![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
what modification does he do to ohm's law |
I = deltaE/R rather than just V |
|
|
P wave is from |
depolarization of the atria
starts on right and goes left. has an expected duration. |
|
|
QRS complex is from |
depolarization of the ventricles |
|
|
T wave is from |
repolarization of the ventricles |
|
|
what intervals are there and what are the boundaries?
what is the significance? |
PR interval from P to beginning of QRS- atria to ventricles this is conduction through AV node
QT from beginning of QRS to end of T- that's during the plateau period of the myocyte
QRS
ST: beginning of S to beginning of T |
|
|
how are the QRS waves defined? |
q is any downward deflection in the beginning r is any upward S is downward after an upward |
|
|
how does the vector thing work with the ventricular depolarization example |
phase 0 for each myocyte makes a small eletrical signal from depolarized tissues to polarized tissues. We add all of them up to an electrical vector that is much larger |
|
|
what points are the measurements taken from? what are the leads? what do they make up? |
sensor on both wrists and a ground on the leg
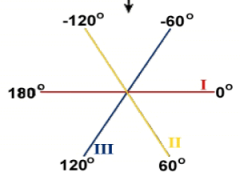
bipolar leads: these are - -> + I Right to Left shoulder II right shoulder to abdomen III left should to abdomen
makes Einthoven's triangle |
|
|
so how do the vectors translate to the leads |
about the shadow: if parallel will have high intensity signal, if perpendicular none
vector originates at center of triangle: so can be positive or negative in direction = deflection positive or negative depending which pole it points to |
|
|
we don't really use Einthoven's triangle now but a modern representation
three bipolar leads version |
|
|
|
in addition to the bipolar leads we usually add 3 unipolar leads. how does that work? |
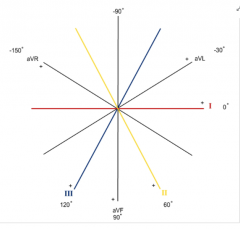
it's not a true monopolar- just the pole they're measured against is some made up one that isn't affected by the heart's activity ("indifferent" node) |
|
|
where is the plane of the leads relative to the body |
limb leads: center is in the heart frontal plane = parallel to ant and post surfaces of the body
chest leads: as well as thrid dimension with electrodes on pt chest for leads V1-V6 in a plane perpendicular to the limb leads |
|
|
so how many total leads for ECG? |
12
6 limb and 6 chest |
|
|
what is the standard axis size for ECG? |
standard paper speed 25mm/sec = 0.4sec/cm standard gain 1mv/cm |
|
|
what is the mean electrical axis? what is a typical one?
how is this calculated? |
vector depicting avg electrical activity over entire QRS complex: -30 to +90 range
you make a mean electrical axis modern machines calculate for you |
|
|
how does the waves align with events? |
upstroke of atrial muscle AP is during the P wave (it blends over because there are different myocytes that do it at different times)
QRS: atrial repolarization is "buried" in it, phase 0 of AP from ventricular myocytes
T: phase 3 AP repolarization ventricular (same orientation because it travels the opposite direction) |
|
|
what are normal duration and intervals
P wave PR interval QRS duration QT interval (corrected for HR) |
P wave < 0.12s PR interval 0.12-0.20s QRS 0.06-0.10s QT male: < 0.45 sec female <0.47s |
|
|
you see that the PR interval is prolonged. meaning? |
first degree block of AV node
conduction velocity is slowed but ultimately gets there |
|
|
computer says "NSR" |
normal sinus rhythm |
|

ECG: variable PR intervals, occasionally P wave without QRS or T |
second degree AV block only some of the signals get through AV node |
|

P waves not related to QRS + T waves |
third degree AV block
AV-node junctional region takes over as pacemaker for ventricles: junctional pacemaker
or excitable focus within ventricular myocardium acts as a ventricular ectopic pacemaker causing ventricular ectopic beat = premature ventricular contraction |
|
|
in pt with third degree AV block what implant may be used? |
demand pacemaker |
|
|
Heartbeat normally originates within the ___ node ___ the ventricles: this is called ___ rhythm.
in situations like ___ the beat may originate within one of the ventricles. These ventricular beats (___) cause ___ and can have consequences like ___ leading to ___ |
SA node above the ventricles: supraventricular rhythm
myocardial ischemia, PVC arrhythmias -> ventricular fibrillation -> sudden cardiac death |
|
|
how do PVCs look like on EKG? |
no P wave before it, occurs beore the next expected sinus beat = premature, and shape/amplitude/duration of QRS is "bizarre"
in interrupts the normal P wave so there is a compensatory pause until the next beat is scheduled |
|
|
what is usually the cause of VEB? |
myocardial ischemia causing either
increased automaticity: slowly depolarizes during Phase 4 or "after depolarizations"- Em fluctuates to more depolarized states sometimes making AP re-entrant pathway: two beats, normal followed by PVC in a coupled fashion = pulsus alternans or ventricular bigeminy |
|
|
how does re-entrant pathway work? |
unidirectional block and decremental conduction
there are separation of paths and crossovers. Usually the signal collides at the crossovers to cancel out.
If a unidirectional block one branch cut off, the circling signal does decremental conduction back up and around (UNIdirectional block doesn't stop) and another beat happens |
|
|
what's the condition that will get you the shock paddles? |
ventricular tachycardia = V-tach ventricular fibrillation (VF)
these have to be fixed quickly or pt dies |
|
|
during what phases are the myocytes equal in potential |
diastole ~-80 plateau ~0
|
|
|
if a MI has happened how is that seen? |
if some myocardium is ischemic it will not depolarize so it's at a different potential during electrical systole- makes for a "current of injury" flowing during the ST portion of the ECG
so on ECG there will be an ST elevation on one of the leads (checking the ST of the different leads will identify the location and size of the MI) |