Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
112 Cards in this Set
- Front
- Back
|
|
|
|
|
|
|
|
|
|
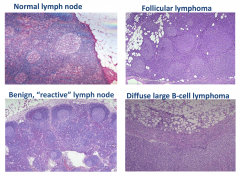
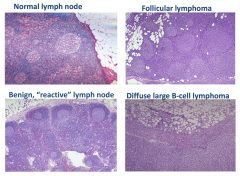
Normal Lymph Nodes
|

|
|
|
Causes of patient's lymphadenopathy
|
Can be inflammatory (like infection), reactive (like autoimmune), or malignancy
|
|
|
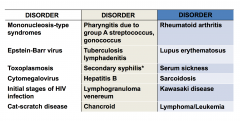
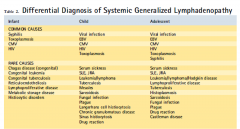
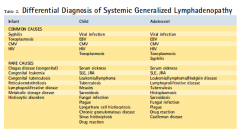
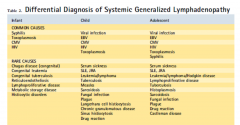
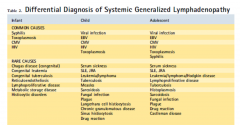
Some causes of lymphadenopathy
|
|
|
|
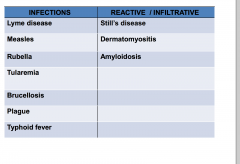
Less common causes of lymphadenopathy
|
|
|
|
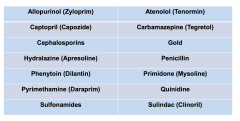
Medications that may cause lymphadenopathy
|
|
|
|
|
|
|
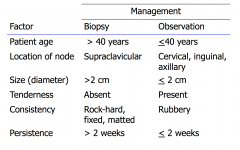
Factors that influence the management of lymphadenopathy
|
|
|
|
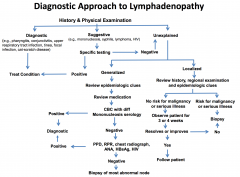
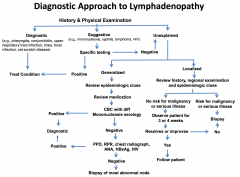
Diagnostic considerations for lymphadenopathy
|
- Squamous cell cancer of the head and neck
- Metastatic cancer --- lung/esophageal/gastrointestinal/melanoma/others - Lymphoid malignancy -- lymphoma/leukemia |
|
|
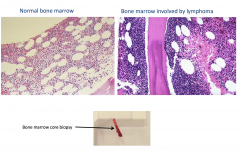
Pathologic diagnosis of cervical lymph node biopsy.
What would sections show? |
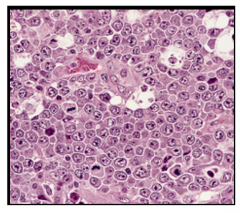
Sheets of tumor cells characterized by lymphocytes with large cell size, round to irregular nuclear contours, vesicular chromatin, multiple distinct eosinophilic nucleoi, and moderate amounts of eosinophilic cytoplasm.
|
|
|
Flow cytometry of cervical lymph node biopsy
|
Reveals monoclonal B-cell population of large size which was CD10(+) and lambda light chain restricted
|
|
|
Immunohistochemical stains associated with tumor cells (lymph nodes)
|
Strong positivity for CD20 and BCL-2. The cyclin-D1 stain is neg in tumor cells. A Ki-67 stain shows proliferative index of approx 80% in the tumor cells
Associated with diffuse large B-cell lymphoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
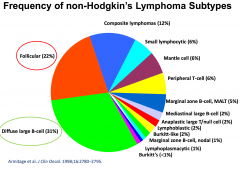
Follicular Lymphoma
|
bcl-2 staining
|
|
|
Most common reason for enlarged spleen (entire world)
|
Malaria
|
|
|
Most common reason for enlarged spleen (US)
|
lymphadenopathy
|
|
|
|
|
|
|
|
|
|
|
|
Presenting symptoms of non-Hodgkin's Lymphoma
|
- Painless enlargement of lymph nodes
- Presence of "B symptoms" -- fevers -- night sweats -- weight loss - Unexplained pain, particularly back / abdominal - Cough - Swelling, especially in ankles or legs - Severe fatigue - Loss of appetite - Less common, but serious complications: --- low blood counts, kidney failure, liver failure, neurological symptoms (brain or spinal cord), blood clots, bowel obstruction, high calcium levels. |
|
|
Non-Hodgkin's Lymphoma: Clinical Features
|
Lymphadenopathy
Splenomegaly Hepatomegaly Tissue Infiltration "B" symptoms CBC abnormalities |
|
|
Staging Work-up of Non-hodgkin's lymphoma
|
Physical exam
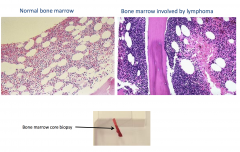
CT scans of chest, abdomen, pelvis PET scan Bone marrow biopsy +/- Lab - CBC, LFTs, Basic chemistries, uric acid, LDH, beta-2 microglobulin and serum protein electrophoresis Infectious agents - HIV, Hep C, H. pylori |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment for Diffuse Large B-cell lymphadenopathy
|
Chemo-immunotherapy:
Cyclophosphamide Doxorubicin Vincristine Prednisone Rituximab R-CHOP (or CHOP-R) Administered every six weeks x 6 cycles |
|
|
Of the drugs in the R-CHOP regimen, which of the following are most likely to put the patient at risk for both hemorrhagic cystitis and dilated cardiomyopathy?
|
Cyclophosphamide, doxorubicin
|
|
|
Adverse effects of Doxorubicin
|
• Cardiotoxicity
• Myelosuppression • GI, alopecia |
|
|
Adverse effects of vincristine
|
• Peripheral neuropathy,
neurotoxicity • Alopecia, constipation |
|
|
Adverse effects of cyclophosphamide
|
• GI, alopecia
• Myelosuppression • Hemorrhagic cystitis |
|
|
Adverse effects of Rituximab
|
• Infusion reactions
• Fever, chills • Lymphopenia • Tumor lysis syndrome |
|
|
Adverse effects of Prednisone
|
Na+
/water retention, K+ depletion • Incr. appetite, weight gain • Elevated glucose • Hypertension • Increased infection risk |
|
|
Of the R-CHOP drugs, which is a pro-drug?
|
Cyclophosphamide
|
|
|
Cyclophosphamide --CYP450s---->
|
phosphoramide mustard + acrolein
|
|
|
How is this activation related to hemorrhagic
cystitis? |
• Acrolein is a highly reactive aldehyde -- associated
with sterile hemorrhagic cystitis |
|
|
Is there an agent to prevent/lessen this cystitis?
|
• 2-mercaptoethanesulfonate (MESNA)
• scavenges acrolein |
|
|
mechanisms of action associated with doxorubicin
|
Binds DNA/topoisomerase II complex
Causes lipid peroxidation and free radical damage Intercalates in DNA, distorts DNA helix |
|
|
Mechanism of action of cyclophosphamide
|
Once activated, phosphoramide mustard is an alkylating agent
• Alkylates DNA causing strand breaks, adducts, crosslinks |
|
|
Mechanism of action of rituximab
|
• Monoclonal Ab that binds to CD20 on cell surface of B lymphocytes (>90% of non-Hodgkins lymphomas)
• Blocks cell cycle initiation, differentiation • Bound antibody recruits immune cells --> cell lysis |
|
|
Mechanism of action of vincristine
|
Binds tubulin, blocks assembly of microtubules, mitotic spindle
|
|
|
Mechanism of action of prednisone
|
Binds tubulin, blocks assembly of microtubules, mitotic spindle
|
|
|
Prognostic factors of outcome in Diffuse Large Cell Lymphoma
|
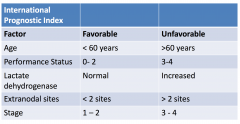
Think "APLES"
|
|
|
Curative Therapy for a patient with recurrence of their lymphoma
|
• High-dose chemotherapy followed by autologous stem cell transplantation. Try to shrink the tumor, but with increased dose you get increased toxicity to tissues.
• This treatment is effective if there is good response to a second line of chemotherapy first. • He received three cycles of chemotherapy with: • Rituxan, Ifosfamide, Carboplatin, and Etoposide (RICE) |
|
|
Mechanism of action of etoposide
|
Irreversibly binds/stabilizes DNA-topoisomerase II complexes
|
|
|
Mechanism of action of Carboplatin
|
• Platinum coordination complex
that causes DNA crosslinks • Cisplatin analog • Intrastrand crosslinks |
|
|
Mechanism of action of Ifosfamide
|
• Cyclophosphamide analog
• Ifosfamide ---> nitrogen mustard + acrolein |
|
|
What drugs are associated with myelosuppression?
|
Ifosfamide
Carboplatin Etoposide |
|
|
Adverse effects of Ifosfamide
|
• Like cyclophosphamide (GI,
alopecia, myelosuppression) • Additional: nephrotoxicity, neurotoxicity (encephalopathy) - related to chloroacetaldehyde metabolite |
|
|
Adverse effects of carboplatin
|
• Cisplatin analog
• Myelosuppression, GI upset • Less nephrotoxicity, neurotoxicity, ototoxicity than cisplatin |
|
|
Adverse effects of etoposide
|
• Myelosuppression, alopecia
• GI upset (mild-moderate) • Allergic reactions (low %) |
|
|
Patients having a neck mass should have
|
An excisional biopsy
|
|
|
Autoimmune disease and NHL (Non-hodgkin's Lymphoma)
|
Life-time risk of NHL is 5% in Sjogren Syndrome
Occurs at a mean of ~7 years after SS diagnosis Generally low-grade lymphoma (MALT) |
|
|
Lymphadenopathy
|
Abnormality in size or consistency of a lymph node
|
|
|
Enlargement of lymph node may be due to?
|
Cellular hyperplasia, cellular infiltration, or reactive tissue edema
A thorough history and a comprehensive physical exam are essential in evaluating pediatric lymphadenopathy |
|
|
Initial diagnostic impression of lymphadenopathy in kids will be more refined when considering what additional details?
|
- Patient age
- Size of nodules - Location of nodes - Distribution (localized or generalized) - Quality of nodes - Time course of lymphadenopathy and associated symptoms |
|
|
Volume of lymph tissue increases with?
|
Age and the overall maturity of the immune system as aggregate antigenic exposure increases
|
|
|
Newborns and lymph nodes
|
In general, new borns should not have palpable lymph nodes, though they may have congenital lesions that could mimic a node
|
|
|
Enlarged node in a neonate
|
Should prompt consideration of congenital infections such as toxoplasmosis or CMV
|
|
|
Older infants and younger children - lymph nodes
|
They will frequently have "shotty" nodes in the head and neck, axillary, or inguinal regions, even when otherwise healthy
|
|
|
School-aged children and adolescents
|
Less frequently have palpable nodes
|
|
|
Nodes and age
|
Age determines exposure and risk
|
|
|
Pre-school and early school-aged children
|
Constantly bombarded with viruses
Risk of malignancy varies with age (hodgkin lymphoma is uncommon for under 10) Teenagers can get communicable causes of inguinal adenopathy |
|
|
Size of lymph nodes
|
A size that could be considered pathologic in one anatomic region may be physiologic in another
In general, head and neck region nodes should be subcentimeter, inguinal nodes should be less than 1.5 cm, and most other regions should be less than half a centimeter |
|
|
Lymph
|
An important component of the immune system
Lymphatic system is an open circulatory system responsible for circulating lymph through lymphatic vessels, nodes, the spleen, and other lymphoid tissues Understanding drainage pathways is key to developing a differential diagnosis |
|
|
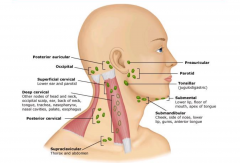
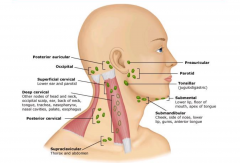
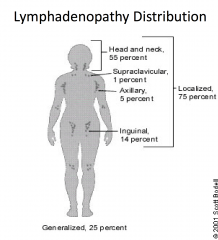
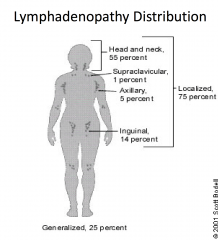
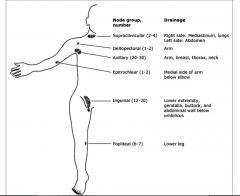
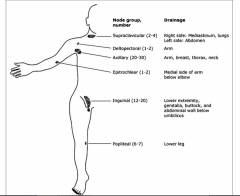
Lymphatic Drainage of the body
|
|
|
|
|
|
|
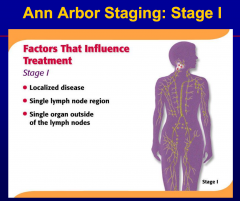
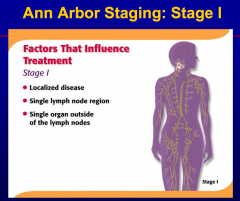
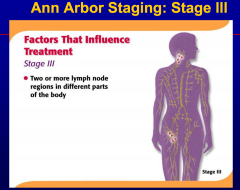
Involvement of one nodal group or contiguous
nodal groups constitutes |
localized or regional adenopathy.
|
|
|
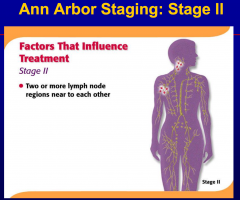
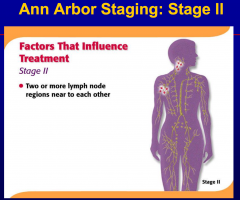
Involvement of two or more non-contiguous
nodal groups constitutes |
generalized adenopathy
|
|
|
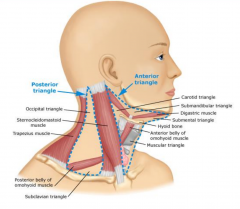
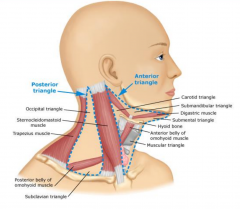
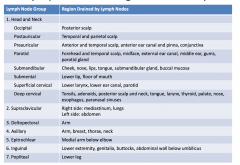
Sites of Local Lymphadenopathy and Associate Diseases
|
1. Cervical
2. Anterior auricular 3. Supraclavicular 4. Epitrochlear 5. Inguinal 6. Hilar (not palpable, found on chest radiograph or CT 7. Axillary 8. Abdominal |
|
|
|
|
|
Quality of lymph nodes
|
- Quality of nodes provides important information
- Normal nodes are soft, compressible, and freely mobile - Tenderness is most often an indication of infection and may be associated with overlying skin changes such as redness or swelling |
|
|
Hard nodes are indicative of
|
fibrosis secondary to cancer or previous infection
|
|
|
Firm and rubbery nodes are indicative of ?
|
Lymphomatous infiltration
Fixing and matting are signs of infiltrative changes |
|
|
Time course of symptom development
|
Can help differentiate among causes of lymphadenopathy
- acute enlargements are more likely to be infectious - adenopathy of over four weeks duration is considered chronic and is more likely to be related to malignancy for chronic infections |
|
|
Acute Unilateral Cervical Lymphadenitis
|
Cervical adenopathy is an incredibly common presentation in children and deserves special consideration
|
|
|
Acute bilateral (reactive) lymphadenopathy
|
Lymphoid hyperplasia usually secondary to a head and neck infection. Typical pathogens include:
- RSV, adenovirus, influenza, other viral upper respiratory tract pathogens - occasionally, EBV and CMV can cause mononucleosis that presents with bilateral (typically posterior) cervical adenopathy |
|
|
Pathophysiology of acute unilateral cervical lymphadenitis
|
Frequently bacterial in nature, with either Staph aureus or group A streptococcal species being implicated
Other important pathogens include oral flora, including anaerobes, from poor dentition Presence of bacterial species in a lymph node incites a localized inflammatory reaction |
|
|
Pathophysiology of chronic cervical lymphadenopathy
|
Frequently infectious in children
-- TB -- Atypical mycobacteria -- Bartonella henselae infecton (cat scratch) |
|
|
Non-infectious etiologies of cervical lymphadenopathy
|
- Malignant
- Immunologic - Endocrinologic - Misc |
|
|
Treatment of infectious cervical adenopathy
|
Treatment should be based upon microbiologic testing whenever possible
Often times, empiric treatment will have to suffice and should be directed against the most likely pathogens Treatment with glucocorticoids should be avoided at all costs, unless life-threatening airway compromise is present. |
|
|
Acute unilateral cervical lymphadenitis: Most common bacterial pathogens
|
Staph, strep
|
|
|
Drug treatments for strep, mssa
|
– Cephalexin, clindamycin, amoxicillin+clavulanate
– Macrolides (e.g. erythromycin) – MSSA: oxacillin, dicloxacillin, cloxacillin |
|
|
Drugs for community-acquired MRSA
|
- Linezolid, clindamycin (also covers Strep.)
- Doxycycline; TMP/SMX (not good for strep) |
|
|
Subacute or chronic lymphadenitis due to Cat-scratch disease
|
Bartonella henselae
Azithromycin: note of caution - if you are considering empiric treatment, get a PPD first! Others: cipro, rifampin, TMP/SMX Generally resistant to beta-lactams |
|
|
Cervical lymphadenitis due to atypical mycobacteria
|
MAC (Mycobacterium avium-intracellulare)
• Clarithromycin, rifabutin • Others: ethambutol, amikacin, isoniazid |
|
|
Regional Lymphadenopathy
|
• Infectious etiologies in the drainage area
should be the first consideration • Consider further studies and diagnoses if the lymphadenopathy fails to resolve with observation or empiric treatment • Non-infectious considerations: – Kawasaki disease – Malignancy – Sarcoidosis |
|
|
|
|

|

|
|

|

|
|
|
|
|
|
|
|
|
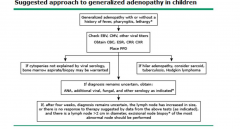
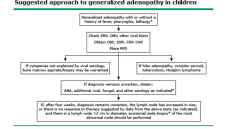
Empiric treatment of lymphadenopathy should
take into consideration |
the risk of malignancy, tuberculosis, and atypical mycobacterial infection
|
|
A 30-year-old female presents with tender
cervical lymphadenopathy. She has had low-grade fever on and off for a few weeks. A biopsy performed shows a normal lymph node with multiple germinal centers. Many macrophages containing debris from ingested lymphocytes are present (tingible body macrophages). |
Benign reactive lymphadenitis
|
|
A 25-year-old woman had recurrent low grade fever
and cervical lymphadenopathy. Photomicrographs of a lymph node biopsy (Figure G6.7) showed fibrosis, atypical mononuclear cells in lacunae, characteristic multinuclear cells, and some eosinophils. |
Hodgkin Disease
|
|
A 65-year-old man is evaluated for left
upper-quadrant abdominal discomfort, early satiety, and recent weight loss (5% loss of baseline weight in 6 months). Remainder of history is non-contributory. PE: Lymphadenopathy is absent, but the spleen is palpable to the level of the umbilicus. Remainder of the PE is unremarkable. WBC 18,000/μL with 60% lymphocytes, • CT scan: Splenomegaly and multiple lymph nodes <1 cm are visible in the mesenteric and retroperitoneal lymph node regions. • A marginal zone B-cell lymphoma, an indolent low-grade lymphoma, is identified by flow cytometry. |
Hep C
|
|
|
Splenomegaly and circulating lymphocytes:
|
MZL
(aka splenic lymphoma with villous lymphocytes) • Associated with hepatitis C virus • Treatment of hepatitis C may produce remission • Splenectomy is an option if hepatitis C is negative |
|
|
EBV
|
African Burkitt’s, extranodal NK-T-cell nasal
type, and lymphomatoid granulomatosis NHL |
|
|
H. pylori
|
Gastric MALT
|
|
|
HTLV-1
|
Adult T-cell lymphoma/leukemia
|
|
|
Hep B
|
not associated with any lymphoma
|
|
A patient with relapsing non-Hodgkin’s Lymphoma
presents with weight gain, foot ulcers, vision problems, elevated blood glucose, oral Candida, and recent onset of drastic mood changes. |
Adverse effects of prednisone
|
|
A 35-year-old homeless man presents to the emergency room complaining for an intense itch on his head. On examination, you note small ovoid whitish structures attached to his hair. There are scalp excoriation and enlarged posterior cervical lymph nodes.
|
Pediculus humanus
|
|
|
Bartonella henselae
|
|
|
A 32-year-old male is brought to you in the ER. He is running a
temperature, has not passed urine for the last 48 hours, and complains of pain in the flank. He had an upper respiratory tract infection about 10 days back and was put on a penicillin-group of drug. His fever had subsided with the medicine only to return 2 days back. He was perfectly well before the respiratory tract infection.Clinical examination reveals a febrile (102 F), normotensive person with erythematous maculopapular rash over his trunk and proximal extremities. Urinalysis reveals: • Proteinuria - moderate • Hematuria • Urine sediment - RBC + • WBC + • WBC casts + • Serum creatinine - 3.6mg/dl • Serum BUN - 40mg/dl You suspect acute renal failure. |
Acute interstitial nephritis
|
|
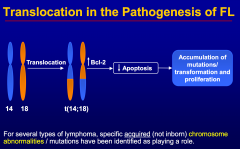
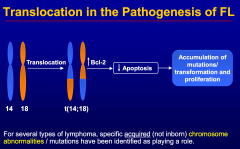
A patient presents with cervical lymphadenopathy. Biopsy demonstrates a follicular lymphoma.
|
bcl-2 activation
|
|
|
Reed-Sternberg Cells
|