Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
123 Cards in this Set
- Front
- Back
|
Is the vulva hair bearing skin?
|
Yes
this means you can get skin related diseases: - psoriasis - eczema - allergic dermatitis - infections - skin cysts |
|
|
- This is a common cyst of the Vulva
- can occur in all ages - second to infection with obstruction of the duct |
Bartholin cyst
Obstruction of the Barholin gland |
|
|
Barolin cyst pic
What is the Tx for these cysts? |
Tx: excision of cyst
|
|
|
This is a disease of the vulva:
- second to inflammation of surface mucosa and glands -small ulcerations of mucosa |
Vestibulitis
|
|
|
What is the tx for vestibulitis?
|
Tx: excision
|
|
|
ok this is sad but....
There are 5 Non-Neoplastic Epithial Disorders of the vulva you need to know: he did not details these |
1. Leukoplakia
2. Vitiligo 3. Inflammatory lesions-psoriasis, chronic dermititis 4. Intraepithelial neoplasia --> invasive carcinoma 5. Paget's disease |
|
|
If on exam you see:
white/opaque plaquelike scaley mucosal lesion what is your Dx? |
Leukoplakia
A non-neoplastic epithelial disorder of the Vulva |
|
|
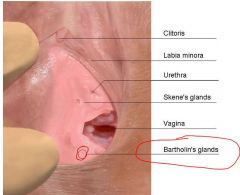
What is the Vulva?
|
The structures of the external genitalia for women
|
|
|
What is this disease?:
- atrophy, fibrosis, scarring of vulva - skin becomes pale gray, "parchment like" - Labia become atrophied - introitus is narrowed - characteristic- subepithelial fibrosis*** - most commonly occur after menopause - may present as an autoimmune disease |
Lichen sclerosis of the vulva
|
|
|
If on exam you see:
- white parchment like patches of the skin of the vulva and labial atrophy What is your Dx? |
Lichen Sclerosis
|
|
|
There are 4 cardinal histological features of Lichen sclerosis?
|
1. atrophy - thinning of the epidermis, disappearance of rete pegs
2. Hydropic degeneration of basal cells 3. Replacement of underlying dermis - by dense collagenous fibrous tissue 4. Monoclonal bandlike lymphatic infiltrate - can look like leukoplakia |
|
|
What is hydropic degeneration of basal cells?
|
hydropic degeneration is a condition of cell in which cloudy swelling appears.in this condition granulation in cell also present so it also know as albuminous degeneration also.
|
|
|
picture of lichen sclerosis
|

|
|
|
What age is primary affected by lichen sclerosis?
|
affects women >50yrs old
tends to be slow in developing insidious progressive |
|
|
Is Lichen sclerosis pre-cancerous?
|
Nope
BUT does confer increased risk of subsequent cancer 1-4% |
|
|
This is a non-specific condition resulting from rubbing or scratching the skin.
It is Characterized by acanthosis of the vulvar squamous epithelium - frequently with hyperkeratosis May see thickened epithelium increased mitotic activity in both the basal and prickle cell layers? |
Lichen simplex chronicus
|
|
|
What is acanthosis?
wiki style |
Acanthosis is diffuse epidermal hyperplasia.[1] Acanthosis implies increased thickness of stratum spinosum. It is a disease of the prickle cell layer of the skin, where warts appear on the skin or inside the mouth.
|
|
|
what is hyperkeratosis?
wiki style |
is thickening of the stratum corneum, often associated with a qualitative abnormality of the keratin,[1] and also usually accompanied by an increase also in the granular layer.
|
|
|
In what layers may you see increased mitotic activity with:
Lichen simplex chronicus |
1. basal layer
2. prickle cell layer |
|
|
Lichen simplex chronicus and cancer risks....
|
1. is sometimes associated with carcinoma
2. considered a significant cancer precursor - unless........ epithelial atypia coexists |
|
|
Now what if epithelial atypia actually does also exist?
|
Lichen simplex chronicus is then classified as a precancerous lesion!
VIN/vulvar intraepithelial neoplasia |
|
|
What is indicated for a lichen simplex chronicus lesion?
|
BIOPSY all lesions***** EXAM
|
|
|
What is lichen simplex chronicus second to?
|
pruritis
|
|
|
What infections can lichen simplex chronicus be associated with?
|
Tinea
or Candida and also unknown causes |
|
|
lichen simplex chronicus
wiki style |
Lichen simplex chronicus (also known as "Neurodermatitis"[1]) is a skin disorder characterized by chronic itching and scratching.[2]:58 The constant scratching causes thick, leathery, brownish skin.
|
|
|
Let's just take a minute and recap:
Vulva: 1. Bartholin cyst 2. Vestibulitis 3. 5 Non-Neoplastic Epithelial Diorders 4. Lichen Sclerosis 5. Lichen Simplex Chronicus |
moving now to neoplasms
|
|
|
What types of glands do the vulva contain?
|
modified apocrine sweat glands
|
|
|
This is a s a sharply circumscribed nodule of ectopic breast tissue usually found on the labia majora or the interlabial folds. It is benign tissue (not cancerous) but is often confused clinically with carcinoma of the vulva because of its tendency to ulcerate.
It is identical in appearance to intraductal papillomas of the breast? |
Papillary hidradenoma
|
|
|
this is a benign adenoma is a cutaneous condition, primarily occurring in adult women, that is a form of benign adnexal neoplasm
presents as a sharply circumscribed nodule in the apocrine sweat gland? |
Hidradenoma
|
|
|
Where do papillary hidradenoma and hidradenoma most likely occur?
|
Labia majora
or interlabial folds has a tendency to ulcerate |
|
|
Where are hidradenoma papilliferum most commonly found?
|
small discrete nodule is usually seen in the interlabial sulcus
|
|
|
Do hidradenimas present before or after puberty?
|
virtually nonexistent in prepubertal females
|
|
|
If you see a micro slide and it says:
the tumor is well-circumscribed, soft, gray-white to red, solid or cystic nodule what is it? |
HIDRADENOMA PAPILLIFERUM
|
|
|
on a slide you see:
well-circumscribed subepithelial nodule composed of papillae having prominent fibrovascular cores |
HIDRADENOMA PAPILLIFERUM
|
|
|
This is a benign raised/wartlike aka verrucous condition of the vulva:
1. Condyloma acuminatum 2. Mucosal polyps 3. syphilitic condyloma latum |
all involve warts
main to know is condyloma acuminatum :) |
|
|
a papillomavirus induced squamous lesion
aka venereal wart this is the most common venereal wart |
Condyloma acuminatum
|
|
|
this is a benign stromal proliferation covered with squamous epithelium
|
mucosal polyps
|
|
|
Sexually transmitted, benign tumors with a distinctly verrucous gross appearance
often appear in coalesce can be found around the perineal area, vulvar, and perianal regions looks identical to those lesions on male's penis and around anus in men |
Condyloma acuminatum
|
|
|
What HPV types cause warts?
|
multiple genital warts
caused mainly by HPV, types 6 and 11*** |
|
|
Are warts caused by HPV 6 & 11 malignant or benign?
|
benign genital warts
|
|
|
Where do the warts 6 & 11 replicate?
|
in the squamous epithelium
the lifecycle is completed in the mature superficial cells of the epithelium |
|
|
What is the cell you will see with HPV?
|
Koilocytic atypia
|
|
|
Lesions consist of a branching, treelike proliferation of stratified squamous epithelium supported by a fibrous stroma
|
Condyloma
know tree branching!!!**** |
|
|
What will you see on surface cells in cells infected with HPV?
|
Acanthosis, parakeratosis, hyperkeratosis, and nuclear atypia in the surface cells
Acanthosis: Acanthosis is diffuse epidermal hyperplasia.[1] Acanthosis implies increased thickness of stratum spinosum. perikeratosis: Parakeratosis: The orderly but abnormal keratinization of cells so that the keratin layer consists of plump nucleated keratinized cells instead of annular squames. It is associated with the thinning or loss of the granular layer and is usually seen in diseases of increased cell turnover, whether inflammatory or neoplastic |
|
|
Leech definition of Koilocytosis
|
koilocytosis = combination of perinuclear cytoplasmic clearing + crinkling of nuclear membrane
|
|
|
Is carcinoma of the vulva common?
|
NOPE
Carcinoma of the vulva – is an uncommon lesion (1/8 as frequent as cervical cancer) |
|
|
If a carcinoma of the vulva did occur what would this be in?
|
About 2/3’s occur in women > 60 years
|
|
|
What is the most common type of permalignant / malignant neoplasm?
|
85% of these malignant tumors are squamous cell carcinomas
The remainder are BCC’s, melanomas, adenoca |
|
|
Vulvae scc’s –can be divided into two general groups
|
1. cancer-related (high risk) HPV
2. Associated with squamous cell hyperplasia and lichen sclerosis |
|
|
Group 1:
cancer-related (high risk) HPV what is this group frequently preceded by? |
Frequently coexists with or preceded by VIN/vulvar intraepithelial neoplasia
|
|
|
What is a disease included with VIN?
|
Includes CIS/Bowen disease
|
|
|
What is CIS/Brown disease?
|
Carcinoma In Situ
a neoplastic skin disease, it can be considered as an early stage or intraepidermal form of squamous cell carcinoma. |
|
|
What are features of VIN cells?
|
Vulvar Intraepithelial Neoplasia
nuclear atypia in the epithelial cells, increased mitoses, and lack of surface differentiation normal progression of cell maturation within the vulvar squamous epithelium from basal layer to surface is lost/ “loss of polarity” |
|
|
What will may some cells look like in VIN histology?
|
Some cells look like undifferentiated basaloid cells
|
|
|
If you see evidence of single cell keratinization (“dyskeratosis”)
What is this? |
VIN
|
|
|
ON EXAM:
what do 90% of cases of VIN contain? |
90% of cases of VIN contain HPV DNA , specifically types 16, 18 and other high risk types
|
|
|
What age and status increases the risk of invasive cancer?
|
Risk of progression to invasive cancer increases in older women (> 45 y.o.) or immunosuppressed women
|
|
|
What do HPV-associated vulvar squamous cell carcinoma start as?
|
Begin as classic VIN lesions
Present as discrete flesh-colored or pigmented slightly raised lesions Coexiting carcinomas may be exophytic or indurated, frequently with ulceration |
|
|
Second group of SCC:
Associated with squamous cell hyperplasia and lichen sclerosis What is the cause? |
unknown
|
|
|
Is the second group of SCC:
Associated with squamous cell hyperplasia and lichen sclerosis typically associated with HPV? |
NOPE
|
|
|
What is the second group of SCC termed?
|
Unusual form of VIN termed differentiated (simplex) VIN****
|
|
|
What is the second group SCC associated with?
|
also been associated with increased accumulation of p53 protein/detect by ICC***
|
|
|
This ends the HPV(+) vular SCC
|
now begin HPV (-) vulvar SCC
|
|
|
These are Carcinomas associated with lichen sclerosis, lichen simplex chronicus, and differentiated may develop quickly
|
HPV(-) VULVAR SCC
|
|
|
May be seen as nodules in a background of vulvar inflammation
|
HPV(-) VULVAR SCC
|
|
|
What can this inflammation be mistaken for?
|
This inflammation can be mistaken for dermatitis, eczema, or leukoplakia
|
|
|
What are the main complaints of HPV(-) vulvar SCC?
|
Complaints are chiefly non-specific/local discomfort, itching and exudation d/t superficial secondary infection
|
|
|
What is the VIN grading system?
|
VIN1
VIN2 VIN3 CIS |
|
|
mild; dysplastic cells are confined to the lower third of the epithelium
|
VIN1
|
|
|
moderate; dysplastic cells occupy up to the lower 2/3’s of the epithelium
|
VIN2
|
|
|
severe; CIS/carcinoma in situ; here, dysplastic cells extend into the upper 1/3 of the epithelium
|
VIN3
|
|
|
term may be used when dysplastic cells occupy the full thickness of the epithelium and the underlying stroma has not been invaded
|
CIS
|
|
|
What is the risk of invasive cancer developement with VIN?
|
mainly a function of age, extent of tumor and immune status
|
|
|
What is metastatic spread linked to once invasion takes place in VIN?
|
Once invasion takes place – metastatic spread is linked to size of tumor, depth of invasion, and lymphatic involvement
|
|
|
What lymph nodes are commonly involved with cancer in VIN?
|
The inguinal, pelvic, iliac, and periaortic lymph nodes are most commonly involved
|
|
|
What is the final stage of cancer development in VIN that is also the worst?*****
|
Finally, lymphohematogenous spread lungs, liver, other internal organs
|
|
|
What is the survival rate if the cancer is <2cm?
|
If < 2 cm 5 yr.
Survival rate (s/p one stage vulvectomy + lymphadenectomy) = 60-80% |
|
|
How common is SCC?
|
SCC – represents about 95% of all vulvar malignancies
|
|
|
What are the risk factors for Invasive squamous cell carcinoma?
|
Risk factors include: cigarette smoking, number of sexual partners, and chronic granulomatous disease
|
|
|
Vulvar SCC – divided into 2 general ‘types:’
|
First type: affects older women and is not related to HPV
Second type: affects younger women and is related to HPV |
|
|
affects younger women and is related to HPV
|
second type
|
|
|
affects older women and is not related to HPV
|
first type
|
|
|
INVASIVE SCC – CLINICAL FEATURES
|
can begin as an area of induration
But progresses to form an exophytic mass Or an endophytic ulcer with raised, everted edges |
|
|
Where do most invasive SCC form?
location |
***EXAM :)
The labia are the most common location (90% labia majora more than minora; clitoris 10%) |
|
|
Are most squamous cell carcinoma of the vulva:
well differentiated or poorly differentiated |
Well differentiated
Are well differentiated with keratinization, i.e., with keratin formation VIN and keratosis (i.e., epithelial hyperplasia) are often present at the margins |
|
|
What may some high grade SCC show areas of?
|
Some high grade SCC’s show focal areas of glandular differentiation
invasive SCC |
|
|
What is the clinical course of Invasive SCC?
|
1) The tumor grows slowly – extends to the contiguous skin
2)Invades deeply to involve the vagina and rectum with mets to regional L.N.’s 3) Regional L.N. mets occur in ca. 20% of cases 4) Tumors of labia first to regional inguinal L.N.’s; clitoris mets directly into deep nodes 5) Overall 5 yr. Survival of treated pts. Is 50% for (+) nodes, and 75% for (-) nodes |
|
|
How do the invasive SCC spread of tumors of the labia compare with clitoris?
|
Tumors of labia first to regional inguinal L.N.’s;
clitoris mets directly into deep nodes |
|
|
What is Tx for invasive SCC?
|
Usual treatment – radical vulvectomy with bilateral radical inguinal L.N. dissection
|
|
|
What could you so in advanced cases of invasive SCC?
|
Iliac lymphadenectomy and pelvic exenteration are reserved for advanced cases
|
|
|
What is the tx for early cases of invasive SCC?
|
Early cases – treated conservatively/wide local excision
|
|
|
Finish vulvar disease
|
moving to vagina
|
|
|
Do many disease affect the vagina?
|
Remarkably free from primary disease
Uncommon congenital anomalies Usually associated with genetic syndromes |
|
|
This involves Lateral walls of vagina --> wolffian duct rests
|
Gartner duct cysts
|
|
|
What are 3 infectious diseases of the vagina?
|
Gardnerella vaginalis
Candidiasis Trichomonas |
|
|
When do benign lesions of the vagina occur?
|
Occur during repoductive years
|
|
|
This is a benign lesion of the vagina that has a skeletal muscle origin?
|
Skeletal muscle origin - rhabdomyoma
|
|
|
what does this describe?
the cells lie in a collagenous or myxoid stroma stroma contains thin-walled blood vessels cells with cross striations may be abundant focally mitotic figures generally are absent |
Vaginal Rhabdomyoma
|
|
|
What does this describe?
dense fibrovascular stroma lies beneath an intact squamous epithelium/benign lesion |
Vaginal stromal polyp
|
|
|
What may a stomal polp arise from?
|
stromal polyp may arise from expansion of the subepithelial stromal zone
|
|
|
How are stromal polyps (which are benign) compare with rhabdomyosarcoma?
|
unlike rhabdomyosarcoma (in young children) it lacks rapid growth, invasion of adjacent tissues, hypercellularity, and cells with striations
|
|
|
What are the 3 benign neoplasms of the vagina?
|
1. Skeletal muscle origin-rhabdomyoma
2. Stromal lesions - stromal polyps 3. Atrophic vaginitis |
|
|
What are most premalignant and malignant neoplasms of the vagina?
|
95% are squamous cell carcinoma
Most are associated with HPV |
|
|
What is the greatest risk factor for vagina cancer?
|
Greatest risk factor is previous ca of cervix or vulva
|
|
|
What is VAIN?
|
Vaginal intraepithelial neoplasia
|
|
|
When is VAIN most likely to occur?
|
Although the age range is broad – most patients are postmenopausal
|
|
|
How is VAIN graded?
|
VAIN I: mild dysplasia
VAIN II: moderate dysplasia VAIN III: severe dysplasia/carcinoma in situ/CIS |
|
|
for grading VAIN how are they like cervical cancer?
|
grading squamous intraepithelial neoplasms of the vagina are the same as those for lesions of the cervix
|
|
|
Is invasive squamous cell carcinoma/SCC common in the vagina?
|
Much less common than its counterpart in the cervix or vulva
|
|
|
What must you do 1st when determining invasive cancer of the vagina?
|
One must exclude – metastases from a cervical or vulvar primary
|
|
|
How can you call a invasive squamous cell carcinoma - primary vaginal
|
Call a vaginal carcinoma primary – only if the cervix is uninvolved or minimally involved by a tumor ‘obviously’ arising in the vagina
|
|
|
how does the appearance on micro slides for vaginal compare with cervical and vulvar cancers?
|
vaginal morphologic appearance duplicating that of their more common cervical and vulvar counterparts
|
|
|
How are most vaginal cancers treated?
|
Is usually treated by a combination of external and intracavitary radiation
|
|
|
when would you consider a radical vaginal surgery?
|
Radical surgery for selected cases located in the upper vaginal third or posterior wall
|
|
|
What is vaginal clear cell cacinoma?
wiki style |
A rare type of tumor, usually of the female genital tract, in which the insides of the cells look clear when viewed under a microscope. Also called clear cell carcinoma and mesonephroma.
|
|
|
How is vaginal and clear cell carcinoma associated?
|
The association of vaginal and cervical clear cell carcinoma with in utero*** exposure to DES is well known
|
|
|
What is DES?
|
A synthetic form of the hormone estrogen that was prescribed to pregnant women between about 1940 and 1971 because it was thought to prevent miscarriages. DES may increase the risk of uterine, ovarian, or breast cancer in women who took it. It also has been linked to an increased risk of clear cell carcinoma of the vagina or cervix in daughters exposed to DES before birth. Also called diethylstilbestrol.
|
|
|
What is the median age of clear cell carcinoma?
|
Patients range in age from 7 to 37 years/median age is 19 years
|
|
|
When is clear cell distinctly uncommon?
|
The tumor is distinctly uncommon before age 12 and after age 30
|
|
|
What will the clear cell carcinoma look like grossly?
|
appears as a polypoid, nodular, flat, or ulcerated mass/usually in the anterior or lateral wall of the upper vagina
|
|
|
On micro slide you read:
-consists of sheets of cells with pleomorphic nuclei and clear cytoplasm - and papillae with cells having dense, eosinophilic cytoplasm |
Clear cell adenocarcinoma
|
|
|
When clear cell metastasizes where does it go?
|
When it metastasizes pelvis, lungs and supraclavicular L.N.’s
|
|
|
What is this?:
Aka sarcoma batryoides polypoid mass protruding from the vagina Uncommon Usually in infants and children < 5 y/o Tx with surgery and chemotherapy |
Embryonal Rhabdomyoscarcoma
|