Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
What are the functions of sleep?
|
- Restoration and recovery
- Energy conservation - Behavioral adaptation - Neural networks / plasticity |
|
|
What are the five behavioral characteristics of sleep in animals?
|
- Behavioral quiescence (inactivity)
- Stereotypic posture - Elevated arousal threshold - Rapid state reversibility - Achieved spontaneously |
|
|
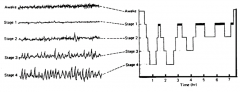
What are the features of brain waves during the awake stage?
|

Low voltage, random and fast
|
|
|
What are the features of brain waves during the drowsy stage?
|

- 8-12 Hz
- Alpha waves |
|
|
What are the features of brain waves during the stage 1 sleep?
|

- 3-7 Hz
- Theta waves |
|
|
What are the features of brain waves during the stage 2 sleep?
|

- 12-14 Hz
- Sleep spindles and K complexes |
|
|
What are the features of brain waves during the stage 3-4 sleep?
|

- 1/2 - 2 Hz
- Delta waves > 75 µV |
|
|
What are the features of brain waves during the REM sleep?
|

- Low voltage
- Random, fast w/ "sawtooth pattern" |
|

What is this wave pattern characteristic of?
|

Awake
Low voltage, random and fast |
|

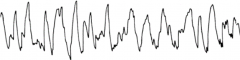
What is this wave pattern characteristic of?
|

Drowsy Stage
- 8-12 Hz - Alpha waves |
|

What is this wave pattern characteristic of?
|

Stage 1 Sleep
- 3-7 Hz - Theta waves |
|
What is this wave pattern characteristic of?
|

Stage 2 Sleep
- 12-14 Hz - Sleep spindles (bracket) |
|
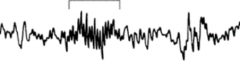
What is this wave pattern characteristic of?
|

Stage 2 Sleep
- 12-14 Hz - K complexes (tall peak) |
|
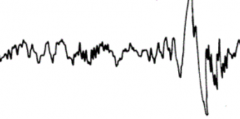
What is this wave pattern characteristic of?
|

Stage 3/4 Sleep:
- 1/2 - 2 Hz - Delta waves > 75 µV |
|

What is this wave pattern characteristic of?
|

REM Sleep:
- Low voltage - Random, fast w/ "sawtooth pattern" |
|
|
How frequently do you go through cycles of REM sleep?
|
Every 90-120 minutes (ultradian rhythm)
|
|
|
A lesion where would cause narcolepsy?
|
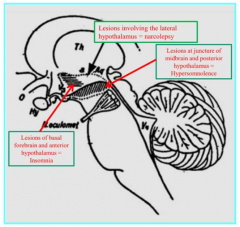
Lateral Hypothalamus
|
|
|
A lesion where would cause hypersomnolence?
|
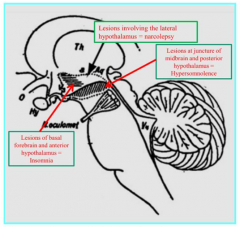
Juncture of midbrain and posterior hypothalamus
|
|
|
A lesion where would cause insomnia?
|
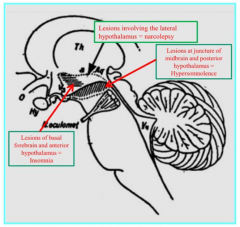
Basal forebrain and anterior hypothalamus
|
|
|
What happens if there is a lesion involving the lateral hypothalamus?
|
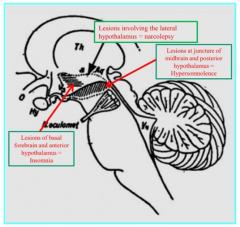
Narcolepsy
|
|
|
What happens if there is a lesion involving the juncture of the midbrain and posterior hypothalamus?
|
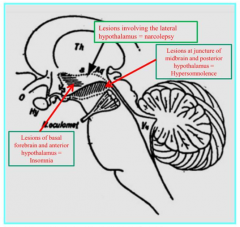
Hypersomnolence
|
|
|
What happens if there is a lesion involving the basal forebrain and anterior hypothalamus?
|
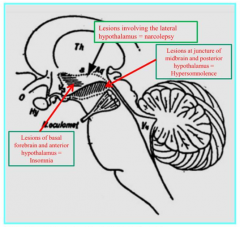
Insomnia
|
|
|
What happens if there is a lesion to the pontomesencephalic brainstem (lesion between pons and mesencephalon)?
|
Coma
|
|
|
A lesion where can cause a coma?
|
Pontomesencephalic brainstem (lesion between pons and mesencephalon)
|
|
|
What do ascending arousal systems connect?
|
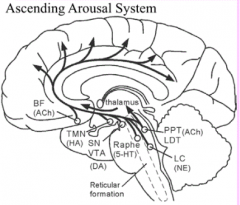
- From brainstem and posterior hypothalamus
- To forebrain, cortical and subcortical targets |
|
|
What kind of neurons innervate ascending arousal system and cerebral cortex?
|
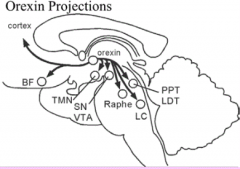
Orexin neurons
|
|
|
Which NTs inhibit cells in the PPT / LDT during W and NREM sleep?
|
Aminergic (NE, 5HT, Histamine)
|
|
|
Which NTs inhibit arousal during NREM sleep?
|
GABA and Galanin from VLPO
|
|
|
Which neurons drive REM sleep? Which are inhibited?
|
- Cholinergic neurons
- Aminergic inputs are inhibited during REM, thereby dis-inhibiting the PPT/LDT |
|
|
What is happening at the PPT/LDT during REM and NREM sleep?
|
- REM: disinhibited d/t silent aminergic inputs
- NREM: inhibited by aminergic inputs |
|
|
What signals cause REM sleep to be atonic (no muscular tone)?
|
- Post-synaptic inhibition of motor neurons
- Hyperpolarization of motor neuron membranes - Activated thalamus |
|
|
What hormone is responsible for the Circadian rhythm?
|
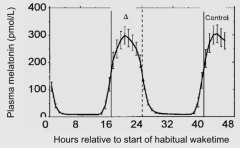
Melatonin: high during the night and low during the day
|
|
|
What happens if you have no cues to tell you when to go to bed (clocks/sun)?
|
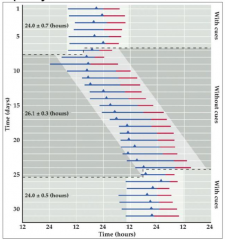
- Without cues you start going to bed an hour later everyday
- Your body thinks the day has about 26 hours without cues vs 24 hours with cues |
|
|
What kind of somatic activity occurs during NREM vs REM sleep?
|
- NREM: few motor events, body repositioning
- REM: paralysis, phasic events (rapid eye movements and muscle twitches) |
|
|
How does the CNS activation during NREM and REM sleep compare?
|
NREM:
- mean discharge rate of neurons decreased - cerebral glucose utilization is decreased overall REM: - mean discharge rate of neurons increased in many regions (PGO spikes and rapid eye movements) - cerebral glucose utilization increased (resembles W) - cerebral blood flow greatly increased |
|
|
How does the HR change during NREM vs REM sleep relative to when awake? Why?
|
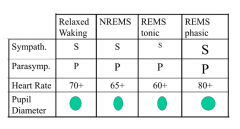
NREM:
- Slightly lower HR (70-->65 bpm) - D/t more parasympathetic activity REM (tonic): - Lower HR (70-->60 bpm) - D/t less sympathetic and more parasympathetic activity REM (phasic): - Higher HR (70-->80 bpm) - D/t more sympathetic and more parasympathetic activity |
|
|
During what phase of sleep is the pupil diameter the greatest? Smallest?
|
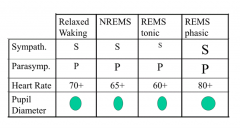
- Largest: REM phasic sleep
- Smallest: NREM and REM tonic sleep |
|
|
How does the BP compare for NREM and REM sleep?
|
- NREM: BP tends to decrease
- REM: BP is highly variable |
|
|
How does the CO and blood vessel diameter compare for NREM and REM sleep?
|
NREM:
- CO reduced - Blood vessels dilated REM: - Blood vessels constricted |
|
|
Which hormones are elevated during sleep?
|
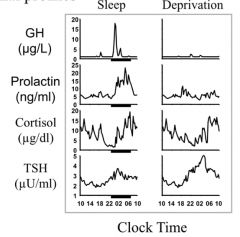
- Growth Hormone
- Prolactin - Melatonin |
|
|
Which hormones are suppressed during sleep?
|
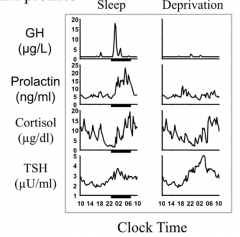
- Thyroid Stimulating Hormone
- Cortisol |
|
|
What happens to Cortisol during sleep?
|
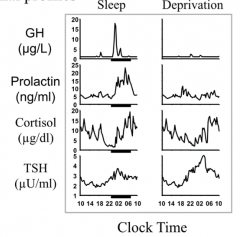
- Inhibited by sleep onset
- Progressive increase to high levels toward end of sleep |
|
|
What happens to TSH during sleep?
|
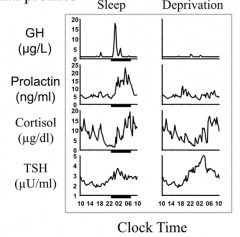
- Inhibited by sleep onset
- Decreased across sleep period |
|
|
How does thermoregulation compare for NREM and REM sleep?
|
NREM:
- Lowered temperature set point - Shivering threshold lower - Sweating at normal ambient temperatures REM: - No regulation - No shivering response - No sweating at high ambient temperature - Body temperature drifts toward ambient (surroundings) temperature Wakefulness: - Full regulation |
|
|
How does HR, RR, and penile erection change during REM sleep?
|

- HR elevated
- RR elevated - Penile erection during REM sleep that gets stronger closer to morning |
|
|
What types of tests are used in sleep medicine?
|
- Polysomnography
- Multiple Sleep Latency Testing - Actigraphy - Sleep Diary |
|
|
What kind of sleep disorders can be diagnosed by testing?
|
- Obstructive sleep apnea
- Central sleep apnea - Periodic limb movement disorder - Parasomnias - Narcolepsy - Circadian rhythm disorders |
|
|
What is Polysomnography useful for diagnosing?
|
- Obstructive Sleep Apnea (OSA)
- Periodic Limb Movement Disorder |
|
|
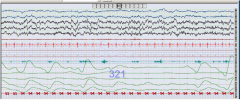
What is monitored on Polysomnography?
|
- EEG: recording of the brain's spontaneous electrical activity
- EOG: measuring the resting potential of the retina in the human eye - EMG: evaluating physiologic properties of muscles - Respiratory electrodes Get full physiologic monitoring. |
|
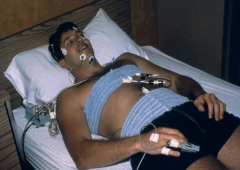
What is this an example of?
|
Polysomnogram
|
|
|
How do you determine the breathing pattern during Polysomnography?
|
- Pressure sensor under nose
- Temperature detector - Also have abdominal and thoracic belts to detect if there is effort to breathe |
|
|
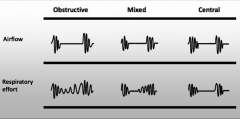
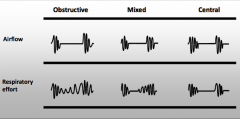
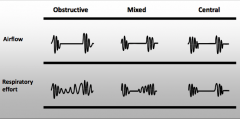
What are the three characteristic patterns of apnea?
|
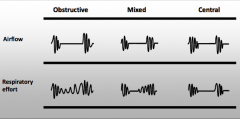
- Obstructive
- Central - Mixed |
|
|
What happens in an Obstructive Apnea?
|
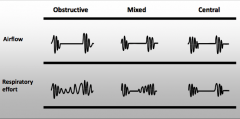
- Absence of airflow despite persistent ventilatory efforts
- Demonstrated by contraction of respiratory muscles such as the diaphragm |
|
|
What happens in a Central Apnea?
|
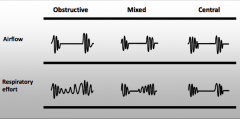
- Absence of airflow due to the lack of ventilatory effort
- Since no effort is made to breathe, no airflow occurs |
|
|
What happens in a Mixed Apnea?
|
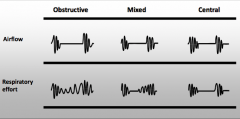
- Includes both Obstructive and Central Apnea components
- Initial Central component followed by an Obstructive component |
|
|
Which of the sleep apneas are treated in the same way?
|
- Obstructive
- Mixed |
|

Top is airflow, bottom is respiratory effort.
What kind of apnea? Why? |
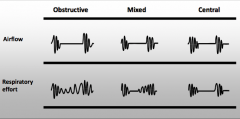
Obstructive Apnea
- Absence of airflow despite persistent ventilatory efforts - Demonstrated by contraction of respiratory muscles such as the diaphragm |
|

Top is airflow, bottom is respiratory effort.
What kind of apnea? Why? |
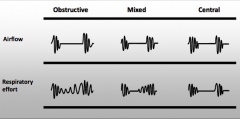
Mixed Apnea
- Includes both Obstructive and Central Apnea components - Initial Central component followed by an Obstructive component |
|

Top is airflow, bottom is respiratory effort.
What kind of apnea? Why? |
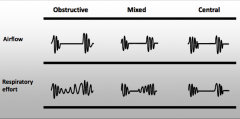
Central Apnea
- Absence of airflow due to the lack of ventilatory effort - Since no effort is made to breathe, no airflow occurs |
|
|
What can we diagnose from a sleep study?
|
- Sleep disordered breathing (evaluation and treatment)
- Movement disorders of sleep - Parasomnias |
|
|
When would a sleep study be useful for research?
|
- Sleep structure in health and disease
- Insomnia and effect of medications |
|
|
What are the uses of a sleep diary?
|
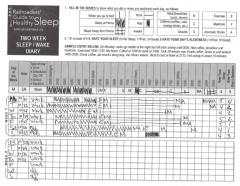
- Quantifying sleep
- Assessing pattern of sleep - Assessing factors affecting sleep timing (e.g., alcohol, caffeine, exercise, medicine, nap, etc) |
|
|
What does Actigraphy do?
|

- Motion detector
- Reinforces / compliments sleep diary |
|
What are these results from? What do they show?
|
- Actigraphy
- Normal sleeper |
|
|
What are the uses of Actigraphy?
|
- Objectively quantifies sleep over time
- Objectively assesses sleep patterns - Can be useful for assessing larger numbers of people for sleep quality (research and clinical tool) - Useful for assessing a child or cognitively impaired person's sleep pattern |
|
|
What is Actigraphy unreliable for?
|
Insomnia
|
|
|
What happens in a Multiple Sleep Latency Test (MSLT)?
|
- Objectively measures sleepiness
- 20 minute opportunities to nap every 2 hours for 5 sessions in a row - Unit of measure is minutes from lights out to sleep onset |
|
|
What is a normal sleep latency? What indicates pathological sleepiness?
|
- Normal is > 10 minutes
- Pathologically sleepy is < 8 minutes |
|
|
What is normal / abnormal for REM sleep during MSLT?
|
REM sleep during more than one nap is abnormal (it takes 90-120 minutes normally to get into REM sleep so even one nap is abnormal)
|
|
|
What is measured in a Multiple Sleep Latency Test (MSLT)?
|
- Central (1, 2) and Occipital (3, 4) EEG leads
- Chin movement (5) - should be no movement during REM - EOG (eye movements seen in REM) (6, 7) - EKG (8) |
|
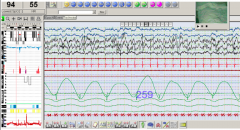
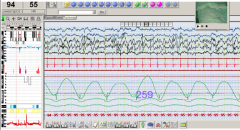
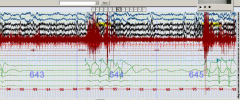
Case: 5'7" 240 lb male w/ CAD and diabetes who is snoring very loudly. He has trouble staying awake during the day and while driving even though he gets "8 hours" of sleep / night.
What is wrong? |
Probably Obstructive Sleep Apnea
- Air flow channels are showing no air flow (not breathing) - Chest wall is moving a bit (there is effort) |
|
|
What are the effects of Obstructive Sleep Apnea on the heart?
|
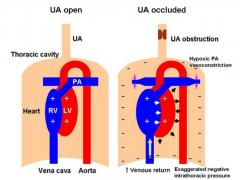
- Increased negative intrathoracic pressure from trying to inhale but no air coming in d/t obstruction
- Increases LV transmural pressure and LV afterload - Also increases venous return, increasing RV preload - Hypoxia causes PA vasconstriction and pulmonary HTN - Leads to RV distension and leftward displacement of IV septum during diastole which impairs LV filling and diminishes LV preload and stroke volume |
|
|
What are the effects of Obstructive Sleep Apnea on sympathetic nerve activity?
|
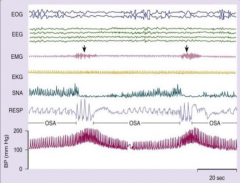
- Symp nerve activity (SNA) increases progressively during apnea because of activation of the peripheral and central chemoreflexes by hypoxia and hypercapnia
- Leads to vasoconstriction and surges in BP, which reaches peak during hyperventilation - SNA abruptly ceases at onset of breathing - Also have increased muscle tone (EMG) toward end of apnea in relation to arousals from REM sleep |
|
|
What are the negative effects on the CV system of the hypoxia and consequential sympathetic activation?
|
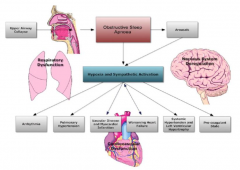
- Arrhythmias (A. Fib)
- Pulmonary HTN - Vascular disease and MI - Worsening heart failure - Systemic HTN and LV Hypertrophy - Pro-coagulant state |
|
Case: Patient is snoring at night, has history of diabetes, HTN, leg swelling. Wakes up in the night and has to sit up on edge of bed to catch his breath. Has to urinate 5-6x/night.
What is wrong? |
Central Sleep Apnea
- No air flow and no effort - Also Cheyne-Stokes breathing (crescendo-decrescendo pattern) |
|

What kind of breathing is this? What happens to CO2 levels?
|
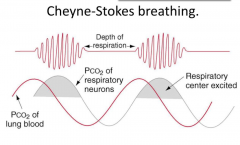
Cheyne-Stokes Breathing
- PCO2 of lung blood goes up and down (sine pattern) - PCO2 of respiratory neurons slightly behind - Overshoot and undershoot CO2 levels |
|
|
Case: 26 year old med student has been sleepy for many years. Prior to this study he completed a sleep diary confirming he was sleeping at least 8-9 hours every night.
What can we do next to evaluate his sleepiness? |
Multiple Sleep Latency Test - he may have narcolepsy or other problem
|
|
|
What does the mean sleep latency on MSLT tell you?
|
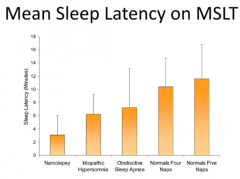
- < 3-6 minutes: narcolepsy
- 6-9 minutes: idiopathic hypersomnia - 7-13 minutes: obstructive sleep apnea - >10 minutes: normal |
|
|
How common is narcolepsy?
|
Affects 0.03%-0.1% of general population
|
|
|
What hormone is commonly missing in patients with narcolepsy?
|
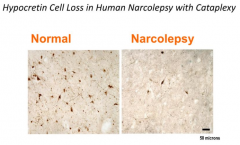
Orexin (aka hypocretin) - involved in controlling sleepiness, when you don't have this you are more likely to have narcolepsy
|
|
|
What genetic relationships are there with narcolepsy?
|
- Familial clustering occurs in about 10% of cases
- Most monozygotic twins are discordant |
|
|
What environmental factors are possibly involved in narcolepsy?
|
- Unknown antigen binding w/ HLA DQB1*0602
- Head trauma, virus, toxins - Sleep deprivation, change in sleep / wake cycle |
|
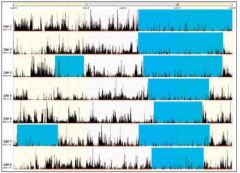
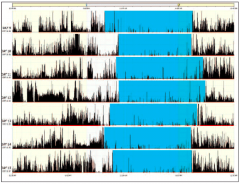
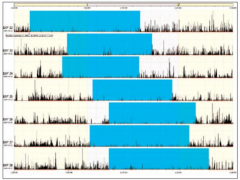
What does these actigraphy results show?
|
College student? Going to bed at 4 am and waking up at noon and taking naps during the day
|
|
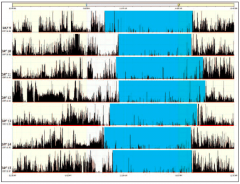
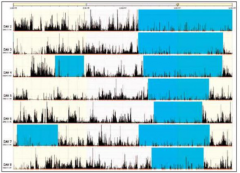
What does these actigraphy results show?
|
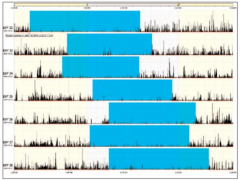
Marching through day, non-24 hour sleep
- Could be patient who is ocularly blind - Ocular nerve communicates w/ superchiasmatic nucleus to tell us when to be awake and asleep |
|
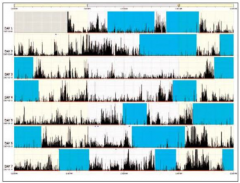
What does these actigraphy results show?
|
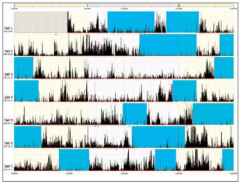
Chaos - 3rd shift sleep patterns are often all over the place
|
|
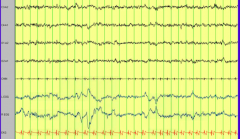
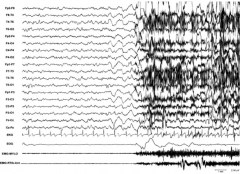
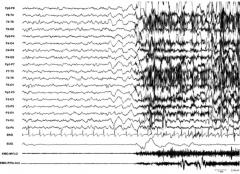
What do these results show?
|
REM sleep but limb leads are very active (lack of atonia) = REM behavior disorder
|
|
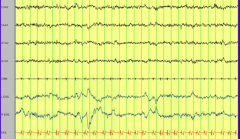
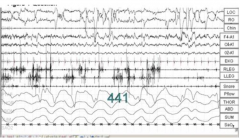
What do these results show?
|
Onset of Night Terror
- Spontaneous attack during stage 3 of NREM sleep - 2 seconds of diffuse hyper-synchronous high voltage delta wave arousal - Brief EEG delta discharge immediately preceding the clinical episode - Increased HR (shown from EKG) |
|
|
What does parasomnia mean?
|
Dissociated sleep states which are partial arousals during the transitions between wakefulness and NREM sleep, or wakefulness and REM sleep.
|
|
|
What happens during NREM parasomnias?
|
- Sleep walking
- Sleep talking - Sleep related eating - Confusional arousal - Night terrors |
|
|
What happens during REM parasomnias?
|
- Nightmares
- Sleep paralysis - REM behavior disorder |
|
|
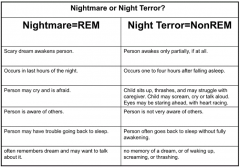
When do nightmares and night terrors occur?
|
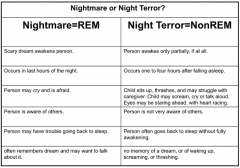
- Nightmare: REM
- Night Terror: NREM |
|
|
Do you awake from nightmares and night terrors?
|
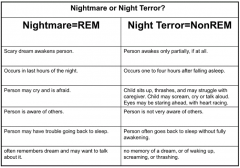
- Nightmare: REM, scary dream awakens person
- Night Terror: NREM, person awakes only partially, if it all |
|
|
When do nightmares and night terrors occur?
|
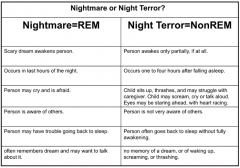
- Nightmare: REM, last hours of the night
- Night Terror: NREM, one to four hours after falling asleep |
|
|
What are the actions of someone experiencing a nightmare vs night terror?
|
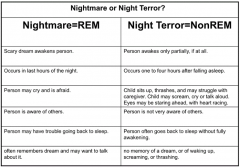
- Nightmare: REM, person may cry and is afraid
- Night Terror: NREM, child sits up, thrashes, and may struggle w/ caregiver, may scream, cry or talk aloud, eyes may be staring ahead w/ heart racing |
|
|
What is the awareness of others in nightmares and night terrors?
|
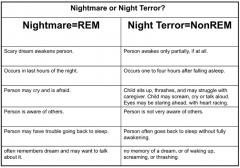
- Nightmare: REM, aware of others
- Night Terror: NREM, not very aware of others |
|
|
Do people go back to sleep after nightmares vs night terrors?
|
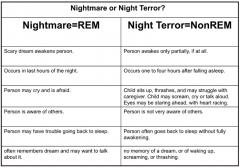
- Nightmare: REM, may have trouble going back to sleep
- Night Terror: often goes back to sleep w/o fully awakening |
|
|
What is the memory of nightmares vs night terrors?
|
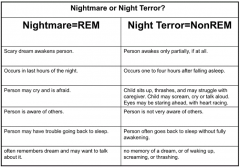
- Nightmare: REM, often remembers dream and may want to talk about it
- Night Terror: no memory of dream, or of waking up, screaming, or thrashing |
|
|
Nightmares:
- Type of sleep? - Awaken? - When? - Actions? - Awareness of others? - Ability to sleep after? - Memory? |
- REM
- Awakens them - Last 4 hours of night - May cry and is afraid - Aware of others - May have trouble falling back asleep - Often remembers dream and may want to talk about it |
|
|
Night terrors:
- Type of sleep? - Awaken? - When? - Actions? - Awareness of others? - Ability to sleep after? - Memory? |
- NREM
- If they awake, only partially if at all - After 1-4 hours of sleep - Sit up, thrash, struggle w/ caregiver, scream, cry, talk aloud, eyes may stare ahead w/ heart racing - Not aware of others - Go back to sleep w/o fully awakening - No memory of dream, waking up, screaming, or thrashing |
|
|
Which of the following conditions is bet evaluated w/ a polysomnogram?
- Nightmares - Obstructive sleep apnea - Restless leg syndrome - Delayed sleep phase syndrome |
Obstructive sleep apnea syndrome
|
|
|
How do you best evaluate Obstructive sleep apnea syndrome?
|
Polysomnogram
|
|
|
How do you best evaluate a REM behavior disorder?
|
Polysomnogram
|
|
|
If patient is going to bed at sundown, what syndrome do they have?
|
Advanced sleep phase syndrome
|