![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
198 Cards in this Set
- Front
- Back
|
When are screening exams performed? |
when the patient's primary subjective complaint is related to an extremity or a part of the spine |
|
|
what should be examined if there is an UE complaint? What if there is a LE complaint? |
if UE complaint: cervical and thoracic spine should be examined if LE complaint: lumbar spine and pelvis should be examined |
|
|
what are components of the lower quarter screening exam in standing? |
PATHS 1. Postural assessment 2. Active forward, backward, and lateral bending of lumbar spine 3.Standing flexion test/ Gillet's test 4. Toe Raises (S1, tibial nn) 5. Heel walking (L4, L5 deep fibular nerve) |
|
|
what are the components of the lower quarter screening exam in sitting? |
5 SAP RD 1. Sitting flexion test 2. Active rotation of the lumbar spine 3. Passive OP if symptom free 4. resisted hip flexion (L1, L2, femoral nn) 5. resisted knee ext (L3, L4, femoral nn) 6. Resisted ankle DF (L4, L5 deep fibular nn) 7. resisted big toe ext (L5 deep fibular nn) 8. resisted ankle eversion (L5, S1 superficial peroneal nn) 9. DTR: patellar (L3, L4) and Achilles tendon (S1, S2) |
|
|
What are the components of the lower quarter screening exam in supine? |
![1. dermatome sensory testing
2. SLR (L4, L5; S1)
3. Passive ROM of hip
4. Sciatic nn tension test (SLR w/ variations for tibial nn [DF/eversion], peroneal nn [PF/inversion], sural [Df/inversions]](https://images.cram.com/images/upload-flashcards/51/71/10/8517110_m.png)
RNDS 1. Passive ROM of hip 2. Sciatic nn tension test 3. dermatome sensory testing 4. SLR (L4, L5; S1)
1. dermatome sensory testing 2. SLR (L4, L5; S1) 3. Passive ROM of hip 4. Sciatic nn tension test (SLR w/ variations for tibial nn [DF/eversion], peroneal nn [PF/inversion], sural [Df/inversions] |
|
|
What are the components of the lower quarter screening exam in prone? |

BF 1. Femoral nn tension test 2. Babinski reflex test (UMN)
|
|
|
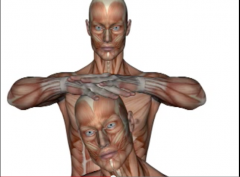
What are the components of the upper quarter screening exam? |
PAP VAQ BAR9 Passive OP if symptom free AROM cervical spine Postural assessment
Vertebral artery test Active shoulder flexion, abduction, IR, ER Quadrant test
Babinski Reflex test (UMN) AROM of elbow Resisted: 1-2 elbow flexion (C6) ext (C7) 3-4 wrist flexion (C7) ext (C6) 5 -thumb ext (C8) 6- finger abduction (T1) 7- cervical spine rotation (C1) 8-9 shoulder elevation (C2, C3, C4) and abduction (C5) |
|
|
What is the accessory mobility scale? |
-complete joint play/ testing of joint mobility when the joint capsule is most relaxed or in the loose packed position 0 Ankylosed joint 1 considerable limitation/hypomobility 2 slight limitation/hypomobility 3 Normal 4 slight hypermobility 5 considerable hypermobility 6 Pathologically Unstable |
|
|
What are the 4 possible findings of resisted mm testing? and what does each indicate? |
1. strong and painless: no pathology in contractile tissue 2. Strong and painful: minor structural lesion of the muscle-tendon unit 3. Weak and Painless: complete rupture of muscle-tendon unit or neuro deficit present. Further testing is needed 4. Weak and painful: partial disruption of muscle-tendon unit. Pain response due to serious pathology or concurrent neurological deficit |
|
|
How can you differentiate the action of a one-joint muscle from that of a multi-joint muscle? |
place the multi-joint mm at a disadvantage -if a muscle that crosses two or more joints produces simultaneous movement at all of the joints it crosses, it soon reaches a length at which it cannot generate full mm force = active insufficiency |
|
|
What is active insufficiency? |
Decrease in torque produced by a muscle when the full ROM is attempted simultaneously at all joints crossed by the multi-joint mm ex: hand grasp with wrist in full flexion (limiting strength?) |
|
|
What is passive insufficiency? |
-when 2-joint or multi-joint muscles are of insufficient extensibility to allow full ROM to be produced simultaneously at all joints crossed by these muscles. -passive tension developed in these stretched muscles is sufficient to either cause motion or to limit motion: ex: cause motion: full wrist flexion causes fingers to extend due to insufficient length of finger extensors stretched over flexed wrist ex: limit motion: finger flexion with wrist flexion is limited by length of finger extensors; or -rectus femoris limits active knee flexion with hip extended -HS limits active knee ext if hip in position of flexion *Corey's a good example of this "passive insufficiency limiting motion" |
|
|
what are the MMT grades? |
Normal = 5/5 can move into test position against gravity with maximal resistance Good = 4/5 Same as normal but can only resist moderate pressure Fair + = 3+/5 Same as Good but can resist only mild pressure Fair = 3/5 full range against gravity, no resistance Fair - = 3-/5 Same as fair but gradual release against gravity Poor + = 2+/5 Moves against gravity in small ROM Poor = 2/5 Full ROM in gravity eliminated position Poor - = 2-/5 can only initiate ROM with gravity eliminated Trace = 1/5 Fasciculation or palpable mm contraction but unable to move Zero= 0 No visible or palpable mm contraction |
|
|
What are components of the Neurological examination? |
NURDS Neural tension Testing UMN test (Babinski and Clonus) Resisted muscle testing DTRs Sensation (dermatomes) |
|
|
Describe signs and symptoms that differentiate UMN vs LMN lesions |

|
|
|
When is further testing required during the sensory testing portion of the neurological exam? |
-if light touch is different between sides or there is a decr in LT over a specific area then further testing is required -such as pin prick (superficial pain), vibration, two-point discrimination, or proprioception |
|
|
What is the grading scale for DTRs? |
4+ = Hyperactive reflex with clonus (indicates UMN disorder) 3+ = Hyperreflexia (brisk): palpable (mod-strong) contraction with exaggerated joint movement (still within normal variation) 2+ = Normal = palpable ctx with visible extremity movement 1+ = hyporeflexia (sluggish) palpable mm ctx with no extremity movement (indicative of LMN disorder) 0 = Areflexia (absent) no visible or palpable mm ctx |
|
|
What is the purpose of neural tension tests? |
by stretching the peripheral nerves with specific body movements, the mobility of the spinal dura and nerve roots can be tested |
|
|
What (in general) nerve does the SLR test bias? What are the variations? |
sciatic nerve 1. Passive SLR with DF and eversion = tibial nn 2. Passive SLR with PF and inversion = peroneal nn 3. Passive SLR with DF and inversion = sural nn DET PIP DIS
|
|
|
What neural tension test biases the femoral nerve/ |
Prone knee bend |
|
|
What neural tension test biases the spinal dura? |
passive neck flexion |
|
|
How is ankle clonus test performed? |
Position leg in slight knee flexion and rapidly DF ankle (+) test if series of involuntary mm contractions |
|
|
how is the babinski test performed? |
stroke the plantar aspect of the foot from the lateral side of the heel to the base of the great toe with a blunt instrument (+) great toe DFs and other toes fan out |
|
|
What test should be performed before any manual treatment of the cervical spine? |
vertebral artery test and must be repeated as ROM increases |
|
|
What is the vertebral artery test? |

-assesses integrity of the vertebrobasilar vascular system -pt in supine and progress as below 1. extend head and neck for 30 secs. if no change progress to next step 2. extend head and neck with rotation left the for 30 sec then repeat with right rot for 30 sec (+) test provokes referring symptoms (Right rot will decr contralat artery and reproduce L symptoms and vice versa) - pt should report tinnitus, dizziness, nausea, throbbing, confusion, or unsual sensation. Clinician obesrves for pupillary constriction or dilation and nystagmus which indicate VA compression |
|
|
What should be done if the Vertebral artery test is positive? |
avoid mobilization and cervical spine movements into ext and rot at ranges that produce symptoms -notify physician of test findings |
|
|
What cervical motions test intervertebral foramen vs VA and vice versa? |
IVF: decreased space with extension (blood flow normal with isolated ext; IVF > dear on ipsilateral side) VA: ext + rot = bilat decr with > decr on contral side aa. |
|
|
What is the quadrant test for the cervical spine? |
= Spurling's test/foraminal compression (identifies compression of cervical nerve roots) -perform if pt c/o nerve root symptoms which are diminished or absent at time of exam (i.e. UE symptoms) -Spurlings: pt in sitting w/ head bent TOWARDS UNINVOLVED side; apply pressure straight down; repeat towards involved side.
|
|
|
Quadrant test and alternatives |
Maximum cervical compression test = (ext + rot + SB + compression) spurling's = foraminal compression (SB head to uninvolved side and add compression straight down. repeat on opposite side) |
|
|
How is Spurling's test performed and positive results? |
SB head to uninvolved side and add compression straight down. -repeat on opposite side (+) test = pain radiates into arm toward which head is side flexed which indicates pressure on a nerve root (cervical radiculitis) (-) = neck pain with NO radiating pain |
|
|
How is the maximum cervical compression test performed? |
aka maximum cervical compression test -identifies compression of neural structures at IVF and/or facet dysfunction - patient in sitting -passively move head into SB and rot toward non painful and add ext then compression (SRE is the order!) -repeat on painful side (+) = pain and/or paresthesia in dermatomal pattern on same side as SB and rot or localized pain in neck if facet dysfunction |
|
|
When is the distraction test indicated? |
when pt c/o radicular symptoms in hx and presents with radicular sx during the exam -indicates compression of neural structures at the IVF or facet joint dysfunction |
|
|
How to perform the distraction (cx) test? |

supine hold pt under chin and occiput and flex neck whiled distraction force of about 14 pounds applied (+) = decr in symptoms in neck (facet condition) or decr in UE pain (indicating nerve root compression) |
|
|
What is the purpose of Hautant's test? |
-to differentiate vascular vs vestibular causes of dizziness/vertigo |
|
|
Describe positive Hautant's test. |
2 steps 1. sitting with shoulders flexed to 90 and palms up. Have pt close eyes for 30 sec. If arms lose position = (+) vestibular condition 2. sitting with shoulders flexed to 90 and palms up. close eyes and have pt extend head and neck with R Rot and then L Rot holding in each for 30 sec. (+) for vascular cause if arms lose position *Think Haunted Haunt - arms out like a zombie only supine:)
|
|
|
What is the purpose of the transverse ligament stress test? |
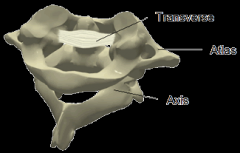
test integrity of tranverse ligament of C-spine -prevents anterior movement of atlas on axis and posterior movement of axis on atlas |
|
|
What is a positive test for transverse ligament stress test? |

-supine -head on table -glide C1 anterior Normal end feel = firm (+) = soft end-feel, dizziness, nystagmus, lump sensation in throat, nausea |
|
|
What is the purpose of the anterior shear test? |
assess integrity of upper c-spine ligaments and capsule |
|
|
how is anterior shear test performed and positive test? |
-supine with head on table -glide C2-C7 anterior normal end-feel = firm (+) = ligament laxity, dizziness, nystagmus, lump sensation in throat, nausea Much like the transverse ligament test only for C2-C7 instead of C1 |
|
|
What is positive Shoulder abduction test? |

(+) = decr in UE symptoms when pt places one hand on top of head Indicates compression of neural structures in IVF |
|
|
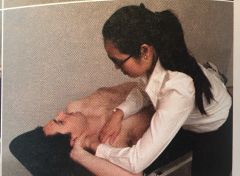
What is Lhermitte's sign? |

identifies dysfunction of SC and/or UMN lesion -long sitting -passively flex head and one hip while keeping knee in ext, repeat with other hip (+) pain down the spine and into upper or lower limb = indicates dural or meningeal irritation in spine or possible cervical myelopathy *Pic's not exact - but think Lhermitte the hermit has pain from his spine that radiculates |
|
|
What is the Romberg Test? |

standing close eyes for 30 seconds (+) for UMN lesion if excessive sway or lose of balance |
|
|
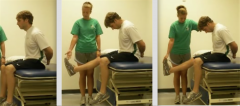
What is the standing flexion test? |
-tests iliosacral motion to determine joint dysfunction (motion restriction of innominate) -palpate both PSIS and ask pt to bend forward Normal = both PSIS move superior and anteriorly (+) side with motion restriction is the one that move furthers or first cranially and is considered blocked |
|
|
What is the slump test? |
- sitting on edge of table with knees flexed and hands behind back -pt slump sits while maintaining neutral head and neck. then add progressions below 1. passively flex pt head and neck. if no symptoms then 2. passively extend one of pt knees. If no sx then 3. Passively DF ankle of LE with extended knee Repeat on other side. if positioning reproduces patients symptoms and cervical ext relieves symptoms = (+) for increased tension in the neuromeningeal tract |
|
|
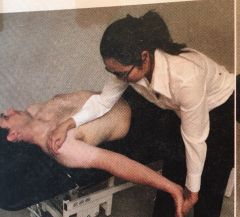
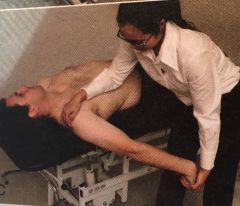
What is the Lasegue's test? |

aka SLR (with DF and Cx Flex) supine, passively flex hip of one LE with knee ext until pt complain of shooting pain into LE -slowly lower until pain subsides, then DF ankle -also can add neck flexion (+) = reproduction of pathological neurological symptoms when foot is DF and when neck flexed (+)= asymmetry between sides (+) = reproduction of sx between 35-70 deg hip flexion biases the sciatic and tibial nerves |
|
|
What is Cross (Well Leg) SLR? |
SLR on uninvolved reproduces patient's symptoms -one leg is lifted and pt c/o pain in opposite LE = indication of space-occupying lesion (e.g. herniated disc, large IV disc protrusion) -stretches ipsilateral and contralateral nerve root. |
|
|
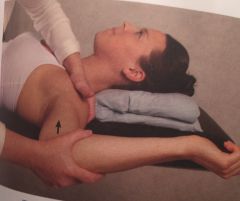
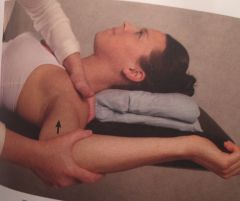
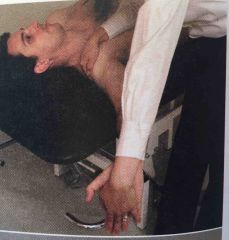
What is the femoral nerve traction test? |

identifies compression of femoral nerve anywhere along its course -sidelying on nonpainful side with unaffected knee and hip slightly flexed (painful side is up) -head/neck slighlty flexed -with affected knee in ext, extend the hip approx 15 deg -if no sx then flex knee (+) = neurological pain radiate down anterior thigh |
|
|
What is the lumbar quadrant test? |
identifies compression of neural structures at IVF and facet dysfunction 1. in standing, for IVF test: SB L, Rot L, and Ext = max closing of IVF on L 2. in standing for Facet dysfunction SB L, Rot R, and Ext = max compression of facets on L (Rot opposite for Facet) (+) = localized pain for facet dysfunciton pain &/or paresthesia in dermatomal pattern for the involved nerve root *With the IVF you want to clamp down on the foramina and with facet, you want to create shear which is why the only difference is rotation in the opposite direction |
|
|
What is the Prone knee bend test? |
aka femoral nerve stretch -used to identify L1-L3 nerve root lesion (also stretches femoral nn) -prone + passive knee flex + hip ex (+) for nerve root involvement = unilat pain in lateral or posterior aspect of hip, into lumbar spine, or into anterior thigh |
|
|
What is Stork standing test? |
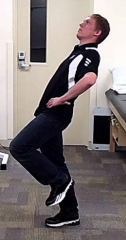
-identifies spondylolisthesis -stand on one leg + lumbar ext and repeat on opp leg (+) = LBP with ipsilateral LE on ground = unilat stress fracture of pars interarticularis "S" for Stork and Spondylolisthesis |
|
|
What is the Bicycle test of van Gelderen? |
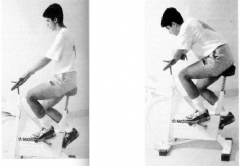
-identifies neurogenic claudication (spinal stenosis) vs intermittent claudication -ride stationary bike sitting erect and time how long can ride at set pace -repeat with slumped posture and time how long -spinal stenosis (+) if can ride longer in slumped posture or if reproduces sx in erect posture which are relieved with slumped posture |
|
|
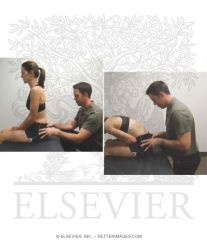
What is Gillet's test? |

-used to identify SI joint dysfunction -thumb on PSIS and other thumb on sacrum at same level -pt standing then asked to flex hip and knee on side you are palpating -PSIS should move inferiorly (+) = PSIS does not move or moves cranially which indicates ipsilateral motion restriction
If palpate PSIS on WBing side -innominate should rotate posteriorly (PSIS move inferiorly) (+) if PSIS on stance side moves cranially (ant rot) = decr motor control of lumbopelvic stabilizers |
|
|
What is Long-sitting test? |
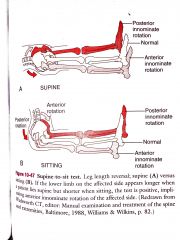
-measures functional leg length -ALS and SLP -determines if there is a posteriorly or anteriorly rotated innominate based on apparent leg length differences -if LE longer in supine but shorter in sitting = (+) anterior innominate rotation on affected side -if LE shorter in supine and appears longer in sitting = posterior innominate rotation *ALS and SLP |
|
|
What are the 5 test that indicate SIJ pain and how many have to be positive? |
3 out of 5 to indicate SIJ pain with high spec and sensitivity DT SCG 1. Distraction/Gapping 2. Thigh thrust 3. Gaenslen's test 4. Sacral thrust 5. Compression |
|
|
What is the distraction/gapping test? |

SIJ dysfunction (1 of 5 cluster of tests) -supine -cross arm pressure to bilat ASIS in down outward direction (+) = symptoms reproduced or increase in unilat gluteal or in posterior leg |
|
|
What is the thigh thrust test? |

SIJ dysfunction (1 of 5 cluster of tests) supine with hip flexed to 90 -push posteriorly directed force through femur (+) = Pain incr or reproduced on thrusting |
|
|
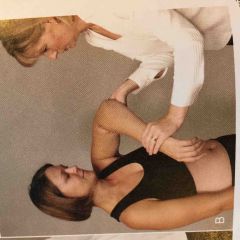
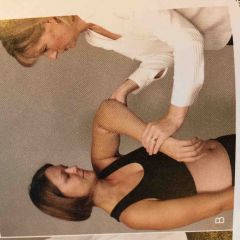
What is Gaenslen's test? |
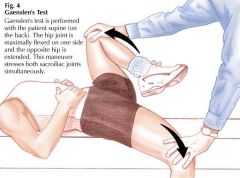
SIJ dysfunction (1 of 5 cluster of tests) supine near edge of the table with affected leg hanging over edge of table -other leg is flexed toward pt's chest -firm pressure is applied to both the hanging leg and the leg flexed toward the chest (+) = pain in the SIJ is reproduced or increased |
|
|
What is the sacral thrust test? |

SIJ dysfunction (1 of 5 cluster of tests) in prone, examiner applies a force vertically downward to the apex of the sacrum (+) = SIJ pain incr or is reproduced |
|
|
What is the compression test? |

SIJ dysfunction (1 of 5 cluster of tests) sidelying with affected side up hips are flexed approx 45 and knees flexed to 90 -vertically force applied downward on ASIS (+) = SIJ pain increases or is reproduced |
|
|
What is the sitting flexion test? |
-identifies SIJ dysfunction -Thumbs on PSIS in sitting -pt crosses arms over chest with feet on floor and bends forward bringing elbows between knees (+) = blocked joint moves first or further cranially |
|
|
What are the tests for impingement in shoulder? |
HNP Hawkins-Kennedy Neer's Painful arc |
|
|
What are the tests for RC dysfunction/pathology? |
BILS DIE Belly Press test Infraspinatus Muscle test Lift off test Supraspinatus muscle test Drop Arm Test IR Lag Sign ER Lag Sign
1. Supraspinatus muscle test (Empty Can Test)
2. Infraspinatus Muscle test (90 deg elbow flexion and humerus IR to 45 deg & apply medial rotation force while pt resists) * Think "I" for Infra and IR
3. Drop Arm Test (AB shoulder to 120 have to slowly lower)
4. ER Lag Sign (elbow/shoulder 90/90 w/ ER ask t to hold)
5. IR Lag Sign (same position as lift-off test -except arm is passively lifted off Low back and pt asked to hold position)
6. Lift off test (see above but actively lift arm away from body)
7. Belly Press test (pt presses belly while PT IRs at the elbow; if elbow springs back with release [+]) |
|
|
What are the special tests for AC joint dysfunction/ pathology? |
PROPH Paxinos Sign Resisted Horizontal Extension test O'Brien's Sign Palpation of the AC joint Horizontal Adduction test
1. Horizontal Adduction test (-sitting, passive forward shoulder flexion to 90 deg, then horizontally adduct arm as far as possible)
2. Resisted Horizontal Extension test (90 deg Flex and IR -examiner pushes elbow into horizontal add and pt pushes into horizontal and)
3. O'Brien's Sign (think of stopping traffic sign w/ PT pressing down and then with forearm supinated)
4. Paxinos Sign (think Pinch Test - examiner stands posterior to patient -thumb on posterior acromion; index and fingers over middle part of clavicle -thumb pushes anteriosuperiorly and fingers push inferior and posterior (+) = AC pain
5. Palpation of the AC joint |
|
|
What are tests for the GH labrum? |
BBC CORP Biceps Load I Test Biceps Load II Test Crank Test Compression Rotation Test O'Brien's Active Compression Test Resisted supination ER test Pain Provocation Test
1. Crank Test (Shoulder ABD in scap plane 160 deg and elbow 90 deg flexion -apply axial load through elbow while ER and IR humerus)
2. Biceps Load I Test (see future card w/ details)
3. Biceps Load II Test (see future card w/ details)
4. Pain Provocation Test (-arm abd to 90-100 deg and PT sup and pro forearm at wrist - (+) if pain more in pronation)
5. Compression Rotation Test - like crank but in supine and using axial compression at the elbow
6. O'Brien's Active Compression Test
7. Resisted supination ER test (supine with scapula near edge of table -examiner holds arm at elbow and hand -90 abd, 65 deg elbow flexion, forearm neutral or slight pronation -ask pt to max supinate hand while examiner resists -while pt continues to supinate, examiner ER shoulder to ER (+) = anterior or deep shoulder pain, clicking or catching in shoulder, or reproduction of symptoms (-) = posterior shoulder pain, no pain, or apprehension)
|
|
|
What are special test for cubital tunnel syndrome? |
PFT Pressure provocative test Flexion Test Tinel's sign
1. Pressure provocative test - with elbow at 20 deg - apply pressure to the cubital area for 60 sec.)
2. Flexion Test (fully flex elbow with wrist extension and shoulder girdle 90 deg abd and depression & hold for 3-5 min (+) = tingling or paresthesia in ulnar nerve distribution of forearm and hand =cubital tunnel syndrome - think "I don't know" for arm/hand position)
3. Tinel's sign - tap region where ulnar nn passes through cubital tunnel |
|
|
What are special tests for MCL tears at the elbow? |
1. Valgus stress at 30, 60, 70, 90 deg of elbow flexion 2. Moving Valgus Stress Test
1. Valgus stress at 30, 60, 70, 90 deg of elbow flexion ( -stabilize arm with one hand at the elbow, other hand is place above the wrist -an abduction or valgus force (pushing wrist laterally/toward thumb) is applied to distal forearm while the ligament is palpated at the elbow -do at 30, 60, 70, and 90 deg of elbow flexion (+) = laxity, decreased mobility, or pain)
2. Moving Valgus Stress Test ( arm abducted and elbow full flexed -while examiner maintains valgus stress at the hand, the examiner quickly extends the elbow (+) = reproduction of pain between 70-120 deg = partial tear of MCL) |
|
|
What are special tests for lateral epicondylitis? |
1. Tennis Elbow Test 2. Mill's Test
1. Tennis Elbow Test (like revving a motor cycle with resistance to wrist ext) -elbow stabilized by examiner. Pt. asks to make a fist, pronate forearm, and radially deviate and extend the wrist while examiner resists the motion (+)= pain over lateral epicondyle 2. Mill's Test - elbow ext with full wrist flex (& OP) 3. Resist extension of the 3rd digit distal to the PIP (stressing ED (+) = pain over lateral epicondyle |
|
|
What are special tests for wrist and hand ligamentous instability? |
1. Thumb Ulnar Collateral Ligament Test 2. Test for Tight Retinacular Ligaments 3. Lunatetriquetral ballottement test
|
|
|
What are special tests for integrity of wrist and hand tendons and muscles? |
1. Finkelstein's Test 2. Sweater finger sign for rupture of the FDP tendon 3. Bunnel-Littler Test
1. Finkelstein's Test (pt makes a fist with the thumb inside the fingers -examiner stabilizes forearm and deviates wrist toward ulnar side)
2. Sweater finger sign for rupture of the FDP tendon - inability to close finger into a fist
3. Bunnel-Littler Test (1. hold MCP in max ext (intrinsics stretched) then passively flex PIP 2. Then hold MCP in flexion and passivley flex PIP (+) = if PIP flex is greater with MCP flexion then intrinsics are tight) |
|
|
What are tests for neurological dysfunction in the wrist and/or hand? |
1. Tinel's sign 2. Phalen's test (DOWN) 3. Reverse Phalen's Test (UP) 4. Carpal Compression Test 5. Froment's Sign (aka paper sign) |
|
|
What are special tests for circulation in the wrist and hand? |
1. Allen's test - diminished pulse with shoulder/elbow 90/90 and patient looking to opposite side 2. digit blood flow (nail bed compression) |
|
|
What are special tests of hip pathology? |
1. Patrick's (FABER) test (Piriformis) 2. Flexion Adduction IR (FADIR) Impingement Test (anterior impingement / anterior hip pain) 3. Scour Test (hip OA) 4. Trendelenberg Sign |
|
|
What are Ligamentous test of the knee? |
1. Lachman's Test 2. Anterior Drawer Test 3. Pivot-Shift Test 4. Valgus Stress Test 5. Varus Stress TEst 6. Posterior Drawer
1. Lachman's Test (Anterior Drawer test in 30 deg. knee flexion - ACL)
2. Anterior Drawer Test (ACL)
3. Pivot-Shift Test (hip 30 deg, knee ext>IR tib/fib w/ axial load & val force and knee flex - ACL)
4. Valgus Stress Test (MCL- ab hip flex knee to 30 deg. & add valgus stress)
5. Varus Stress Test (LCL- same as above but add various stress)
6. Posterior Drawer (PCL) |
|
|
What are tests for Meniscus in the knee? |
1. McMurray's Test 2. Apley Test 3. Thessaly Test 4. Bounce Home Test 5. Joint Line Tenderness
1. McMurray's Test (Supine, knee fully flex., IR & ext. (valgus stress) for Lat. Men / ER & ext. (varus stress) for Med. Men 2. Apley Test (like scour only prone, using distraction, and compression, & for knee not hip) 3. Thessaly Test (SLS w/ rotation) 4. Bounce Home Test (hold post ankle and knee with knee flexed and then drop hand from behind knee) 5. Joint Line Tenderness |
|
|
What are tests for patellar instability? |
Patellar apprehension test (30 deg. knee flex. PT applies lateral pressure to patella [+] if quad contracts and pt looks apprehensive) |
|
|
What are tests for Patellofemoral syndrome? |
1. McConnell Test 2. Passive Patellar Tilt Test 3. Clarke's Sign (Patellar compression test)
1. McConnell Test (using quads resist knee flex in sitting at 120 deg, 90 deg, 60 deg, full ext. for 10 sec. hold ea. - pain at any point passively bring knee to full ext. then medially displace patella while flexing knee to point where pain was felt - if pain dec. this is a [+] sign)
2. Passive Patellar Tilt Test (supine w/ knee ext. elevate lateral boarder and depressing med boarder. 15 deg normal; < hypomobile & > hypermobile
3. Clarke's Sign (Patellar compression test) hold patella superiorly w/ downward pressure & have pt contract quads) |
|
|
What are tests for IT band friction syndrome? |
Noble compression test (supine with PT's thumb over lateral femoral epicondyle, flex knee to 90 and ext [+] with pain under pts thumb) |
|
|
What are tests for ligamentous instability at the ankle? |
1. anterior drawer test 2. Talar tilt 3. Squeeze test for syndesmosis injury
1. anterior drawer test (ant. talo-fibular ll - knee at 90 anke relaxed at 20 PF) 2. Talar tilt (long sitting PT holds ant distal tib and talus tilting into ad (pain=calcanea fibular ll; abd =deltoid ll) 3. Squeeze test for syndesmosis injury (interlock fingers or push hands together and squeeze tib/fib together) |
|
|
What is the the test for Achilles rupture? |
Thompson's test (pt prone with feet over end of plinth; squeeze gastric/soleus mm belly - intact tendon causes PF) |
|
|
What are the movement tests, postural analysis findings and example for an anterior innominate rotation - pelvic girdle dysfunction/ |
Direction of motion restriction = posterior rotation Movement test: Standing flexion test Long sitting test Posture Analysis: -Iliac Crest/PSIS high, ASIS low in standing -ASIS low in supine -supine length length longer -sitting length length shorter example: L anterior innominate (+) standing flexion and long sitting tests on the L L PSIS high, L ASIS low in standing L leg longer in supine L leg shorter in long sitting |
|
|
What are the movement tests, postural analysis findings and example for an posterior innominate rotation - pelvic girdle dysfunction/ |
Motion Restriction = Anterior rotation Movement Test: Standing flexion test Long sitting test Postural Analysis: ASIS higher, PSIS lower in standing Supine leg length shorter Long sitting leg length longer Example: Left Posterior Innominate (+) standing flexion and long sitting tests on L = L ASIS high, PSIS low in standing L leg shorter in supine L leg longer in long sitting |
|
|
What is innominate upslip definition? |
vertical shear of an entire innominate in which the ASIS and iliac crest are up in comparison to the opposite side innominate (ASIS and PSIS on one side will be higher than opposite side) |
|
|
What are the movement tests, postural analysis findings and example for an upslip of innominate - pelvic girdle dysfunction/ |
Movement Test: Standing Flexion Test Postural analysis: -ASIS and PSIS higher than contral side in standing supine and long sitting leg length shorter than other side Example: Left upslip innominate L PSIS and ASIS higher in standing L leg shorter in supine and long sitting |
|
|
What are the movement tests, postural analysis findings and example for a forward or backward sacral torsion - pelvic girdle dysfunction/ |
Movement Test: Sitting flexion test Postural Analysis: -Sacral sulcus (base of sacrum and ilium) deep (in prone) & sacral inferior lateral angle (near apex) (ILA) posterior and down (shallow) on opposite side example: forward or backward torsion Sitting flexion test (+) on Right Sacral sulcus deep on R and ILA posterior on L = L rotation of sacrum on R oblique axis (see notes and print out) |
|
|
How are sacral torsions named? |
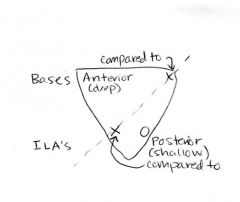
Sitting flexion test: the (+) side is the hypomobile side. Opposite side is considered axis (so if L side is (+) then axis is R -draw the upside down triangle put (+) for the ILA or sulcus that is palpated as more deep/anterior and negative for the opposite side that is more posterior/shallow -if the (+) is at the base/sulcus of sacrum then rotation is the same as the axis so, for example, it would be R rotation on R axis. -if the (-) is at the base/sulcus, then rot is opposite to axis so would (-) on L base would be L rot on R axis |
|
|
What is Yergason's special test? |

-test for biceps muscle pathology (tendonosis/tendonopathy)/integrity of transverse ligament which holds biceps tendon in the bicepital groove -sitting with shoulder in neutral and elbow flexed to 90 and stabilized against trunk with forearme pronated -examiner resists supination with ER -tendon of long head of biceps will pop out of groove if transverse humeral ligament is torn -tenderness/pain without dislocation indicates bicipital tendionpathy |
|
|
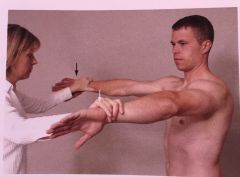
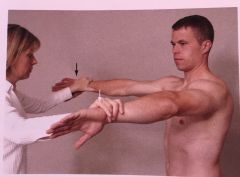
What is Speed's Test? |
-identifies bicipital tendonosis/tendonopathy -sitting or standing -UE full ext and forearm supination resist shoulder flexion. Repeat with forearm in pronation -can also do with shoulder at 90 deg flexion and push into ext -->eccentric biceps contraction -do in supination and pronation (+) = increased tenderness in bicipital groove/long head of biceps tendon esp with supination position |
|
What test is this ? |
Speed's Test for biceps tendinopathy |
|
|
What is the Neer's Test? |

-to identify impingement of long head of biceps and supraspinatus tendon under the acromion -sitting -shoulder passively IR then fully abducted (+) reproduces pain in shoulder |
|
What test is this? |
Neer's test for impingement of Biceps tendon and supraspinatus |
|
|
What is the Hawkins-Kennedy Test? |
-identify impingement of supraspinatus -standing -passive forward shoulder flexion to 90 deg -then forcibuly IR the shoulder (+) = pain indicating supraspinatus tendinosis/tendinopathy |
|
What test is this? |
Hawkins-Kennedy Test for shoulder impingement |
|
|
What is the supraspinatus test? |
"empty can" test -identifies tear and or impingement of supraspinatus tendon or possible suprascapular nerve neuropathy -90 deg of shoulder abduc and neutral rotation. Resist abduction -then medially rotate shoulder and horizontal add 30 deg (so in plane of scapula and thumbs point down). Resist abd (+) = weakness or pain indicating SPST or subscap neuropathy |
|
What test is this? |
Supraspinatus ("Empty Can") Test to test for impingement of supraspinatus tendon or subscap neuropathy |
|
|
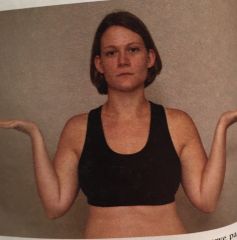
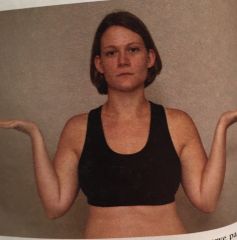
What is the infraspinatus Test? |
-to identify IFST strain arm at side with 90 deg elbow flexion and humerius IR to 45 deg -apply medial rotation force while pt resists (+) pain or weakness = IFST strain |
|
What test is this? |
Infraspinatus test to identify IFST strain |
|
|
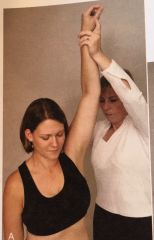
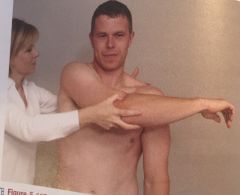
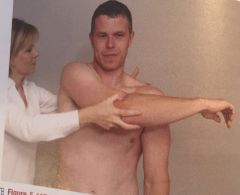
What is the Drop-Arm Test? |
-identify RC tear -examiner abducts arm to 120 deg and then asks pt to slowly lower the arm to the side (+) = pt unable or has severe pain when attempting and indicates tear in RC |
|
What test is this? pg 334 |
Drop-Arm Test to identify RC tear |
|
|
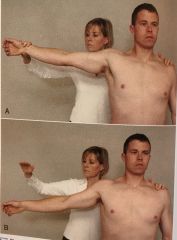
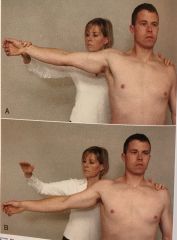
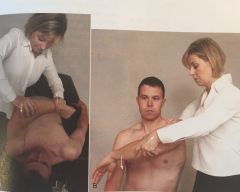
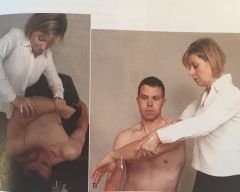
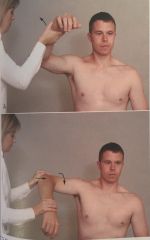
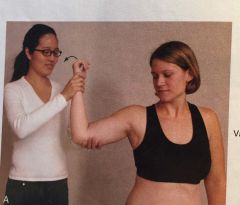
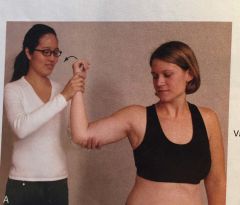
What is the External Rotation Lag sign? |

-identify IFST and Teres minor weakness or IFST or SPST tears -Passive abduction of shoulder to 90 deg with elbow in 90 deg flexion. -passively ER shoulder to end range. -ask pt to hold (+) = cannot hold position/hand springs forward/arm drops into medial Rot = weakness or tear of IFST and/or supraspinatus pg 336 |
|

What is this test? |
ER Lag Sign/Test indicating weakness or tear of IFST and/or supraspinatus |
|
|
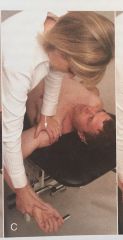
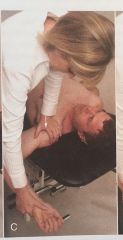
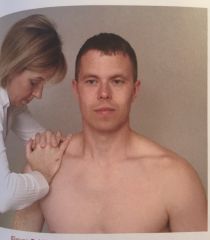
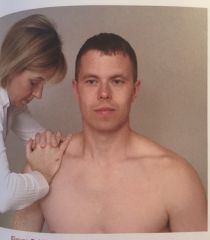
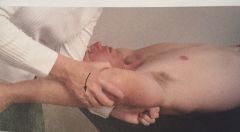
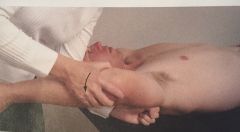
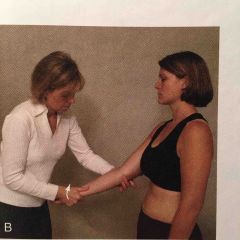
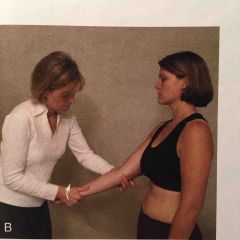
What is the IR Lag sign? |

-identifies subscapularis tear or weakness -same position as lift-off test -except arm is passively lifted off Low back and pt asked to hold position (+) = hand moves toward the back/cannot hold position indicating weakness or pain in SUBscap |
|

what test is this? |
IR Lag sign identifies subscapularis tear or weakness |
|
|
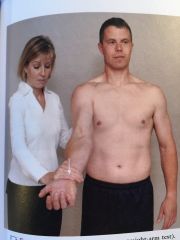
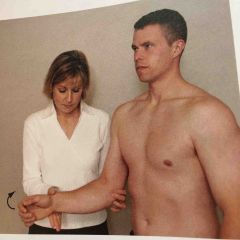
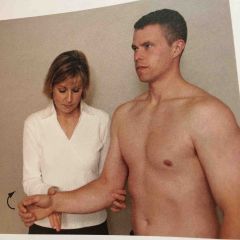
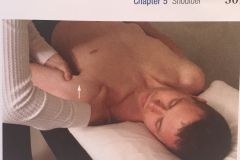
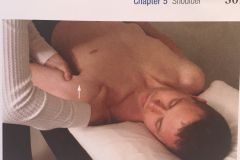
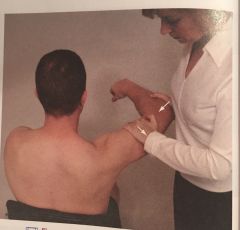
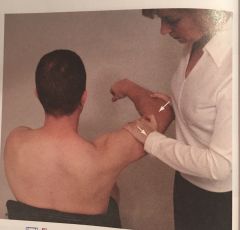
What is the lift off test? |
-dorsum of hand on back pocket or against midlumbar spine. -pt lifts hand away from back (+) = inability to lift hand away indicating lesion of subscapularis mm
|
|
|
What is the sulcus sign? |
-test for inferior shoulder instability -standing with arm by side and shoulder mms relaxed -grasp forearm below elbow and pull arm distally (+) = space between inferior margin of acromion and humeral head but only positive if pt is symptomatic (pain/ache on activity, or shoulder does not "feel right" with activity) -indicates inferior instability or glenohumeral laxity +1 = <1 cm +2 = 1-2 cm +3 = >2 cm |
|

What test is this? |
Sulcus sign indicating inferior shoulder instability or GH laxity |
|
|
What is the Anterior Apprehension Test? |

-identifies past history of anterior dislocation of shoulder -pt supine with shoulder in 90 deg abd. -slowly passively ER shoulder (+) = pt looks or feels apprehensive or alarmed and resists further motion (also may state that it feels like what it felt like when shoulder dislocated |
|

What test is this? |
Anterior Apprehension Test for anterior shoulder instability |
|
|
What is the Relocation Test for shoulder? |
test for anterior shoulder instability -during end of Anterior apprehension test (90 deg abd with elbow flex to 90 and max ER) -apply posterior translation stress to the head of the humerus (+) = apprehension and pain decr indicating GH instability, subluxations, or dislocation |
|
What test is this? |
Relocation test for anterior shoulder instability |
|
|
What is the anterior drawer test of the shoulder? |
testing for anterior shoulder instability -pt in supine, shoulder abducted 80-120, fwd flexed 20 deg, and ER up to 30 deg -stabilize scapula with opposite hand, pushing spine of scapula forward with index and middle finger and thumb on coracoid process -using arm closest to pt's feet, place hands around upper arm and draw humerus forward (+) = click, apprehension or both indicating anterior instability |
|
What test is this? |
Anterior Drawer test for anterior instability of the shoulder |
|
|
What is the Jerk test for the shoulder? |
test for posterior instability -pt in sitting with arm IR and forward flexed to 90 deg -examiner grasps elbow and axially loads humerus in proximal direction -maintaining axial loading, move arm into horizontal adduction across body (+) = sudden jerk or cluck as humeral head slides off the back of the glenoid. When arm is returned to original 90 deg abd, 2nd jerk as head reduces = posterior instability |
|
What test is this? |
Jerk test for posterior shoulder instability |
|
|
What is the Posterior Apprehension Test? |
-identifies posterior instability of shoulder -in sitting or supine -elevate shoulder in plane of scap to 90 deg while stabilizing scapula -apply posterior force through elbow -maintain axial load and horizontally adduct and IR arm. (+) = look of apprehension or alarm and resistance to motion or reproduciton of symptoms -normal is translation of 50% of HH diameter or less movement of HH posteriorly more than 50% of diameter = posterior instability |
|
What test is this? |
Posterior Apprehension Test for posterior shoulder instability |
|
|
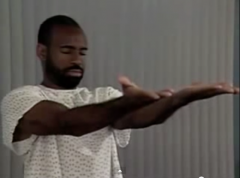
What is the AC Horizontal Adduction Test? |
-identifies dysfunciton of AC joint -sitting, passive forward shoulder flexion to 90 deg, then horizontally adduct arm as far as possible (+) = localized pain over AC joint |
|
What test is this? |
AC Horizontal Adduction test for AC joint dysfunction |
|
|
What is the AC Shear Test? |
-identifies AC joint dysfunction (e.g. arthritis, separation) -in sitting -examiner cups his/her hands over deltoid mm with one hand on clavicle and one on spine of scap -squeezes heels of hands together (+) = abnormal mvmt and/or pain |
|
What test is this? |
AC Shear Test for AC joint dysfunction |
|
|
What is AC Resisted Horizontal Extension Test? |
-test for AC joint dysfunction -90 deg Flex and IR -examiner pushes elbow into horizontal add and pt pushes into horizontal abd (+) = AC pain |
|
What test is this? |
AC Resisted Horizontal Extension Test |
|
|
What is the O'Brien's Sign? |
finding from Active Compression Test of O'Brien that indicates AC joint pathology -Active Compression Test of O'Brien typically for identifying of Labral lesions -standing position -90 deg flexion, full elbow ext -10-15 deg Horizontal ADD, full IR -examiner stands behind and applies downward force to arm at wrist -arm returned to start position and repeat with palm supinated and resistance is applied (+) for AC joint pathology = pain over AC joint (+) for labral lesion = pain on GH joint line or painful clicking inside shoulder in first part and eliminated or dec in 2nd part |
|
What test is this? |
Active Compression Test of O'Brien for labral lesions or AC joint dysfunction |
|
|
What is Paxinos Sign? |
identifies AC joint dysfunction -examiner stands posterior to patient -thumb on posterior acromion -index and fingers over middle part of clavicle -thumb pushes anteriosuperiorly and fingers push inferior and posterior (+) = AC pain |
|
What test is this? |
Paxinos Sign for AC joint pathology |
|
|
What is the Crank Test? |

identify Glenoid Labral lesion/tear supine or sitting -Shoulder ABD in scap plane 160 deg and elbow 90 deg flexion -apply axial load through elbow while ER and IR humerus (+) = pain on rotation with or without a click or reproduction of pt's symptoms (e.g. catching sensation) |
|
What test is this? |
Crank Test for glenoid labral tear/lesion |
|
|
What is the Clunk Test? |
-testing for glenoid labral tear -supine -one hand on posterior aspect of HH -other holds humerus above elbow -fully abduct shoulder -push anteriorly with hand over HH while other hand rotates humerus into ER -can vary ABD by moving arm in different abd degrees while maintaining ER (+) = clunk or grinding sound = tear of labrum |
|
What test is this? |
Clunk Test for glenoid labral tear |
|
|
What is the Biceps Load Test I? |
-to detect Glenoid Labral lesion -supine or sitting -shoulder 90 deg abd -90 elbow flexion -axial compression through elbow -while maintaining axial load, arm elevated diagonally upward while other hand applies downward and backward force to proximal arm (+) = sudden onset of posterior shoulder pain and click = posterioinferior labral lesion |
|
|
What is Biceps Load Test II? |

same as Biceps Load test I but 120 deg of abd -to detect Glenoid Labral lesion -supine -shoulder 120 deg abd -90 elbow flexion -full ER or until apprehension -ask pt to flex elbow while resisting at wrist (-) for SLAP lesion= with resisted elbow flexion, apprehension decr or pt feels more comfortabel (+) for SLAP lesion = apprehension remains the same or shoulder becomes more painful
|
|
What test is this? |
Biceps Load Test I for labral lesion |
|

what test is this? |
Biceps Load Test II for SLAP lesions |
|
|
What is the Pain provocation test of shoulder? |
-to identify superior labral lesion (SLAP) sitting -arm abd to 90-100 deg -ER arm by holding wrist -take forearm into max supination and pronation (+) = pain is provoke only in pronated position or more sever in pronated position = (+) for superior tear (SLAP) |
|
What test is this? |
Pain Provocation Test for superior tears of glenoid labrum (SLAP) |
|
|
What is the compression rotation test of the shoulder? |
-to test for glenoid labral tear -supine -passive shoulder abd 20-90 deg -90 deg elbow flexion -axial compression through elbow (pushing up through the elbow) while passively rotating humerus back and forth (+) = pain, clicking or catching sensation = torn labrum |
|
What test is this? |
Compression Rotation Test for glenoid labral tear |
|
|
What is O'Brien's Active Compression Test? |
finding from Active Compression Test of O'Brien that indicates AC joint pathology -Active Compression Test of O'Brien typically for identifying of Labral lesions -standing position -90 deg flexion, full elbow ext -10-15 deg Horizontal ADD, full IR -examiner stands behind and applies downward force to arm at wrist -arm returned to start position and repeat with palm supinated and resistance is applied (+) for AC joint pathology = pain over AC joint (+) for labral lesion = pain on GH joint line or painful clicking inside shoulder in first part and eliminated or dec in 2nd part |
|
|
What is the Resisted Supination External Rotation Test? |

-to check for SLAP lesions -supine with scapula near edge of table -examiner holds arm at elbow and hand -90 abd, 65 deg elbow flexion, forearm neutral or slight pronation -ask pt to max supinate hand while examiner resists -while pt continues to supinate, examiner ER shoulder to ER (+) = anterior or deep shoulder pain, clicking or catching in shoulder, or reproduction of symptoms (-) = posterior shoulder pain, no pain, or apprehension |
|

What test is this? |
Resisted Supination External Rotation Test for identifying SLAP lesions |
|
|
What is the elbow flexion test? |
--to identify cubital tunnel (ulnar nerve) syndrome -fully flex elbow with wrist extension and shoulder girdle 90 deg abd and depression -hold for 3-5 min (+) = tingling or paresthesia in ulnar nerve distribution of forearm and hand =cubital tunnel syndrome |
|
What test is this? |
Elbow Flexion test for cubital tunnel syndrome |
|
|
What is the Lateral Grip Test? |
test for median nn entrapment (anterior interosseous nn.) -ask pt to pinch tips of index and thumb togther (make OK sign) -pt is unable to meet tip to tip and has an abnormal pinch of the index finger and thumb = (+) for pathology to ant interosseous nn., possibly entrapment as it passes between the 2 heads of pronator teres mm. |
|
|
What is Tinel Sign at the Elbow? |
-tap ulnar nn in the groove between the olecranon process and medial epicondyle (+) = tingling sensation in ulnar distribution of forearm and hand distal to point of compression |
|
|
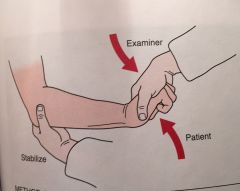
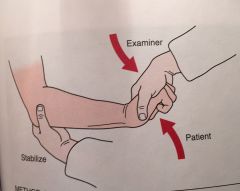
What is the Valgus stress test for the elbow |
-tests for valgus instability (MCL tears) -stabilize arm with one hand at the elbow, other hand is place above the wrist -an abduction or valgus force (pushing wrist laterally/toward thumb) is applied to distal forearm while the ligament is palpated at the elbow -do at 30, 60, 70, and 90 deg of elbow flexion (+) = laxity, decreased mobility, or pain |
|
What test is this? |
Valgus Stress test for MCL of the elbow (valgus instability)
|
|
|
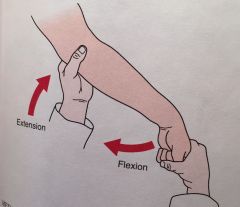
What is the Moving Valgus Stress Test? |
-identifies partial tear of MCL standing or supine with arm abducted and elbow full flexed -while examiner maintains valgus stress at the hand, the examiner quickly extends the elbow (+) = reproduction of pain between 70-120 deg = partial tear of MCL |
|
What test is this? |
Moving Valgus Stress Test for elbow MCL tear |
|
|
What is the test for pronator teres syndrome? |
sitting with elbow flexed to 90 deg -examiner resists pronation as the elbow is extended (+) = tingling or paresthesia in the median nn distribution of the hand and forearm = median nn entrapment |
|
|
What is tennis elbow test? |
3 tests 1. elbow stabilized by examiner. Pt. asks to make a fist, pronate forearm, and radially deviate and extend the wrist while examiner resists the motion (+)= pain over lateral epicondyle 2. Mill's Test 3. Resist extension of the 3rd digit distal to the PIP (stressing ED (+) = pain over lateral epicondyle |
|
What test is this? |
Tennis Elbow Test 1 |
|

What Test is this? |
Tennis Elbow Test 3 |
|
|
What is the Mill's Test? |
variation of tennis elbow test -while palpating lateral epicondlye, passively pronate forearm, flex wrist and extend the elbow (+) = pain over lateral epicondyle (may also be radial nerve compression) |
|

What test is this? pg. 409 |
Mill's Test for lateral epicondylitis |
|
|
What is Golfer's Elbow Test? |
test for medial epicondylitis -palpate medial epicondyle, while passivley supinate forearm and extending elbow and wrist (+) = pain over medial epicondyle |
|
|
What is the Thumb Ulnar Collateral Ligament Laxity Test? |
-test for tears of Ulnar collat ligament -examiner stabilizes 1st metacarpal -takes thumb into extension -and applies valgus stress to MCP (pushing proximal phalange of thumb laterally) (+) for complete tear of ulnar collateral = >30-35 deg valgus movement (+) for partial tear is <30-35 deg but > norm of 15 deg & > unaffected side |
|
What Test is this? |
Thumb Ulnar Collateral Ligament Laxity Test (test for gamekeeper's or skier's thumb |
|
|
What are the finger coupled actions? |
1. Active ext of PIP accompanied by ext of DIP (ORL stretched by PIP ext bc volar to PIP joint but ORL attaches dorsally to DIP causing ext of DIP) 2. Active or passive flexion of DIP accompanied by flexion of PIP (passive tension at distal site of ORL attachment transmits passive flexor force to proximal site of ORL that is volar to PIP axis) 3. Full flexion of PIP prevents DIP from being actively extended (loss of tension of terminal tendon and ORLs eliminating extensor force) |
|
|
What is the test for tight retinacular ligaments in the hand? |
-test for oblique retinacular ligament tightness to help determine whether DIP flexion restriction is due to ORL tightness or joint contracture -with PIP held in neutral (ORL lengthened), passively flex DIP -if DIP does not flex, ORL or PIP capsule are tight -next, hold PIP in flexion and passively flex DIP -greater DIP flexion when PIP flexed (ORL on slack) than when PIP extended = ORL tight |
|
|
What is the Lunotriquetral Ballottement TEst? |
-test to determine integrity of the lunotriquetrum ligament -grasp triquetrum between thumb and 2nd finger of one hand and the lunate with thumb and 2nd finger of other hand. -move the lunate up and down (ant and post) (+) for lunotriquetral instability = laxity, crepitus, or pain |
|
|
What is Finkelstein's Test? |
-used to determine the presence of de Quervain or Hoffmann disease, a paratenonitis in the thumb. -pt makes a fist with the thumb inside the fingers -examiner stabilizes forearm and deviates wrist toward ulnar side. (+) = pain over APL and EPB tendons at wrist and = paratenonitis of these 2 tendons. Compare to normal side bc can cause discomfort in normal individuals as well. |
|
|
What is sweater finger sign? |
-test for FDP rupture -ask pt to make fist -if distal phalanx of one finger does not flex = (+) for ruptures FDP |
|

What test/sign is this? |
sweater finger sign for FDP rupture |
|
|
What is the Bunnel-Littler Test? |
-test for tightness of hand intrinsic and extrinsic muscles 1. hold MCP in max ext (intrinsics stretched) then passively flex PIP 2. Then hold MCP in flexion and passivley flex PIP (+) = if PIP flex is greater with MCP flexion then intrinsics are tight
If PIP flexion is still limited with MCP flexion (i.e. if MCP position does not change PIP flexion) then indicates tight joint capsule
-for extrinsic mm tightness testing same procedure as above but PIP flexion will be greater with MCP extension (extrinsics on slack/finger extensors are not stretched as much) |
|
|
What is Phalen's Test? |
-flex the wrist maximally and hold for one min but pressing them together at wrist (+) = tingling in thumb, 2nd and 3rd digit and lat half of 4th indicating pressure on median nn in carpal tunnel |
|
|
What is Reverse Phalen's test |
-extend wrist in prayer position and bring down toward waist keeping palms in full contact. hold for 1 min (+) = same symptoms as Phalen's test and indicates median nn compression |
|
|
What is the Carpel Compression Test? |
- to identify CTS -examiner holds the supinated wrist in both hands and applies direct pressure over median nn in carpal tunnel for up to 30 sec. (+) = production of pt's symptoms |
|
|
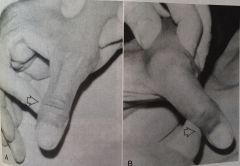
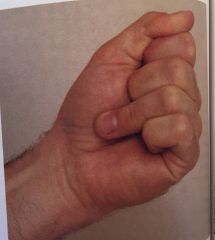
What is Froment's Sign? |
-paper sign (aka) -test for ulnar nerve palsy -pt attmpets to grasp piece of paper between thumb and index finger (+) = when examiner pulls paper away, terminal phalanx of thumb flexes due to paralysis of adductor pollicis (FPL is intact due to innervation from median nn) this indicates ulnar nerve paralysis |
|
|
What is Allen's Test? |
test for circulation in hand -pt asked to open and close hand several times as quickly as possible and then squeeze hand tightly -examiner's thumb and index finger placed over radial and ulnar arteries compressing them -pt opens hand while pressure maintained over arteries -one artery tested by releasing pressure over artery to see if the hand flushes -repeat to test other artery
|
|
|
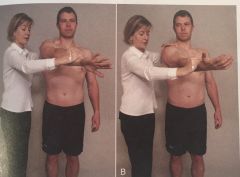
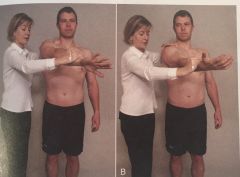
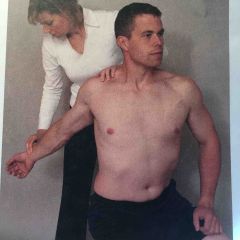
What is Adson's Test? |
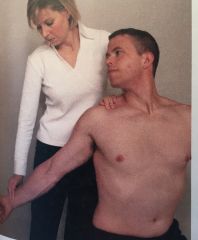
test for Thoracic outlet syndrome -locate radial pulse -pt head is rotated to face the test shoulder --pt extends head while examiner ER and extends shoulder -pt instructed to take deep breath and hold it (+) = disappearance of pulse pg 345 |
|
|
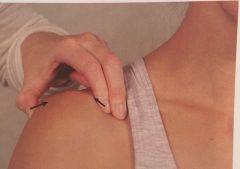
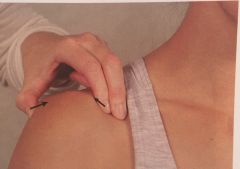
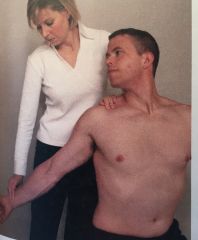
What is Costoclavicular syndrome test? |
aka Military brace -test for TOS -find radial pulse -examiner draws shoulder down and back (+) = disappearance of pulse
|
|
What test is this? |
Costoclavicular syndrome test for TOS pg. 345 |
|
What test is this? |
Adson's Test for TOS pg 345 |
|
|
What is the Roos Test? |
aka Elevated arm stress test (EAST) -pt stands and abducts arm to 90, ER shoulder, elbow flexion 90 deg -pt opens and closes hands slowly for 3 min (+) = pt unable to keep arms in position for 3 min or has ischemic pain, heaviness or profound weakness of arm, or numbness and tingling of the hand |
|
|
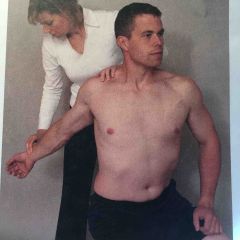
What is Wright Test? |
aka Hyperabduction test test for TOS -find radial pulse -max ABD and ER of shoulder -take a deep breath and then rotate head away from test side (+) = pulse disappears or neurological symptoms are reproduced |
|
|
What is Allen's Manuever for TOS? |

-find radial pulse -90 deg ABD, ER, and elbow flexion -pt rotates head away from test side (+) = pulse disappears when head is rotated pg 347 |
|
What test is this? |
Wright (Hyperabduction) test for TOS |
|

What test is this? |
Allen's Test for TOS |
|
|
What is the order for Upper limb neuro tension test 1? |
Shoulder depression and 110 deg abd Elbow ext Forearm supination wrist ext finger and thumb ext Cervical spine contralat side flexion |
|
|
what nerve does the ULNT1 bias? |
median nerve anterior interosseous nn C5, C6, C7 |
|
|
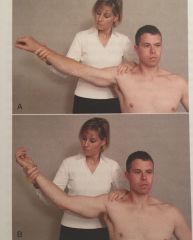
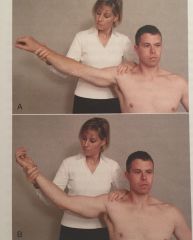
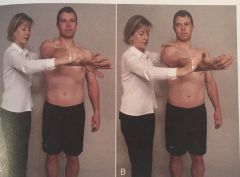
What is the order for ULNT2? |
Shoulder depression and 10 deg ABD Elbow ext Forearm supination wrist ext finger and thumb ext shoulder ER cervical contral side flexion |
|
|
What nerve does ULTT 2 bias? |
median nn musculocutaneous nn axillary nn
|
|
|
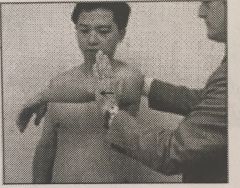
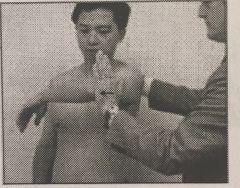
What is the order for ULNT3? |
Shoulder depression and 110 Deg abd Elbow ext forearm pronation wrist flexion and ulnar deviation finger and thumb flexion Shoulder IR cervical contralat side flexion |
|
|
What nerve does ULNT 3 bias? |
radial nn |
|
|
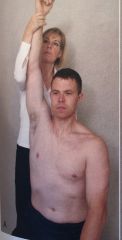
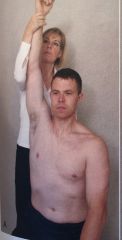
What is the order for ULNT 4? |
extend wrist and radially deviate extend fingers supinate or pronate forearm fully flex elbow depression shoulder ER shoulder shoulder abd (10-90 deg, hand to ear)
|
|
|
What nerve does the ULNT4 bias? |
ulnar nn C8 and T1 nerve roots |
|
What test is this? |
ULNT 1 - median nn bias median nerve anterior interosseous nn C5, C6, C7 |
|
What test is this? |
ULNT 2 median nn musculocutaneous nn axillary nn
|
|
what test is this? |
ULNT 3 radial nn bias |
|
what test is this |
ULNT4 ulnar nn |
|
|
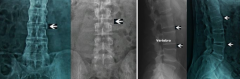
Spondylitis vs Spondylosis vs Spondylolysis vs Spondylolisthesis |
-(Ankylosing) spondylitis: an inflammatory disease that can cause some of the vertebrae in your spine to fuse together -Spondylosis: general term for age-related wear and tear affecting the spinal disks -Spondylolysis: stress fracture of the pars interarticularis -Spondylolisthesis: the forward displacement of a vertebra, especially the fifth lumbar vertebra, most commonly occurring after a break or fracture (can be slippage from 25% to 100%). Spondylolysis and spondyolisthesis are thought to be a congenitally defective pars interarticularis
|
|
What is occurring in this x-ray? |

Ankylosing Spondylitis - aka Bamboo spine |
|

What is occurring in this x-ray? |

Spondylosis - aka DDD/age related wear and tear affecting discs
|
|

What is occurring in this x-ray? |
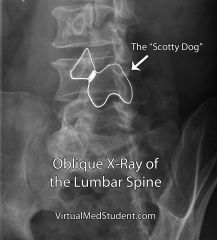
Spondylolysis - aka "scotty dog fracture" - unilateral fracture of pars interarticularis |
|

What is occurring in this x-ray? |

Spondylolisthesis - slippage due to fracture of pars interarticularis (bilaterally?) |
|

what test is this |
Lift off test for (RC) Subscapularis |
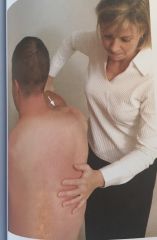
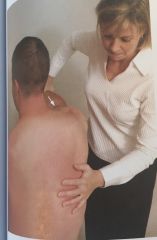
|

what test is this |
Drop Arm Test: identifies tear or full rupture of rotator cuff (supra-spinatus?) -patient sitting with shoulder passively abducted to 120°. Patient instructed slowly to bring arm down to side. Guard patient's arm from falling in case it's gives way (+) = Patient unable to lower arm back to side |
|
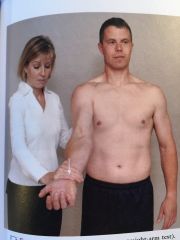
|
Adson's test |

Test for TOS: palpate radial pulse with arm ext. beyond coronal plane -have pt ext. neck -have pt rotate neck toward test side -have pt take deep breath and hold -diminished or absent pulse = + |