![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
331 Cards in this Set
- Front
- Back
|
Number one cause of preventable morbidity and mortality in the U.S.? |
Smoking |
|
|
Bad effects of smoking? |
- Atherosclerosis - Cancer - COPD |
|
|
Number two cause of preventable morbidity and mortality in the U.S.? |
Alcohol |
|
|
Bad effects of alcohol? |
- >1/2 of accidental and intentional deaths involve alcohol - Number one cause of preventable mental retardation (fetal alcohol syndrome) - Cancer / cirrhosis - Potentially fatal in withdrawal - Wernicke encephalopathy / Korsakoff dementia |
|
|
Classic lab finding associated with alcoholic hepatitis? |
AST:ALT > 2:1 (although both may be elevated) |
|
|
Vitamin for reproductive age women? Why? |
Folate - prevent neural tube defects |
|
|
Vitamin needed in pernicious anemia? Why? |
B12 - prevent permanent neurologic deficits |
|
|
Vitamin deficiency associated with isoniazid? |
B6 - Pyridoxine |
|
|
Treatment for Wernicke encephalopathy in alcoholics? Why? |
Thiamine - prevent Korsakoff dementia |
|
|
Most common cause of anemia? |
Iron deficiency - menstrual loss in reproductive age women and cancer in men / menopausal women (if no other cause is obvious) |
|
|
Which vitamin is a known teratogen?
|
Vitamin A (eg, acne treatment isotretinoin) |
|
|
What is involved in roughly one half of deaths in the U.S.? |
Atherosclerosis |
|
|
Potential complications of atherosclerosis? |
- MI - Heart failure - Stroke - Gangrene |
|
|
Primary risk factors for atherosclerosis? |
- Age/sex - Family history - Cigarette smoking - HTN - DM - High LDL - Low HDL |
|
|
Potential complications of DM? |
- Atherosclerosis - Retinopathy - Nephropathy - Peripheral vascular disease - Peripheral neuropathy (sensory and autonomic) - Increased infection incidence |
|
|
Leading cause of blindness in U.S.? |
Diabetic retinopathy |
|
|
Leading cause of ESRD in U.S.? |
Diabetic nephropathy |
|
|
Leading cause of limb amputation in U.S.? |
Peripheral vascular disease secondary to DM |
|
|
Neural pathways affected by diabetic peripheral neuropathy? |
Sensory, Autonomic |
|
|
Manifestations of severe HTN / hypertensive emergency? |
- Headaches - Dizziness - Blurry vision - Papilledema - Cerebral edema - AMS - Seizures - Intracerebral hemorrhage (classically in basal ganglia) - Renal failure / azotemia - Angina - MI - Heart failure |
|
|
Classic location of intracerebral hemorrhage in patients with severe HTN / hypertensive emergency? |
Basal ganglia |
|
|
Which diseases, when mild, can be treated with lifestyle modifications (diet, exercise, weight loss, cessation of alcohol/tobacco)? |
- HTN
- HLD - DM - GERD - Insomnia - Obesity - Sleep apnea |
|
|
Exogenous causes of hyponatremia? |
- Oxytocin - Surgery - Narcotics - Inappropriate IV fluids - Diuretics - Anti-epileptics |
|
|
EKG finding with hyperkalemia? |
Tall, tented T waves |
|
|
EKG finding with hypokalemia? |
Loss of T waves / T-wave flattening, U waves |
|
|
EKG finding with hypocalcemia? |
QT prolongation |
|
|
EKG finding with hypercalcemia? |
QT shortening |
|
|
Treatment of shock? |
- O2 - IV line --> fluid bolus (1L NS or LR) if no signs of CHF (e.g., bibasilar rales) - Monitors: pulse ox, ECG, frequent vital signs |
|
|
Virchow's triad? |
- Endothelial damage - Venous stasis - Hypercoagulable state |
|
|
Causes of endothelial damage that may lead to DVT (component of Virchow's triad)? |
- Surgery - Trauma |
|
|
Causes of venous stasis that may lead to DVT (component of Virchow's triad)? |
- Immobilization - Surgery - Severe heart failure |
|
|
Causes of hyper-coagulable state that may lead to DVT (component of Virchow's triad)? |
- Malignancy - Birth control pills - Pregnancy - Lupus anticoagulant - Inherited deficiencies |
|
|
Therapy components for CHF? |
- Diuretics (eg, furosemide) - ACE-Inhibitors - Beta-blockers (for stable patients) - Treat HLD if applicable - Treat smoking addiction if applicable |
|
|
What is Cor Pulmonale? |
Right sided heart enlargement, hypertrophy, or failure caused by primary lung disease (usually COPD)
|
|
|
Most common cause of R-sided heart failure? |
L-sided heart failure (not for pulmonate) |
|
|
What should you check in patients presenting with Atrial Fibrillation? |
Underlying cause - TSH, electrolytes, echo |
|
|
Main management issues of Atrial Fibrillation? |
- Ventricular rate - if needed, slow rate with meds - Atrial clot formation / embolic disease - consider anticoagulation with warfarin |
|
|
What conditions are treated with immediate defibrillation? |
- Ventricular fibrillation - Pulseless ventricular tachycardia |
|
|
How do you treat ventricular fibrillation? |
- Immediate defibrillation - Followed by epinephrine, vasopressin, amiodarone, and lidocaine |
|
|
How do you treat pulseless ventricular tachycardia? |
- Immediate defibrillation - Followed by epinephrine, vasopressin, amiodarone, and lidocaine |
|
|
How do you treat ventricular tachycardia with a pulse? |
Amiodarone and synchronized cardioversion |
|
|
What value do you use to distinguish obstructive vs restrictive lung disease? |
FEV1/FVC ratio - Low in Obstructive pathology - Normal in Restrictive pathology |
|
|
Most common type of esophageal cancer? |
Adenocarcinoma |
|
|
Risk factors for esophageal adenocarcinoma? |
- GERD - Barrett esophagus |
|
|
Second most common type of esophageal cancer? |
Squamous cell carcinoma |
|
|
Risk factors for esophageal squamous cell carcinoma? |
- Smoking - Alcohol abuse |
|
|
Management of gastric ulcers? |
Biopsy, or follow to resolution to exclude malignancy |
|
|
How do you best distinguish upper from lower GI bleeding? |
Nasogastric tube aspirate for blood (although bright red blood via mouth or anus is a fairly reliable sign of a nearby bleeding source) |
|
|
One of the most common causes of GI complaints? |
Irritable Bowel Syndrome |
|
|
How do you diagnose Irritable Bowel Syndrome? |
Physical and diagnostic studies are negative - diagnosis of exclusion |
|
|
Crohn's Disease vs Ulcerative Colitis: place of origin? |
- CD: distal ileium, proximal colon - UC: rectum |
|
|
Crohn's Disease vs Ulcerative Colitis: thickness of pathology? |
- CD: transmural - UC: mucosa / submucosa only |
|
|
Crohn's Disease vs Ulcerative Colitis: progression? |
- CD: irregular (skip lesions) - UC: proximal, continuous from rectum, no skipped areas |
|
|
Crohn's Disease vs Ulcerative Colitis: bowel habit changes? |
- CD: obstruction, abdominal pain - UC: bloody diarrhea |
|
|
Crohn's Disease vs Ulcerative Colitis: classic lesions? |
- CD: fistulas / abscesses, cobblestoning, string sign on barium enema - UC: pseudopolyps, lead pipe colon on barium x-ray, toxic megacolon |
|
|
Crohn's Disease vs Ulcerative Colitis: colon cancer risk? |
- CD: slightly increased - UC: markedly increased |
|
|
Crohn's Disease vs Ulcerative Colitis: surgery? |
- CD: no (may make worse) - UC: yes (proctocolectomy with illegal anastomosis) |
|
|
Distinguishing causes of viral hepatitis during acute stage? |
All forms present similarly - need serology testing and history to distinguish |
|
|
Forms of viral hepatitis that are transmitted parenterally? |
B, C, and D |
|
|
Potential complications of hepatitis B, C, or D? |
- Chronic infection - Cirrhosis - Hepatocellular carcinoma |
|
|
Most common known genetic disease in white people? |
Hereditary hemochromatosis |
|
|
Initial symptoms of hereditary hemochromatosis? |
- Fatigue - Impotence - Hepatomegaly |
|
|
Screening for hereditary hemochromatosis? |
- Transferrin saturation test (serum iron / TIBC) - Ferritin level |
|
|
Treatment for hereditary hemochromatosis? |
Phlebotomy after confirming diagnosis with genetic testing and liver biopsy |
|
|
Sequelae of liver failure? |
- Coagulopathy (cannot be fixed with vitamin K) - Jaundice - Hyperbilirubinemia - Hypoalbuminemia - Ascites - Portal HTN - Hyperammonemia / encephalopathy - Disseminated intravascular coagulation |
|
|
Common causes of pancreatitis? |
- Alcohol
- Gallstones |
|
|
Signs/symptoms of pancreatitis? |
- Abdominal pain - Nausea/vomiting - Elevated amylase / lipase |
|
|
Treatment for pancreatitis? |
- Supportive care - Pain control |
|
|
Potential complications of pancreatitis? |
- Pseudocyst formation - Infection / abscess - Adult respiratory distress syndrome |
|
|
Most common cause of jaundice / hyperbilirubinemia in neonates? Treatment? |
Physiologic - monitor and follow-up lab tests are needed |
|
|
Is jaundice at birth ever ok? |
No - always pathologic |
|
|
Examples of primary endocrine disturbances? |
- Graves - Hashimoto - Addison disease |
|
|
What is wrong in primary endocrine disturbances? |
Gland malfunctions but the pituitary or another gland and the CNS respond appropriately |
|
|
What is wrong in secondary endocrine disturbances? |
Gland itself is doing what it is told to do by other controlling forces (e.g., pituitary gland, hypothalamus, tumor, disease) - they are the problem, not the gland |
|
|
Examples of secondary endocrine disturbances? |
- ACTH-secreting lung carcinoma - Heart failure induced hyperreninemia - Renal failure induced hyperparathyroidism |
|
|
Corticosteroid side effects? |
- Weight gain - Easy bruising - Acne - Hirsutism - Emotional lability - Depression - Psychosis - Menstrual changes - Sexual dysfunction - Insomnia - Memory loss - Buffalo hump - Truncal and central obesity with wasting of extremities - Round plethoric facies - Purplish skin striae - Weakness (especially proximal muscles) - HTN - Peripheral edema - Poor wound healing - Glucose intolerance or diabetes - Osteoporosis - Hypokalemic metabolic alkalosis (resulting from mineralocorticoid effect of certain corticosteroids) - Growth may be stunted in children |
|
|
What electrolyte/metabolic derangement can occur with corticosteroids? Why? |
Hypokalemic Metabolic Alkalosis - due to mineralocorticoid effects of certain corticosteroids |
|
|
Most common cause of arthritis? |
Osteoarthritis (>75% of cases) |
|
|
Findings suggestive of osteoarthritis? |
- Joint is not hot or swollen typically - Arthrocentesis does not have significant findings |
|
|
Overall highest types of cancer in males? |
1. Prostate 2. Lung 3. Colon |
|
|
Overall highest types of cancer in females? |
1. Breast 2. Lung 3. Colon |
|
|
Overall cancer with highest mortality in males? |
1. Lung 2. Prostate 3. Colon |
|
|
Overall cancer with highest mortality in females? |
1. Lung 2. Breast 3. Colon |
|
|
Sequelae of lung cancer? |
- Hemoptysis - Horner syndrome - Superior vena cava syndrome - Phrenic nerve involvement / diaphragmatic paralysis - Hoarseness from recurrent laryngeal nerve involvement - Paraneoplastic syndromes |
|
|
Types of paraneoplastic syndromes associated with lung cancer? |
- Cushing syndrome - Syndrome of Inappropriate secretion of ADH (SIADH) - Hypercalcemia - Eaton-Lambert Syndrome |
|
|
Term for loss of peripheral vision in both eyes? |
Bitemporal hemianopsia |
|
|
Cause of bitemporal hemianopsia? Management? |
Space occupying lesion pushing on the optic chasm (classically a pituitary tumor) until proven otherwise; order a CT or MRI of the brain
|
|
|
Potential risks and side effects of estrogen therapy (e.g., contraception or post-menopausal hormone replacement)? |
- Endometrial cancer - Hepatic adenomas - Glucose intolerance / diabetes - DVT - Stroke - Cholelithiasis - HTN - Endometrial bleeding - Depression - Weight gain - Nausea/vomiting - Headache - Drug-drug interactions - Teratogenesis - Aggravation of pre-existing uterine leiomyomas (fibroids), breast fibroadenomas, migraines, and epilepsy |
|
|
Specific potential risks and side effects of combined estrogen / progesterone therapy (e.g., contraception or post-menopausal hormone replacement)? |
- Coronary artery disease - Breast cancer |
|
|
Characteristics of a mole that make you suspicious for malignant transformation? |
- Asymmetry - Borders (irregular) - Color (change in color or multiple colors) - Diameter (bigger the lesion, the more likely it is malignant) - Evolving over time |
|
|
What should you do for a mole with concerning ABCDE characteristics or for a mole that starts to itch or bleed? |
Excisional biopsy |
|
|
Bronchiolitis vs. Croup vs. Epiglottitis: child's age? |
- Bronchiolitis: 0-18 months - Croup: 1-2 years - Epiglottitis: 2-5 years |
|
|
Bronchiolitis vs. Croup vs. Epiglottitis: commonness? |
- Bronchiolitis: yes - Croup: yes - Epiglottitis: no |
|
|
Bronchiolitis vs. Croup vs. Epiglottitis: common causes? |
- Bronchiolitis: RSV (>75%), parainfluenza, influenza - Croup: parainfluenza (50-75%), influenza - Epiglottitis: H. influenzae, Staph species, Strep species |
|
|
Bronchiolitis vs. Croup vs. Epiglottitis: symptoms / signs? |
- Bronchiolitis: initial viral URI symptoms followed by tachypnea and expiratory wheezing - Croup: initial viral URI symptoms followed by "barking" cough, hoarseness, inspiratory stridor - Epiglottitis: rapid progression to high fever, toxicity, drooling, and respiratory distress |
|
|
Bronchiolitis vs. Croup vs. Epiglottitis: x-ray findings? |
- Bronchiolitis: hyperinflation - Croup: subglottic tracheal narrowing on frontal x-ray (steeple sign) - Epiglottitis: swollen epiglottis on lateral neck x-ray (thumb sign) |
|
|
Bronchiolitis vs. Croup vs. Epiglottitis: treatment? |
- Bronchiolitis: humidified O2, bronchodilators (efficacy uncertain); ribavirin for severe RSV or high risk RSV infections - Croup: dexamethasone, nebulized epi, humidified O2 - Epiglottitis: prepare to establish an airway, antibiotics (3rd gen. cephalosporin and anti-staphylococcal agent active against MRSA, such as vancomycin or clindamycin) |
|
|
Sequelae of streptococcal infection? |
- Rheumatic fever - Scarlet fever - Post-streptococcal glomerulonephritis (not prevented by use of antibiotics) |
|
|
What should you think of when you have a young adult with recurrent, varied neurologic signs/symptoms with no other cause evident? |
Multiple sclerosis |
|
|
Best diagnostic test for Multiple Sclerosis? |
- MRI (most sensitive) - LP (elevated IgG oligoclonal bands and myeline basic protein levels, mild elevation in lymphocytes and protein) - Evoked potentials (slowed conduction through areas with damaged myelin) |
|
|
What are the findings of MS on LP?
|
- Elevated IgG oligoclonal bands - Elevated myelin basic protein levels - Mild elevation in lymphocytes and protein |
|
|
Empiric treatment for unconscious or delirious patient in ED with no history or signs of trauma? |
- Thiamine (before glucose) for deficiency in alcoholic - Glucose for hypoglycemia - Naloxone for opioid overdose |
|
|
Aside from empiric treatment for unconscious or delirious patient in ED with no history or signs of trauma; what other commonly tested causes should you check for? |
- Alcohol use - Illicit or prescription drug use - Diabetic ketoacidosis - Stroke - Epilepsy or post-octal state - Subarachnoid hemorrhage (eg, aneurysm rupture) |
|
|
Delirium vs Dementia: onset? |
- Delirium: acute and dramatic - Dementia: chronic and insidious |
|
|
Delirium vs Dementia: common causes? |
- Delirium: illness, toxin, withdrawal - Dementia: Alzheimer disease, multi infarct dementia, HIV/AIDS |
|
|
Delirium vs Dementia: reversibility? |
- Delirium: usually - Dementia: usually not |
|
|
Delirium vs Dementia: attention? |
- Delirium: poor - Dementia: usually unaffected |
|
|
Delirium vs Dementia: arousal level? |
- Delirium: fluctuates - Dementia: normal |
|
|
Before what types of management should a reproductive age woman be screened for pregnancy? |
Potentially teratogenic therapies or tests (e.g., anti-epileptic drugs, x-ray, CT scan) |
|
|
Common causes of anaphylaxis? |
- Bee stings - Food allergy (peanuts, shellfish, etc) - Meds (PCN, sulfa drugs, etc) - Latex allergy |
|
|
Signs/symptoms of anaphylaxis? |
Symptoms develop rapidly and dramatically: - Agitation - Flushing - Itching (urticaria) - Facial swelling (angioedema) - Difficulty breathing |
|
|
Treatment for anaphylaxis?
|
- Secure airway (laryngeal edema may prevent intubation, in which case do a cricothyroidotomy if needed) - Give subcutaneous or IV epinephrine - Antihistamines and corticosteroids are not useful for immediate severe reactions that involve the airway |
|
|
Colorectal cancer screening guidelines? |
Starting >50 years for all studies: - Colonoscopy q10y - Flexible sigmoidoscopy q5y - Double-contrast barium enema q5y - CT colonography q5y - Fecal occult blood test annually - Fecal immunochemical test annually - Stool DNA test, interval uncertain |
|
|
Colon / Prostate cancer screening guidelines? |
Digital rectal exam annually once >40 years |
|
|
Prostate cancer screening guidelines? |
PSA (controversial, but offer annually) once >50 years, except >45 years if African American or >40 years if first-degree relative diagnosed at early age |
|
|
Cervical cancer screening guidelines? |
Pap smear beginning at age 21 years regardless of sexual activity: - Pap q3y until 30 - Pap + HPV q5y if both negative |
|
|
Gynecologic cancer screening guidelines? |
Pelvic exam starting at age 21y - Annually, after 3 normal exams, every 2-3 years - ≥65 years, annually, when to stop is not clearly established |
|
|
Endometrial cancer screening guidelines? |
Endometrial biopsy at menopause - no recommendation for routine screening in the absence of symptoms |
|
|
Breast cancer screening guidelines? |
- Breast self exam >20 years (benefits and limitations should be discussed, no longer recommended by American Cancer Society) - Physical exam by doctor between 20-40 years q3y; >40 years annually - Mammography >40 years annually |
|
|
Lung cancer screening guidelines? |
- Sputum / CXR not recommended for asymptomatic individuals even if at high risk - CT scan annually is controversial but may be indicated for smokers and former smokers aged 55-74 years who have smoked >1ppd for >30 years |
|
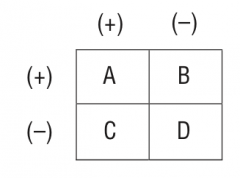
Calculation for Sensitivity? |
A / (A+C) |
|
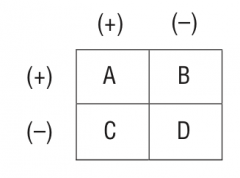
Calculation for Specificity? |
D / (B+D) |
|
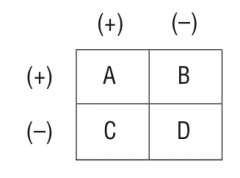
Calculation for PPV? |
A / (A+B) |
|

Calculation for NPV? |
D / (C+D) |
|
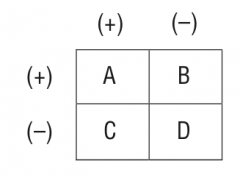
Calculation for Odds Ratio? |
(A * D) / (B * C) |
|
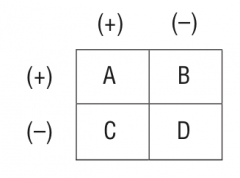
Calculation for Relative Risk? |
[A / (A+B)] / [C / (C+D)] |
|
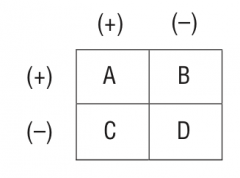
Calculation for Attributable Risk? |
[A / (A+B)] - [C / (C + D)] |
|
|
What does the "p-value" represent? |
Likelihood of making a type I error or claiming an effect or difference where none existed (i.e., results were obtained by chance) This expresses our confidence in the data |
|
|
What does it mean to reject the null hypothesis in a trial testing a new treatment? |
Null hypothesis hypothesizes that no difference exists
To reject the null hypothesis means the new treatment works |
|
|
Side effects of anti-psychotics? |
- Acute dystonia - Akathisia - Tardive dyskinesia - Neuroleptic malignant syndrome - Hyperprolactinemia - Autonomic nervous system related effects |
|
|
Drugs of abuse that are potentially fatal in withdrawal? |
- Alcohol - Barbiturates - Benzodiazepines |
|
|
Drugs of abuse that are potentially fatal in overdose? |
- Alcohol - Cocaine - Opiates - Barbiturates - Benzodiazepines - Phencyclideine (PCP) - Inhalants |
|
|
Most common preventable cause of infertility in U.S.? |
Pelvic Inflammatory Disease (PID) |
|
|
Most likely cause of infertility in younger, normally menstruating women?
|
Pelvic Inflammatory Disease (PID) |
|
|
Likely diagnosis in woman who is "heavy, hirsute, and [h]amenorrheic"?
|
Polycystic Ovarian Syndrome (PCOS) |
|
|
Most common cause of dysfunctional uterine bleeding? |
Polycystic Ovarian Syndrome (PCOS) |
|
|
Risk associated with Polycystic Ovarian Syndrome (PCOS)? Why? |
Endometrial cancer due to unopposed estrogen |
|
|
Cause of fetal / neonatal macrosomia? |
Maternal diabetes until proven otherwise |
|
|
Treatment for maternal diabetes? |
Diet and insulin (no oral agents) |
|
|
Causes of low maternal serum alpha fetoprotein (AFP)? |
- Down syndrome - Inaccurate dates (most common) - Fetal demise |
|
|
Causes of high maternal serum alpha fetoprotein (AFP)? |
- Neural tube defects - Ventral wall defects (e.g., omphalocele, gastroschisis) - Inaccurate dates (most common) - Multiple gestation |
|
|
When do you typically measure maternal serum alpha fetoprotein (AFP)? |
16-20 weeks gestation |
|
|
Definition of pre-eclampsia? |
HTN + Proteinuria in pregnancy (until proven otherwise) |
|
|
Signs/symptoms of ectopic pregnancy?
|
- Positive pregnancy test (not a clinically apparent pregnancy) - Vaginal bleeding and abdominal pain |
|
|
Diagnostic workup for suspected ectopic pregnancy? |
Pelvic ultrasound if patient is stable |
|
|
Early decelerations (normal/abnormal)? Cause? |
Normal - caused by head compression |
|
|
Variable decelerations (normal/abnormal)? Cause? Management? |
Common - usually caused by cord compression (turn the mother on her side, give O2 and fluids, stop oxytocin)
|
|
|
Late decelerations (normal/abnormal)? Cause? |
Abnormal - caused by uteroplacental insufficiency, most worrisome pattern Turn mother on her side, give O2 and fluids, stop oxytocin, measure fetal O2 saturation of scalp pH; prepare for prompt delivery |
|
|
Management of third trimester bleeding? |
Always perform an ultrasound before a pelvic exam (in case placenta previa is present) |
|
|
Most common cause of postpartum bleeding? |
Uterine atony - usually caused by uterine over distention (e.g., twins, polyhydramnios), prolonged labor, and/or oxytocin usage |
|
|
Acute abdomen pathology in RUQ? |
- Gallbladder / biliary (cholecystitis, cholangitis) - Liver (abscess) |
|
|
Acute abdomen pathology in LUQ? |
Spleen - rupture with blunt trauma |
|
|
Acute abdomen pathology in RLQ? |
- Appendix (appendicitis) - PID |
|
|
Acute abdomen pathology in LLQ? |
- Sigmoid colon (diverticulitis) - PID |
|
|
Acute abdomen pathology in epigastric region? |
- Stomach (peptic ulcer) - Pancreas (pancreatitis) |
|
|
6 W's of Post-op Fever? |
- Water - UTI - Wind - Atelectasis / PNA - Walk - DVT - Wound - wound infection - Wawa - breast (only in postpartum state) - Weird drugs - drug fever |
|
|
What should you think of in post-op patient with daily fever spikes that do not respond to antibiotics? Management? |
Post-surgical abscess - order a CT scan to locate, then drain the abscess if present |
|
|
ABCDEs of trauma? |
- Airway - Breathing - Circulation - Disability - Exposure |
|
|
Six rapidly fatal thoracic injuries? |
1. Airway obstruction 2. Open pneumothorax 3. Tension pneumothorax 4. Cardiac tamponade 5. Massive hemothorax 6. Flail chest |
|
|
Management of airway obstruction? |
Establish airway |
|
|
Management of open pneumothorax? |
Intubate and close defect on three sides |
|
|
Management of tension pneumothorax? |
Perform needle thoracentesis followed by chest tube |
|
|
Management of cardiac tamponade? |
Perform pericardiocentesis |
|
|
Management of massive hemothorax? |
Place chest tube to drain, thoracotomy if bleeding does not stop |
|
|
Management of flail chest? |
Consider intubation and positive pressure ventilation if oxygenation is adequate |
|
|
Causes of neonatal conjunctivitis? When is each most common? |
- Chemical conjunctivitis - first 12-24 hours of giving drops for prophylaxis - Gonorrhea - 2-5 days after birth, usually prevented with prophylactic drops - Chlamydia - 5-14 days after birth, often not prevented by prophylactic drops |
|
|
Most common form of glaucoma? |
Open-angle form (90%) |
|
|
Signs/symptoms of open angle glaucoma? |
- Painless (no "attacks") - Asymptomatic until irreversible vision loss (that starts in periphery) occurs |
|
|
Most common cause of blindness in African Americans?
|
Open angle glaucoma |
|
|
What should you think of in a patient with uveitis? |
Systemic conditions: - Juvenile idiopathic arthritis - Sarcoidosis - Inflammatory bowel disease - Ankylosing spondylitis - Reactive arthritis - Multiple sclerosis - Psoriasis - Lupus |
|
|
Common complaints of patient with uveitis? |
- Photophobia - Blurry vision - Eye pain |
|
|
Causes of bilateral (although often asymmetric) painless gradual loss of vision in older adults? |
- Cataracts - Macular degeneration - Glaucoma |
|
|
What is the name for the vision change that is a normal part of aging? Symptoms? |
Presbyopia - affects only near vision (i.e., accommodation) |
|
|
Common causes of compartment syndrome? |
After trauma or surgery |
|
|
Signs/symptoms of compartment syndrome? |
6 P's: - Pain - present on passive movement and often out of proportion to injury - Paresthesias - numbness, tingling, decreased sensation - Pallor - or cyanosis - Pressure - firm feeling muscle compartment, elevated pressure reading - Paralysis - late, ominous sign - Pulselessness - very late, ominous sign |
|
|
Treatment for compartment syndrome?
|
Fasciotomy to relieve compartment pressure and prevent permanent neurologic damage |
|
|
Functions of radial nerve? |
- Motor: wrist extension (watch for wrist drop) - Sensory: back of forearm, back of hand (first 3 digits) |
|
|
Functions of ulnar nerve? |
- Motor: finger abduction (watch for "claw" hand) - Sensory: front and back of last 2 digits |
|
|
Functions of median nerve? |
- Motor: pronation, thumb opposition - Sensory: palmar surface of hand (first 3 digits) |
|
|
Functions of axillary nerve? |
- Motor: abduction, lateral rotation - Sensory: lateral shoulder |
|
|
Functions of peroneal nerve? |
- Motor: dorsiflexion, eversion (watch for foot drop) - Sensory: dorsal foot and lateral leg |
|
|
Clinical scenario that commonly damages radial nerve? |
Humeral fracture |
|
|
Clinical scenario that commonly damages ulnar nerve? |
Elbow dislocation |
|
|
Clinical scenario that commonly damages median nerve? |
Carpal tunnel syndrome, humeral fracture |
|
|
Clinical scenario that commonly damages axillary nerve? |
Upper humeral dislocation or fracture |
|
|
Clinical scenario that commonly damages peroneal nerve? |
Knee dislocation |
|
|
Pediatric hip disorders? |
- Congenital hip dysplasia (CHD) - Legg-Calvé-Perthes Disease (LCPD) - Slipped Capital Femoral Epiphysis (SCFE) |
|
|
Congenital Hip Dysplasia vs. Legg-Calvé-Perthes Disease vs. Slipped Capital Femoral Epiphysis: common age of onset? |
- CHD: at birth - LCPD: 4-10 years - SCFE: 9-13 years |
|
|
Congenital Hip Dysplasia vs. Legg-Calvé-Perthes Disease vs. Slipped Capital Femoral Epiphysis: common presentation? |
- CHD: female, firstborn, breech delivery - LCPD: short male with delayed bone age - SCFE: overweight male adolescent |
|
|
Congenital Hip Dysplasia vs. Legg-Calvé-Perthes Disease vs. Slipped Capital Femoral Epiphysis: signs/symptoms? |
- CHD: Barlow and Ortolani signs - LCPD: Knee, thigh, groin pain, limp - SCFE: Knee, thigh, groin pain, limp |
|
|
Congenital Hip Dysplasia vs. Legg-Calvé-Perthes Disease vs. Slipped Capital Femoral Epiphysis: Treatment? |
- CHD: harness - LCPD: orthoses (braces) - SCFE: surgical pinning |
|
|
Can Congenital Hip Dysplasia, Legg-Calvé-Perthes Disease, or Slipped Capital Femoral Epiphysis occur in adults? |
Yes, may present in an adult as arthritis of the hip |
|
|
Under what circumstances should you avoid doing an LP? What should you do instead? |
Patient with head trauma or signs of intracranial pressure because of the risk of herniation; perform CT scan without contrast instead |
|
|
Most common causes of neck masses in children? |
75% are benign (e.g., lymphadenitis, thyroglossal duct cyst) |
|
|
Most common causes of neck masses in adults? |
75% are malignant (e.g., squamous cell carcinoma and or metastases, lymphoma) |
|
|
Management of carotid artery stenosis between 70-99%? |
Carotid Endarterectomy |
|
|
Management of carotid artery stenosis less than 50%? |
Medical management - anti-HTN agents, statins, anti-platelet therapy; treat atherosclerosis risk factors |
|
|
Management of carotid artery stenosis between 50-69%? |
Data on management is less clear, and patient specific factors affect the decision |
|
|
What should you think of with a pulsatile abdominal mass plus hypotension? |
Ruptured abdominal aortic aneurysm (AAA) until proven otherwise
|
|
|
Management of ruptured AAA? |
Immediate laparotomy - 90% mortality rate |
|
|
Conditions best viewed as anginal equivalents? |
- Transient ischemic attacks (TIAs) - Claudication - Chronic mesenteric ischemia |
|
|
Management of TIAs, claudication, chronic mesenteric ischemia? |
Arterial workup and imaging |
|
|
Main identifiable risk factor for testicular cancer? |
Cryptorchidism |
|
|
Complications of cryptorchidism? |
- Risk factor for testicular cancer - Can cause infertility |
|
|
Treatment of cryptorchidism? |
- Surgical retrieval - Orchiopexy or orchiectomy |
|
|
Presentation of Benign Prostatic Hypertrophy / Hyperplasia (BPH)? |
- Acute renal failure - Distended bladder and bilateral hydronephrosis on ultrasound |
|
|
Treatment of Benign Prostatic Hypertrophy / Hyperplasia (BPH)? |
- Drain the bladder first (catheterize) - Perform transurethral resection of the prostate (TURP) |
|
|
Causes of impotence? |
- Physical - vascular, nervous system, drugs - Psychogenic (less common) |
|
|
Signs of psychogenic impotence? |
Patients have normal nocturnal erections and a history of dysfunction only in certain settings |
|
|
Most common cause of delayed puberty? |
Constitutional delay - a normal variant |
|
|
Findings suspicious for child abuse? |
- Failure to thrive - Multiple injuries in different stages of healing - Retinal hemorrhages plus subdural hematomas (shaken baby syndrome) - STDs - Caretaker story that does not fit the child's injury or complaint - Childhood behavioral or emotional problems - Multiple personality disorder as an adult |
|
|
Categories of APGAR score? |
- Color - Heart rate - Reflex irritability - Muscle tone - Respiratory effort |
|
|
APGAR scoring for color? |
- 0: pale, blue - 1: body pink, extremities blue - 2: completely pink |
|
|
APGAR scoring for heart rate? |
- 0: absent - 1: <100 bpm - 2: >100 bpm |
|
|
APGAR scoring for reflex irritability? |
- 0: none - 1: grimace - 2: grimace and strong cry, cough, and sneeze |
|
|
APGAR scoring for muscle tone? |
- 0: limp - 1: some flexion of extremities - 2: active motion |
|
|
APGAR scoring for respiratory effort? |
- 0: none - 1: slow, weak cry - 2: good, strong cry |
|
|
Metabolic derangements associated with thiazide diuretics? |
- Hypercalcemia (calcium retention) - Hyperglycemia - Hyperuricemia - Hyperlipidemia - Hyponatremia - Hypokalemic metabolic alkalosis - Hypovolemia |
|
|
What kind of allergy is associated with thiazide diuretics? |
Sulfa allergies because this is a sulfa drug |
|
|
Metabolic derangements associated with loop diuretics? |
- Hypokalemic metabolic alkalosis - Hypovolemia (more potent than thiazides) - Ototoxicity - Hypocalcemia (calcium excretion) |
|
|
What allergy is associated with loop diuretics? |
Sulfa allergies - except for ethacrynic acid |
|
|
Metabolic derangements associated with carbonic anhydrase inhibitor diuretics? |
Metabolic acidosis |
|
|
Metabolic derangements associated with potassium-sparing diuretics (e.g., spironolactone)? |
Hyperkalemia |
|
|
Antidone for overdose of acetaminophen? |
Acetylcysteine |
|
|
Antidone for overdose of benzodiazepines?
|
Flumazenil |
|
|
Antidone for overdose of beta blockers? |
Glucagon |
|
|
Antidone for overdose of carbon monoxide? |
Oxygen (hyperbaric in cases of severe poisoning) |
|
|
Antidone for overdose of cholinesterase inhibitors?
|
Atropine, Pralidoxime |
|
|
Antidone for overdose of copper or gold? |
Penicillamine |
|
|
Antidone for overdose of digoxin? |
Normalize K+ and other electrolytes, digoxin antibodies |
|
|
Antidone for overdose of iron? |
Deferoxamine |
|
|
Antidone for overdose of lead? |
Edetate (EDTA), use sucker in children |
|
|
Antidone for overdose of methanol or ethylene glycol? |
Fomepizole; ethanol |
|
|
Antidone for overdose of muscarinic blockers? |
Physostigmine |
|
|
Antidone for overdose of opioids? |
Naloxone |
|
|
Antidone for overdose of quinidine? |
Sodium bicarb (cardioprotective) |
|
|
Antidone for overdose of tricyclic antidepressants? |
Sodium bicarb (cardioprotective) |
|
|
Side effects of Aspirin / NSAIDs? |
- GI bleeding / gastric ulcers - Renal damage (interstitial nephritis, papillary necrosis) - Allergic reactions - Platelet dysfunction (life of platelet for aspirin, reversible dysfunction with NSAIDs) - Reye syndrome (encephalopathy and/or liver failure in a child taking aspirin in the setting of a viral infection) |
|
|
Metabolic derangements of overdose of aspirin? |
- Metabolic acidosis - Respiratory alkalosis |
|
|
Complication of overly rapid correction of hyponatremia? |
Central Pontine Myelinolysis (brainstem damage and possibly death) |
|
|
What cellular shifts and symptoms can be caused by alkalosis? |
Alkalosis ---> symptoms of hypokalemia or hypocalcemia |
|
|
If someone with alkalosis or acidosis has symptoms of potassium and/or calcium derangement how do you treat? |
pH correction is needed (rather than direct treatment of calcium or potassium levels) |
|
|
What metabolic derangement can make hypocalcemia and hypokalemia unresponsive to replacement therapy? |
Magnesium depletion (must correct magnesium to get responsiveness to treatment of hypocalcemia and hypokalemia) |
|
|
If a patient is incompetent (including younger minors who lack adequate decision making capacity) and you need an emergency treatment, what should be done? |
Seek a family member or court-appointed guardian to make healthcare decisions; if no one is available, treat as you see fit in an emergency or contact the courts in a non-emergency setting |
|
|
What should be done if a patient has a living will or has made their wishes known if a family member is dissenting? |
Respect patient wishes and living wills (assuming that they are appropriate), but take time to listen to family members' concerns |
|
|
Under what circumstances can you break doctor-patient confidentiality? |
1. Patient asks you to do so 2. Child abuse is suspected 3. Courts mandate you to do so 4. You must fulfill the duty to warn or protect (if a patient says that he is going to kill someone or himself, you have to tell the person who is threatened, the authorities, or both) 5. Patient has a reportable disease 6. Patient is a danger to others (e.g., if a patient is blind or has seizures, let proper authorities know so they can revoke the patient's license to drive; if the patient is an airplane pilot and is paranoid, hallucinating schizophrenic, then authorities need to know) |
|
|
Causes of "false" laboratory disturbances? |
- Hemolysis --> hyperkalemia - Pregnancy --> elevated ESR and Alk Phos - Hypoalbuminemia --> hypocalcemia - Hyperglycemia --> hyponatremia |
|
|
ECG findings of myocardial infarction? |
- Flipped or flattened T waves - ST segment elevation (depression means ischemia; elevation means injury) - Q waves in a segmental distribution (eg, leads II, III, aVF for inferior infarct) - ST segment depression may also be seen in "reciprocal" / opposite leads |
|
|
Drugs that may be useful in the setting of acute coronary syndrome? |
- Aspirin - Morphine - Nitroglycerin - Beta blocker - ACE inhibitor - Clopidogrel - HMG-CoA reductase inhibitor - Glycoprotein IIb/IIIa receptor inhibitors - Heparin (unfractionated or low-molecular-weight heparin) - Tissue plasminogen activator (t-PA, strict criteria for use) |
|
|
What should you do for a patient with no CHD risk factors depending on LDL? |
- LDL <160 - none (meets goal) - LDL 160-189 - diet +/- meds - LDL ≥190 - meds (+ diet) |
|
|
What should you do for a patient with ≥2 CHD risk factors depending on LDL? |
- LDL <100 - none (meets goal) - LDL 100-129 - diet +/- meds - LDL ≥130 - meds (+ diet) |
|
|
What should you do for a patient with known CHD/equivalent depending on LDL? |
- LDL <100 - none (meets goal) - LDL ≥100 - meds (+ diet) |
|
|
What should you do for a patient with very high risk factors depending on LDL? |
- LDL <70 - none (meets goal) - LDL 70-99 - diet +/- meds - LDL ≥100 - meds (+ diet) |
|
|
Type 1 vs 2 diabetes: occurrence? |
- Type 1: 10% of cases - Type 2: 90% of cases |
|
|
Type 1 vs 2 diabetes: age at onset? |
- Type 1: most commonly <30 years - Type 2: most commonly >30 years |
|
|
Type 1 vs 2 diabetes: associated body habits? |
- Type 1: thin - Type 2: obese |
|
|
Type 1 vs 2 diabetes: development of ketoacidosis? |
- Type 1: yes - Type 2: no |
|
|
Type 1 vs 2 diabetes: development of hyperosmolar state? |
- Type 1: no - Type 2: yes |
|
|
Type 1 vs 2 diabetes: level of endogenous insulin?
|
- Type 1: low to none - Type 2: normal to high (insulin resistance) |
|
|
Type 1 vs 2 diabetes: twin occurrence? |
- Type 1: <50% - Type 2: >50% |
|
|
Type 1 vs 2 diabetes: human leukocyte antigen association? |
- Type 1: yes - Type 2: no |
|
|
Type 1 vs 2 diabetes: response to oral hypoglycemics? |
- Type 1: no - Type 2: yes |
|
|
Type 1 vs 2 diabetes: antibodies to insulin? |
- Type 1: yes (at diagnosis) - Type 2: no |
|
|
Type 1 vs 2 diabetes: risk for diabetic complications? |
- Type 1: yes - Type 2: no |
|
|
Type 1 vs 2 diabetes: islet cell pathology? |
- Type 1: insulitis (loss of most B cells) - Type 2: normal number, but with amyloid deposits |
|
|
Normal BP? |
- Systolic <120 - Diastolic <80 |
|
|
Prehypertension? |
- Systolic 120-139 - Diastolic 80-89 |
|
|
Stage 1 HTN? |
- Systolic 140-159 - Diastolic 90-99 |
|
|
Stage 2 HTN? |
- Systolic ≥160 - Diastolic ≥100 |
|
|
Condition associated with friction rub? |
Pericarditis |
|
|
Condition associated with Kussmaul breathing (deep, rapid breathing)? |
Diabetic ketoacidosis |
|
|
Condition associated with Kayser-Fleischer ring in eye? |
Wilson disease |
|
Condition associated with Bitot spots? |
Vitamin A Deficiency |
|
|
Condition associated with dendritic corneal ulcers on fluorescein stain of the eye? |
Herpes keratitis |
|
|
Condition associated with cherry red spot on the macula without hepatosplenomegaly? |
Tay-Sachs disease |
|
|
Condition associated with cherry red spot on the macula with hepatosplenomegaly? |
Riemann-Pick disease |
|
|
Condition associated with bronze skin plus diabetes? |
Hemochromatosis |
|
|
Condition associated with malaria rash on the face? |
Systemic Lupus Erythematosus |
|
|
Condition associated with heliotrope rash (purplish rash on eyelids)?
|
Dermatomyositis |
|
|
Condition associated with clue cells? |
Gardnerella vaginalis infection |
|
|
Condition associated with meconium ileum? |
Cystic fibrosis |
|
|
Condition associated with rectal prolapse? |
Cystic fibrosis |
|
|
Condition associated with salty tasting infant? |
Cystic fibrosis |
|
|
Condition associated with café-au-lait spots with normal IQ? |
Neurofibromatosis |
|
|
Condition associated with café-au-lait spots with mental retardation? |
McCune-Albright syndrome or Tuberous Sclerosis |
|
|
Condition associated with worst headache of the patient's life? |
Subarachnoid hemorrhage |
|
|
Condition associated with abdominal striae? |
Cushing syndrome or pregnancy |
|
|
Condition associated with honey ingestion? |
Infant botulism |
|
|
Condition associated with LLQ tenderness / rebound?
|
Diverticulitis |
|
|
Condition associated with children who torture animals? |
Conduct disorder |
|
|
Condition associated with currant jelly stools in children? |
Intussusception |
|
|
Condition associated with ambiguous genitalia and hypotension? |
21-hydroxylase deficiency in girls |
|
|
Condition associated with catlike cry in an infant? |
Cri-du-chat syndrome |
|
|
Condition associated with infant weight >10 pounds? |
Maternal diabetes |
|
|
Condition associated with anaphylaxis from immunoglobulin therapy? |
IgA deficiency |
|
|
Condition associated with postpartum fever unresponsive to broad-spectrum antibiotics? |
Septic pelvic thrombophlebitis |
|
|
Condition associated with increased hemoglobin A2 and anemia? |
Thalassemia |
|
|
Condition associated with heavy young woman with papilledema and negative CT/MR scan of head? |
Pseudotumor cerebri |
|
|
Condition associated with low-grade fever in the first 24 hours after surgery? |
Atelectasis |
|
|
Condition associated with Vietnam veteran? |
PTSD |
|
|
Condition associated with bilateral hillier adenopathy in an African American patient? |
Sarcoidosis |
|
|
Condition associated with sudden death in a young athlete? |
Hypertrophic obstructive cardiomyopathy |
|
|
Condition associated with fractures or bruises in different stages of healing in a child? |
Child abuse |
|
|
Condition associated with absent breath sounds in a trauma patient? |
Pneumothorax |
|
|
Condition associated with shopping sprees? |
Mania
|
|
|
Condition associated with constant clearing of throat in child or teenager? |
Tourette syndrome |
|
|
Condition associated with intermittent bursts of wearing?
|
Tourette syndrome |
|
|
Condition associated with koilocytosis? |
HPV or cytomegalovirus |
|
|
Condition associated with rash developing after administration of ampicillin or amoxicillin for sore throat? |
EBV infection (mono) |
|
|
Condition associated with daytime sleepiness and occasional falling down (cataplexy)? |
Narcolepsy |
|
|
Condition associated with facial port wine stain and seizures? |
Sturge-Weber syndrome |
|
|
Babinski sign? |
Stroking the bottom of the foot yields extension of the big toe and fanning of the other toes --> upper motor neuron lesion |
|
|
Beck triad? |
Jugular venous distention, muffled heart sounds, and hypotension --> Cardiac Tamponade |
|
|
Brudzinski sign? |
Pain on neck flexion with meningeal irritation --> meningitis |
|
|
Charcot Triad? |
Fever/chills, jaundice, RUQ pain --> Cholangitis |
|
|
Chvostek sign? |
Tapping on facial nerve elicits tetany --> hypocalcemia |
|
|
Courvoisier sign? |
Painless, palpable gallbladder plus jaundice --> pancreatic cancer |
|
|
Cullen Sign? |
Bluish discoloration of periumbilical area --> pancreatitis with retroperitoneal hemorrhage |
|
|
Cushing reflex? |
Hypertension, bradycardia, and irregular respirations --> high intracranial pressure |
|
|
Grey Turner sign? |
Bluish discoloration of flank --> pancreatitis with retroperitoneal hemorrhage |
|
|
Homans sign?
|
Calf pain on forced dorsiflexion of foot --> DVT |
|
|
Kehr sign? |
Pain in L shoulder --> ruptured spleen |
|
|
Leriche syndrome? |
Claudication and atrophy of the buttocks with impotence --> aortoiliac occlusive disease |
|
|
McBurney sign? |
Tenderness at McBurney point --> appendicitis |
|
|
Murphy sign? |
Arrest of inspiration during palpation under the rib cage on the right --> cholecystitis |
|
|
Ortolani sign / test? |
Abducting an infant's flexed hips causes a palpable / audible click --> congenital hip dysplasia |
|
|
Prehn sign? |
Elevation of a painful testicle relieves pain --> epidiymitis (vs testicular torsion) |
|
|
Rovsing sign? |
Pushig on LLQ than releasing you hand produces pain at McBurney point --> appendicitis |
|
|
Tinel sign? |
Tapping on the volar surface of the wrist elicits paresthesias --> carpal tunnel syndrome
|
|
|
Trousseau sign? |
Pumping up a BP cuff causes carpopedal spasm --> tetany from hypocalcemia |
|
|
Virchow triad? |
Stasis, endothelial damage, hyper coagulability --> risk factors for DVT |