Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
61 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
OLD CARTS
|
Onset, location, duration, character, aggravating factors, relieving factors, timing, severity
|
|
|
|
Vision is blurry for hours or days. Sometimes their glasses help but sometimes they don’t. Sometimes they see better without their glasses. They have an otherwise normal eye exam.
|
Poorly controlled diabetic; shifts in blood sugar cause osmotic shifts in the lens which change the refractive power
|
|
|
The patient reports periodic blurry vision. It is often worse when reading, working on the computer, or driving (tasks that decrease blinking frequency). Vision is initially excellent, then gets worse, and is improved with closing or rubbing the eyes.
|
Transient - tear film
|
|
|
|
: Visual symptoms include transient blackouts or whiteouts of vision that may have progressed to complete vision loss in one eye. Systemic associations may include fevers, fatigue, malaise, weight loss, night sweats, shoulder and hip pain (POLYMYALGIA RHEUMATICA), scalp tenderness, and jaw claudication.
|
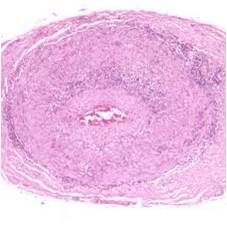
Transient - optic disc giant cell arteritis
Ischemic optic neuropathy due to inflammation within arteries |
|
|
|
optic disc giant cell arteritis
Chalky, pale disc Poor vision Relative or frank afferent pupillary defect (APD) |
|
|
Recent viral injury
|
Meningitis
|
|
|
History of hypercoagulability
|
Cerebral venous sinus thrombosis
|
|
|

Young female with weight gain
|
Pseudotumor cerebri
|
|
|
Transient blackouts when patients head is down. Diplopia (CN6 palsy)
|
Increased intracranial pressure
|
|
|

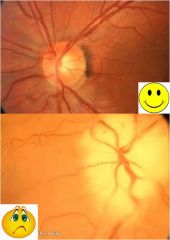
Testing for increased intracranial pressure (papilladema)
|
Fundoscopic exam shows disc edema; complete neurologic exam should be performed
Lumbar puncture (including opening pressure as well as laboratory tests) MRI/MRV |
|
|
|
Amaurosis fugax
|
Loss of vision in one eye due to temporary lack of blood flow to retina; may indicate impending stroke similar to TIA
|
|
|
|
Sudden loss of vision in one eye that lasts seconds to minutes. It may be associated with other neurologic symptoms if the patient has had a stroke.
|
Amaurosis fugax
|
|
|
|
Migraine aura; can be confused with amaurosis fugax (temp lack of blood flow to retina); colorful lights with slowly emerging blind spot in the same field of vision in both eyes - lasts 30-60 minutes
|
|
|

|
Carotid stenosis; can cause transient vision loss by blocking blood flow to retina (amagurosis fugax); work up for additional cardiac and vascular risk factors
|
|
|

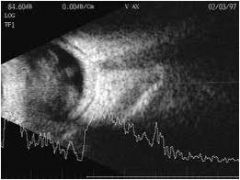
flashes of light, floaters, and a visual field defect or asymptomatic
|
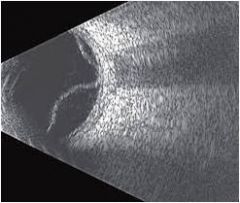
Retinal detachment
An ultrasound can show the detachment |
|
|

|
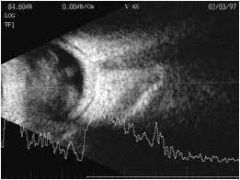
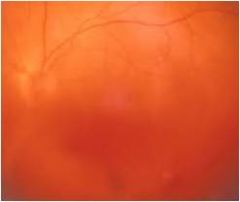
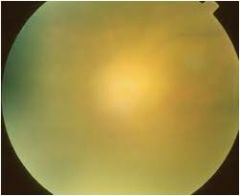
Vitreous debris; vitreous hemorrhage; usually painless
history may include DM, sickle cell, fungemia |
|
|
|
Vitreous debris; vitreous hemorrhage; usually painless
history may include DM, sickle cell, fungemia |
|
|
|
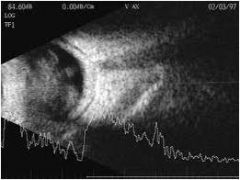
Endophthalmitis with viritis
hx may include dm, sickle cell, fungemia |
|
|

Cherry red spot
|
Central retinal artery occlusion; CRAO has an afferent pupillary defect (APD)
|
|
|

Hx of vascular risk factors, htn, glaucoma
|
Central retinal vein occlusion; CRVO will have APD if defect is severe; blood backs up
|
|
|
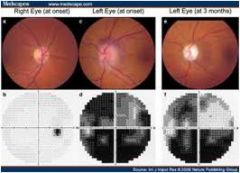
Vascular risk factors; VISION LOSS AFTER WAKING UP IN MORNING
|
Nonarteritic ischemic optic neuropathy; damage to optic nerve from insufficient blood supply
vision loss in morning bc of blood pressure fall during sleep (nocturnal arterial hypotension) APD present on exam; initially optic disk appears hyperemic |
|
|

Hx of vascular risk factors
|

Stroke; visual field defect corresponding with the location of the stroke and a normal dilated eye exam
|
|
|

Ketchup/mustard
|
K/M fundus + vision loss + AIDS = CMV
|
|
|
salt and pepper fundus
|
Congenital rubella and syphilis "Salt and pepper" fundus; can also have cataracts and glaucoma
|
|
|
|
Sudden onset, deep eye pain often with nausea and vomiting. Initially halos around lights and blurred vision but may progress to vision loss.
Affected eye feels firm and APD present |

Glaucoma
Red eye without discharge, fixed and mid dilated pupil, hazy cornea and an APD; eye feels firm in touch in comparison to other eye |
|
|
|
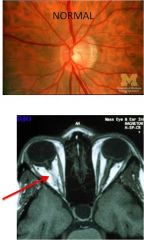
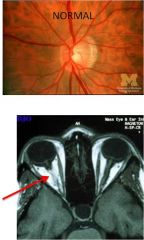
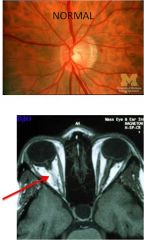
Normal
|
|
|
Pain with eye movement; often NORMAL dilated eye exam intiially
|
Optic neuritis; check MRI for additional plaques indicating MS
|
|
|
|
Pt is stressed out and can't see
|
Malingering/conversion syndrome; can use exam techniques to stimulate a visual response in pts who claim they can't see. Can also evoke visual potential in brain response to visual stimuli
|
|
|

|
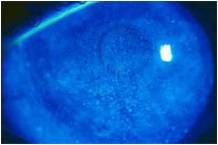
Keratoconus scarring
|
|
|

|
Mucopolysaccharidosis
|
|
|

|
corneal ulcer; can be acute or chronic pending cause; can lead to scarring
|
|
|

|
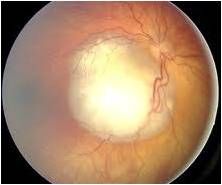
Leukocoria; retinoblastoma; calcifications can be seen on ultrasound and CT scan; mri used to detect extraocular spread of tumor
|
|
|
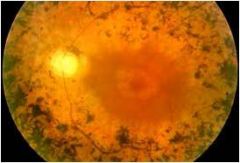
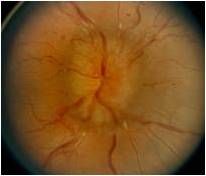
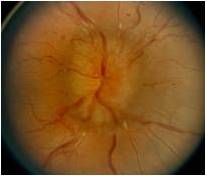
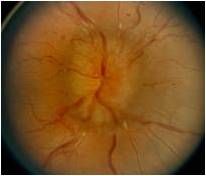
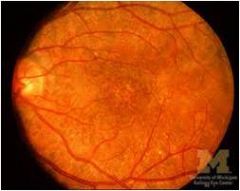
Poor night vision
Bony spicules in the peripheral retina, attenuation of the vessels, waxy pallor of th disc and sparing of the macula until very late in the disease |
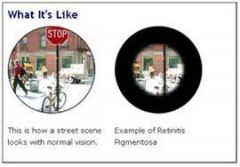
Retinitis pigmentosa;
|
|
|

Gradual or sudden decreasing vision
|
Diabetic retinopathy; do dilated eye exam
|
|
|

|
Macular degeneration
|
|
|
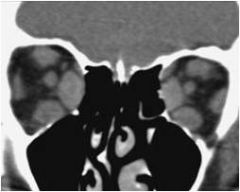
Diplopia, protosis, decreased vision. Could be slow or acute onset
|

Enlarged extraocular muscles; leads to compression of the optic nerve at the orbital apex; seen in thyroid disease
|
|
|

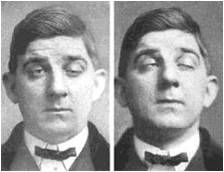
|
Lid retraction seen in thyroid dz; often asymmetric
|
|
|

|
Optic nerve glioma (tumor); lead to vision loss through compression or direct invasion; can also cause proptosis and diplopia
|
|
|
|
Monocular vs Binocular
|
Monocular: Pt has double vision with one eye open
Binocular: Double vision is only present when both eyes are open |
|
|
|
Keratoconus
|
Corneal dystrophy associated w progressive deformation of the cornea
|
|
|
|
Marfan's
|
Dislocated lens
|
|
|
|
Ehler's Danlos
|
Dislocated lens
|
|
|
|
Astigmatism
|
Irregularly shaped cornea or lens; causes light to bend abnormally
|
|
|
|
Pt reports diplopia or blurring of images while reading or working on the computer that resolves with blinking
|
Monocular Diplopia: Tear film
|
|
|
|
Pinhole device
|
Only lets a small, central amount of light through to the retina; can resolve symptoms in monocular diplopia
|
|
|
|
Binocular Diplopia
|
"If I close either eye, I see single again." This can be LIFE THREATENING so do not ignore a pts complaint of new onset, binocular double vision
|
|
|
|
Cranial nerve pneumonic to extraoculars
|

SO4LR6 - all others are three
Lateral Rectus - 6 Superior oblique - 4 Everything else is 3, including elevating the eyelid and pupillary constriction |
|
|
|
what muscles are controlled by CN3
|

superior, inferior and medial rectus
|
|
|
|
Acute onset of double vision and ptosis
|
Aneurysm of the post. communicating artery
|
|
|
|
Subacute onset of double vision and ptosis
|
CN3 compression from tumor
|
|
|
|
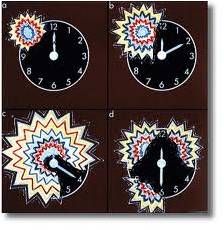
Congenital CN4 palsy
|
most dont have diplopia bc contralateral head tilt to accomodate
|
|
|
|
Function of the superior oblique
|
Controlled by trochlear nerve; intorts and depresses the eye
|
|
|
|
Basilar skull fracture
|
CN6 palsies; the nerve takes a sharp 90 degree turn intracranially which places it at risk for injury due to stretch with increased intracranial pressure.
|
|
|
|
Explanations for extraocular movement deficits which do not fit on specific cranial nerve pattern
|
MG, orbital pathology, cavernous sinus pathology, CNS pathology
|
|
|
With variability and fatiguability
|
Myasthenia gravis; ptosis mcc but can also affect extraocular movements causing diplopia
|
|
|
|
Dx of MG?
|

Tensilon test; acetylcholinesterase inhibitor increases Ach in NMJ to overcome AchR ab temporarily
AchR test (but negative in 50% of pts with ocular MG) |
|
|

|
muscle trapped in orbital fracture; can limit vertical gaze and is a surgical emergency
since many nerves enter from the posterior orbit and travel to corresponding muscles any inflammatory or infectious process within the orbit can cause EOM disturbance |
|
|
|
Thyroid eye disease
|
Muscles become enlarge and fibrotic which causes restriction of that muscle. The most commonly involved muscles are the inferior rectus and medial rectus although all may become involved.
|
|

|
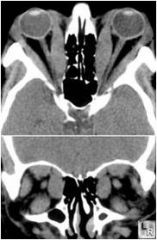
Orbital tumor:
May infiltrate one or more extraocular muscles or cause movement disruption by mass effect. Shown to the left is an adenocystic carcinoma of the lacrimal gland which can cause downward and medial displacement of the globe leading to diplopia. |
|
|
|
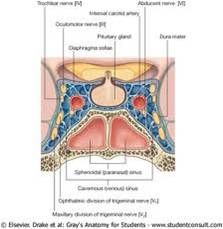
Binocular diplopia
As seen in the anatomy of the cavernous sinus at the right, several cranial nerves that innervate the extraocular muscles are in close proximity. Therefore any lesion in this area can lead to involvement of multiple nerves. Given that V1 branch of CN 5 also travels in the area, patients may have sensory deficits or pain in that dermatome. Examples include: Vascular lesions – fistulas Infectious/Inflammatory – often spread from the sinuses Tumors – from sinuses, pituitary, meningiomas, metastases |
|
|

|
Internuclear opthalmoplegia
Lesion om MLF that connects CN3 and 6 nuclei to coordinate medial and lateral rectus for horizontal gaze Can be caused by small microvascular event or demyelinating dz such as MS in younger pts |
|