue that connects the calcaneus to the toes
- supports the arch of the foot and helps reduce stress to the foot at midstance - inflammation of the fascia is termed plantar fasciitis and commonly occurs at the insertion on the calcaneus. |
|
|
|
What is the etiology of plantar fasciitis? ***
|
- thought to be caused by repetitive microtrauma to the fascia
- can be due to physiological, structural or external factors: ---- high arches or flat feet ---- obesity ---- footwear lacking arch support ---- prolonged walking or standing on hard surfaces. - pain may also be caused by tibial nerve entrapment in the tarsal funnel |
|
|
|
Signs and symptoms of plantar fasciitis ***
|
- progressive worsening of medial heel pain, most commonly at the insertion on the calcaneus
- pain usually worse in the morning or when walking or standing after periods of non-weight-bearing - limited flexibility in gastrocnemius and soleus - possible limited extension of first MTP joint and ROM of talocrual joint. - antalgic gait pattern - tenderness of gastrocnemius, soleus or plantar fascia when palpated |
|
|
|
Treatment for plantar fasciitis ***
|
- myofascial release to calf and plantar fascia
- joint mobilization of talocrural joint or MTP joint, if restricted - stretching of the calf and plantar fascia. - taping of the plantar fascia to provide support - orthotic insoles or night splints - ultrasound - pulsed for acute phase, continuous for chronic phase - corticosteroid injections - partial or complete fasciotomy for severe cases |
|
|
|
Most of our functional activities occur in the _______, not the anatomic planes. ***
|
diagonal
|
|
|
|
What is the purpose behind "getting in the groove"? ***
|
- to orient the patient to the movement
- to check pt's ROM |
|
|
|
What is the patient's natural response to "getting in the groove"? ***
|
- patient picks up the movement
- patient starts shifting the movement from passive to active |
|
|
|
For how long do you perform PNF on a diagonal? ***
|
to fatigue of patient
(and when they fatigue in one area, move to another diagonal--recuperative movement) |
|
|
|
Another term for "getting in the groove" ***
|
rhythmic initiation
|
|
|
|
How can you change the focus of PNF? ***
|
- it can be passive or active (depending on pt)
- can offer a bit of resistance - can work more slowly (increasing strength) - can work at functional speed (increasing endurance) |
|
|
|
How can PNF be done with stronger patients? ***
|
they can use dumbbells or pulleys
|
|
|
|
What is the progression of normal movement? ***
|
distal to proximal
|
|
|
|
For what types of patients was PNF originally intended? With what types of patients is it now used? ***
|
- neurological patients
- any patients |
|
|
|
How do you guide the patient's movements in PNF? ***
|
with manual resistance you provide
|
|
|
|
If you want to (silently) cue the patient to squeeze your hand, what is the best way to do so? ***
|
squeeze theirs
|
|
|
|
What are repeated contractions? ***
|
- performing PNF in a smaller ROM (like one command)
(e.g., repeatedly performing the "plantar flex and evert" portion of D1E extension) - necessary for learning - helps weak muscle ---- facilitate initiation of motion ---- enhance recruitment ---- increase active ROM and strength ---- offset fatigue - repeat until fatigue noted - emphasis on one pattern, using quick stretch as needed toward end range |
|
|
|
What is irradiation? ***
|
- a.k.a. overflow
- recruits other muscles (either other fibers or adjacent muscles) (e.g., I push harder, they push harder in return--which requires recruitment of more fibers and/or muscles.) - spread of facilitation with increased effort - use of stronger muscles to increase response of weaker muscles |
|
|
|
What is slow reversal? ***
|
- reversing of the agonist and antagonist
- both directions of a diagonal pattern are performed in a smooth, rhythmic fashion with changes of direction occurring without pause or relaxation - generally begin with the stronger pattern first - increase strength and endurance - teach reversal of movement, proper timing - increase coordination |
|
|
|
How are isometrics incorporated into PNF for strengthening? ***
|
- isometric contractions added at different points in range, either
---- at weakest point to strengthen (shown to increase motor neuron recruitment), or ---- at strongest point to recruit overflow (irradiation) |
|
|
|
What is recuperative movement/motion? ***
|
- allowing rest in one pattern, but working on another pattern
- if patient tires from one movement or motion, move on to another (e.g., if tired in one diagonal, move to the other, since different muscle groups are used--flexors vice extensors, external vice internal rotators, etc.) |
|
|
|
What is reversal of agonist? ***
|
- use of eccentric muscle contractions within a pattern to enhance control and strength
(e.g., pt is taken through D1F to shoulder, at which pt holds for an eccentric contraction as therapist pulls the limb back to start, overpowering the pt's hold) |
|
|
|
What are alternating isometrics? ***
|
- alternating isometric contractions of antagonist muscles
- therapist provides isometric resistance in one direction (usually the stronger), telling pt not to let therapist move them - resistance is (gradually) switched to the other direction (by moving one hand at a time), again, instructing pt not to allow themselves to be moved - single plane - start slowly, work to increase speed - no movement of pt or joint should occur - can be done at any point, in any position, with any motion |
|
|
|
What is rhythmic stabilization? ***
|
- alternating isometric contractions progress to this next step (because stabilization is needed first)
- similar to alternating isometrics, but the resistance occurs in opposite directions simultaneously (bidirectional, rotational) - alternating isometric contractions of both agonist and antagonist patterns, resulting in cocontraction - emphasizes rotational stability - produces smooth co-contraction in all three planes simultaneously - can also be the random resistance given on extremities (pt doesn't know where resistance will be offered) |
|
|
|
What is cross transfer? ***
|
- unilateral resistive exercise/strengthening exercises to a limb will increase the strength in the unexercised contralateral limb
|
|
|
|
D1F components of motion ***
(fingers to scapula, since motion is distal to proximal) |
fingers - flexion
wrist - supination, flexion toward radial side forearm - supination elbow - flexion shoulder - flexion, adduction, external rotation scapula - upward rotation, abduction/protraction, (anterior) elevation (putting on an earring) |
|
|
|
D1E components of motion ***
(fingers to scapula, since motion is distal to proximal) |
fingers - extension
wrist - pronation, extension toward ulnar side forearm - pronation elbow - extension shoulder - extension, abduction, internal rotation scapula - downward rotation, adduction/retraction, (posterior) depression (Wolverine) |
|
|
|
D2F components of motion ***
(fingers to scapula, since motion is distal to proximal) |
fingers - extension
wrist - supination, extension toward radial side forearm - supination elbow - flexion shoulder - flexion, abduction, external rotation scapula - upward rotation, adduction/retraction, (posterior) elevation (hitching a ride) |
|
|
|
D2E components of motion ***
(fingers to scapula, since motion is distal to proximal) |
fingers - flexion
wrist - pronation, flexion toward ulnar side forearm - pronation elbow - extension shoulder - extension, adduction, internal rotation scapula - downward rotation, abduction/protraction, (anterior) depression (sheathing a sword) |
|
|
|
D1F components of motion ***
(toes to hip, since motion is distal to proximal) |
toes - extension
foot/ankle - inversion, dorsiflexion knee - flexion hip - flexion, adduction, external rotation (Riverdance) |
|
|
|
D1E components of motion ***
(toes to hip, since motion is distal to proximal) |
toes - flexion
foot/ankle - eversion, plantar flexion knee - extension hip - extension, abduction, internal rotation (IR arabesque) |
|
|
|
D2F components of motion ***
(toes to hip, since motion is distal to proximal) |
toes - extension
foot/ankle - eversion, dorsiflexion knee - flexion hip - flexion, abduction, internal rotation (donkey kick) |
|
|
|
D2E components of motion ***
(toes to hip, since motion is distal to proximal) |
toes - flexion
foot/ankle - inversion, plantar flexion knee - extension hip - extension, adduction, external rotation (crossing the leg) |
|
|
|
Where is rhythmic stabilization typically used? ***
|
trunk
(although it can be used on extremities with random touch or body blade) |
|
|
|
D1F UE is: ***
|
UE flexion-adduction-external rotation with elbow flexion
|
|
|
|
D1E UE is: ***
|
UE extension-abduction-internal rotation with elbow flexion
|
|
|
|
D2F UE is: ***
|
UE flexion-abduction-external rotation with elbow flexion
|
|
|
|
D2E UE is: ***
|
UE extension-adduction-internal rotation with elbow extension
|
|
|
|
D1F LE is: ***
|
LE flexion-adduction-external rotation with knee flexion
|
|
|
|
D1E LE is: ***
|
LE extension-abduction-internal rotation with knee extension
|
|
|
|
D2F LE is: ***
|
LE flexion-abduction-internal rotation with knee flexion
|
|
|
|
D2E LE is: ***
|
LE extension-adduction-external rotation with knee extension
|
|
|
|
Most common uses of PNF
|
- restore ROM
- increase strength & endurance - hasten motor learning - improve coordination - facilitate proximal stability - decrease pain - begin functional progression |
|
|
|
Basic principles of PNF
|
- maximal demands to achieve maximal potential
- strong segments used to facilitate the weak - improvement in specific functional activities is always the goal |
|
|
|
It is widely believed that the CNS, through ____ ____, plays a part in strength gains beyond those attributable to increases in muscle hypertrophy.
|
neural adaptation
|
|
|
|
What is reciprocal innervation?
|
states that contraction of the agonist produces simultaneous relaxation (inhibition) of the antagonist
(the basis for reciprocal inhibition/agonist contraction) |
|
|
|
For what stages of rehabilitation is PNF useful?
|
all stages
- acute - isometric contractions, manual contacts, and indirect approach (e.g., overflow/irradiation, cross transfer) - techniques and patterns can be modified to avoid pain and protect integrity of surgical procedure and/or joint - ultimately, PNF can progress from isometric to concentric and eccentric strengthening with pulleys, dumbbells, etc. |
|
|
|
What proprioceptive and sensory inputs are used to conduct PNF? Toward what goals?
|
- tactile stimulation through PTA's manual contact/grip
- resistance - stretch - irradiation (overflow) - traction - approximation - verbal commands - visual cues used to facilitate motor responses and motor learning |
|
|
|
What are the only surfaces the therapist should touch during PNF? For what purpose?
|
- the area being facilitated
- to apply a demand (appropriate resistance) and give proper cutaneous/pressure stimulation - to control direction of motion and eliminate, correct, or minimize substitution |
|
|
|
How is manual contact usually positioned?
|
- one distal (for movement)
- one proximal (for stabilization) |
|
|
|
Upon what does placement of manual contact depend?
|
strength of patient
|
|
|
|
What a hallmark of PNF and cornerstone of many of its techniques?
|
resistance
|
|
|
|
Why is resistance used in PNF?
|
- to guide movement
- to secure maximal effort - to aid motor relearning |
|
|
|
What is optimal resistance?
|
resistance that is graded appropriately for the intention of the movement
|
|
|
|
What is maximal resistance in PNF?
|
the most resistance that can be applied by the therapist and still result in smooth, coordinated motion for a particular activity performed by the pt
|
|
|
|
Optimal resistance can vary throughout the ROM, depending on...
|
- strength
- joint stability - pain - ability of the pt |
|
|
|
The intention of isometric muscle work is not motion, but....
|
postural stability
(and strengthening) |
|
|
|
Why is PNF especially suited for use with a functional injury?
|
because of the emphasis on varying the type and speed of control needed, especially eccentric control
|
|
|
|
At what strength range does equipment (dumbbells, pulleys, tubing) become necessary for PNF?
|
greater than 4/5
|
|
|
|
What is considered one of the most powerful neurophysiologic tools available?
|
quick stretch
(especially when followed by resistance--facilitates the muscle stretched) |
|
|
|
How is the quick stretch administered?
|
- a quick nudge or tap to muscles under tension, either from fully elongated starting position or superimposed on an active muscle contraction
|
|
|
|
When is the quick stretch contraindicated?
|
- pain
- fracture - recent surgery |
|
|
|
When quick stretch and resistance are used together, what can result?
|
irradiation (overflow) from stronger to weaker segments
|
|
|
|
Into which muscles does irradiation (overflow) typically proceed)?
|
- synergists to the prime mover
- stabilizers of the motion |
|
|
|
What is the key to using a strong motion to reinforce a weaker motion?
|
irradiation (overflow)
|
|
|
|
To what is the amount of irradiation (overflow) directly proportional?
|
to the amount of strength in the resisted muscle groups and the amount of resistance appllied
|
|
|
|
What are traction and approximation?
|
- elongating vector force applied along the long axis of limb to separate joint surfaces, generally to promote isotonic movement (distraction)
- compressive force applied through long axis of limb to facilitate stabilization, extension, and tonic muscle responses (compression) |
|
|
|
Criteria for PNF verbal commands
|
- simple
- direct - timed to coordinate effort and motion - soft commands are soothing and useful in indirect approach - firm commands usually elicit stronger effort from pt |
|
|
|
Benefits of spiral/diagonal movement
|
- combine all planes of motion
- cross midline - are similar to normal functional movement |
|
|
|
A narrow groove of motion at shoulder (UE) and hip (LE) exists at which
|
maximum power is achieved
|
|
|
|
Largest ROM occurs in _____ and _____, least in ____, but Kabat considers it the most important in eliciting strength and endurance changes
|
- flexion and extension
- rotation |
|
|
|
At the UE, what motions always occur together, regardless of diagonal? ***
|
- shoulder flexion and ER with forearm supination
- shoulder extension and IR with forearm pronation - shoulder abduction and hand/wrist extension - shoulder adduction and hand/wrist flexion |
|
|
|
At the LE, what motions always occur together, regardless of diagonal? ***
|
- hip flexion, ankle dorsiflexion, toe extension
- hip extension, ankle plantar flexion, toe flexion - hip adduction with hip ER and foot inversion - hip abduction with hip IR and foot eversion |
|
|
|
Which are the intermediate joints and what is notable about their movement?
|
- elbow and knee
- they may be flexed, extended, or remain straight - varying the position changes the muscle activity, partly because it changes the lever arm |
|
|
|
Patterns may be performed unilaterally or bilaterally. If bilateral, in what two ways can it be conducted?
|
- symmetrically (same diagonals, like butterfly stroke)
- asymmetrically (opposite diagonals going toward same side, like throwing the hammer) |
|
|
|
Bilateral patterns allow the therapist to elicit irradiation (overflow) from a strong segment to.....
|
facilitate weaker motions in the ipsilateral or contralateral extremity
(if contralateral, wouldn't this be cross transfer?) |
|
|
|
What is normal timing of PNF patterns?
|
distal to proximal, leading with hand or foot
|
|
|
|
Even when the pt has adequate strength, the normal timing of PNF patterns may be off. How may the normal timing be facilitated?
|
- by manually restraining the proximal segment until the distal component is activated (with quick stretch and resistance if need be)
- this normal timing promotes motor learning |
|
|
|
In using PNF philosophy of using the strong to facilitate the weak, the PT must first...
|
identify the individual's strength
(an extremity/quadrant that is - pain free - strong - and has controlled and coordinated motion) |
|
|
|
After the PT identifies the pt's strength, what is next?
|
- impairments in ROM, strength, and control
then - functional limitations, such as inability to jump w/o pain then - specific goals |
|
|
|
When administering PNF, how should the therapist be positioned?
|
- facing direction of motion
- shoulders and pelvis facing line of movement - taking up all slack in all components of motion |
|
|
|
What is the best starting position for the patient in PNF?
|
in optimal elongation
|
|
|
|
How is quick stretch administered?
|
- nudge
- using body weight, not arm strength |
|
|
|
How does the therapist move with the patient during PNF?
|
- therapist's COG must move
- distal component initiates motion |
|
|
|
When performing reversals, how does the therapist maneuver his/her hands?
|
change distal manual contact first
|
|
|
|
Examples of how the PNF patterns are progressed
|
- LE - until able to do standing with narrow BOS
- UE - standing and using weights - bilateral for trunk control |
|
|
|
What are considered the most underused but most helpful PNF patterns? Why are they so helpful?
|
- those for the scapula
- because stability and mobility of the scapula is required for normal and pain-free UE function |
|
|
|
Any time two-extremity (bilateral) patterns are combined, the emphasis shifts to....
|
the trunk and proximal extremity components
|
|
|
|
Symmetric bilateral PNF patterns eliminate...
|
the trunk rotation component of the movement
|
|
|
|
Asymmetric bilateral PNF patterns for the UE are called ____ and _____, and can be used to...
|
- lifts
- chops - strengthen trunk or to irradiate into neck, scapula, and extremities |
|
|
|
Chops are....
|
- asymmetric bilateral PNF patterns for the UE
- combine extension-abduction in lead arm with extension-adduction in the grasping arm |
|
|
|
Lifts are....
|
- asymmetric bilateral PNF patterns for the UE
- combining flexion-abduction in one arm with flexion-adduction in the other |
|
|
|
PNF mobility techniques (stretching)
|
- reciprocal inhibition
- autogenic inhibition - rhythmic initiation |
|
|
|
PNF strengthening techniques
|
- slow reversals
- agonist reversal - repeated contractions - timing for emphasis |
|
|
|
PNF stability techniques
|
- alternating isometrics
- rhythmic stabilization |
|
|
|
PNF skill techniques
|
- timing for emphasis
- resisted progression |
|
|
|
PNF endurance techniques
|
- slow reversals
- agonist reversals |
|
|
|
Stages of movement control
|
- mobility
- strengthening - stability - skill - (endurance) |
|
|
|
Advantages of PNF over traditional progressive-resistive programs
|
- therapist can more precisely monitor and correct substitutions
- use of normal movement patterns - emphasis on eccentric control and functional progression - ability to vary speed - better carryover to functional performance measures - techniques can be used with equipment |
|
|
|
Why is eccentric work an essential part of preparation for functional activities?
|
- because the vast majority of high-skill activities have deceleration components
- must be able to control lowering, etc. |
|
|
|
Stability includes both....
|
- nonweight-bearing isometric muscle stability
- dynamic postural activities while weight bearing in proper biomechanical alignment |
|
|
|
Father of preventive medicine
|
Hippocrates
|
|
|
|
What is physical activity?
|
any bodily movement produced by skeletal muscles that results in energy expenditure
|
|
|
|
What is exercise?
|
a type of physical activity that is planned, structured, repetitive, and purposely aimed at improving physical fitness
|
|
|
|
What is physical fitness?
|
a set of attributes that people have or achieve and includes components of:
- health-related (cardiorespiratory endurance, body composition, muscular endurance, muscular strength, flexibility) and - athletic-related skills |
|
|
|
Being physically fit enables an individual to:
|
- perform daily tasks without undue fatigue and with sufficient energy to
- enjoy leisure-time activities and to - respond to emergency situations if they occur |
|
|
|
Name a primary activity used to achieve physical fitness.
|
cardiorespiratory endurance training
|
|
|
|
What is cardiorespiratory endurance training?
|
- performance of repetitive movements of large muscle groups fueled by adequate response from circulatory and respiratory systems to sustain physical activity and eliminate fatigue
- ability of the whole body to sustain prolonged exercise |
|
|
|
Another term for cardiorespiratory endurance training
|
aerobic training
|
|
|
|
What is aerobic capacity?
|
highest rate of oxygen the body can consume during maximal exercise
|
|
|
|
What is considered the best measure of aerobic capacity (and thus of cardiorespiratory endurance and fitness?
|
maximal oxygen uptake
(VO2 max) |
|
|
|
How is MET calculated?
|
(metabolic equivalent)
maximal or submaximal oxygen uptake divided by 3.5 |
|
|
|
What is the body's basic energy source for cellular metabolism and performance of muscular activity?
|
ATP
|
|
|
|
What is the body's preferred energy source?
|
carbohydrates
|
|
|
|
What is the only fuel capable of being used by the CNS?
|
carbohydrates
|
|
|
|
Which is the only fuel that can be used during anaerobic metabolism?
|
carbobhydrates
|
|
|
|
How are carbohydrates metabolized?
|
- converted to glucose
- stored in muscle cells and liver as glycogen |
|
|
|
How many kcal of energy can be stored in the body?
|
1,200 to 2,000 kcal
|
|
|
|
What is the body's largest store of potential energy? How much does it constitute?
|
- fat
- a reserve of about 70,000 kcal in a lean adult |
|
|
|
How is fat generally stored?
|
as triglycerides
|
|
|
|
What must happen to make triglycerides available for use as energy?
|
they must be broken down into free fatty acids (FFA) and glycerol
(a.k.a. lipolysis) |
|
|
|
How are FFAs processed into ATP?
|
by aerobic oxidation
|
|
|
|
Which are more efficient sources of fuel, carbohydrates or fats?
|
- carbohydrates, because lipolysis requires significant amounts of oxygen
- this is why carbohydrates are preferred during high-intensity exercise |
|
|
|
When does protein become an energy source?
|
- during starvation or extreme energy depletion
- provides 5-12% of energy needed to perform endurance exercise |
|
|
|
What is the end product of glycolysis? What is it converted into?
|
- pyruvic acid
- lactic acid |
|
|
|
What does lactic acid do?
|
- accumulates in muscles
- inhibits further glycogen breakdown - eventually impedes muscle contraction |
|
|
|
Another name for aerobic oxidation? Where does this occur?
|
- cellular respiration
- in the mitochondria |
|
|
|
Presence of oxygen enables significantly ______ energy to be produced and results in ability to perform longer periods of work without muscle contraction impeded by lactic acid buildup.
|
more
|
|
|
|
Low-intensity exercise (less than 50% of maximal oxygen consumption) performed for long durations uses what types of fuel? In which pathway?
|
- FFA and carbohydrate
- aerobic oxidative pathway |
|
|
|
In presence of abundant oxygen, as exercise duration increases or intensity decreases, the body uses more...
|
FFAs than carbohydrates for ATP production
|
|
|
|
During moderate to heavy exercise (more than 50% of maximal oxygen consumption) what fuel is used?
|
carbohydrates more than FFAs
|
|
|
|
How is HR affected by exercise? What affects the magnitude of change?
|
- as workload/intensity increases, so does HR
- affected by ---- age ---- fitness level ---- type of activity ---- presence of disease ---- medications ---- blood volume ---- environmental factors (e.g., temperature, humidity) |
|
|
|
What is stroke volume? How is it affected by exercise?
|
- amount of blood (mL) ejected from the heart's left ventricle per heart beat
- as workload increases, SV increases linearly up to about 50% of aerobic capacity, after which it increases only slightly |
|
|
|
What is cardiac output?
|
amount of blood (liters) ejected from the left ventricle per minute
|
|
|
|
Upon what do changes in cardiac output depend?
|
- age
- posture - body size - presence of disease - level of physical conditioning |
|
|
|
What factors influence magnitude of change in SV with exercise?
|
- ventricular function
- body position - exercise intensity |
|
|
|
What is arterial-venous oxygen difference?
|
- amount of oxygen extracted by the tissues from the blood
(oxygen the arteries bring in less what the veins return) |
|
|
|
How does exercise affect arterial-venous oxygen difference?
|
- as intensity increases, arterial-venous oxygen difference increases linearly, indicating the tissues are extracting more oxygen from the blood, creating a decreasing venous oxygen content
|
|
|
|
How does blood flow change with exercise?
|
- at rest, 15-20% of cardiac output goes to muscle
- during exercise, 80-85% to the muscles, away from viscera (why it's not a good idea to eat before working out--no blood for digestion) - during heavy exercise, or when body starts to overheat, blood flow to skin increases to conduct heat away from the core, leaving less blood for working muscles (why athletes cramp up) |
|
|
|
How do SBP and DBP respond to exercise?
|
- SBP increases linearly
- DBP changes little, regardless of intensity (since it is a measure of pressure in the arteries at rest) |
|
|
|
What is a normal DBP change with exercise?
|
< 15 mm Hg
|
|
|
|
How is respiration (pulmonary ventilation) affected by exercise?
|
- increased rate and depth to increase air exchanged per minute
- both tidal volume and respiratory rate increase in proportion to intensity of exercise |
|
|
|
Signs and symptoms of exercise intolerance
|
- angina: chest, left arm, jaw, back, lower neck pain or pressure
- unusual or severe SOB - abnormal diaphoresis - pallor, cyanosis, cold/clammy skin - CNS symptoms: vertigo, ataxia, gait problems, confusion - leg cramps or intermittent claudication - physical or verbal manifestations of severe fatigue or SOB |
|
|
|
Why is respiratory component of performance generally not a limiting factor in development of endurance?
|
because the capacity of the respiratory system to deliver oxygen to the body typically surpasses the ability of the body to use it.
|
|
|
|
What are some coronary risk factors?
|
- male family history of CAD at less than 55 years
- female family history of CAD at less than 65 years - current or recent smoker (quit in past 6 months) - hypertension (140/90 and up) - dyslipidemia ---- LDL > 130 mg/dL ---- HDL < 40 mg/dL ---- total cholesterol > 200 mg/dL - impaired fasting glucose >120 mg/dL - obesity (BMI > 30) - sedentary lifestyle |
|
|
|
Which is the pattern of choice for initiating rotator cuff activities? Why?
|
- D1F
- because of reduced external rotation and abduction ROM components |
|
|
|
Progression of the movements
|
- PROM
- AAROM - AROM - against resistance - slow for strengthening - functional speed for endurance |
|