Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
|
identify grade 1/2 hypertensive retinopathy
|

1-2: moderate- severe retinal arteriole NARROWING
2: arteriovenous NICKING |
|
|
features of grade 3 hypertensive retinopathy
|
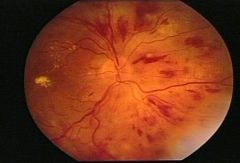
bilateral soft EXUDATES or flame-shaped HAEMORRHAGES
|
|
|
features of grade 4 hypertensive retinopathy
|
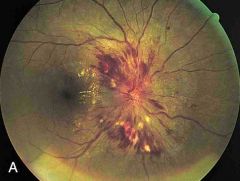
bilateral optic nerve PAPILLOEDEMA
|
|
|
5 types of end-organ damage
|
CHF
coronary artery disease - MI cerebrovascular disease- STROKE renal failure hypertensive retinopathy |
|
|
6 secondary causes for HTN
|
fibromuscular dysplasia
renal/ renovascular disease coarctation of aorta hyperaldersteronism Cushing's Phaeochromocytoma (adrenal medullar --> ⇧NA & adrenaline) |
|
|
epidemiology of coronary heart disease:
gender age culture status race |
men ♂
<60 western deprived BLACK men ♂ |
|
|
BMI ranges for overweight/ obese
|
25-30 = overweight
>30 = obese |
|
|
5 major food groups
|
fruit & veg
carbs dairy meat & fish (eggs & beans) fat/ sugar |
|
|
what defines high fat food
|
>20g per 100g
sat fat worse |
|
|
what defines high sugar foods
|
>15g per 100g
|
|
|
what's the daily salt recommendation and what defines high salt foods
|
6g/day
>1.5g per 100g |
|
|
the big 4's & little 4s - modifiable risk factors for CVD
|
big: - HTN, ⇧cholesterol, smoing, obesity
little: physical inactivity, alcohol, stress, deprivation |
|
|
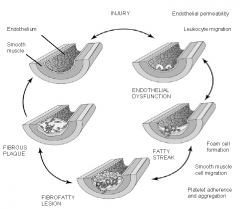
events in atherosclerosis developing
|
|
|
|
what 5 cinical effectsmanifest from an atherosclerotic plaque
|
impaired vision
TIAs/ strokes IHD: angina renal failure POAD (intermittent claudication) |
|
|
what 4 factors ↑ oxidative stress in arteries
|
↑LDL
↑BP DM smoking |
|
|
What are the role and course of macrophages in atherosclerosis
|

migrate through endothelial wall
take up oxidised LDL foam cells fatty streak |
|
|
normal ranges (mmol/L) for:
- cholesterol - triglycerides - LDL -HDL |
cholesterol: <6
triglycerides: <2 LDL: <4.4 HDL: >1 |
|
|
what's the mainstay of treatment for high cholesterol
action effects |
STATINS- comp inhib HMG-CoA reductase (cholesterol synthesis)
- ↓total & LDL - pleotrophic |
|
|
some clinical markers for dyslipidaemia / hyperlipidaemia
|
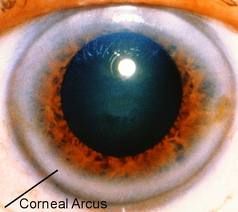
xanthelasma (eyes)
xanthomas (skin) corneal arcus (can be normal >50) |
|
|
normal BP range
target for high risk groups (who are these?) |
<140/90
<130/80: DM, renal disease |
|
|
pharamacological management HTN
- <55 - ≥55 |
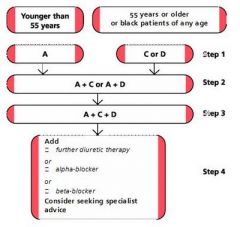
ACE- lisinopril, ARB- losartan, CCB- nicorandil, thiazide- bendrfluazide
|
|
|
what 4 factors contribute to metabolic syndrome
|
obese
↑ waist circumference (M>102, F>88) ↑triglycerides ↑fasting glucose |
|
|
what link does ↑CRP have in CVD
|
linked with MI & ↑TC:HDL
|
|
|
how can you calculate an individuals risk for CVD
|
ASSIGN score
|
|
|
3 medications and 2 targets for established atherosclerosis
|
aspirin (anti-platelet)
statin BBs (atenolol, metropolol) ACEI (lisinopril) exercise smoking cessation |
|
|
6 secondary causes of HTN
|
fibromuscular dysplasia
renal/ renovascular disease coarctation of aorta hyperaldersteronism Cushing's Phaeochromocytoma (adrenal medullar --> ⇧NA & adrenaline) |
|
|
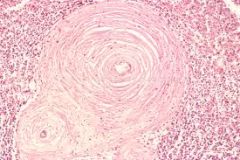
what BP rage defines MALIGNANT/ accelerated HTN - needs URGENT treatment
pathological hallmark |
papilloedema of the optic nerve (grade 4 HTN retinopathy)
>180/110 FIBRINOID NECROSIS |
|
|
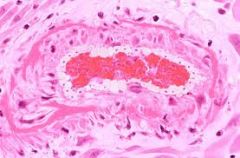
3 pathological changes of blood vessels in HTN
|
microvascular injury- scarring from fibrosis
medial thickening hyaline athersclerosis (plasma proteins in walls) |
|
|
4 arterial pathological consequences of atherosclerosis
|
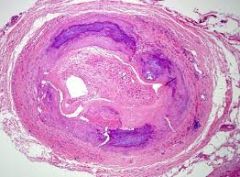
artery stenosis
arterial thrombosis/ embolism aneurysm dissection |
|
|
how does arterial thrombosis occur
|
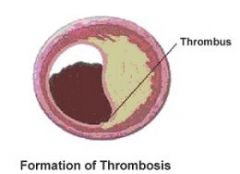
thin fibrous plaque ruptures
collagen release stimulates COAGULATION cascade |
|
|
what's an aneurysm
|
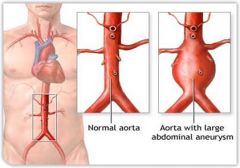
abnormal DILATATION & reduced elasticity of artery wall
media weakened by atherosclerosis ---> RUPTURE! |
|
|
what's a dissection
|
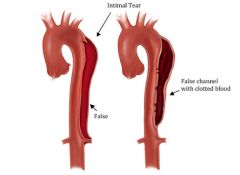
media SPLIT --> sudden TEARING pain
|
|
|
what's LVH, why and how is it dysfunctional (3)
|
fibrous, collagenous = stiff & less complaint
- DIASTOLIC dysfunction - DISARRAY of electric impulse - arrhythmias - thicker= reduced PERFUSION |
|
|
if repeated clinic BP is >140/90 what do you do?
how is this done? |
offer ABPM to confirm HTN diagnosis
- 2 per hr during WAKING hrs (average of 14) |
|
|
alternative to ABPM
how is this taken |
HBPM
- 2 consecutive measurements >1min apart - seated - BD (morn/ eve) - 7days - discard 1st measurement |
|
|
What 4 ways do you assess target end organ damage in pt's with HTN?
|
- proteinuria (albumin:creatinine), haematuria
- Bloods: glucose, U&Es, eGFR, cholesterol - hypertensive retinopathy - ECG |
|
|
ABPM/ HBPM target
|
135/85
|
|
|
what's classified as stage 2 and severe/ accelerated HTN
|
stage 2- 160/100
severe- S>180 or D>110 |
|
|
is adding drugs or increasing dose of monotherapy more effective in treating HTN
|
adding = synergistic
|
|
|
who's offered CCBs as first line treatment of HTN
|
≥55
BLACK person of African/ Caribbean origin - any age |
|
|
What 2 reasons would you give a1-blocker to treat HTN
|
?after step 4 (A+C+D)
or benign prostatic hyperplasia |
|
|
at what BP do you treat ALL pt's
|
≥160/100
|
|
|
when would you treat a pt with BP ≥130/80
|
DM or CKD
Target end organ damage: - HTN retinopathy - stroke/ TIAs - HF/ CHD/ LVH - POAD |
|
|
HTN below what age is likely to be secondary HTN
|
<40yrs
|
|
|
which HTN range do you treat IMMEDIATELY
|
malignant/ accelerated (w/ papilloedema) > 180/110
|