Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
renin-producing granular cells do what? where are they located?
|
sense pressure, reduce store and release rennin
in afferent arteriole |
|
|
macula densa
|
salt sensor of the nephron
|
|
|
extraglomeular mesangial cells
|
can contract or relax dependent on endogenous substances
Contraction of these cells may restrict flow through some of the capillary loops, thus effectively reducing the area available for filtration (thus a decrease in Kf) and thus a decrease in GFR |
|
|
what is GFR and normal?
|
The volume of filtrate formed per unit time
Don’t forget the units…VOLUME/TIME norm = 180L/Day |
|
|
Rate of filtration =?
|
Kf x NFP
Kf= hydraulic permeability X surface area (thi sis the filtration coefficient) NFP= Net filtration pressure |
|
|
NFP =
|
net filtration pressure
(PGC-PBC-OncoticGC) PGC= glomerular capillary hydrostatic pressure PBC= Bowman's capsule hydrostatic pressure PieGC= Glomeruluar capillary oncotic pressure |
|
|
if you relax the glomeruluar mesangial cells, what will this do to Kf?
|
this increases Kf
so according to Kf x NFR= GFR this increases the GFR |
|
|
FINISH TABLE 2-2
|
SLIDE 11
have to know it |
|
|
if you increase the afferent arteriole resistant, what does it do to PGC? what does this mean for GFR?
|
decrease PGC
decrease GFR |
|
|
if you increase the efferent arteriole resistant, what does it do to PGC? what does this mean for GFR?
|
increase PGC
increase GFR |
|
|
if you decreases renal plasma flow what happens to GFR?
|
When the flow is slow you will get a rapid increase in oncotic GC…this can mean that you stop filtration b/c the oncontic GC opposes filtration
according to Kf x NFP you will decrease GFR |
|
|
Filtration factor=
|
GFR/RPF
|
|
|
Filtration factor is greater at low or high plasma flow?
|
LOW
FF=GFR/RPF |
|
|
if you increase afferent arteriole resistance, what does this do to RBF?
|
decrease
|
|
|
if you increase efferent arteriole resistance, what does this do to RBF?
|
decrease
|
|
|
if you increase afferent AND efferent arteriole resistance, what does this do to RBF?
|
decrease
|
|
|
how is it possible to constrict the efferent arteroile and cause increase GFR and decrease RBF?
|
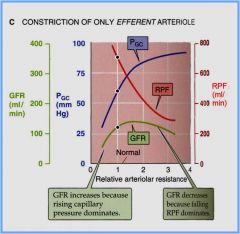
when you vasoconstrict you will increase GFR up to a certain point, yet as RBF starts to decrease, you will reach a threshold where you will not have enough RBF to cause an increase in GFR...
|
|
|
With SNS stimulation (and angiotensin II), BOTH afferent and efferent resistances _____ and RBF _____
|
increase
decrease |
|
|
when you have an increase in RAAS after volume depletion the combined effect will do what to GFR?
|
it will be maintained
even though you decrease RBF this was on a test before..worth knowing that when you have volume depletion and you activate RAAS that GFR will be maintained |
|
|
You give a person a drug that dilates the afferent arteriole and constricts the efferent arteriole by the same amounts.
What effect will this have on GFR, RBF, and FF? |
GFR= increase
RBF= no change FF= increase in spite of the fact that you have that PGC effect to increase GFR, FF is increasing oncotic pressure (you are leaving proteins left behind in the capillary), this will blunt the effect GFR |
|
|
Your patient has entered the ER after a motorcycle accident. His blood pressure is very low and he is tachycardic. You believe he has lost a great deal of blood volume.
What will happen to RAAS? What about FF? |
RAAS will increase
FF will increase after RAAS |
|
|
Your patient has renal artery stenosis. What effect will the stenosis have on RAAS and subsequently on GFR?
|
increase RAAS
maintain GFR angiotension works right where you have that threshold of constricting the efferent arteriole that sets RBF and PGC about equal... |
|
|
what is they myogenic response and where does it occur?
|
increase in BP that would increase the RBF, you get a vasoconstriction to maintain RBF to maintain GFR
this also works in the reverse for low BP THIS HAPPENS AT THE AFFERENT ARTERIOLE**** note this only blunts the effect |
|
|
effects of RAAS/SNS on RBF and GFR
|
RAAS system: Ang II constricts afferent and efferent arterioles (efferent more than afferent)
SNS: constricts both afferent and efferent arterioles Net effect: decrease in RPF w/ only a little or no change in GFR |
|
|
what does ADH do to RBF and GFR?
|
does vasoconstrict, but normally RBF and GFR remain constant
|
|
|
what does ANP do to GFR and RBF?
|
afferent dilation, thus causes increases in both GFR and RBF; also inhibits the secretion of renin
|
|
|
low dose dopamine does what
|
causes low dose vasodilation
|
|
|
generally protective against excessive vasoconstriction like the excess you might see with lots of SNS and ANG II...this describes?
|
Prostaglandins
|
|
|
If you have an increase in renal arterial pressure, what does this do to GFR?
|
this increases PGC
in the equation GFR= Kf (PGC-PBC-OncoticGC) so increase GFR |
|
|
what does decreasing afferent arteriolar resistance do to GFR?
|
this increases PGC
in the equation GFR= Kf (PGC-PBC-OncoticGC) so increase GFR |
|
|
what does efferent constriction do to GFR?
|
this increases PGC
in the equation GFR= Kf (PGC-PBC-OncoticGC) so increase GFR |
|
|
if you have obstruction of a tubule or increased intratubular pressure, what does this do to GFR?
|
this increases PBC
in the equation GFR= Kf (PGC-PBC-OncoticGC) so decrease GFR |
|
|
if you have an increase in systemic-plasma oncotic pressure what will this do to GFR?
|
this increases OncoticGC
in the equation GFR= Kf (PGC-PBC-OncoticGC) so decrease GFR |
|
|
decrease in renal plasma flow will do what to GFR?
|

this causes an increase rise of oncotic GC
so in the equation GFR= Kf (PGC-PBC-OncoticGC) so decrease GFR |