Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
75 Cards in this Set
- Front
- Back
|
List the derivatives of the pharyngeal pouches.
|
Pharyngeal Pouches:
1: Epithelium of middle air, auditory tube 2: Epithelium of palatine tonsil 3: Thymus, Inferior Parathyroid 4: Superior parathyroid |
|
|
Scapular Winging:
Nerve and Muscle Affected |
Serratus anterior
Long thoracic N |
|
|
Serratus anterior:
Action |
Fixes scapula against posterior chest wall
|
|
|
Deltoid:
Action Nerve |
Flex, extend, abduct arm
Axillary |
|
|
Rhomboid Major:
Action Nerve |
Dorsal Scapular
Draws scapula medially |
|
|
Budding cells in esophagus
|
Candida
|
|
|
Immune defenses against candida:
Roles of each defense |
1) Th1 cells--local defense
2) Neutrophils: prevents hematogenous spread (via phagocytosis) |
|
|
What distinct infections would low complement predispose someone to?
|
SHiN bacteria bc can't form MAC
|
|
|
Following total ishemia, when do cardiac myocytes cease to contract?
When does irreversible ischemic injury occur? |
Within 60 seconds
Irreversible ischemia ~30 minutes after |
|
|
First-line treatment for HTN
|
Thiazide diuretics
|
|
|
First-line treatment for HTN s/p MI
|
beta-blockers
|
|
|
What is the best way to prevent neonatal tetanus?
|
Vaccinate mom while she's pregnant with tetanus toxoid.
She'll produce IgG Ab's which will be transferred to the baby via the placenta! |
|
|
Antithyroid Drugs:
MOA Examples How do they differ? AE |
Methimazole, PTU:
Prevent oxidation of iodine in thyroid gland (which prevents iodination of tyrosine residues) PTU decreases peripheral conversion of T4 to T3, has a shorter half-life, and is drug of choice in pregnancy. MTZ is a TERATOGEN. AE: AGRANULOCYTOSIS!!! |
|
|
34 year-old female
h/o Hypercalcemia treated with neck surgery Bitemporal visual field defects Diagnosis Pathophys of Syx |
Hypercalcemia treated with neck surgery likely was a parathryoid adenoma (tumor)
Bitemporal visual defects due to pituitary tumor extending above sella tursica and consequently compressing optic chiasm. Patient with h/o pituitary and hyperparathyroid tumor should be evaluated for pancreatic tumor because of MEN TYPE 1 SYNDROME |
|
|
Describe the following stages of acute tubular necrosis:
Initiation Maintenance Recovery |
Initiation:
Ischemic injury to renal tubules secondary to hemorrhage, acute MI, sepsis, surgery, etc. Maintenance (24-36 hours after inciting event): Dec'd urine output, fluid overload, inc'd Cr/BUN, hyperkalemia Recovery (1-2 weeks after maintenance staget): Gradual increase in urine output leading to high-volume diuresis. Electrolyte abnlts may include dec'd K, Mg, PO4, and Ca due to slowly recovering tubular function. |
|
|
Why is it that human influenza viruses can undergo reassortment when exposed to animal viruses?
How does this lead to pandemic? Which family of viruses does influenza belong to? What other virus can undergo this reassortment? |
Influenza A is an orthomyxovirus and has a segmented genome. Can undergo genetic reassortment with animal orthomyxoviruses which sometimes result in altered viral surface glycoproteins (eg, hemagglutinin). This can lead to pandemic.
Other virus that can do this is Rotavirus because it is also segmented. Note: Reassortment involves exchange of entire genome segments, a far more dramatic process than point mutations in genetic drift. |
|
|
This region of the hypothalamus produces oxytocin and ADH.
|
Supraoptic and Paraventricular nuclei
Note: oxytocin and ADH are then transported to posterior pituitary for release. |
|
|
This region of the hypothalamus mediates hunger.
|
Lateral nuclei
If lesion lateral nuclei-->starvation ensues (no hunger) |
|
|
This region of the hypothalamus mediates sweating and vasodilation.
|
Anterior nuclei (via PSymp)
If lesion--> hyperthermia |
|
|
This region of the hypothalamus mediates satiety.
|
Ventromedial
If lesion-->hyperphagia and obesity |
|
|
Hepatic encephalopathy:
Pathophys Treatment Treatment MOA |
Hepatic damage-->dec'd ability to detoxify nitrogenous wastes (carry out Ammonia-->Urea)
Inc'd ammonia results in disorientation Tx: Lactulose--bacterial action on lactulose results in acidic colonic contents-->converts absorbable ammonia into nonabsorbable ammonium ion (an ammonia trap) |
|
|
Von Recklinghausen's Disease:
Presentation |
AKA Neurofibromatosis type 1
PNS tumor syndrome Pts develop neurofibromas, optic nerve gliomas, Lisch nodules (pigmented nodules of iris), CAFE AU LAIT SPOTS |
|
|
Neurofibromatosis II:
Presentation |
B/L CN VIII (vesitbulocochlear) Schwannomas, multiple meningiomas
|
|
|
Sturge-Weber Syndrome:
Presentation |
Cutaneous facial angiomas and leptomeningeal angiomas
Skin involvement overlies ophthalmic (V1) and maxillary (V2) distributions of trigeminal nerve Also presents with MR, seizures, hemiplegia, TRAM-TRACK radiopacities on skull radiographs |
|
|
Tuberous Sclerosis:
Presentation |
Kidney/liver/pancreatic cysts
CNS cortical and subependymal hamartomas |
|
|
Oslwer-Weber-Rendu Syndrome:
Presentation |
Congenital telangectasias
Ruptures may result in epistaxis (rhinitis w/hayfever), GI bleeds, hematuria NO CYSTS PRESENT |
|
|
von Hippel-Lindau Disease:
Presentation |
Cappilary hemangioblastomas in retina and/or cerebellum
Congenital cysts and/or neoplasms in kidney, liver, pancreas INc'd risk RCC (b/l) |
|
|
Enlarged tongue
Jaundice Hypotonia Poor feeding 1 month-old Diagnosis |
Congenital hypothyroidism
Causes severe, irreversible MR if not treated immediately (need T4 for normal brain dev't and myelination during early life) |
|
|
What are the derivates of the aortic arch?
|
1st--MAXIMAL; maxillary artery
Second = Stapedial and hyoid aa Third = C is third letter of alphabet-->Carotid artery 4th--4 limbs!--systemic circuln; on left: aortic arch, on right: proximal right subclavian artery (there is no 5th) 6th arch: pulmonary aa and (on left only) ductus arteriosus |
|
|
Branchial arch derivates
|
1-M's, T's--Mandible, malleus incus, muscles of MASTICATION, mylohyoid
2-S's--Stapes, styloid process, stylohyoid 3-Pharyngeal--stylopharyngeus 4th: cricothyroid 6th: everything in larynx except cricothyroid |
|
|
Branchial pouch derivatives
|
1st: middle ear
2nd: palatine tonsil 3rd: INFERIOR PARATHY, THYMUS TOO 4th: SUPERIOR PARATHY Note 4th ends up being more superior than 3rd! |
|
|
24-year old female
Infertile Treated with menotropins following single injection of hCG Explain drug MOA |
Menotropin: acts like FSH and leads to formation of dominant ovarian follicle
hCG causes an LH surge |
|
|
5 year-old
Bounding pulse over upper left sternum Continuous murmur Diagnosis |
PDA (CONTINUOUS MURMUR)
|
|
|
When do double-stranded DNA breaks occur?
|
After exposure to ionizing radiation: X-rays, gamma-rays
|
|
|
Describe the events that occur following UV light damage (and subsequent repair) to skin cells.
|
UV light causes thymine dimer formation
Excision of dimer and surrounding nucleotides by UV-ENDOnuclease (not exo!!)--this is accomplished by nicking strand at thymine dimer Signals removal and replacement of DNA by POLYMERASE and LIGASE |
|
|
Anastrozole:
MOA Use |
Used in malignant breast cancer
Prevents aromatization of Androgens to Estrogen REMEMBER: Estrogen is the main hormone responsible for the growth and dev't of malignant breast tumors Aromatase inhibitors suppress estrogen to postmenopausal levels. |
|
|
HER2/neu receptor type
|
Tyrosine kinase
(Trastuzumab!) |
|
|
Congenital deafness due to fetal infection
|
Rubella
|
|
|
Congenital malformed teeth due to fetal infection
|
Syphilis
|
|
|
Polyarthritis
Rash that began on face and spread downward Generalized LAD Diagnosis |
Rubella
|
|
|
Congenital rubella:
Presentation |
Sensorineural deafness
Cataracts Cardiac Malformations (PDA) |
|
|
Describe how Fructose-2,6-bisphosphate affects glucose breakdown.
What is its effect on alanine metabolism? |

Note: Alanine is transaminated to pyruvate during gluconeogenesis!
|
|
|
Describe the Calcium-related events for skeletal muscle contraction.
|
Upon release from Sarcoplasmic Reticulum, calcium binds to TROPONIN C on thin filaments.
This shifts the position of TROPOMYOSIN exposing MYOSIN BINDING SITE on ACTIN filament. Lasts only a fraciton of a second before calcium resequestered within SR by Ca2+-ATPase pump |
|
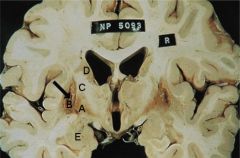
Label
|
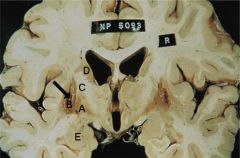
A) Globus Pallidus (part of basal ganglia along w/caudate and putamen)
B) Putamen C) Internal Capsule D) Caudate (affected in HD) E) Amygdala (limbic system) |
|
|
What is the effect of organophosphate poisoning on muscle activity?
Pathophys of Organophosphate poisoning Treatment |
Organophosphate poisoning irreversibly inhibits cholinesterase.
Inc'd ACh concentration in nicotinic synapses (which are also ACh dependent) leads to muscle fasciculations followed by paralysis. Atropine will reverse muscarinic symptoms, but has no effect on NICOTINIC receptors. Use PRALIDOXIME to reverse both muscarinig and nicotinic side effects by restoring cholinesterase from its bond with these substances. |
|
|
MHC I vs MHC II:
Present on which cells? What does each present? |
MHC I: present on all nucleated cells; present self-antigen, tumor antigen, or cell antigen in response to viral infection
MHC II: APCs only (DC's, macs, B cells)--bacterial organisms, viral particles, freely circulating antigenic material is endocytosed and presented |
|
|
Describe the process of presenting a bacterial antigen on an APC.
|
Antigen is phagocytosed and is loaded onto MHC II with ACIDIFIED ENDOSOMES.
MHC II protein-antigen complex is then expressed on cell surface for subsequent interaction with T cells Failure to acidify lysosomes would lead to deficient expression of MHC II bound to foreign antigen and subsequent lack of interaction b/t APCs and T cells |
|
|
Which enzymes in glycolysis are unidirectional?
How is this overcome during gluconeogenesis? |
Unidirectional:
Hexokinase PFK Pyruvate Kinase Enzymes are bypassed via: Pyruvate Carboxylase (Pyruvate-->OAA) (-->Malate to exit mitochondria) Malate--> OAA OAA-->Phosphoenolpyruvate via Phosphoenolpyruvate carboxykinase (PEPCK) Then use Fructose 1,6-bisphosphatase (to bypass PFK) Glucose-6-phosphatase (to bypass hexokinase) |
|
|
What metabolic processes provide glucose during fasting?
|
Between meals: glycogenolysis (until glycogen depleted) and gluconeogenesis
After 12-18 hours of fasting (when glycogen is depleted): Gluconeogensis (OAA-->Malate-->Phosphoenolpyruvate-->Glucose) |
|
|
What virus is polycistronic?
What structurally enables this? What does it require? |
Echovirus mRNA is polycystronic (contains multiple genes within sema mRNA transcript) and produces polyprotein product.
For individual viral proteins to be generated, polyprotein product must be cleaved by specific viral protease. Can do this because it's Single Stranded, Positive Sense, and Non-Segmented. |
|
|
Carvedilol:
MOA Use |
non-specific blockage of beta-1, beta-2, alpha-1
Use in CHF |
|
|
Describe how Neisseria meningitidis gains access to the CNS.
|
First colonized nasopharynx
INvades mucosa to gain access to the bloodstream Spreads to choroid plexus through blood Passess BBB Initiates inflammatory response |
|
|
C3a:
Effects |
Component of complement
C3a, 4a, 5a all trigger histamine release from mast cells, resulting in vasodilation and enhanced vasc perm |
|
|
C5a:
Effects |
Vasodilation, enhanced vasc perm
Recruits and activates NEUTROPHILS |
|
|
5-HETE:
Effects Associated enzyme |
5-Lipoxygenase
Neutrophil chemotaxis |
|
|
Leukotriene B4:
Effects Associated enzyme |
5-lipoxygenase
Neutrophil chemotaxis |
|
|
Luekotriene C4:
Effects Associated enzyme |
Vasoconstriction
Bronchospasm*** Inc'd vasc perm This is true for LK-C4/D4/E4 |
|
|
Lipoxin A4:
Effects Associated Enzyme |
Vasodilation
INHIBITION of neutrophil chemotaxis Stimulates monocyte adhesion Made by 12-lipoxygenase |
|
|
PGI2:
Effects Associated Enzyme |
COX1,2
PGI2 AKA PROSTACYCLIN Vasodilation Inhibition of PLT agg |
|
|
Thromboxane:
Effects Associated Enzyme |
COX-1,2
Vasoconstriction (CONSTRICT) Promotes PLT agg (PROMOTES) |
|
|
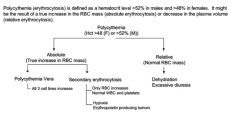
What is the laboratory cutoff for polycythemia and how would you classify it?
|
|
|
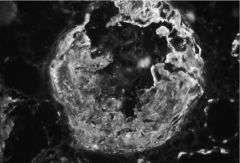
Diagnose
What is being deposited? Pathophys |
Crescent formation consistent with Rapidly Progressive Glomerulonephritis
Slide shows deposition of fibrin Crescents consist of proliferated glomerular parietal cells, monocytes, macs that have migrated to Bowman's space. As progresses, fibrin becomes sclerotic. This is sign of severe renal injury. Usually leads to rapid and irreversible loss of renal function. |
|

Diagnose
What is being deposited? Pathophys |
LInear deposits of C3 and IgG consistent with TYpe 1 Rapidly Progressive GN (i.e., GOODPASTURE SYNDROME)
C4 deposition is NOT found. |
|
|
Ulceration in which segment of the GI tract is LEAST associated with malignancy?
|
Duodenum
Usually due to H pylori or NSAIDs |
|
|
65 year-old male
Progressive weight loss Jaundice Anorexia Palpable gall bladder, non-tender Diagnosis Most important environmental risk factor |
JAUNDICE AND NONTENDER GALLBLADDER IS PANCREATIC CARCINOMA!!!!!!!!!!!!!!
Biggest environmental risk factor is smoking |
|
|
When is general anesthesia achieved?
How is potency of anesthetic defined? |
General anesthesia achieved when threshold amount of anesthetic accumulates in brain
Potency determined by minimal dose to depress CNS; when brain saturated with anesthetic, partial pressure of gas in brain = partial pressure in other compartments. So use alveolar concentration. Minimal alveolar concentration is used to measure potency: it refers to concentration of inhaled anesthetic that renders 50% of pts unresponsive to painful stimuli. Lower MAC-->more potent anesthetic |
|
|
What properties of anesthetics give it a slow onset of action?
|
High blood/gas partition means highly soluble in blood-->slow onset
High blood/lipid partition-->high solubility in tissues-->slow onset of action |
|
|
Episodic HTN
|
Pheochromocytoma
|
|
|
Vitiligo:
Pathophys |
Some sort of autoimmune activity (not really known) leads to COMPLETE LOSS OF EPIDERMAL MELANOCYTES
|
|
|
Wilson's Disease:
Treatment |
Penicillamine (Cu chelator)
|
|
|
Lead poisoning:
Treatment |
Dimercaprol and EDTA (chelators for lead)
|
|
|
Hemochromatosis:
Chelating Treatment |
Deferoxamine (BRONZE DIABETES)
|
|
|
Child suddenly dies
Erythroid precursor cells found in liver and spleen Diagnosis Pathophys |
Extramedullary hematopoiesis likely caused by severe chronic hemolytic anemia, such as beta-thalassemia
|
|
|
What is the effect of beta-blockers on EKG waveforms? Why?
|
Beta-blockers slow AV conduction and will increase the PR interval.
Remember: PR interval is the period of time from beginning of atrial depolarization to the beginning of ventricular depolarization. The longer the PR interval, the longer it takes for an electrical stimulus to travel from the SA node to the ventricles via the AV node, bundle of His, and fascicles. |
|
|
What EKG abnormality is associated with increased risk for Torsade de pointes?
What drugs cause this abnormality? |
Long QT; quinidine, sotalol most frequently associated with long QT
|